
Abstract
Background
Bronchiolitis, a common lower respiratory tract infection in children under 2, is primarily caused by respiratory syncytial virus (RSV). During the coronavirus disease (COVID-19) pandemic, respiratory infections initially decreased due to non-pharmaceutical interventions; however, patients with bronchiolitis have surged in the post-pandemic period. This study examined the burden and severity of bronchiolitis in the post-COVID era in a tertiary center in Saudi Arabia.
Methods
This retrospective review was conducted on pediatric patients aged < 2 years who were diagnosed with bronchiolitis at a tertiary hospital in Riyadh between September 2021 and March 2024. The collected data included demographics, comorbidities, viral polymerase chain reaction results, clinical management, disposition, and outcomes. Statistical analysis was performed using SPSS, with statistical significance at p < 0.05.
Results
Out of 482 patients, 56% were male, with a mean age of 6.37 months. RSV was the most common virus (53.79%) among the 132 tested patients. Oxygen therapy was administered to 93.15% of patients, with only 4.36% requiring high-flow nasal cannula and 0.41% requiring intubation. Pediatric Intensive Care Unit admission was necessary for 5.6%, with most managed with non-invasive support. Complications were infrequent; only 4.77% developed pneumonia.
Conclusions
The findings reflect a significant increase in patients with bronchiolitis post-COVID, consistent with the global trends. Despite this increase, most patients required minimal intervention, aligning with pre-pandemic management practices. This study highlighted the post-pandemic resurgence of bronchiolitis. While the caseload has increased, outcomes remain favorable, reinforcing the importance of supportive care and judicious resource allocation during the bronchiolitis season.
Similar content being viewed by others

Background
Bronchiolitis is the most common lower respiratory tract infection in children under the age of 2 years, and it is defined as an acute inflammation of the bronchioles that is usually caused by a viral infection. This condition commonly affects children younger than 2 years, with peak incidence occurring between 1 and 6 months of age [1]. Bronchiolitis is a seasonal disease that typically appears as an epidemic during winter. Respiratory syncytial virus (RSV) is the most common organism responsible for approximately 70% of patients worldwide [1]. In 2015, an estimated 33.1 million RSV acute lower respiratory tract infection (LRTI) episodes occurred worldwide, leading to over 3.2 million hospital admissions and 59,600 (48,000–74,500) in-hospital deaths in children younger than 5 years [2]. During the coronavirus disease (COVID-19) pandemic, the nationwide lockdown in addition to the recommendations of the World Health Organization (WHO) and Center for Disease Control and Prevention (CDC) for isolation and non-pharmacological interventions (NPIs) such as mask use, social distancing, and contact precautions, including hand hygiene, led to a dramatic impact on the incidence of LRTIs including RSV. In Saudi Arabia, the prevalence of bronchiolitis in children is between 25% and 88%, with RSV accounting for 35–95% of the detected viruses [3,4,5,6,7]. Nevertheless, a significant drop in the rate of LRTI was observed in 2020 compared to previous years. Despite this, the decline in admission rates in patients with bronchiolitis was not statistically significant [3]. Changes in the epidemiological pattern were observed worldwide after COVID-19, guiding interventions for seasonal flu. While non-pharmaceutical interventions during the COVID-19 pandemic significantly reduced respiratory infections in children, the post-pandemic resurgence of bronchiolitis highlights the need for updated data on its burden and severity in pediatric populations. This study addresses this gap by analyzing the epidemiological trends, clinical management, and outcomes of bronchiolitis in children aged < 2 years in a tertiary care setting in Saudi Arabia.
