
Abstract
Background
Stress affects adolescents’ daily lives by disrupting their working capacity and begets comorbidity. This study aimed to estimate the prevalence of stress symptoms and the factors associated with these symptoms among secondary school-going adolescents in Bangladesh.
Methods
A cross-sectional study using two-stage cluster sampling was conducted. A self-administered questionnaire was given to 2355 adolescents from nine secondary schools in Dhaka, Bangladesh. Of the respondents, 2313 completed the 10-item Perceived Stress Scale (PSS-10). Sociodemographic information, self-reported body image, a modified Leisure Time Exercise Questionnaire (LTEQ), and the WHO Global Physical Activity Questionnaire (GPAQ) were used to determine the sociodemographic and lifestyle factors associated with stress symptoms among adolescents.
Results
Findings suggest that about 65% of adolescents experienced moderate stress symptoms, and about 9% experienced high-stress symptoms. Females (58.7%) suffered more from stress compared to males (41.3%). Age, grade, and residential setting were significantly associated with stress. Logistic regression estimates show that level of physical activity (AOR: 1.52; 95% CI:1.26–1.84), sleep dissatisfaction (AOR: 1.33; 95% CI: 1.07–1.65), and perception of self as overweight/obese (AOR: 1.46; 95% CI: 1.13–1.89) were significantly associated with stress symptoms among adolescents.
Conclusions
Stress symptoms are highly prevalent among secondary school adolescents in Bangladesh. Further exploratory investigations are needed on possible intervention strategies to reduce the burden of stress among adolescents.
Similar content being viewed by others


Introduction
Adolescence, commonly defined as the period between 10 and 19 years [1], is an important phase of human growth and development, bridging childhood to adulthood. The numerous psychosocial and physiological changes adolescents experience during this time make them especially vulnerable to stress [2]. In view of the magnitude of this transition, it is understandable that this period is often characterized as a tempestuous, stressful stage of life [3].
Identified adolescent stressors include rapid changes in their bodies, sexual awakenings, establishing social networks, and a multitude of others, all of which pose threats to stable development and mental well-being. The most significant mental health issues that adolescent stress contributes to are depression, anxiety, suicide, drug use, and antisocial behaviour [4]. Adolescents with elevated stress levels have been found to indulge in a variety of maladaptive and harmful activities, such as increased alcohol and substance use, unprotected sexual intercourse, physical inactivity, unhealthy eating habits, and poor sleep hygiene [2]. The physiological impact stress has on general wellbeing, as well as specific health outcomes, such as weakened immune systems and diseases (cancer, diabetes, dermatological conditions, etc.), are well known. More recently, cognition, coping mechanisms, and social reinforcement have been identified as mediating and moderating factors between stress and different health consequences [4].
Persistent stress symptoms throughout adolescence can lead to chronic stress, which could have a significant impact on livelihood through factors such as job absenteeism. In Sweden, stress is the most frequently diagnosed reason for long-term sick leave, and adults who experienced chronic stress during childhood suffer most. A 2009Swedish study on children’s living conditions estimated that 60% of female and 38% of male high school adolescents suffer from stress-related problems due to daily life stressors [3]. Deterioration in health, an inevitable result of stress, can take the form of mental fatigue, physical weakness, or cognitive difficulties [5]. Studies have shown that Indian adolescents face additional stressors from cultural influences, such as strong parental expectations, constrictive living arrangements, social hierarchies, and academic concerns, to name just a few [6].
In Bangladesh, a substantial number of studies have been conducted on the mental health of youth or tertiary level students [7, 8]. These studies have measured depression, anxiety, and stress levels. However, most studies research stress along with multiple other symptom measures, and a review of the literature shows a dearth of studies on secondary school-aged youths. Furthermore, not a single study focused exclusively on stress among this important sub-population. But addressing stress among adolescents is necessary since chronic stress has the probability of triggering non-communicable diseases (NCDs), such as high blood pressure, heart disease as well as obesity. Apart from these, persisting stress can lead to other mental health conditions including clinical depression and anxiety, which have become more common among youths [9]. This study aims to fill these gaps in the literature by focusing on factors that influence stress levels in secondary school-aged adolescents. To the best of our knowledge, this is one of the few studies that explored secondary school-aged adolescents’ stress and the factors linked to it in Bangladesh.
