
Abstract
Purpose
This study aims to analyze the clinical characteristics of Chinese children with spinal cord injury (SCI) without radiographic abnormality (SCIWORA) and explore their contributing factors and mechanisms of occurrence.
Methods
A retrospective analysis was conducted on the clinical data of pediatric patients diagnosed with SCIWORA from January 2005 to May 2020. Epidemiological, etiological, mechanistic, therapeutic, and outcome aspects were analyzed.
Results
A total of 47 patients with SCIWORA were included in this study, comprising 16 males and 31 females. The age range was 4 to 12 years, with an average age of 7.49 ± 2.04 years, and 70% of the patients were below eight. Sports-related injuries constituted 66%, with 70% attributed to dance backbend practice. Thoracic segment injuries accounted for 77%. In the American Spinal Injury Association (ASIA) classification, the combined proportion of A and B grades accounted for 88%. Conservative treatment was chosen by 98% of the patients, with muscle atrophy, spinal scoliosis, hip joint abnormalities, and urinary system infections being the most common complications.
Conclusion
SCIWORA in Chinese children is more prevalent in those under eight years old, with a higher incidence in females than males. Thoracic spinal cord injuries are predominant, dance backbend as a primary contributing factor, and the social environment of “neijuan” is a critical potential inducing factor. Furthermore, the initial severity of the injury plays a decisive role in determining the prognosis of SCIWORA.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Spinal Cord Injury (SCI) Without Radiographic Abnormality (SCIWORA), first described in 1974 [1], was subsequently defined by Pang and Wilberger in 1982 as “SCI without evidence of vertebral fracture or dislocation on X-ray and computed tomography (CT), excluding penetrating injuries, electrical injuries, birth trauma, and congenital spinal deformities [2].” SCIWORA accounts for 13–42% of all pediatric spinal cord injuries, posing a high risk of disability due to the lack of effective treatment methods [3, 4]. Children’s specific physiological and anatomical characteristics are considered the basis for SCIWORA. Compared to adults, children have a larger head-to-trunk ratio, relatively weaker neck muscles, vertically oriented vertebral bodies, and higher water content in intervertebral discs and vertebral rings. From an anatomical perspective, children are more prone to this specific type of SCI [3, 5, 6].
Many hospitals and institutions in Western countries have researched pediatric SCIWORA (PSCIWORA), summarizing their experiences in diagnosis, treatment, and outcomes [3, 5, 7, 8]. With China’s large population, the number of PSCIWORA patients is higher than in other regions. Unfortunately, there are few related research reports in China, and based on the cases we have encountered, the characteristics of Chinese patients differ from those reported in Western countries. Therefore, this retrospective case study aims to analyze and summarize the clinical features of PSCIWORA in China.
Methods
Patients
Clinical data of children diagnosed with SCIWORA admitted to our hospital from January 2005 to May 2020 was collected, including age, gender, cause of injury, location of injury, diagnostic imaging methods, treatment strategies, neurological function grading, and prognosis. Analysis was performed on the etiology, incubation period, diagnosis, lesion level, treatment, and outcomes. Inclusion criteria: (1) Age < 18 years; (2) Clinical symptoms and signs of SCI; (3) There is no evidence of spinal column fracture or dislocation on X-ray and CT. Exclusion criteria: (1) penetrating injuries, electrical injuries, or birth trauma; (2) history of neurological or psychiatric diseases; (3) concurrent traumatic brain injury; (4) congenital spinal deformities. This retrospective study followed institutional and national research committee ethics, and approval was obtained from the ethics committee (Ethics No. Fast 23,805).It also has been registered in the Clinical Trial Registry, retrospectively registered.
Diagnosis
Upon emergency admission, all patients underwent a neurological examination to assess their motor and sensory functions. The American Spinal Injury Association (ASIA) classification evaluated the neurological status. X-rays and CT were used to assess fractures, subluxations, dislocations, deformities, and soft tissue injuries. Conventional magnetic resonance imaging (MRI) was further employed to assess spinal cord and soft tissue injuries. Further evaluation was conducted for patients with neurological symptoms and negative findings on routine MRI using MR diffusion tensor imaging (DTI).
