
Abstract
Background
Validated measures of patient-reported experiences are essential for assessing and improving the quality of mental health services and interventions. In Norwegian mental healthcare settings, the Client Satisfaction Questionnaire (CSQ-8) is increasingly being used for this purpose, but the validity and reliability of the Norwegian translation have not been investigated.
Methods
We examined the factor structure and internal consistency of a digitally administrated Norwegian translation of the CSQ-8 in a sample of 338 patients recruited from outpatient treatment. The relationship between satisfaction scores and the change in symptom severity during treatment, measured by the Patient Health Questionnaire-4, was also investigated.
Results
The Norwegian CSQ-8 showed a clear unidimensional structure with one factor explaining 74% of the variance. Internal consistency was very high, with a Cronbach’s alpha of 0.95. Satisfaction showed a small-to-moderate negative relationship with change in symptom severity. Satisfaction scores were negatively skewed, and the presence of ceiling effects is discussed.
Conclusion
Our results support the use of the Norwegian CSQ-8 as a valid and reliable measure of satisfaction with mental healthcare services. Further studies are needed to determine the test-retest reliability of the questionnaire, its sensitivity to change, and to assess its propensity to ceiling effects.
Similar content being viewed by others


Background
Over the last several decades, patients’ satisfaction with services has emerged as an essential outcome measure in health care quality assessment and is viewed as a necessary addition to more traditional outcome measures, such as symptom reduction. Patient satisfaction is also a major political issue worldwide, and regarded as an important outcome, with international organizations such as The World Health Organization, The Commonwealth Fund, and the Organisation for Economic Co-operation and Development, emphasizing the importance of conducting both national, and cross-national studies [1]. Larsen et al. [2] have highlighted three main reasons for its importance. First, measuring the clinicians’ perspective alone leads to an incomplete and biased appraisal of services provided. The second reason refers to the need to adhere to legislative mandates of patient involvement. The third reason is the importance of maintaining the interests of vulnerable populations, e.g., people of low socioeconomic status, who may be unable to choose between different health service alternatives.
Although the assessment of patient satisfaction has been stressed as essential for evaluating the quality of mental healthcare [3,4,5,6], different systematic reviews have described the patient satisfaction literature as flawed [5, 7, 8]. In particular, the lack of gold standard measures with well-established psychometric properties has been highlighted. In addition, many measures have been developed ad-hoc and used only a handful number of times, which makes it difficult to conduct inter-program comparisons and comparisons across different samples.
The Client Satisfaction Questionnaire (CSQ) is one of the most used questionnaires for measuring patient-reported satisfaction in mental healthcare settings [5, 9]. While different versions exist (varying from 3 to 18 items), the CSQ-8, with eight items, is the most widely used. Each question is answered on a 4-point scale (possible range from eight to 32, where a higher score indicates a higher level of overall satisfaction with services[2, 10,11,12].
Globally, the CSQ-8 has been translated into 51 languages [10] and used to assess patient satisfaction in a range of mental healthcare services. The CSQ-8 has been used in studies examining the quality of inpatient forensic services, community and substance abuse services, inpatient services, and outpatient clinical settings[5]. In addition, the CSQ has been used to assess patient satisfaction across various populations, including both voluntary and involuntary admitted patients [13], as well as pre-therapy educational interventions [11, 14], teletherapy [15], and follow-up interventions [16]. Finally, a slightly modified version has been used to evaluate web-based treatments [17].
The original English version of the CSQ-8 showed good internal consistency and one-factor structure [12]. Validated translations include German [18], French [19, 20], Spanish [21, 22], Thai [23], Japanese [24], Dutch [25, 26], and Cebuano and Wary, two regional languages in the Philippines [27]. Results from these studies dovetail with the findings from Nguyen et al., [12] and suggest that the questionnaire possesses good to excellent internal consistency, and a clear unidimensional factor structure across the different translations [2, 10, 12, 19, 22, 25,26,27,28]. In all of the beforementioned validation studies, the questionnaire has been administrated primarily by paper, sent by mail [25, 26], or filled out on-site [2, 10, 12, 21, 22, 29]. Interview has also been used, either on-site [27] or over the telephone [19]. In addition, a validation of a slightly modified version, specifically adapted to measure satisfaction with web interventions, suggests that it might also be suitable for digital use [17]. However, despite its frequent use, a digital version of the CSQ-8 has never been validated. There are often a priori assumptions about the equivalency of digital questionnaires and their pen and paper counterparts, but a systematic review conducted by Alfonsson et al., found that interformat reliability varied from r = .35 to r = .99 [30]. They proposed several reasons for the disparity: difference in the context where the questionnaire is filled out (e.g., at home instead of on-site), the visual presentation of questions (e.g., one question at a time instead of everything at once), and the level of perceived anonymity. Therefore, equivalency cannot be assumed.