Methods
Study design and setting
This cross-sectional study was conducted between January 2019 and February 2020 among secondary school students in urban, semi-urban, and rural areas of the Dhaka district (Fig. 1). Dhaka is the capital of Bangladesh and, as such, provides robust population variation for sampling. Information on urbanization of each area was based on a combination of factors, including education, health, civil organization, and other factors. A research team with intimate knowledge of the Dhaka region and beyond had several discussions to identify key areas, from which a convenience sample was drawn. Dhanmondi thana within Dhaka city was the urban data collection site. The semi-urban site was Savar thana, located 24 km northwest of Dhaka. The rural site was Dhamrai Upazila, located 40 km northwest of Dhaka. Variability in socio-economic contexts and accessibility of the areas for the research team were considered when choosing these areas. Sampling techniques were used within these areas to select participants.

Location map of the study area
In the first stage of the study, a list of all the secondary schools in the study areas was prepared. Among 16 secondary schools in the Dhanmondi (urban) area, 14 in the Savar (semi-urban) area, and 16 in the Dhamrai (rural) area, three schools were randomly chosen from each collection site (Fig. 2).

Flow diagram of two-stage sampling procedure
Study population
The targeted population for this study was adolescents of grades 8–10 (12–17 years old), as grades 6–10 are considered secondary education in Bangladesh. A two-stage cluster sampling technique was followed, and the n (713) was multiplied by the three study sites for a minimum sample size of 2139. Using a 10% non-response rate, a target recruitment of 2353 respondents was calculated for this study.
Data collection procedure
Before field implementation of the study, student lists of grades 8, 9, and 10 were collected from respective school authorities. With the support of the headmasters/principals of the schools and the teachers of respective classes, the research team then presented the rationale of the research to students of different classes. Students were instructed to seek permission from their parents to participate, and their parents’ signed consent was required on the consent form students took home. When students returned the completed consent forms the following day, they were given an assent form to ensure that their participation was completely voluntary. After obtaining proper consent and assent from parents and students respectively, data were collected from 2313 students. The data collection procedure was conducted in classrooms with the presence of a schoolteacher, lead researcher, and study team member. Students who did not take part in the study did activities of their choice during data collection.
Outcome measure
Stress symptoms were measured using the 10-item Perceived Stress Scale (PSS-10). The PSS-10measures the degree to which one appraises situations in life as stressful [10]. The PSS-10 has been shown to be an acceptable self-reported tool for screening stress in adolescents within community settings [10,11,12]. Items ask how often respondents have experienced each of 10 symptoms during the past month (e.g., felt upset, felt nervous and stressed, felt unable to control important things in life, felt confident, etc.) using a 5-point Likert scale, with 0 indicating ‘never,’ 1 = almost never, 2 = sometimes, 3 = fairly often, and 4 indicating ‘very often.’ A total score for each adolescent was obtained by summing the scores across all 10 items for a total range of 0 to 40. A higher score indicated higher perceived stress, with a score of 14–26 used to indicate the presence of moderate stress and 27 or more indicating high stress [13].
Standardized Bangla version of PSS-10, achieved by translation from original English version, was utilized in this study. Following the ‘state of the art procedures’ of translation, the standardized Bangla version of the questionnaire was prepared [14]. In keeping with the study objective, the questionnaire was repeatedly revised and reviewed by the research team. Additionally, for the finalization of the questionnaire, an expert questionnaire review panel comprising a professor of public health, a professor of statistics, and two other experts in public health research was formed, who reviewed and edited the questionnaire so that it meets the study objectives. Based on the feedback of the review panel, the questionnaire was modified and sent back to them for the final draft for pre testing.
Other measures
Sociodemographic variables
Data on gender, age, grade in school, birth order, parent education, family size, and residential setting were collected. During data collection, it was discovered that many students did not know their family’s socioeconomic status, so the researchers excluded these questions from the survey.