Treatment
Patients diagnosed with SCIWORA were typically advised bed rest and immobilization. They may be required to wear appropriate braces to maintain spinal stability and prevent secondary injuries. Additionally, bed rehabilitation training includes turning, resetting, massage, and exercise therapy. Catheterization was performed for patients with urinary retention. For patients with clinical symptoms within three days, methylprednisolone or dexamethasone is typically administered for shock treatment. Mannitol was used to eliminate spinal cord and soft tissue edema. Additionally, neurotrophic drugs such as mecobalamin and ganglioside were added for auxiliary treatment. Vasodilators were administered to improve spinal cord blood microcirculation after ruling out hemorrhagic diseases. Patients were generally advised to undergo neurorehabilitation treatment and hyperbaric oxygen therapy in a rehabilitation hospital once their condition stabilized.
Statistical analysis
Utilize the Statistical Package for the Social Sciences (SPSS) version 24.0 (IBM, Armonk, New York, USA) and Microsoft Excel (Microsoft Corporation, Redmond, Washington, USA) to manage and analyze data. Calculate descriptive statistics for SCIWORA patients, primarily employing frequency analysis. Individual characteristics were described as numerical values or mean ± standard deviation.
Results
Epidemiology
A total of 47 cases of PSCIWORA were collected, with 16 males and 31 females, resulting in a male-to-female ratio close to 1:2. The average age was 7.49 ± 2.04 years, and the majority were under eight years old, accounting for 70% (Table 1).
Etiology of injury
Sports-related trauma accounted for the majority of injuries (66%), with traffic accidents being the second most common cause (19%). Violence, falls, and other causes accounted for 9%, 4%, and 2% of injuries, respectively. Dance backbend practices accounted for 71% of all sports-related injuries (Table 2).
Location of injury
Through routine MRI examinations, injury sites were identified in 91% of patients. In a small subset of patients with negative findings on conventional MRI, DTI revealed the disruption of nerve fibers (Figs. 1 and 2). The majority of spinal cord injuries involved the thoracic segment, with proportions of 13%, 47%, and 17% for the cervical-thoracic, thoracic, and thoracolumbar regions, respectively. 19% of spinal cord injuries were cervical, while 4% were lumbar. (Table 2).

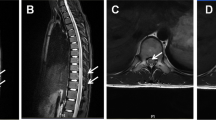
A 10-year-old female patient presented with paralysis after dance backbend practice. X-ray (A, B) and CT (C) scans did not detect any fractures or dislocations. No abnormmality was found on T1-weighted MRI (D), T2-weighted MRI (E) showed localized spinal cord thinning at the T10-12 vertebral level. DTI fiber reconstruction images (F) revealed local fiber areas and thinning of fiber bundles

An 8-year-old female patient presented with paralysis after dance backbend practice. X-ray (A, B) and CT (C) scans did not detect any fractures or dislocations. MRI (D, E) examination also showed no apparent abnormalities. However, DTI fiber reconstruction images (F) revealed localized thinning, fracture, and sparse fibers below the ninth thoracic vertebra
Treatment and outcome
Most patients exhibited severe neurological dysfunction immediately after injury, with 28 cases of ASIA classified as grade A and 13 cases as grade B, accounting for a total proportion of 88% (Table 3). Most patients (98%) opted for conservative treatment due to the inability to identify specific spinal cord compressions. At the last follow-up, only one case of grade D improved to normal after surgical treatment, while the others still had neurological dysfunction. Three cases improved from grade A to B, one case improved from grade A to C, four cases improved from grade B to C, and two cases improved from grade C to D (Table 3). Various complications were observed in the follow-up, with muscle atrophy, spinal scoliosis, hip joint abnormalities, and urinary system infections being the most common. Some patients developed complications such as pressure sores, dermatitis, urethral stones, renal pelvis dilation, and brittle bone fractures due to poor care (Table 1).