Methods
This retrospective study was conducted in a tertiary hospital in Riyadh, Saudi Arabia. We reviewed the medical records of all pediatric patients aged < 2 years who presented to the emergency department (ED) and were diagnosed with bronchiolitis as the final diagnosis according to the International Classification of Diseases (ICD) 9 coding system. The diagnosis of bronchiolitis in our study population was primarily based on clinical evaluation and standardized coding criteria. Pediatric patients under 2 years of age who presented to the ED with an acute onset of cough, wheezing, tachypnea, and signs of respiratory distress were identified using the ICD-9 codes for bronchiolitis. In addition to the clinical features, supportive findings—such as evidence of hyperinflation or patchy atelectasis on chest imaging when available and the detection of a viral pathogen (most notably respiratory syncytial virus) via nasopharyngeal aspirate polymerase chain reaction—were considered for the diagnoses. We included the data from winter of every year between September 1 2021 until March, 31, 2024.
From the electronic medical records of each patient, the following data were collected: demographic variables (age, sex), clinical risk factors, and comorbidities (prematurity, chronic lung disease, bronchopulmonary dysplasia, asthma, atopy, congenital cardiac illness, and immunodeficiency), results of nasopharyngeal aspirate polymerase chain reaction panels (PCR) and COVID-19 if done, disposition status as admission or discharged, and if critical care or general ward admission needed, length of stay, treatment administered including nebulization, fluids, steroid or antibiotic), type of respiratory support (low flow, high flow, Non-invasive or invasive ventilation) and return visits after discharge. In the current study, low-flow oxygen therapy was defined as oxygen delivered via standard nasal cannula at flow rates ≤ 2 or < 4 L/min, without humidification which is sufficient for patients with mild hypoxemia (oxygen saturation below 92% on room air) and minimal breathing.
In contrast, High-flow nasal cannula (HFNC) is defined as heated and humidified oxygen delivered via a specialized system, typically initiated at ≥ 1–2 L/kg/min, capable of meeting or exceeding the patient’s inspiratory flow demands, improved oxygenation, and minimal breathing in patients with more severe respiratory distress [1, 18]. This study has been approved by the Institutional Research Ethics Committee number 23–390 in King Fahad Medical City in Riyadh, Kingdom of Saudi Arabia. The consent to participate was obtained from the parents or legal guardians.
Outcomes
The primary outcome measured was the frequency of hospitalizations due to bronchiolitis during winter, specifically from September 1 to March 31, 2021–2024. Secondary outcomes included the duration of in-hospital and pediatric intensive care (PICU) stay as well as the requirement for oxygen, non-invasive respiratory support (NIRS), or mechanical ventilation (MV). NIRS involves the application of low-flow oxygen therapy, non-rebreather mask, HFNC, or continuous positive airway pressure (CPAP). Data on the duration of each instance of respiratory support were collected. Virological results and the types of tests conducted, specifically for RSV and co-infections, were documented. We documented the distribution of hospitalizations across the winter seasons.
Statistical analysis
Continuous variables are expressed as means with standard deviations, whereas categorical variables are expressed as frequencies and percentages. Statistical comparisons between groups, such as RSV-positive versus non-RSV and PICU-admitted versus non-PICU patients, were conducted using the Chi-square test to identify the potential risk factors associated with illness severity. Statistical significance was set at p < 0.05. All statistical analyses were performed using SPSS software version 22 (IBM Corp., Armonk, NY, USA).
Results
Between September 1, 2021, and March 31, 2024, of each consecutive winter season, 482 patients presented to the ED with bronchiolitis. The mean age was 6.37 months (Standard deviation [SD] = 5.69), with 270 (56%) male and 212 (44%) female. Most patients were Saudi nationals (93.36%), and only 27 (5.6%) received prophylaxis against RSV. Among the 482 patients, 228 (47.3%) had comorbidities, such as congenital heart disease, chronic lung disease, neuromuscular disorder, gastroesophageal reflux disease, and prematurity. However, most of them did not have complications after the infection (92.7%). The remaining demographic and clinical characteristics of patients are represented in Table 1.
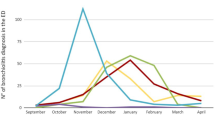
In winter (from January to March and from September to December), an increase in the number of bronchiolitis cases presenting to the ED was observed, from 59 patients in 2021 to 127 patients in 2022 and 180 patients in 2023, followed by 116 patients in 2024, as shown in Fig. 1.