Lifestyle factors
Following a modified Leisure Time Exercise Questionnaire (LTEQ) and the WHO Global Physical Activity Questionnaire (GPAQ) physical activity and screen based behaviors were measured in this study [15, 16]. Physical activity (PA), Screen-Based Sedentary Behaviour (SBSB), and sleep patterns were measured to assess the lifestyle of the adolescents. Three different PA levels were in the questionnaire: low-level PA (unintentional walking < 30 min/day), moderate PA (walking or meditation/yoga ≥30 min/day), and vigorous PA (jogging, cycling, playing sports, or gym workouts ≥60 min/day) [17,18,19]. To measure SBSB, adolescents were asked how many hours they spent on various medias, such as Facebook, Twitter, Instagram, YouTube, or watching television. High screen time was regarded as > 2 hours/day, which is in line with commonly used screen time guidelines [20].
Statistical analysis
To achieve the objectives of the study both descriptive and inferential statistical analyses were done. To find out the prevalence of stress symptoms among the adolescents, descriptive analysis, such as, frequency, mean etc. were done. After that, to identify any association between different risk factors, inferential analyses, e.g., chi square and logistic regression were conducted. The chi-square test was used to identify any significant relationship between the study variables. Logistic regression models were used to detect any significant associations of the study variables with the outcome variable. Necessary assumptions of regression: independence of errors, linearity in the logit for continuous variables, absence of multicollinearity, and lack of strongly influential outliers, were checked prior to the logistic regression [21]. For the final regression model, adjusted odds ratios (AORs) with 95% Confidence Intervals (CIs) were reported after adjusting for various factors. The level of significance was set at 0.05. The PSS-10 scores were turned into a binary factor, with a cut-point of ≥14 used to differentiate between those who were stressed vs. non-stressed. The Statistical Package for the Social Sciences (SPSS) software for Windows, version 26.0 (IBM, Armonk, NY, USA) was used to analyse all data.
Results
Prevalence of stress symptom among adolescents
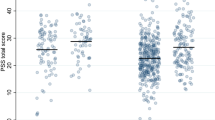
The overall prevalence of stress symptoms among adolescents was found to be 73.5% (considering PSS total score 0–13 as stress negative and ≥ 14 as stress positive). Figure 3 demonstrates the severity of stress symptoms among urban, semi-urban and rural adolescents in Dhaka, Bangladesh. Low stress was found to be prevailing more among rural adolescents (32.00%). On the other hand, semi-urban adolescents were the highest in number suffering from high stress, with 10% of them were found to be experiencing that. Lastly, moderate stress was more prevalent among urban adolescents (70.70%) than among semi-urban and rural adolescents.

Severity of stress symptom in urban, semi-urban and rural areas of Dhaka, Bangladesh
Sociodemographic characteristics of adolescents
In this study, about 40% of the adolescents were from the urban area, while almost 32% were from semi-urban and rural areas respectively [22]. Approximately 52% of the participants were female and the rest of them were male. More than a third (32.2%) of the respondents were of 14 years of age and about two fifths (42.5%) of the participants were studying in class 9. Besides, a larger portion (51.1%) of the respondents reported to be the first child of their parents [22]. In case of parental characteristics, about 40% of the fathers completed graduation or above, while almost 30% of the mothers completed secondary/higher secondary level of education. The fathers and mothers were mostly service holders (43.3%) and homemaker (81.5%) respectively. More than three fifths (62%) of the adolescents reported that they had 4 members or less than that in their families [22].
Relationship between sociodemographic variables and stress symptoms
Table 1 represents associations between sociodemographic variables and stress symptoms. Female gender was found to be significantly associated (χ2: 131.47; p: < 0.001) with stress symptoms, since more than half of them (58.7%) were found to be experiencing the symptoms. Likewise, age (χ2: 24.42; p: < 0.001) and student’s grade (χ2: 10.68; p: 0.005) were also found to have a statistically significant link with stress symptoms. Besides, residential setting was also found to have significant association (χ2: 22.50; p: < 0.001) with stress symptoms, and more than 30% of the urban and semi-urban adolescents were reported to be stressed.