Discussion
SCIWORA is a term commonly used to describe a specific type of pediatric SCI, with 90% of SCIWORA cases occurring in children [4]. During childhood, a particular physiological developmental stage, a combination of a relatively larger head, shallow-angled small joints, lax ligaments, and immature Luschka joints, results in toddlers having a hypermobile spine with a pivot point for movement different from that of adults. The range of motion in the spine is significantly greater than that of spinal cord activity [7]. When the body undergoes excessive flexion or extension along the longitudinal axis, the spinal cord and meninges cannot adapt to the substantial elastic changes in the spine, leading to traction or compression injuries to the spinal cord. Additionally, In children under eight, the sagittal and transverse diameters of the spinal canal are narrowest at the level of T4–9, the anastomosis between the extraspinal and intraspinal arteries is minimal, making the spinal cord vulnerable to even slight traction or flexion, which can result in ischemic necrosis [9]. As age increases, spinal stability improves, enhancing tolerance to low-energy injuries [10]. Therefore, SCIWORA is more prevalent in children under eight years old, consistent with our epidemiological observations.
Research has indicated that due to the instability of the cervical spine in young children, pediatric SCIWORA often occurs in the cervical region, primarily manifesting as incomplete SCI [11]. Dynamic imaging studies have shown that the pivot point of the cervical spine in maximal flexion shifts from C2-C3 in infants and toddlers to C3-C4 at 5–6 years old, reaching C5–C6 in adulthood [12]. Consequently, in children under eight years old, injuries are more likely to occur in the upper cervical segments. However, beyond the age of 8, the anatomical structure of the pediatric cervical spine approaches that of adults, with increased stability in the upper cervical spine and a subsequent rise in the incidence of injuries to the lower cervical spine. These findings suggest that the upper cervical segments have the greatest physiological mobility during infancy and early childhood but are also the most susceptible to flexion injuries [9]. Surprisingly, the thoracic spine was predominant in our study and most of the patients presented with complete spinal cord injuries. These discrepancies may be attributed to differences in the patients’ mechanisms and causes of injuries. According to previous reports, the top three causes of pediatric traumatic spinal cord injuries in regions such as East Asia, North America, and Oceania are traffic accidents (46–74%), falls from heights (12–35%), and sports and entertainment activities (10–25%) [13]. Traffic accidents are often associated with whiplash injuries, with the cervical spine being the most commonly affected area [14]. However, in our study, the primary cause of injuries was sports-related (66%), with 71% of sports-related injuries occurring in the lower back. According to Wang et al.‘s study [15], there are similar discrepancies between Chinese and foreign studies, but they did not explore the potential causes of these differences. We believe that the societal phenomenon of “Neijuan” in Chinese society may contribute to this variability.
“Neijuan” is a popular Chinese internet term that refers to the phenomenon where individuals excessively strive for success in an intensely competitive social environment, leading to an unhealthy competitive atmosphere and social phenomenon. This phenomenon is prevalent in China. Influenced by prolonged exposure to this unhealthy competitive atmosphere, parents project their societal anxiety onto the care of the next generation, often articulated as “Do not let the children fall behind at the starting line.” Consequently, Chinese children have to face numerous additional extracurricular classes, and dance is one of the primary choices. The foundational elements of dance focus on enhancing muscle flexibility, with bending at the waist a crucial movement. Due to the developmental stage of a child’s spine, characterized by a lax and unstable anatomical structure, the spine’s adaptability is greater than that of the spinal cord [10]. When a child bends at the waist, most stress concentrates on the mid-thoracic vertebrae, leading to extreme thoracic spine extension [16]. Nevertheless, the cervical vertebrae, lumbar vertebrae, medulla oblongata, and conus cauda equina are relatively fixed in position. Passive stretching of the anterior longitudinal ligament and the protrusion of the wrinkled yellow ligament into the vertebral canal further reduce the reserve space within the vertebral canal [16]. When the stress level reaches a certain level, the facet joints may immediately experience horizontal sliding or vertebral dislocation. This puts the spinal cord under a huge amount of stress at once, which can cause both transverse and complete spinal cord injuries [8]. Simultaneously, due to poor blood supply to the spinal cord in the T2 to T4 segments, the incidence of thoracic segment SCIWORA is relatively high. Some also believe that it may be related to fibrocartilaginous embolism [17]. Bending at the waist can damage the intervertebral discs and the blood vessels still present in the intervertebral discs of young children, causing mucoid fibrous cartilaginous emboli to enter the central artery of the spinal cord, leading to spinal cord ischemia.