The CSQ-8 has been shown to correlate with treatment outcome, measured both in symptom relief and well-being, and treatment adherence; higher satisfaction is associated with treatment adherence, while dissatisfaction is associated with a higher risk of dropping out [9, 31,32,33].
The validation of a Norwegian translation of the CSQ-8 is particularly timely. First, over the last few years, it has increasingly been used as a measure of patient satisfaction [14, 15, 34,35,36,37,38,39,40,41,42,43]. Second, several registered trials plan to use the questionnaire as an outcome measure [44,45,46,47,48]. Despite this, the psychometric properties of a Norwegian version of the questionnaire have never been investigated. As a digitally administered CSQ-8 is warranted, this study aims to test the psychometric properties of a digital Norwegian version of the CSQ-8.
In line with previous research, we expect the Norwegian digital version of the CSQ-8 to be unidimensional, have good internal consistency, be negatively correlated with change in symptom severity during treatment, and not be correlated with age [2, 12, 49]. We also do not expect sex differences in satisfaction.
Methods
Participants and data collection
The data used in this study were collected from 338 patients referred to the outpatient sections of the Nidaros DPS, a community mental health care center in Trondheim, Norway, between March 2020 and September 2021. As part of treatment, every patient received a battery of electronic self-report questionnaires, which were completed a few days before starting treatment, and immediately after treatment termination. Symptom severity was measured both before and after treatment. The CSQ-8 was administered only at treatment termination.
Patients were prompted by a text message inviting them to participate in research and their assessment process. After clicking on the provided link, they were first required to give their consent before answering any of the questionnaires. Both the consent form and the questionnaires were answered on a secure online server provided by the company Checkware AS. Because the results are explicitly used in the treatment assessment process (a therapist can see the self-reported data of her own patients), the degree of anonymity felt by the patients is uncertain.
To be eligible for inclusion in this study, participants had to: be referred to Nidaros DPS for psychological assessment and/or treatment in the given period, provide informed consent for their participation, and be at least 18 years old. Second, patients that did not report symptom severity either before or following treatment termination, or satisfaction at treatment termination were excluded. All other patients were included. The final sample consisted of 338 patients, 66% female, with a mean age of 29.97 years.
This study was approved by the Regional Committee for Medical Research and Ethics in Norway (REK 2019/31,836) and the Norwegian Centre for Research Data (2019/605,327). Every participant was informed that participation was voluntary and that they could withdraw at any time without it affecting any other aspects of their treatment or resulting in any future consequences.
Measures
The client satisfaction questionnaire 8
A digital Norwegian version of the CSQ-8 was administrated to the sample to assess overall satisfaction with services in secondary mental health care. The questionnaire consists of eight items, measured on a scale ranging from one to four, with a possible score ranging from eight to 32 [2, 12]. Higher scores indicate higher satisfaction. Two additional open questions to be answered in free text were added; the first asked if the patient had any additional comments, the second asked if they had any suggestions for service improvement.
The patient health questionnaire 4
To measure change in symptoms, the Patient Health Questionnaire 4 (PHQ-4) [50] was used. This is a four-item questionnaire measuring symptoms of depression and anxiety derived from The Patient Health Questionnaire nine items [51] and The Generalized Anxiety Disorder Scale seven items [52]. The first two questions assess symptoms of depression, while the last two assess symptoms of anxiety. All questions are preceded by “over the last two weeks, how often have you been bothered by the following problems?”. Possible answers are presented on a four-point scale ranging from “not at all” to “nearly every day”, scored 0 through 3, making a possible score range of 0–12 [50]. A higher score indicates higher symptom severity. Symptom change was calculated by subtracting the symptom severity score before the start of treatment from the score at treatment termination.