Prevalence of ED presentation post-COVID-19 pandemic in winter months between 2021 and 2024. ED: emergency department; COVID-19: coronavirus disease
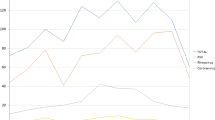
The most prevalent virus identified was RSV, observed in 71 of 132 screened patients (53.79%), followed by rhinovirus, which was present in 34 (25.76%) and metapneumovirus, detected in 7 (5.3%). Other viruses, such as Influenza, Enterovirus, Adenovirus, and Coronavirus, had a relatively lower prevalence, as shown in Fig. 2.

Prevalence of most common viruses identified post-COVID-19 pandemic in winter months between 2021 and 2024. COVID-19: coronavirus disease
Regarding management, the majority of the patients (449; 93.15%) required oxygen therapy upon arrival at the ED due to a lower to borderline oxygen saturation upon ED presentation, with a minority of patients requiring more intensive measures like high flow NC (n = 21, 4.36%) and intubation (n = 2, 0.41%). In the study, 230 patients (47.72%) received nebulization with salbutamol, whereas 181 (37.75%) received racemic epinephrine. Half of the patients (n = 243, 50.41%) received fluids, and 132 patients (25%) received antibiotics, which likely reflects physicians’ concerns about possible bacterial superinfection—especially in sicker or high-risk patients (Table 2). Of 482 patients, 27 (5.60%) required admission to the PICU. PICU admission was based on uniform hospital policy, which mandated intensive care for patients with severe respiratory distress, failure to maintain oxygen saturation above 92% despite supplemental oxygen, or those requiring advanced respiratory support such as HFNC, CPAP, or intubation. Among them, 21 patients (77.77%) received HFNC oxygen for an average of 96.38 h. CPAP was used for three patients (11.11%) for an average of 192 h, whereas intubation was needed for two patients (7.40%) (Tables 3 and 4). The presence of a positive viral screen and underlying comorbidities signifies the need for intensive care (P < 0.001). Admission to the PICU was significantly associated with developing complications such as pneumonia, refractory respiratory failure, and prolonged oxygen requirements (P 0.001) Table 3.
Most patients who were admitted to PICU with bronchiolitis had favorable outcomes without complications; the vast majority (n = 26, 56.4%) were discharged without sequelae, and only one death (2.1%) was reported. Complications, such as prolonged oxygen requirements post-discharge and pneumonia, were more prevalent in patients admitted to the PICU (Table 3). The average ED length of stay was 4.32 h, while admitted patients had an average stay of 111.53 h in the general ward and 100.3 in the PICU. The return visits to the ED were uncommon at approximately 46 patients (9.54%), mainly due to mild respiratory or febrile symptoms at an average of 41.46 h after discharge (Table 5). For palivizumab prophylaxis, no significant difference was observed in the type of oxygen therapy provided between those who received it and those who did not receive it for patients low-flow oxygen therapy and HFNC (χ² = 1.92, P = 0.997). No significant difference was observed in complications between those who received the palivizumab prophylaxis and those who did not (χ² = 5.52, P = 0.938). No significant association was observed between palivizumab prophylaxis status and disease severity, clinical outcomes, or treatment variables (P > 0.05) Table 6. Most patients with bronchiolitis who presented to the ED were discharged with a mean length of stay of 2.66 h (standard deviation: 2.14 h) if no treatment required. The shortest stay was 1 h, and the longest was 11 h.
The single mortality case involved a PICU-admitted patient who developed severe respiratory failure complicated by pneumonia, eventually resulting in refractory respiratory failure. Despite maximal supportive care, including high-flow nasal cannula and CPAP, the patient succumbed to the illness, underscoring the potential severity of bronchiolitis in a vulnerable subset of patients.