The primary manifestations of PSCIWORA injuries include spinal cord contusion, compression, and traction. Early identification of these injuries is crucial for prompt treatment and minimizing the degree of neurological deficit. Traditional radiological examinations, including X-ray and CT scans, are necessary for appropriately assessing the extent and precise location of the injury. However, the challenge arises when X-ray and CT imaging results are negative and biochemical tests such as cerebrospinal fluid analysis and blood routine show no positive findings, making the accurate diagnosis of SCIWORA challenging [18]. The application of MRI provides extensive information on neural and soft tissue injuries [19]. In cases of SCI, MRI can reveal bleeding, ischemia, or swelling with high-intensity signals on T2-weighted images [20, 21]. Despite the powerful capability of MRI in detecting soft tissue injuries, some spinal cord injuries remain undetectable through conventional MRI scans. In our study, most patients’ injuries were precisely located through routine MRI. In contrast, four patients showed no abnormalities on magnetic resonance but were diagnosed through further diffusion tensor imaging (DTI). DTI is a technique based on diffusion-weighted imaging (DWI) that applies a gradient field with 6–55 nonlinear directions to obtain a diffusion tensor image, quantitatively depicting the three-dimensional trajectory of water molecule diffusion in space [22]. The structural morphology of nerve fiber bundles can be visualized through DTI reconstruction and post-processing fiber tracking (FT) techniques. Currently, DTI and FT technologies are widely used in the nervous system. Studies have shown that some patients without conventional MRI abnormalities were found to have high-density signal abnormalities using DTI examinations [23, 24]. In this study, using DTI technology, we saw fiber discontinuity in the spinal cord of four patients whose regular MRI results were negative. This helped us figure out where the injury was. Therefore, for SCIWORA patients exhibiting persistent neurological symptoms without MRI abnormalities, we recommend utilizing DTI examinations to enhance MRI diagnostic sensitivity and explore potential subtle spinal cord injuries.
Given the absence of evident signs of spinal trauma, such as fractures and dislocations, in SCIWORA patients, conservative treatment is the primary therapeutic approach [25]. Conservative treatment involves strict bed rest, immobilization, early administration of high-dose methylprednisolone, dehydration agents, neurotrophic drugs, and hyperbaric oxygen therapy [10]. The primary goal is to protect the remaining gray matter function of the spinal cord and prevent white matter necrosis, maximizing the recovery of spinal cord function. Vasoconstriction and ischemia of spinal cord vessels are the main contributors to PSCIWORA [26]. Consequently, pharmacological interventions should prioritize drugs that alleviate vascular spasms, dilate blood vessels, prevent microthrombus formation, and increase spinal cord blood flow. Dehydration, steroids, and neurotrophic drugs are also part of the treatment regimen. Although a guideline from 2002 recommended a 24-hour course of steroid pulse therapy within 8 h of SCI, there is still controversy surrounding its efficacy [27]. In our study, most PSCIWORA patients showed signs of neurological dysfunction within one hour of injury. Although steroid pulse therapy was administered, only a tiny fraction exhibited improved neurological function, with most patients showing no change in function before and after treatment. Consequently, considering the critical evaluation of the effectiveness and safety of steroid treatment and the existing guidelines, clinicians should exercise caution when considering steroid pulse therapy in the treatment of spinal cord injuries. Moreover, research indicates that early combined hyperbaric oxygen therapy can effectively alleviate spinal cord edema, increase oxygen pressure and blood oxygen content, enhance blood oxygen diffusion radius, improve the ischemic and hypoxic states of the spinal cord, reduce neuronal apoptosis, promote nerve regeneration and repair [28, 29]. In our study, all patients were recommended for subsequent hyperbaric oxygen therapy, but the neurological recovery outcomes were minimal. This may be correlated with the initial state of neurological damage, as most patients in our study presented with initial neurological function in ASIA grades A and B. Therefore, it is crucial to recognize the determining role of the initial injury severity in treatment outcomes and prognosis [10].