Statistical analyses
Mean and standard deviation were calculated for the total score of the CSQ-8 and individual items. Descriptive statistics of the sample and Spearman rank-order correlation coefficients were calculated to explore the relationship between age and satisfaction, and the relationship between change in symptoms and service satisfaction. A Mann-Whitney U-test was conducted to test if there was a statistical difference in satisfaction scores between the sexes. Sex was treated as a binary variable, and the one person not specifying their sex was omitted from this analysis.
Score distribution analysis was performed in terms of range, kurtosis, and skew. Floor and ceiling effects were also examined, by calculating the percentage of scores at minimum or maximum values. Terwee et al., [53] have suggested a cut-off of 15% to indicate ceiling or floor effects in a measure.
The inter-item correlation coefficient for each item and Cronbach’s α were used to examine internal consistency. The factor structure was evaluated with exploratory factor analysis and principal component analysis, after computing the Kaiser-Meyer-Olkin measure of sampling adequacy and Bartlett’s test of sphericity. Considerations regarding sample size were guided by the Consensus-based Standards for the Selection of Health Measurement Instruments-COSMIN [54]. For factor analysis, the COSMIN recommends a sample size of 7 times the number of items, and > 100 is recommended.

Distribution of Satisfaction scores
No imputations were done, and missing results were excluded pairwise, thus counted as a zero in calculating the total score. All analyses were executed using version 27 of IBM SPSS Statistics.
Results
Descriptive statistics of satisfaction scores
Frequencies of different scores for individual items are presented in Table 1. Missing data were less than the recommended cut-off of 5% on all variables [55], with item 8 having the most missing values (2.1%).
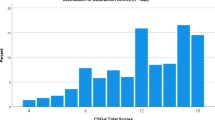
Means and standard deviations for each item are presented in Table 2. Figure 1 shows the distribution of CSQ-8 scores for the sample (M = 23.67, SD = 6.08, Median = 24.00). The scores were not normally distributed, indicated by a significant Shapiro-Wilk test (p < .001), and negatively skewed (Skewness = − 0.50, SE = 0.13; Kurtosis = − 0.50, SE = 0.26). The maximum score (32) was the most common (10.4%). Of the 338 patients in the sample, 112 (33%) answered one or both open questions.
Correlations with, and sex difference in, satisfaction
Information about age and sex are presented in Table 3. A Spearman’s rank correlation was computed to assess the relationship between satisfaction and age, and satisfaction and symptom change during treatment. A statistically significant, but small-to-negligible correlation was found between age and satisfaction, r (335) = 0.13, p = .021. A moderate negative correlation was found between satisfaction and change in symptoms (r (321) = − 0.355, p < .001) in the data. The Mann-Whitney U test found no statistical difference in satisfaction scores between men (Mdn = 25) and women (Mdn = 24), U(Nmen = 113, Nwomen = 224) = 36469.50, z = -1, p =. 100.
Factor structure
The Bartlett’s Test of Sphericity was significant at the p < .001 level, and the Kaiser-Meyer-Olkin Measure was 0.943. Factors were extracted by Kaiser’s criterion. One factor showed an Eigenvalue exceeding 1, explaining 74.1% of the variance (Eigenvalue = 5.93). A scree plot for the data is provided in Fig. 2. All factor loadings exceeded 0.80. An overview of factor loadings is presented in Table 2.

Scree plot of the digital Norwegian CSQ-8
Internal reliability
The CSQ-8 showed very high internal consistency with alpha values of 0.95, with no higher scores if any of the items were to be deleted, and all items showed a corrected Item-total correlation higher than the recommended cut-off of 0.70 [54]. All values are presented in Table 4.
Discussion
This study aimed to test, for the first time, the psychometric properties of a digital version of the CSQ-8, a satisfaction measure widely used worldwide, which in recent years has seen increased use in Norway.
The Norwegian version appears to have a solid unidimensional structure and very high internal consistency. The amount of variance explained by the single factor is comparable to the normative English American sample (74.1% compared to 75%) [2, 12]. In other validation studies, the total variance explained has ranged from 48.8% (Eigenvalue = 3.89) in the Waray translation [27] to 65.5% (Eigenvalue = 5.24) in the Dutch translation [26]. A shorter version of the CSQ-8, the CSQ-3, consisting of item 3, 7, and 8, has been suggested after analysing the factor loadings that emerged out of the normative sample [12]. In this study, item 2, 3, and 7 had the highest factor loadings, with item 7 having the highest. All factor loadings are presented in Table 2. An alpha value of 0.95 is higher than other alpha values in the literature, which range from 0.80 [22] to 0.94 [55], and 0.87, the value found in the normative English sample [12].
