
Abstract
Background
Antibiotic prescription for respiratory tract infections (RTIs) in children attending primary care centres is almost double that predicted according to bacterial prevalence. Delayed antibiotic prescription (DAP) is designed to deploy a more rational use of antibiotics. While studies have evaluated DAP efficacy and safety for children with RTIs, little research has been conducted on the economic implications.
Methods
Our trial compared cost-effectiveness for DAP, immediate antibiotic prescription (IAP), and no antibiotic prescription (NAP) for children aged 2–14 years with acute uncomplicated RTIs attended to in 39 primary care centres in Spain. The main outcome was the incremental cost-effectiveness ratio (ICER), measured in euros per gained quality-adjusted life days (QALDs). Net monetary benefit (NMB) was also calculated as a tool for decision making. The analysis was performed from a societal perspective for a time horizon of 30 days, and included healthcare direct costs, non-healthcare direct and indirect costs, and the antimicrobial resistance (AMR) cost.
Results
DAP was the most cost-effective strategy, even when the cost of AMR was included. QALD values for the three strategies were very similar. IAP compared to DAP was more costly (109.68 vs 100.90 euros) and similarly effective (27.88 vs 27.94 QALDs). DAP compared to NAP was more costly (100.90 vs 97.48 euros) and more effective (27.94 vs. 27.82 QALDs). The ICER for DAP compared to NAP was 28.84 euros per QALD. The deterministic sensitivity analysis indicated that non-healthcare indirect costs had the greatest impact on the ICER. The cost-effectiveness acceptability curve showed that DAP was the preferred option in approximately 81.75% of Monte Carlo iterations, assuming a willingness-to-pay value of 82.2 euros per gained QALD.
Conclusions
When clinicians are in doubt about whether an antibiotic is needed for children with RTIs attending PC centres, those treated with the DAP strategy will have slightly better efficiency outcomes than those treated with IAP because its costs are lower than those of IAP. DAP is also the most cost-effective strategy over a time horizon of 30 days if AMR is considered, despite higher short-term costs than NAP. However, if in the long term the costs of AMR are larger than estimated, NAP could also be an alternative strategy.
Trial registration
This trial has been registered at www.clinicaltrials.gov (identifier NCT01800747; Date: 28/02/2013 (retrospectively registered).
Similar content being viewed by others


Background
One of the most frequent reasons for antibiotic prescription to children in primary care (PC) is a respiratory tract infection (RTI), [1] representing a significant economic burden for the health system [2]. The rate of outpatient antibiotic prescription for RTIs in children is high, [3,4,5] at almost double the rate predicted according to bacterial prevalence [3]. Most RTIs have a viral aetiology and are self-limiting, but antibiotics are indicated if a bacterial infection is suspected. Antibiotic prescription is typically associated with cases of diagnostic uncertainty [6,7,8] but is also the outcome of other factors, such as patient pressure for antibiotic prescription [9, 10]. Antibiotic prescription increases belief in efficacy and the demand for new consultations, [11, 12] although antibiotics are the most frequent cause of adverse effects in children, e.g., gastrointestinal and skin problems [13].
Over the long term, overuse of antibiotics is associated with bacterial resistance, [14] and reducing this resistance is a major global public health challenge [15]. According to the European Centre for Disease Prevention and Control (ECDPC), antimicrobial resistance (AMR) is responsible for approximately 33 110 deaths and 874 541 disability-adjusted life-years in the European Union/European Economic Area (EU/EEA) [16]. While this impact is recognized, relatively few countries have specific actions in place to reduce antibiotic intake.
Delayed antibiotic prescription (DAP) for RTIs, a strategy designed to foster more rational use of antibiotics, is recommended by clinical practice guidelines when there is uncertainty regarding immediate antibiotic prescription (IAP) [17, 18]. DAP is defined as a prescription issued for an antibiotic to be taken only if the condition has not improved or has worsened some days after the visit. A recent individual-patient-data meta-analysis comparing DAP, IAP, and no antibiotic prescription (NAP) reported that RTI symptom severity was similar for DAP and IAP, symptom duration was around the same for DAP and NAP and slightly shorter for IAP, re-consultations and complication rates were lower for DAP versus NAP, and patient satisfaction was higher for DAP [19].
While several randomized clinical trials (RCTs) have evaluated the efficacy and safety of DAP in children with RTIs, [19] there is a lack of cost-effectiveness studies evaluating antibiotic prescription strategies [20,21,22,23] in paediatric populations. Studies that do exist have focused on otitis media and have been carried out in the USA [20, 21, 23] and Canada [22]. Those studies have one important limitation: the cost of AMR was not taken into account [20,21,22,23].