Relationship between lifestyle variables and stress symptoms
Table 2 illustrates associations between the lifestyle factors of the students and stress symptoms. Concerning physical activity (PA), more than 70% of adolescents who were not involved in PA (χ2: 7.12; p: 0.008), did irregular PA (χ2: 4.84; p: 0.028) and reported doing PA < 30 min/day (χ2:28.96; p: < 0.001), were found to have statistically significant association with stress symptoms. Similarly, a statistically significant association between stress symptoms and screen-based recreation (χ2: 7.77; p: 0.005) as well as sleep dissatisfaction (χ2: 14.39; p: < 0.001) was found among approximately three quarters of the adolescents.
Association between study variables and stress symptoms
Table 3 details associations between stress symptoms and study variables from the logistic regression analyses. Both bivariate and multivariate analyses were conducted. Variables were first adjusted for all presented sociodemographic variables (age, gender, grade, residence), and then adjusted for PA, SBSB, sleep patterns, and body perception variables. After this final adjustment for sociodemographic and lifestyle variables, the odds ratios changed slightly.
According to adjusted estimate-1, female adolescents had three times greater risk (AOR: 3.35; 95% CI: 2.74–4.09) of experiencing stress symptoms compared to their male counterparts. Besides, older adolescents (≥15 years) were at 1.38 times (95% CI: 1.06–1.78) higher risk of suffering from stress symptoms than adolescents of < 15 years. In addition, urban adolescents were about two times (AOR: 1.94; 95% CI: 1.53–2.47) more likely to suffer from stress symptoms in compared to rural adolescents, while adolescents from semi-urban area were at 1.35 times higher risk (95% CI: 1.06–1.72) of experiencing stress symptoms than rural adolescents.
In adjusted estimate-2, it has been demonstrated that inactive adolescents or adolescents who were doing low-level PA were at 1.52 times (95% CI: 1.26–1.84) more risk of experiencing stress symptoms than adolescents who reported doing moderate to vigorous PA. Again, adolescents dissatisfied with their sleep were at higher risk (AOR: 1.33; 95% CI: 1.07–1.65) of suffering from stress symptoms than those satisfied with their sleep.
Discussion
Findings from this study suggest that moderate to high stress symptoms are common among secondary school-going adolescents in Bangladesh, with a concerning prevalence estimate of 73.5%. As studies on the prevalence rates of stress symptoms among secondary school-aged adolescents in Bangladesh could hardly be found, an extensive literature search was conducted to find available estimates of similar populations. The prevalence estimate of stress symptoms among adolescents in the present study is much higher than that(24.9%) of a study conducted on 590 university students in 2019 in Bangladesh [23]. Another Bangladeshi study with 105 medical students from 2017 also reported a lower prevalence (59.0%) of stress than that of the present study [24]. University-aged youths may have more developed coping mechanisms for stress than secondary school-aged adolescents. Nonetheless, this discrepancy merits further research. Compared to neighboring countries, the prevalence of stress symptoms in the current study is lower than that (87.6%) reported in a study conducted in Delhi, India [25]. However, a study [26] on secondary school adolescents in Delhi, India reported a slightly lower prevalence of stress (60.9%) than the prevalence reported in the current study. Again, the prevalence estimate reported in this study is also 6% higher than that of a 2019 study conducted among secondary school adolescents who had internet addiction [27]. In a Saudi study of adolescents addicted to gaming, only 11% of the participants experienced stress [28]. These variations difference in the prevalence reported in the above-mentioned studies as well as in the current study might be attributable to differences in measurements, study settings, or targeted populations. With associations between screen use and stress being found insignificant in the current study, further research is needed to investigate any link between screen-use behavior and stress among adolescents.