As stated in the introduction, we hypothesized a priori that satisfaction scores would be correlated with treatment characteristics and not client variables. Our results corroborate this hypothesis as we observed a small-to-moderate negative correlation with change in symptoms and no statistical difference in satisfaction between sexes. However, contrary to our hypothesis, we found a weak-to-negligible relationship between age and satisfaction. This mirrors findings from previous validation studies [2, 28, 29, 33, 49]. It is worth noting that there are clinical contexts where we might expect patient characteristics (gender, age differences or other characteristics) to be associated with satisfaction, and contexts where symptom change may not be associated with satisfaction. These contexts include palliative care or the support of people with chronic or degenerative diseases. In turn, patient characteristics may be relevant in treatment settings where one population is in a minority, in populations with heightened stigma, or in more specialized treatment approaches of psychiatric problems which has a different expression in different genders, such as ADHD, autism spectrum disorder, or eating disorders.
As found by earlier studies, the satisfaction scores were in general high, with a mean of M = 23.67, and negatively skewed. Ceiling effects is a common problem with satisfaction measures. In the validation study of the Castilian Spanish version, 20% of participants obtained the maximum score of 32 [22]; in the validation study of the Dutch version, 13% obtained the maximum score [26]; Kelly et al., [28] validated the English version in a substance abuse population, here, 20% obtained a score range of 31–32. Although the maximum score of 32 was the most common (10.4%) in our study and below the proposed cut-off of 15% for ceiling effects [53], the distribution of scores on individual items is concerning (presented in Table 1). This is further discussed below.
It may also be worth noting that item 3 (“To what extent has our service met your needs?”) had the lowest mean in our sample, a tendency seen in other studies as well [10, 12, 22, 28]. Although “overall satisfaction” is a broad term, these results imply that the Norwegian CSQ-8 is a narrow measure of a general sense of satisfaction and may not capture specific domains of patient dissatisfaction that occur in parallel with specific domains of satisfaction.
Even though psychometric equivalency between paper and digital versions cannot be assumed, the CSQ-data derived from the online server performed well and our findings are comparable to the original English version, and other validated translations[2, 10, 12, 19, 22, 25,26,27,28]. Our study found that the digital version of the CSQ-8 showed a solid factor structure and very high internal reliability, implying that it is a valid measure of overall satisfaction with mental health care services. However, as a good measure of global, overall satisfaction, the CSQ-8’s ability to capture dissatisfaction over specific domains of the treatment context may be limited. A low score does not reveal much information about the treatment received and gives few details about the actual problem or cause of dissatisfaction. The inclusion of two additional open questions at the end of the questionnaire, answered in free text, may remedy this problem. One-third of the participants answered at least one open question. This implies that people see these questions as an opportunity to communicate any idiosyncratic needs or feedback that the other questions did not cover.
There is uncertainty surrounding the degree patients felt their answers were anonymous. However, the research on the effects of administrating the CSQ-8 anonymously is not conclusive, where some research has found an effect [56] while other research with a much bigger sample (1397 compared to 100), albeit with a modified version of the CSQ, has not [57]. Although the measures of symptom severity are included and explicitly used by the therapists during assessment, the CSQ-8 may be in a special position since its content does not directly address themes relevant to the treatment process, but the process itself. More research is needed, however, before concluding anything about the beliefs of patients answering the CSQ-8. Which people do they believe have access to their answers? What type of feedback do they think the CSQ-8 asks for specifically and in what context will it be used to evaluate and maybe change existing practices?
In addition, in our sample, the scores were negatively skewed with a high percentage of maximum scores across individual items, giving rise to the question of whether or not the questionnaire is a good differentiator between nuances of high satisfaction and the degree of responsiveness to improvements in satisfaction [53]. To deal with ceiling effects in other satisfaction measures, a 5-point instead of a 4-point scale has been suggested [58]. However, a possible explanation for this might be that these observed ceiling effects might be better explained by selection bias, which is further discussed below.