Discussion
Bronchiolitis is a common viral illness affecting infants under 2 years of age, with varying degrees of severity and complexity. Although the clinical management of bronchiolitis has evolved, it continues to be a significant public health concern owing to its seasonal variability and the recurrent pressure it places on healthcare systems, particularly during winter. In this study, we present our observation in a tertiary hospital in Riyadh, Saudi Arabia, following the COVID-19 pandemic. Our data reflect a marked increase in the incidence of bronchiolitis in the winter following the COVID-19 pandemic, with the number of patients nearly doubling each year. This is consistent with global reports indicating that the relaxation of NPIs and the re-establishment of typical post-pandemic social interactions have led to a resurgence of common respiratory viruses [6, 8,9,10,11,12]. The year 2020 witnessed a sharp decline in bronchiolitis cases globally, attributed to strict COVID-19 public health measures, including lockdowns, masking, and social distancing. These interventions significantly curtailed the transmission of respiratory viruses such as RSV. Our study, focusing on the period from 2021 onwards, observed a rebound effect likely driven by waning population-level immunity due to this ‘immunity debt,’ a concept well-documented in the literature [13].
Most infections occur in young infants with a median age of 6 months, which is not unexpected based on their risk of acquiring infection. During the pandemic, lockdowns and social distancing led to a significant reduction in viral transmission, including that of RSV and other respiratory pathogens. A study conducted by Alharbi et al. reported that pediatric viral infections in Saudi Arabia decreased by 50% during the initial lockdown phase in 2020. With the relaxation of restrictions in mid-2021, the “immunity debt” phenomenon may have played a role in the increased number of patients with bronchiolitis [3].
Internationally, the prevalence of bronchiolitis admission varies between pre- and post-COVID-19 pandemic, ranging from 25% pre-pandemic to 56% post-pandemic, with the lowest rate occurring during the peak of COVID-19 pandemic in 2020 [2,3,4]. During the peak of COVID-19 pandemic, strict public health measures (e.g., lockdowns, masking) led to significantly fewer viral exposures. Hence, fewer patients with severe bronchiolitis were admitted to the hospital, leading to a reduction in admission rates. After lifting the restrictions on COVID-19 in the mid-year of 2022, an early peak of bronchiolitis was observed starting in October, which gradually dropped in the following January, compared with previously observed seasonal patterns starting in May, peaking in November, and subsiding by February [2, 14]. Despite the increase in presenting patients, more than half of our population (57.05%) had been discharged from the ED without requiring admission after the initial intervention, compared to a 56% admission rate worldwide after the pandemic [15]. In Saudi Arabia, a study conducted at a tertiary hospital from January 2005 to December 2010 reported that the prevalence of respiratory viruses among 643 patients under 17 years was 48.1%. Among those, 287 patients were younger than 3 years old; RSV was the most commonly detected organism. (95.5%) Herein, we reported a positive virology test rate of 27.37%, with RSV making up 53.79% of the test results [4]. Other viruses documented are rhinovirus (25.76%), metapneumovirus (5.3%), and influenza. COVID-19 has not been documented or tested frequently following the resolution of restrictions and recommendations for isolation. In comparison, a study in Sidra Medicine in Qatar showed the prevalence of rhinovirus in the post-COVID era was 31.4%, while RSV was observed at 29.1% [12].