In the present study, female adolescents had more than three times the odds of suffering from stress symptoms than their male counterparts, which is in keeping with the findings of another study [29]. This specific finding is also consistent with the updated mental health country profile of Bangladesh [30]. This may be explained by factors such as parent-adolescent relationships and inefficacy in academia affecting female adolescents more than male adolescents [31]. Emotional turmoil during this period, physiological changes, and negative gender stereotypes within society might also play important roles as stressors among female adolescents. The odds of experiencing stress significantly rose with grade level and older age among secondary school adolescents in the current study. Given the excessive academic pressures of upcoming graduation examinations in higher grades and increasing family expectations for academic success, this finding is unsurprising. This study suggests that urban adolescents have higher odds of experiencing stress than rural adolescents, which is consistent with the findings of another study [32]. Recent findings suggest that urbanicity does not impact mental health directly, but it is associated with acute autonomic nervous system and hypothalamic-pituitary-adrenal axis reactivity. Apart from this, increased social stress has been observed more in urban environments compared to rural environments, and living in urban environments has been associated with dysregulated stress system functioning [33, 34]. Findings from neuroimaging studies show that adults who grew up and currently live in urban areas demonstrate differential limbic brain area responsivity towards psychosocial stress in comparison to adults living in and brought up in rural areas, although the exact mechanism for this is still unknown [35, 36].
Those who were inactive or engaged in low levels of PA had higher odds of experiencing stress than those who were very physically active. There is an established bidirectional relationship between stress and PA. Studies show that moderate to vigorous PA is helpful in managing stress among secondary school adolescents [37]. On the other hand, stressed adolescents are less likely to engage in PA [38]. The association found between daily sleep satisfaction and stress among adolescents in this study is also consistent with the findings of other studies [39, 40]. Studies have shown school stress, technology use, and academic overload as factors contributing to sleep dissatisfaction among adolescents, which suggests that sleep may also have a bidirectional relationship with stress [39, 41]. Regression analyses from the current study suggest that self-body image plays an important role in understanding stress among secondary school adolescents. Body image dissatisfaction may trigger peer pressure and bullying [42], contributing to feelings of inferiority among adolescents. In the current study, adolescents who perceived themselves as overweight or obese had higher odds of experiencing stress than those who perceived themselves as normal, which is consistent with the literature [29]. Experiencing bullying due to one’s perceived body weight has been found to cause stress among adolescents [43].
Strengths and limitations
Although stress is an alarming public health issue, very few studies have explored stress symptoms among adolescents in Bangladesh. Many of the existing studies cover only one type of geographical region, without comparing urban, semi-urban, and rural areas simultaneously. To the best of our knowledge, this is till now the only study found to investigate stress symptoms among secondary school adolescents from urban, semi-urban, and rural areas in Bangladesh. The diversity of areas covered makes the findings of this study useful in reformulating local policies that impact adolescent mental health. The comprehensive data collection allows this study to stand out among the limited research available.
One of the limitations of this study lie in the cross-sectional nature of this study, as no causality can be established. Measures used relied on self-reported information, which always involves risks of recall and reporting bias. Although data were collected from regions representing urban, semi-urban, and rural environments, only a small portion of each area was sampled, limiting the generalizability of the findings. Furthermore, the findings of this study might also not be fully representative of populations across all districts of the country. Future research may therefore focus on conducting large-scale longitudinal studies that will cover a nationwide representative sample.
Conclusion
Stress symptoms are highly prevalent among secondary-school adolescents in Bangladesh. Immediate and adequate interventions are needed to address the issue of stress prevalent among adolescents. Findings suggest a need to test if interventions to encourage modification of different lifestyle factors among adolescents will improve their mental health.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
WHO. Adolescent health: World Health Organization; 2022. Available from: https://www.who.int/health-topics/adolescent-health#tab=tab_1
Rentala S, Nayak RB, Patil SD, Hegde GS, Aladakatti R. Academic stress among Indian adolescent girls. J Educ Health Promot. 2019;8:158. https://doi.org/10.4103/jehp.jehp_116_19 Epub 2019/09/24. PubMed PMID: 31544123; PubMed Central PMCID: PMCPMC6745887.
Schraml K, Perski A, Grossi G, Simonsson-Sarnecki M. Stress symptoms among adolescents: the role of subjective psychosocial conditions, lifestyle, and self-esteem. J Adolesc. 2011;34(5):987–96. https://doi.org/10.1016/j.adolescence.2010.11.010 Epub 2010/12/15. PubMed PMID: 21147499.
Krapić N, Hudek-Knežević J, Kardum I. Stress in adolescence: effects on development. Int Encycl Soc Behav Sci. 2015;23:562–9.