The complexity of treating neural injuries results in a less favorable prognosis for a considerable portion of individuals with SCIWORA, which subsequently leads to the manifestation of diverse long-term consequences. Our study found that musculoskeletal and urinary system difficulties were the prevailing issues in PSCIWORA, which aligns with prior findings [30]. Neural dysfunction leads to limited movement of the limbs, which causes muscles to undergo disuse atrophy. Moreover, spinal cord injuries impact the growth and maturation of the skeletal system, and prolonged periods of lying down or sitting in patients can lead to scoliosis and abnormal development of the hip joints [31]. Enhancing rehabilitation training, engaging in passive muscle exercises, and maintaining appropriate posture are effective methods for preventing spine curvature and improper hip joint development. Spinal cord damage frequently leads to impaired urine function, necessitating extended use of catheters and heightening susceptibility to urinary tract infections and bladder stones [32]. Early implementation of intermittent catheterization is a dependable approach for reducing difficulties in the urinary system. Timely, comprehensive rehabilitation treatment can significantly reduce the disability rate of PSCIWORA, promote functional recovery, and improve the quality of life [30].
Limitation
This study has several limitations. Firstly, PSCIWORA is uncommon, and China lacks a systematic nationwide medical record database. As a result, the number of cases collected in this study is relatively small, and it is a single-center study, potentially introducing bias. Secondly, there needs to be more comparative studies with other types of spinal cord injuries, preventing a complete elucidation of the unique characteristics of SCIWORA. Therefore, subsequent multicenter studies with a larger sample size and a case-control design are needed to address these limitations.
Conclusion
SCIWORA in Chinese children is more prevalent in those under eight years old, with a higher incidence in females than males. Thoracic spinal cord injuries are predominant, dance backbend as a primary contributing factor, and the social environment of “neijuan” is a critical potential inducing factor. Furthermore, the initial severity of the injury plays a decisive role in determining the prognosis of SCIWORA.
Data availability
The dataset analyzed during the current study is not publicly available but can be obtained from the corresponding author upon reasonable request.
Abbreviations
- ASIA:
-
American Spinal Injury Association
- CT:
-
Computed tomography
- DTI:
-
diffusion tensor imaging
- DWI:
-
Diffusion-weighted imaging
- FT:
-
Fiber tracking
- MRI:
-
Magnetic resonance imaging
- PSCIWORA:
-
Pediatric spinal cord injury without radiological abnormality
- SCI:
-
Spinal cord injury
- SCIWORA:
-
Spinal cord injury without radiological abnormality
References
Burke DC. Traumatic spinal paralysis in children. Paraplegia. 1974;11(4):268–76. https://doi.org/10.1038/sc.1973.39.
Pang D, Wilberger JJ. Spinal cord injury without radiographic abnormalities in children. J Neurosurg. 1982;57(1):114–29. https://doi.org/10.3171/jns.1982.57.1.0114.
Brauge D, Plas B, Vinchon M, Charni S, Di Rocco F, Sacko O, Mrozek S, Sales De Gauzy J. Multicenter study of 37 pediatric patients with SCIWORA or other spinal cord injury without associated bone lesion. Orthop Traumatol Surg Res. 2020;106(1):167–71. https://doi.org/10.1016/j.otsr.2019.10.006.
Launay F, Leet AI, Sponseller. PD(2005)Pediatric spinal cord injury without radiographic abnormality: a meta-analysis. Clin Orthop Relat R (433): 166.
Konovalov N, Peev N, Zileli M, Sharif S, Kaprovoy S, Timonin S. Pediatric Cervical Spine injuries and SCIWORA: WFNS Spine Committee Recommendations. Neurospine. 2020;17(4):797–808. https://doi.org/10.14245/ns.2040404.202.
McAllister AS, Nagaraj U, Radhakrishnan R. (2019)Emergent Imaging of Pediatric Cervical Spine Trauma. Radiographics 39(4): 1126–42. https://doi.org/10.1148/rg.2019180100.
Farrell CA, Hannon M, Lee LK. Pediatric spinal cord injury without radiographic abnormality in the era of advanced imaging. Curr Opin Pediatr. 2017;29(3):286–90. https://doi.org/10.1097/MOP.0000000000000481.
Carroll T, Smith CD, Liu X, Bonaventura B, Mann N, Liu J, Ebraheim. NA(2015)spinal cord injuries without radiologic abnormality in children: a systematic review. Spinal Cord 53(12): 842–8. https://doi.org/10.1038/sc.2015.110.
Dommisse GF. The arteries, arterioles, and capillaries of the spinal cord. Surgical guidelines in the prevention of postoperative paraplegia. Ann Roy Coll Surg. 1980;62(5):369–76.