Traditionally, the management of bronchiolitis has been supportive, focusing on oxygen therapy and hydration to maintain respiratory and hemodynamic stability. However, despite international and national guidelines advocating for minimal medical intervention, we observed a relatively high use of bronchodilators (47.72% received salbutamol and 37.75% received racemic epinephrine) and antibiotics (25%); this is similar to a previous study where antibiotics were used in 45% of viral documented cases and steroids were used in 15%; similar discrepancy between guideline recommendations and actual clinical practice has been reported in multiple studies [1, 10, 16,17,18]. This variation of practice may be attributed to a lack of conclusive evidence supporting the efficacy of bronchodilators in treating bronchiolitis, as physicians may use these treatments to manage acute respiratory distress or in response to parental pressure. Despite the viral etiology of bronchiolitis, the use of antibiotics in 25% of our cohort raises concerns about potential antibiotic overuse, which could contribute to antimicrobial resistance. This is particularly relevant in patients where bacterial co-infection has not been confirmed. The clinical decision to administer antibiotics may have been influenced by factors such as the presence of comorbidities, severity of illness, and concerns about bacterial superinfection. Steroids were not recommended for bronchiolitis management, as the guidelines advise against their routine use in these patients. Strategies to reduce inappropriate steroid and antibiotic use include enhancing clinician education on current evidence-based guidelines, implementing antimicrobial stewardship programs with regular audits and feedback, and utilizing decision-support tools within electronic medical records to promote adherence to recommended treatment protocols.
We had 42.95% of the patients (207 out of 482) requiring admission, with 5.6% needing intensive care unit care. This is similar to the 6.3% reported by Bukhari et al. from 2005 to 2010. In comparison, Osman et al. reported a PICU admission rate of 16.06%, while Abushahin et al. documented a rate of 23.3% [4, 8, 12]. Among the infants who required admission, 37.35% were admitted to the general ward. Oxygen therapy was the cornerstone of treatment in our cohort, with 93.15% of patients receiving low-flow oxygen therapy upon presentation. HFNC oxygen therapy was administered to 4.36% of patients, a lower rate than reported in certain international studies, such as those conducted in Europe, where up to 18% of patients with bronchiolitis required HFNC [11]. The lower HFNC rate in our study may be attributed to early interventions and management strategies initiated in the ED, potentially reducing the need for more intensive oxygenation measures, as reported by Maya et al. [11]. Nevertheless, further research is warranted to explore the relationship between the early initiation of HFNC and patient outcomes, including the length of hospital stay and the need for escalation to invasive mechanical ventilation [11, 19].
The presence of comorbidities, such as congenital heart disease, chronic lung disease, and prematurity, was significantly associated with PICU admission and the development of complications, such as pneumonia and refractory respiratory failure. This is consistent with the findings of previous studies that identified these comorbidities as significant risk factors for severe bronchiolitis. In a retrospective study by Osman et al., 37% of infants admitted to the PICU were premature at birth, in addition to the presence of other comorbidities. The positivity of the viral nasopharyngeal aspirate, especially the presence of RSV, was not assessed at the time of admission to the PICU. As reported by Osaman et al., non-RSV viruses were more suggestive of a possible requirement for intensive care [8]. In another retrospective review of four hospitals in Italy, no specific risk factors correlated with the need for intensive care admission [3, 8]. Among the children admitted to the PICU, the majority required HFNC (77.77%), with a smaller percentage requiring CPAP (11.11%) or intubation (7.40%). The median duration of HFNC use was 96.38 h, whereas CPAP and intubation were used for 192 h and 48 h, respectively. Despite these interventions, only two patients required intubation, and one died, highlighting that the majority of the children with bronchiolitis experience favorable outcomes with appropriate supportive care. The analysis reported no significant differences in the severity of illness, reflected by oxygen requirements or complications, between patients who received prophylactic palivizumab and those who did not. This finding is different from the result of other studies that have proven the efficacy of palivizumab in preventing severe bronchiolitis necessitating PICU admission [8, 9]. However, the small number of vaccinated individuals in our study limits the power of this comparison and precludes definitive conclusions regarding the efficacy of RSV prophylaxis, in contrast to the findings reported in more extensive studies.
This study has multiple limitations, such as the retrospective design and reliance on electronic medical records, which may limit the completeness of the clinical and demographic data, potentially impacting the analysis. In addition, the absence of pre-pandemic data limits the direct comparison of trends over time. Finally, respiratory virus PCR testing was inconsistently performed, which may have influenced the assessment of viral prevalence and associated outcomes.