Schaufeli W, Enzmann D. The burnout companion to study and practice: a critical analysis: CRC Press; 1998.
Arun P, Garg R, Chavan BS. Stress and suicidal ideation among adolescents having academic difficulty. Ind Psychiatry J. 2017;26(1):64–70. https://doi.org/10.4103/ipj.ipj_5_17 Epub 2018/02/20. PubMed PMID: 29456324; PubMed Central PMCID: PMCPMC5810170.
Arusha AR, Biswas RK. Prevalence of stress, anxiety and depression due to examination in Bangladeshi youths: A pilot study. Child Youth Serv Rev. 2020;116:105254. https://doi.org/10.1016/j.childyouth.2020.105254 Epub 2020/08/25. PubMed PMID: 32834273; PubMed Central PMCID: PMCPMC7367775.
Hossain S, Anjum A, Uddin ME, Rahman MA, Hossain MF. Impacts of socio-cultural environment and lifestyle factors on the psychological health of university students in Bangladesh: a longitudinal study. J Affect Disord. 2019;256:393–403. https://doi.org/10.1016/j.jad.2019.06.001 Epub 2019/06/22. PubMed PMID: 31226611.
APA. How to help children and teens manage their stress: American Psychological Association; 2019. Available from: https://www.apa.org/topics/child-development/stress#:~:text=Prolonged%20stress%20can%20cause%20high,becoming%20more%20common%20in%20youth.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:386–96.
van Jaarsveld CH, Fidler JA, Steptoe A, Boniface D, Wardle J. Perceived stress and weight gain in adolescence: a longitudinal analysis. Obesity (Silver Spring). 2009;17(12):2155–61. https://doi.org/10.1038/oby.2009.183 Epub 2009/06/13. PubMed PMID: 19521353.
Lee EH. Review of the psychometric evidence of the perceived stress scale. Asian Nurs Res (Korean Soc Nurs Sci). 2012;6(4):121–7. https://doi.org/10.1016/j.anr.2012.08.004 Epub 2012/12/01. PubMed PMID: 25031113.
Swaminathan A, Viswanathan S, Gnanadurai T, Ayyavoo S, Manickam T. Perceived stress and sources of stress among first-year medical undergraduate students in a private medical college - Tamil Nadu. Natl J Physiol Pharm Pharmacol. 2016;6(1). https://doi.org/10.5455/njppp.2015.5.1909201574.
Bracken BA, Barona A. State of the art procedures for translating, validating and using Psychoeducational tests in cross-cultural assessment. Sch Psychol Int. 2016;12(1–2):119–32. https://doi.org/10.1177/0143034391121010.
Godin G. The Godin-Shephard leisure-time physical activity questionnaire. Health Fitness J Canada. 2011;4(1):18–22. https://doi.org/10.14288/hfjc.v4i1.82.
Armstrong T, Bull F. Development of the World Health Organization global physical activity questionnaire (GPAQ). J Public Health. 2006;14(2):66–70. https://doi.org/10.1007/s10389-006-0024-x.
WHO. Global physical activity questionnaire (GPAQ): World Health Organization; 2021. Available from: https://www.who.int/publications/m/item/global-physical-activity-questionnaire.
Anjum A, Hossain S, Sikder T, Uddin ME, Rahim DA. Investigating the prevalence of and factors associated with depressive symptoms among urban and semi-urban school adolescents in Bangladesh: a pilot study. Int Health. 2019. https://doi.org/10.1093/inthealth/ihz092 Epub 20191106. PubMed PMID: 31693088.
Godin G, Shephard RJ. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci. 1985;10(3):141–6.
Khan A, Burton NW. Screen-Based Behaviors of Adolescents in Bangladesh. J Phys Act Health. 2016;13(11):1156–63. https://doi.org/10.1123/jpah.2015-0514 Epub 20160824. PubMed PMID: 27334303.
Stoltzfus JC. Logistic regression: a brief primer. Acad Emerg Med. 2011;18(10):1099–104. https://doi.org/10.1111/j.1553-2712.2011.01185.x PubMed PMID: 21996075.