The findings of this study should be seen in light of its limitations. All patients that gave informed consent before treatment initiation received the digital CSQ-8 at treatment termination. However, we cannot rule out the risk of selection bias. For example, patients dropping out may be less inclined to fill out questionnaires at treatment termination and may therefore be underrepresented in our sample, or patients who were more satisfied with their treatment may be more prone to completing the questionnaire. This may also explain the skewness and potential ceiling effects observed in our data. Further research should thus investigate if there are patient or treatment course characteristics that are systematically associated with not answering satisfaction measures. Also, as measuring satisfaction at the end of treatment might be vulnerable to bias, more studies where satisfaction is measured at multiple time points during treatment are needed. This is necessary to further assess the psychometric properties of the Norwegian CSQ-8 by making investigations of test-retest reliability and sensitivity to change possible.
Although mean age was assumed to be representative of the Norwegian outpatient population in community mental health care centers [59], our sample was fairly young (mean age 29.9 years) and generalization to less digitally literate populations should be done with caution (e.g., a geriatric population).
Despite its weaknesses, the strengths of the study should also be highlighted. First, data were collected in a large and appropriate sample of the target population, with an ‘observation to variables’ ratio of 42:1. Second, this study differs from previous validation studies in that it primarily evaluates the digital administration of the CSQ-8 in a clinical setting. Third, adding two open questions to the CSQ-8 is a novelty. This study suggests that a substantial number of patients answer these questions, which in turn can enrich the description of patient experiences if future researchers or clinicians wish to capture more idiosyncratic aspects of patients’ experiences or want more specific feedback on possible improvements in mental health settings. Even though qualitative analysis of open questions is outside the scope of this study, we hope these findings can guide future research which should aim to further explore the utility of such answers alongside aggregated satisfaction scores.
Conclusion
This study aimed to test the psychometric properties of a digital Norwegian version of the CSQ-8, a measure of patients’ overall satisfaction with treatment. The reported data shows for the first time that the digital Norwegian version of the CSQ-8 demonstrates good psychometric properties, and is comparable to the original English version, and other validated translations. The Norwegian CSQ-8 has excellent internal consistency and a robust unidimensional structure. Potential ceiling effects and sensitivity to change require more research. Specifically, future research designs should focus on measuring patient satisfaction at multiple time points. Despite these limitations, we argue that this study indicates that the digital CSQ-8 is an acceptable and feasible measure of treatment satisfaction in Norwegian outpatient populations in adult mental healthcare.
Availability of data and materials
The dataset analysed during the current study is not publicly available, but it can be available from the corresponding author on reasonable written request.
Abbreviations
- CSQ:
-
The Client Satisfaction Questionnaire.
- CSQ-8:
-
The Client Satisfaction Questionnaire 8-item version.
- M:
-
Mean.
- PHQ-4:
-
Patient Health Questionnaire 4-item version.
- SD:
-
Standard Deviation.
- REK:
-
Regional Etisk Kommite. Translated:Regional Ethical Committee.
References
Garratt A, Bjørngaard JH, Dahle KA, Bjertnaes OA, Saunes IS, Ruud T. The Psychiatric Out-Patient Experiences Questionnaire (POPEQ): data quality, reliability and validity in patients attending 90 Norwegian clinics. Nord J Psychiatry. 2006;60(2):89–96.
Larsen DL, Attkisson CC, Hargreaves WA, Nguyen TD. Assessment of client/patient satisfaction: development of a general scale. Eval Program Plann. 1979;2(3):197–207.
Cleary PD, McNeil BJ. Patient satisfaction as an indicator of quality care. Inquiry. 1988;25(1):25–36.
Edlund MJ, Young AS, Kung FY, Sherbourne CD, Wells KB. Does Satisfaction Reflect the Technical Quality of Mental Health Care? Health Serv Res. 2003;38(2):631–45.
Miglietta E, Belessiotis-Richards C, Ruggeri M, Priebe S. Scales for assessing patient satisfaction with mental health care: A systematic review. J Psychiatr Res. 2018;100:33–46.
Shipley K, Hilborn B, Hansell A, Tyrer J, Tyrer P. Patient satisfaction: a valid index of quality of care in a psychiatric service. Acta Psychiatr Scand. 2000;101(4):330–3.