Conclusion
This study highlights a notable increase in patients with bronchiolitis in children under 2 years post-COVID-19, which is attributed to the relaxation of public health measures. Despite the increased caseload, the clinical management and outcomes largely mirrored pre-pandemic standards. Most patients were managed supportively, and a few required intensive intervention. These findings underscore the seasonal and recurrent nature of bronchiolitis, driven predominantly by RSV, and emphasize the ongoing implications for pediatric care in managing respiratory infections.
Data availability
Data that support the findings in the current study are available from the corresponding author on reasonable request.
Abbreviations
- RSV:
-
Respiratory syncytial virus
- COVID-19:
-
Coronavirus disease
- LRTI:
-
Lower respiratory tract infection
- WHO:
-
World health organization
- NPIs:
-
Non-pharmacological interventions
- ED:
-
Emergency department
- ICD:
-
International classification of diseases
- PCR:
-
Polymerase chain reaction
- HFNC:
-
High-flow nasal cannula
- PICU:
-
Pediatric intensive care
- NIRS:
-
Non-invasive respiratory support
- MV:
-
Mechanical ventilation
- CPAP:
-
Continuous positive airway pressure
References
Alharbi AS, Alqwaiee M, Al-Hindi MY, Mosalli R, Al-Shamrani A, Alharbi S, et al. Bronchiolitis in children: the Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Ann Thorac Med. 2018;13:127–43. https://doi.org/10.4103/atm.ATM_60_18.
Nair H, Nokes DJ, Gessner BD, Dherani M, Madhi SA, Singleton RJ, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. 2010;375:1545–55. https://doi.org/10.1016/S0140-6736(10)60206-1.
Alharbi NS, Alnasser Y, Alenizi AS, Alanazi AS, Alharbi AH, AlQurashi FO, et al. Did the national lockdown in Saudi Arabia reduce lower respiratory illnesses in children? Front Pediatr. 2021;9:717739. https://doi.org/10.3389/fped.2021.717739.
Bukhari EE, Elhazmi MM. Viral agents causing acute lower respiratory tract infections in hospitalized children at a tertiary care center in Saudi Arabia. Saudi Med J. 2013;34:1151–5.
Curatola A, Graglia B, Ferretti S, Covino M, Pansini V, Eftimiadi G, et al. The acute bronchiolitis rebound in children after COVID-19 restrictions: a retrospective, observational analysis. Acta Biomed. 2023;94:e2023031.
Ghirardo S, Ullmann N, Zago A, Ghezzi M, Minute M, Madini B, et al. Increased bronchiolitis burden and severity after the pandemic: a national multicentric study. Ital J Pediatr. 2024;50:25. https://doi.org/10.1186/s13052-024-01602-3.
Al-Majhdi FN, Al-Jaralla A, Elaeed M, Latif A, Gissmann L, Amer M. Prevalence of respiratory syncytial virus infection in Riyadh during the winter season 2007–2008 and different risk factors impact. Int J Virol. 2009;5:154–63.
Osman S, Alaa Adeen A, Hetta O, Alsiraihi A, Bader M, Aloufi A, et al. Epidemiology and risk factor analysis of children with bronchiolitis admitted to the intensive care unit at a tertiary care center in Saudi Arabia. Child (Basel). 2023;10:646. https://doi.org/10.3390/children10040646.
Mohammed MHA, Agouba R, Obaidy IE, Alhabshan F, Abu-Sulaiman R. Palivizumab prophylaxis against respiratory syncytial virus infection in patients younger than 2 years of age with congenital heart disease. Ann Saudi Med. 2021;41:31–5. https://doi.org/10.5144/0256-4947.2021.31.
Almadani A, Noël KC, Aljassim N, Maratta C, Tam I, Papenburg J, et al. Bronchiolitis management and unnecessary antibiotic use across 3 Canadian Picus. Hosp Pediatr. 2022;12:369–82. https://doi.org/10.1542/hpeds.2021-006274.