Anjum A, Hossain S, Hasan MT, Uddin ME, Sikder MT. Anxiety among urban, semi-urban and rural school adolescents in Dhaka, Bangladesh: investigating prevalence and associated factors. PLoS One. 2022;17(1):e0262716. https://doi.org/10.1371/journal.pone.0262716 Epub 20220121. PubMed PMID: 35061810; PubMed Central PMCID: PMCPMC8782381.
Mamun MA, Hossain MS, Griffiths MD. Mental health problems and associated predictors among Bangladeshi students. Int J Ment Heal Addict. 2019. https://doi.org/10.1007/s11469-019-00144-8.
Alim SMAHM, Rabbani MG, Karim E, Mullick MSI, Al Mamun A, Khan MZR. Assessment of depression, anxiety and stress among first year MBBS students of a public medical college, Bangladesh. Bangladesh J Psychiatry. 2017;29(1):23–9.
Watode BK, Kishore J, Kohli C. Prevalence of stress among school adolescents in Delhi. Indian J Youth Adolesc Health. 2015;2(4):5–9.
Kumar A, Yadav G, Chauhan N, Bodat S. Prevalence of depression, anxiety and stress among school going adolescents in Delhi: a cross sectional study. Int J Community Med Public Health. 2019;6(12). https://doi.org/10.18203/2394-6040.ijcmph20195177.
Ali A, Horo A, Swain MR, Gujar NM, Deuri SP. The prevalence of internet addiction and its relationship with depression, anxiety and stress among higher secondary school students: north-east perspective. J Indian Assoc Child Adolesc Mental Health. 2019;15(1):13–26.
Rajab AM, Zaghloul MS, Enabi S, Rajab TM, Al-Khani AM, Basalah A, et al. Gaming addiction and perceived stress among Saudi adolescents. Addict Behav Rep. 2020;11:100261. https://doi.org/10.1016/j.abrep.2020.100261 Epub 2020/05/30. PubMed PMID: 32467850; PubMed Central PMCID: PMCPMC7244928.
Pinto AA, Claumann GS, Medeiros PD, Barbosa RMSP, Nahas MV, Pelegrini A. AssociaÇÃo Entre Estresse Percebido Na AdolescÊncia, Peso Corporal E Relacionamentos Amorosos. Rev Paul Pediatr. 2017;35(4):422–8. https://doi.org/10.1590/1984-0462/;2017;35;4;00012.
Hasan MT, Anwar T, Christopher E, Hossain S, Hossain MM, Koly KN, et al. The current state of mental healthcare in Bangladesh: part 1 - an updated country profile. BJPsych Int. 2021;18(4):78–82. https://doi.org/10.1192/bji.2021.41 PubMed PMID: 34747942; PubMed Central PMCID: PMCPMC8554893.
Fam JY, Yaacob SN. Correlates of stress among female adolescents. J Psikologi Malaysia. 2018;32(1):126–35.
Dey BK, Rahman A, Bairagi A, Roy K. Stress and anger of rural and urban adolescents. Psychology. 2014;05(03):177–84. https://doi.org/10.4236/psych.2014.53028.
Lederbogen F, Haddad L, Meyer-Lindenberg A. Urban social stress--risk factor for mental disorders. The case of schizophrenia. Environ Pollut. 2013;183:2–6. https://doi.org/10.1016/j.envpol.2013.05.046 Epub 2013/06/25. PubMed PMID: 23791151.
Mizrahi R. Social Stress and Psychosis Risk: Common Neurochemical Substrates? Neuropsychopharmacology. 2016;41(3):666–74. https://doi.org/10.1038/npp.2015.274 Epub 2015/09/09. PubMed PMID: 26346639; PubMed Central PMCID: PMCPMC4707841.
Lederbogen F, Kirsch P, Haddad L, Streit F, Tost H, Schuch P, et al. City living and urban upbringing affect neural social stress processing in humans. Nature. 2011;474(7352):498–501. https://doi.org/10.1038/nature10190 Epub 2011/06/24. PubMed PMID: 21697947.