Gill L, White L. A critical review of patient satisfaction. Leadersh Health Serv. 2009;22(1):8–19.
Ruggeri M. Patients’ and relatives’ satisfaction with psychiatric services: the state of the art of its measurement. Soc Psychiatry Psychiatr Epidemiol. 1994;29(5):212–27.
Woodward S, Berry K, Bucci S. A systematic review of factors associated with service user satisfaction with psychiatric inpatient services. J Psychiatr Res. 2017;92:81–93.
Attkisson CC. Client Satisfaction Questionnaire (CSQScales®) Brief Summary 2020 [Available from: https://csqscales.com/wp-content/uploads/2020/01/CSQ-Scales-Bibliography-2020-02-01.pdf.
Attkisson CC, Zwick R. The client satisfaction questionnaire: Psychometric properties and correlations with service utilization and psychotherapy outcome. Eval Program Plann. 1982;5(3):233–7.
Nguyen TD, Attkisson CC, Stegner BL. Assessment of patient satisfaction: development and refinement of a service evaluation questionnaire. Eval Program Plann. 1983;6(3–4):299–313.
Smith D, Roche E, O’Loughlin K, Brennan D, Madigan K, Lyne J, et al. Satisfaction with services following voluntary and involuntary admission. J Ment Health. 2014;23(1):38–45.
Lara-Cabrera ML, Salvesen Ø, Nesset MB, De las Cuevas C, Iversen VC, Gråwe RW. The effect of a brief educational programme added to mental health treatment to improve patient activation: A randomized controlled trial in community mental health centres. Patient Educ Couns. 2016;99(5):760–8.
Christensen LF, Gildberg FA, Sibbersen C, Skjoeth MM, Nielsen CT, Hansen JP Videoconferences and Treatment of Depression: Satisfaction Score Correlated with Number of Sessions Attended but Not with Age. Telemedicine and e-Health. 2020;26(7):898–904.
Takano A, Matsumoto TA, Mixed-Methods. Evaluation of Usability and Acceptability of Web-Based Relapse Prevention and Self-Monitoring Program: Secondary Analysis of a Pilot Randomized Controlled Trial. Front Psychiatry. 2021;12:625480.
Boß L, Lehr D, Reis D, Vis C, Riper H, Berking M, et al. Reliability and Validity of Assessing User Satisfaction With Web-Based Health Interventions. J Med Internet Res. 2016;18(8):e234.
Schmidt J, Lamprecht F, Wittmann WW. [Satisfaction with inpatient management. Development of a questionnaire and initial validity studies]. Psychother Psychosom Med Psychol. 1989;39(7):248–55.
Sabourin S, Gendreau P. Assessing Client Satisfaction with Mental Health Treatment among French-Canadians. Appl Psychol. 1988;37(4):327–35.
Kapp C, Perlini T, Baggio S, Stephan P, Urrego AR, Rengade CE, et al. [Psychometric properties of the Consumer Satisfaction Questionnaire (CSQ-8) and the Helping Alliance Questionnaire (HAQ)]. Sante Publique (Bucur). 2014;26(3):337–44.
Roberts RE, Attkisson CC. Assessing client satisfaction among Hispanics. Eval Program Plann. 1983;6(3–4):401–13.
Vázquez FL, Torres Á, Otero P, Blanco V, Clifford Attkisson C. Psychometric Properties of the Castilian Spanish Version of the Client Satisfaction Questionnaire (CSQ-8). Curr Psychol. 2019;38(3):829–35.
Kongsakon R, Jareonsettasin T. Reliability and validity of a new measure of patient satisfaction (CSQ-8) Thai version with psychiatric care. J Psychiatr Assoc Thailand. 2000;45(2):155–63.
Tachimori H, Ito H. Reliability and validity of the Japanese version of Client Satisfaction Questionnaire. Seishin Igaku (Clinical Psychiatry); 1999.
De Brey H. A cross-national validation of the Client Satisfaction Questionnaire: The Dutch experience. Eval Program Plann. 1983;6(3):395–400.
De Wilde EF, Hendriks VM. The Client Satisfaction Questionnaire: psychometric properties in a Dutch addict population. Eur Addict Res. 2005;11(4):157–62.