Pang D. Spinal cord injury without radiographic abnormality in children, 2 decades later. Neurosurgery. 2004;55(6):1325–42. https://doi.org/10.1227/01.neu.0000143030.85589.e6.
Copley PC, Copley PC, Tilliridou V, Tilliridou V, Kirby A, Kirby A, Jones J, Jones J, Kandasamy J, Kandasamy. J(2019)management of cervical spine trauma in children. Eur J Trauma Emerg Surg (Munich: 2007) 45(5): 777–89. https://doi.org/10.1007/s00068-018-0992-x.
Fehlings MG, Wilson JR, Harrop JS, Kwon BK, Tetreault LA, Arnold PM, Singh JM, Hawryluk G, Dettori JR. Efficacy and Safety of Methylprednisolone Sodium Succinate in Acute spinal cord Injury: a systematic review. Glob Spine J. 2017;7(3 Suppl):S116–37. https://doi.org/10.1177/2192568217706366.
New PW, Lee BB, Cripps R, Vogel LC, Scheinberg A, Waugh. MC(2019)global mapping for the epidemiology of paediatric spinal cord damage: towards a living data repository. Spinal Cord 57(3): 183–97. https://doi.org/10.1038/s41393-018-0209-5.
Lee SH, Park HJ, Kim HT, Park SY, Heo I, Hwang EH, Shin BC, Hwang. MS(2021)efficacy of acupuncture for whiplash injury: a protocol for systematic review and meta-analysis. Medicine 100(49): e27767. https://doi.org/10.1097/MD.0000000000027767.
Wang Y, Zeng L, Huang G, Guo X. Letter to the editor: Pediatric spinal cord Injury without Radiographic abnormality: the Beijing experience. Spine. 2021;46(22):E1225. https://doi.org/10.1097/BRS.0000000000004210.
Ren J, Zeng G, Ma YJ, Chen N, Chen Z, Ling F, Zhang. HQ(2017)Pediatric thoracic SCIWORA after back bend during dance practice: a retrospective case series and analysis of trauma mechanisms. Child Nerv Syst 33(7): 1191–8. https://doi.org/10.1007/s00381-017-3407-0.
Fedaravicius A, Feinstein Y, Lazar I, Gidon M, Shelef I, Avraham E, Tamasauskas A, Melamed I. Successful management of spinal cord ischemia in a pediatric patient with fibrocartilaginous embolism: illustrative case. J Neurosurg Case Lessons. 2021;2(11):CASE21380. https://doi.org/10.3171/CASE21380.
Stroman PW, Wheeler-Kingshott C, Bacon M, Schwab JM, Bosma R, Brooks J, Cadotte D, Carlstedt T, Ciccarelli O, Cohen-Adad J, Curt A, Evangelou N, Fehlings MG, Filippi M, Kelley BJ, Kollias S, Mackay A, Porro CA, Smith S, Strittmatter SM, Summers P. Tracey I(2014)the current state-of-the-art of spinal cord imaging: methods. NeuroImage 84: 1070–81. https://doi.org/10.1016/j.neuroimage.2013.04.124.
Freigang V, Butz K, Seebauer CT, Karnosky J, Lang S, Alt V, Baumann F. Management and Mid-term Outcome after Real SCIWORA in Children and adolescents. Glob Spine J. 2022;12(6):1208–13. https://doi.org/10.1177/2192568220979131.
Canosa-Hermida E, Mora-Boga R, Cabrera- Sarmiento JJ, Ferreiro-Velasco ME, Salvador-de La Barrera S, Rodríguez-Sotillo A, Montoto-Marqués. A(2019)epidemiology of traumatic spinal cord injury in childhood and adolescence in Galicia, Spain: report of the last 26-years. J Spinal Cord Med 42(4): 423–9. https://doi.org/10.1080/10790268.2017.1389836.
Talbott JFMP, Huie JRP, Ferguson ARP, Bresnahan JCP, Beattie MSP, Dhall. SSM(2018)MR Imaging for Assessing Injury Severity and Prognosis in Acute traumatic spinal cord Injury. Radiologic Clin North Am 57(2): 319–39. https://doi.org/10.1016/j.rcl.2018.09.004.