Maya M, Rameshkumar R, Selvan T, Delhikumar CG. High-flow nasal cannula versus nasal prong bubble continuous positive airway pressure in children with moderate to severe acute bronchiolitis: a randomized controlled trial. Pediatr Crit Care Med. 2024;25:748–57. https://doi.org/10.1097/PCC.0000000000003521.
Abushahin A, Toma H, Alnaimi A, Abu-Hasan M, Alneirab A, Alzoubi H, et al. Impact of COVID-19 pandemic restrictions and subsequent relaxation on the prevalence of respiratory virus hospitalizations in children. BMC Pediatr. 2024;24:91. https://doi.org/10.1186/s12887-024-04566-9.
Cohen R, Ashman M, Taha MK, et al. Pediatric infectious disease group (GPIP) position paper on the immune debt of the COVID-19 pandemic in childhood, how can we fill the immunity Gap? Infect Dis now. 2021;51(5):418–23. https://doi.org/10.1016/j.idnow.2021.05.004.
Al-Eyadhy A, Almazyad M, Hasan G, Almuhaideb Q, AbuDujain N, Alhaboob AAN, et al. The burden of viral infections in pediatric intensive care unit between endemic and pandemic coronavirus infections: a tertiary care center experience. J Infect Chemother. 2023;29:20–5. https://doi.org/10.1016/j.jiac.2022.09.007.
Camporesi A, Morello R, Ferro V, Pierantoni L, Rocca A, Lanari M, et al. Epidemiology, microbiology and severity of bronchiolitis in the first post-lockdown cold season in three different geographical areas in Italy: a prospective, observational study. Child (Basel). 2022;9:491. https://doi.org/10.3390/children9040491.
Alharbi AS, Al-Hindi MY, Alqwaiee M, Al-Shamrani A, Alharbi S, Yousef A, et al. Saudi initiative of bronchiolitis diagnosis, management, and prevention 2024 updated consensus on the prevention of respiratory syncytial virus. Ann Thorac Med. 2024;19:190–200. https://doi.org/10.4103/atm.atm_69_24.
Bronchiolitis in children: Diagnosis and management. London, National Institute for Health and Care Excellence (NICE).: 2021 Aug 9. (NICE Guideline, No. 9.). https://www.ncbi.nlm.nih.gov/books/NBK573086/.
Ralston SL, Lieberthal AS, Meissner HC, Alverson BK, Baley JE, Gadomski AM, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134:e1474–502–e1502. https://doi.org/10.1542/peds.2014-2742.
Habra B, Janahi IA, Dauleh H, Chandra P, Veten A. A comparison between high-flow nasal cannula and noninvasive ventilation in the management of infants and young children with acute bronchiolitis in the PICU. Pediatr Pulmonol. 2020;55:455–61. https://doi.org/10.1002/ppul.24553.
Acknowledgements
The authors would like to thank all participants who gave their time to help in collecting the data.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
R.A. conceptualized the study and led the project design and oversight. I.A. contributed to data collection and initial data analysis. A.A. assisted in refining the methodology and contributed significantly to manuscript preparation. W.A. participated in data analysis and interpretation. R.A.S. assisted with literature review and contributed to the editing and revision process. A.A.O. helped with data validation and visualization. D.S. contributed to drafting and revising the manuscript. Y.A. assisted in the final editing and formatting of the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the ethical principles outlined in the declaration of Helsinki. This study has been approved by the Institutional Research Ethics Committee number 23–390 in King Fahad Medical City in Riyadh, Kingdom of Saudi Arabia. The consent to participate was obtained from the parents or legal guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Alrashed, R., Almeshawi, I., Alshammari, A. et al. Burden of bronchiolitis post-COVID-19 pandemic in children less than 2 years old in 2021–2024: experience from a tertiary center in Saudi Arabia. BMC Pediatr 25, 453 (2025). https://doi.org/10.1186/s12887-025-05801-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1186/s12887-025-05801-7