Matsubara C, Green J, Astorga LT, Daya EL, Jervoso HC, Gonzaga EM, et al. Reliability tests and validation tests of the client satisfaction questionnaire (CSQ-8) as an index of satisfaction with childbirth-related care among Filipino women. BMC Pregnancy Childbirth. 2013;13(1):235.
Kelly PJ, Kyngdon F, Ingram I, Deane FP, Baker AL, Osborne BA. The Client Satisfaction Questionnaire-8: Psychometric properties in a cross-sectional survey of people attending residential substance abuse treatment. Drug Alcohol Rev. 2018;37(1):79–86.
LeVois M, Nguyen TD, Attkisson CC. Artifact in client satisfaction assessment: experience in community mental health settings. Eval Program Plann. 1981;4(2):139–50.
Alfonsson S, Maathz P, Hursti T. Interformat Reliability of Digital Psychiatric Self-Report Questionnaires: A Systematic Review. J Med Internet Res. 2014;16(12):e268.
Lebow JL. Research assessing consumer satisfaction with mental health treatment: a review of findings. Eval Program Plann. 1983;6(3–4):211–36.
Spensley J, Edwards DW, White E. Patient satisfaction and involuntary treatment. Am J Orthopsychiatry. 1980;50(4):725–7.
Attkisson CC, Zwick R. The client satisfaction questionnaire. Eval Program Plann. 1982;5(3):233–7.
Dragesund T, Nilsen RM, Kvåle A. Norwegian Psychomotor Physiotherapy versus Cognitive Patient Education and active physiotherapy—A randomized controlled trial. Physiother Res Int. 2021;26(2):e1891.
Egeland KM, Ruud T, Ogden T, Färdig R, Lindstrøm JC, Heiervang KS. How to implement Illness Management and Recovery (IMR) in mental health service settings: evaluation of the implementation strategy. Int J Ment Health Syst. 2017;11:13.
Hansen B, Hagen K, Öst L-G, Solem S, Kvale G. The Bergen 4-Day OCD Treatment Delivered in a Group Setting: 12-Month Follow-Up. Front Psychol. 2018;9:639-.
Hansen B, Kvale G, Hagen K, Hjelle KM, Solem S, Bø B, et al. The Bergen 4-Day Treatment for Panic Disorder: A Pilot Study. Front Psychol. 2018;9:1044.
Havnen A, Hansen B, Öst L-G, Kvale G. Concentrated ERP delivered in a group setting: An effectiveness study. J Obsessive-Compulsive Relat Disorders. 2014;3(4):319–24.
Havnen A, Hansen B, Öst LG, Kvale G. Concentrated ERP Delivered in a Group Setting: A Replication Study. Behav Cogn Psychother. 2017;45(5):530–6.
Launes G, Hagen K, Sunde T, Öst LG, Klovning I, Laukvik IL, et al. A Randomized Controlled Trial of Concentrated ERP, Self-Help and Waiting List for Obsessive- Compulsive Disorder: The Bergen 4-Day Treatment. Front Psychol. 2019;10:2500.
Lofthus AM, Westerlund H, Bjørgen D, Lindstrøm JC, Lauveng A, Clausen H, et al. Are Users Satisfied with Assertive Community Treatment in Spite of Personal Restrictions? Community Ment Health J. 2016;52(8):891–7.
Skar-Fröding R, Clausen HK, Šaltytė Benth J, Ruud T, Slade M, Sverdvik Heiervang K. Relationship between satisfaction with mental health services, personal recovery and quality of life among service users with psychosis: a cross-sectional study. BMC Health Serv Res. 2021;21(1):439.
Stubhaug B, Lier HO, Aßmus J, Rongve A, Kvale G. A 4-Day Mindfulness-Based Cognitive Behavioral Intervention Program for CFS/ME. An Open Study, With 1-Year Follow-Up. Front Psychiatry. 2018;9:720.
Holgersen KH, Brønstad I, Jensen M, Brattland H, Reitan SK, Hassel AM, et al. A combined individual and group-based stabilization and skill training intervention versus treatment as usual for patients with long lasting posttraumatic reactions receiving outpatient treatment in specialized mental health care - a study protocol for a randomized controlled trial. Trials. 2020;21(1):432.