Streit F, Haddad L, Paul T, Frank J, Schafer A, Nikitopoulos J, et al. A functional variant in the neuropeptide S receptor 1 gene moderates the influence of urban upbringing on stress processing in the amygdala. Stress. 2014;17(4):352–61. https://doi.org/10.3109/10253890.2014.921903 Epub 2014/05/08. PubMed PMID: 24800784.
Kim HJ, Oh SY, Lee DW, Kwon J, Park EC. The Effects of Intense Physical Activity on Stress in Adolescents: Findings from Korea Youth Risk Behavior Web-Based Survey (2015–2017). Int J Environ Res Public Health. 2019;16(10). https://doi.org/10.3390/ijerph16101870 Epub 2019/05/30. PubMed PMID: 31137869; PubMed Central PMCID: PMCPMC6572335.
Stults-Kolehmainen MA, Sinha R. The effects of stress on physical activity and exercise. Sports Med. 2014;44(1):81–121. https://doi.org/10.1007/s40279-013-0090-5 Epub 2013/09/14. PubMed PMID: 24030837; PubMed Central PMCID: PMCPMC3894304.
Jakobsson M, Josefsson K, Jutengren G, Sandsjo L, Hogberg K. Sleep duration and sleeping difficulties among adolescents: exploring associations with school stress, self-perception and technology use. Scand J Caring Sci. 2019;33(1):197–206. https://doi.org/10.1111/scs.12621 Epub 2018/10/13. PubMed PMID: 30311255.
Mesquita G, Reimao R. Stress and sleep quality in high school brazilian adolescents. An Acad Bras Cienc. 2010;82(2):545–51. https://doi.org/10.1590/s0001-37652010000200029 Epub 2010/06/22. PubMed PMID: 20563434.
Ramamoorthy S, Kamaldeen D, Ravichandran L, Sundaramahalingam M. Effect of stress on sleep hygiene among school going adolescents in Chennai. J Family Med Prim Care. 2019;8(9):2917–20. https://doi.org/10.4103/jfmpc.jfmpc_564_19 Epub 2019/11/05. PubMed PMID: 31681667; PubMed Central PMCID: PMCPMC6820412.
Murray KM, Byrne DG, Rieger E. Investigating adolescent stress and body image. J Adolesc. 2011;34(2):269–78. https://doi.org/10.1016/j.adolescence.2010.05.004 Epub 2010/07/16. PubMed PMID: 20627369.
Ganapathy SS, Tan L, Sooryanarayana R, Hashim MH, Saminathan TA, Ahmad FH, et al. Body Weight, Body Weight Perception, and Bullying Among Adolescents in Malaysia. Asia Pac J Public Health. 2019;31(8_suppl):38S–47S. https://doi.org/10.1177/1010539519879339 Epub 2019/10/17. PubMed PMID: 31617372.
Acknowledgements
We would like to thank all the participants who voluntarily offered their time, conscientiously documented their lives, and provided honest and thoughtful responses. We also thank the personnel who supported field implementation and data collection of this study. Our heartfelt thanks and gratitude are also due to the respective authorities of the schools for their permission to collect data.
Funding
This study was funded by the Ministry of Science and Technology of the People’s Republic of Bangladesh under NST Fellowship-2019.
Author information
Authors and Affiliations
Contributions
Afifa Anjum: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Writing - original draft, Writing – review & editing, Validation. Sahadat Hossain: Conceptualization, Investigation, Data curation, Writing - review & editing, Validation. M. Tasdik Hasan: Writing - review & editing, Validation. Enryka Christopher: Writing - review & editing, Validation. Md. Elias Uddin: Writing - review & editing, Validation. Md. Tajuddin Sikder: Conceptualization, Supervision, Writing - review & editing, Validation. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the Institutional Review Board of Jahangirnagar University (Ref No: BBEC, JU/ M/ 2019 (8) 3). Written informed consent was obtained from all individual participants included in the study (if participants are under 16, from a parent).
We confirm that all the methods in this study were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Anjum, A., Hossain, S., Hasan, M.T. et al. Stress symptoms and associated factors among adolescents in Dhaka, Bangladesh: findings from a cross-sectional study. BMC Psychiatry 22, 807 (2022). https://doi.org/10.1186/s12888-022-04340-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04340-0