Jones DK, Griffin LD, Alexander DC, Catani M, Horsfield MA, Howard R, Williams. SC(2002)spatial normalization and averaging of diffusion tensor MRI data sets. NeuroImage 17(2): 592–617.
Mulcahey MJ, Samdani AF, Gaughan JP, Barakat N, Faro S, Shah P, Betz RR. Mohamed FB(2013)diagnostic accuracy of diffusion tensor imaging for pediatric cervical spinal cord injury. Spinal Cord 51(7): 532–7. https://doi.org/10.1038/sc.2013.36.
Alizadeh M, Fisher J, Saksena S, Sultan Y, Conklin CJ, Middleton DM, Krisa L, Finsterbusch J, Flanders AE, Faro SH, Mulcahey MJ. Mohamed FB(2018)age related diffusion and tractography changes in typically developing pediatric cervical and thoracic spinal cord. Neuroimage-Clin 18: 784–92. https://doi.org/10.1016/j.nicl.2018.03.014.
Atesok K, Tanaka N, O’Brien A, Robinson Y, Pang D, Deinlein D, Manoharan SR, Pittman J, Theiss S. (2018)posttraumatic spinal cord Injury without Radiographic Abnormality. Adv Orthop. 2018;7060654. https://doi.org/10.1155/2018/7060654.
Molinares DM, Gater DR, Daniel S, Pontee NL. (2022)nontraumatic spinal cord Injury: Epidemiology, etiology and management. J Pers Med 12(11) https://doi.org/10.3390/jpm12111872.
Hadley MN, Walters BC, Grabb PA, Oyesiku NM, Przybylski GJ, Resnick DK, Ryken. TC(2002)pharmacological therapy after acute cervical spinal cord injury. Neurosurgery 50(3 Suppl): S63–72. https://doi.org/10.1097/00006123-200203001-00013.
Turner S, Sunshine MD, Chandran V, Smuder AJ, Fuller. DD(2022)hyperbaric oxygen therapy after mid-cervical spinal contusion Injury. J Neurotraum 39(9–10): 715–23. https://doi.org/10.1089/neu.2021.0412.
Harch PG. Hyperbaric oxygen in chronic traumatic brain injury: oxygen, pressure, and gene therapy. Med Gas Res. 2015;5:9. https://doi.org/10.1186/s13618-015-0030-6.
Erden E. Evaluation of clinical characteristics and Comorbid conditions in Pediatric traumatic spinal cord Injury patients. Cureus J Med Sci. 2023;15(9):e44512. https://doi.org/10.7759/cureus.44512.
Rhee I, Do WS, Park KB, Park BK. Kim HW(2021)hip-Spine syndrome in patients with spinal cord injuries: Hyperlordosis Associated with severe hip flexion contracture. Front Pediatr 9: 646107. https://doi.org/10.3389/fped.2021.646107.
Chen YC, Ou YC, Hu JC, Yang MH, Lin WY, Huang SW, Lin WY, Lin CC, Lin VC, Chuang YC. Kuo HC(2022)bladder management strategies for Urological complications in patients with chronic spinal cord Injury. J Clin Med 11(22) https://doi.org/10.3390/jcm11226850.
Funding
This study was funded by the Science and Technology Leading Talent Project of Hunan Science and Technology Innovation Talent Plan in 2021 (No. 2021RC4057), and the Hunan Graduate Innovation Project in 2022 (No. 2022ZZTS0263).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Renfeng Liu, Qizhi Fan, Jingpeng He, Xin Wu, and Zuyun Yan. Renfeng Liu wrote the first draft of the manuscript. Wei Tan, Weiguo Wang, Zhiyue Li, and Youwen Deng participated in study design, evaluation of radiological data, and critically reviewed the initial and the revised draft of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Acknowledgment.
Consent for publication
Not applicable.
Ethics approval
This retrospective study followed institutional and national research committee ethics. The Xiangya Third Hospital, Central South University Ethics Committee accepted this study (Ethics No. Fast 23749).
Informed consent
A retrospective study, The Xiangya Third Hospital, Central South University Ethics Committee exempted informed consent.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, R., Fan, Q., He, J. et al. Clinical characteristics analysis of pediatric spinal cord injury without radiological abnormality in China: a retrospective study. BMC Pediatr 24, 236 (2024). https://doi.org/10.1186/s12887-024-04716-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04716-z