Kvale G, Frisk B, Jürgensen M, Børtveit T, Ødegaard-Olsen ØT, Wilhelmsen-Langeland A, et al. Evaluation of Novel Concentrated Interdisciplinary Group Rehabilitation for Patients With Chronic Illnesses: Protocol for a Nonrandomized Clinical Intervention Study. JMIR Res Protoc. 2021;10(10):e32216.
Mundal I, Gråwe RW, Hafstad H, De Las Cuevas C, Lara-Cabrera ML. Effects of a peer co-facilitated educational programme for parents of children with ADHD: a feasibility randomised controlled trial protocol. BMJ Open. 2020;10(12):e039852.
Vaag JR, Lara-Cabrera ML, Hjemdal O, Gjervan B, Torgersen T. Psychoeducational groups versus waitlist in treatment of attention-deficit hyperactivity/impulsivity disorder (ADHD) in adults: a protocol for a pilot randomized waitlist-controlled multicenter trial. Pilot Feasibility Stud. 2019;5:17.
Wolters LH, Weidle B, Babiano-Espinosa L, Skokauskas N. Feasibility, Acceptability, and Effectiveness of Enhanced Cognitive Behavioral Therapy (eCBT) for Children and Adolescents With Obsessive-Compulsive Disorder: Protocol for an Open Trial and Therapeutic Intervention. JMIR Res Protoc. 2020;9(12):e24057.
Attkisson CC, Greenfield TK. The UCSF Client Satisfaction Scales: I. The Client Satisfaction Questionnaire-8. 2004.
Löwe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122(1–2):86–95.
Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire JAMA. 1999;282(18):1737–44.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7.
Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42.
Prinsen CAC, Mokkink LB, Bouter LM, Alonso J, Patrick DL, de Vet HCW, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018;27(5):1147–57.
Cox GB, Brown TR, Peterson PD, Rowe MM. A report on a state-wide community mental health center outcome study. Community Ment Health J. 1982;18(2):135–50.
Soelling ME, Newell TG. Effects of anonymity and experimenter demand on client satisfaction with mental health services. Eval Program Plann. 1983;6(3):329–33.
Leonhard C, Gastfriend DR, Tuffy LJ, Neill J, Plough A. The effect of anonymous vs. nonanonymous rating conditions on patient satisfaction and motivation ratings in a population of substance abuse patients. Alcohol Clin Exp Res. 1997;21(4):627–30.
Moret L, Nguyen J-M, Pillet N, Falissard B, Lombrail P, Gasquet I. Improvement of psychometric properties of a scale measuring inpatient satisfaction with care: a better response rate and a reduction of the ceiling effect. BMC Health Serv Res. 2007;7(1):197.
Pedersen P, Lilleeng B. S, E. Distriktspsykiatriske tjenester – Driftsindikatorer for distriktspsykiatriske sentre 2017. Helsedirektoratet; 2019. IS-2825.
Acknowledgements
We would like to thank all the patients who have contributed to this study.
Funding
HP is supported by a PhD grant from the Central Norway Regional Health Authority (project no. 90822100). MLL-C received a postdoctoral grant (project no. 90327500, Central Norway Regional Health Authority). The founder had no role in the study design, decision to publish, or preparation of the manuscript.
Open access funding provided by Norwegian University of Science and Technology
Author information
Authors and Affiliations
Contributions
HP: Conceptualization, methodology, formal analysis, writing – original draft. AH: Data curation, writing – review & editing, supervision. MB: Resources, Writing - review & editing. CCA: Developed the questionnaire, writing – review & editing. MLL-C: Conceptualization, methodology, writing – review & editing, supervision. All the authors reviewed and confirmed the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to report.
Ethics approval and consent to participate
This research was approved by the Regional Committee for Medical Research and Ethics in Norway (REK 2019/31836) and the Norwegian Centre for Research Data (2019/605327) and done in accordance with their guidelines and regulations. Every participant provided informed consent digitally and was informed that participation was voluntary and that they could withdraw at any time without it affecting any other aspects of their treatment or resulting in any future consequences.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pedersen, H., Havnen, A., Brattmyr, M. et al. A digital Norwegian version of the client satisfaction questionnaire 8: factor validity and internal reliability in outpatient mental health care. BMC Psychiatry 22, 671 (2022). https://doi.org/10.1186/s12888-022-04281-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04281-8