Although IAP, the current form of treatment, is slightly more effective than DAP, according to a recent meta-analysis [19], previous economic analyses also conclude that DAP is the least costly strategy [20, 21], because it implies less antibiotic consumption, and fewer adverse effects. Therefore, DAP will likely be more cost-effective than IAP. The differences between DAP and NAP, however, are not easy to determine, since the results may depend on the complications derived from the non-use of antibiotics, and/or on the adverse effects derived from antibiotic use. Finally, it should be noted that the impact of DAP in reducing AMR cannot be appreciated over the short term. For children with RTIs, therefore, our aim was to analyse the overall cost-effectiveness of the DAP, IAP, and NAP strategies, including, in addition, an estimate of the AMR cost. This study was conducted in the context of a RCT [24].
Methods
Design
Trial-based cost-effectiveness analysis.
Randomized clinical trial
The RCT [24] compared three antibiotic treatment strategies (DAP, IAP, and NAP), deployed in children with acute uncomplicated RTIs. Recruitment took place between June 2012 and June 2016 in 39 centres in Spain. Participants were children aged 2–14 years who attended with one of the following conditions: pharyngitis, rhinosinusitis, acute bronchitis, or acute otitis media. Children were included if paediatricians had a reasonable doubt about the need to prescribe an antibiotic. Children with pharyngitis were excluded when paediatricians had access to rapid streptococcal testing.
Prescription strategies were as follows:
Immediate antibiotic prescription: an antibiotic was prescribed to be started immediately on the day of the visit.
Delayed antibiotic prescription: an antibiotic was prescribed, but not to be started immediately; rather, parents were given structured recommendations about when to administer the antibiotic and when to consider returning to the paediatrician.
No antibiotic prescription: no antibiotic was prescribed, but parents were given structured recommendations about when to consider returning to the paediatrician.
For both the DAP and IAP strategies, each paediatrician decided the type of antibiotic to prescribe.
Primary outcomes were symptom duration and symptom severity. Symptom duration was measured as days until symptoms disappeared. Symptom severity was collected by parents using a 7-point Likert scale (0 = absence of symptoms, 1–2 = mild symptoms, 3–4 = moderate symptoms, and 5–6 = severe symptoms). Secondary outcomes were antibiotic use, additional visits, complications at 30 days, and beliefs and satisfaction of the parents.
Data were collected by paediatricians at the initial visit. Follow-up data were collected by telephone on days 2 and 30 after inclusion, and additionally, on days 7,15 and 22 when parents stated in the previous telephone call that symptoms persisted.
Cost-effectiveness decision model
A decision tree (Fig. 1) was created to compare the three strategies for a time frame of 30 days. A societal perspective was adopted that included healthcare direct costs, and non-healthcare direct and indirect costs. The three antibiotic strategies were deployed starting with a baseline visit (V0) in which, as the initial treatment, antibiotics were prescribed for the IAP and DAP arms, and no antibiotics were prescribed for the NAP arm. Two outcomes resulted following V0: (1) symptoms resolved; or (2) symptoms persisted. The response to those outcomes then depended on the original strategy assigned to each patient.

Decision tree. *V0 represents the baseline visit for the three strategies, each of which has a different initial treatment value (T0). DAP: delayed antibiotic prescription; IAP: antibiotic treatment; and NAP: no antibiotic. **If symptoms persist, the DAP alternatives are antibiotic prescription or a first additional primary care visit (V1). The only alternative for NAP and IAP is V1
IAP and NAP
If symptoms persisted, the patient returned to the PC centre (V1). Two possible outcomes resulted following V1: (1) antibiotic treatment, either continuation (with the same or a different antibiotic) for the IAP arm, or prescription of an antibiotic to be started immediately for the NAP arm, or further waiting while continuing with the previous treatment; or (2) diagnosis and treatment of possible complications, specifically, pneumonia, abscesses, cellulitis, emergency department (ED) visits, and hospital admissions. The same procedure was applied to successive visits.
DAP
If symptoms failed to resolve after V0, parents could decide to either administer the prescribed antibiotic or return to the PC centre (V1). Following V1, the procedure was the same as for the IAP and NAP strategies.
The observed cases for each subtree and for each strategy, as represented in the decision tree (Fig. 1), were extracted from the RCT and are reported in Table 1.
Resource use and costs
Total costs, in euros for the year 2022, were calculated using a bottom-up costing approach (Table 2). Measurement data were collected during the RCT.
Healthcare direct costs
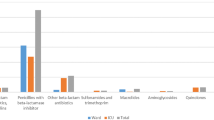
Costed were PC visits and ED visits, antibiotic and non-antibiotic medication use during the 30-day follow-up, doctor time (to explain recommendations for the assigned antibiotic strategy), and additional visits and drugs for adverse effects and complications (ED visits and hospital admissions). ED visits were evaluated by level of urgency as either non-urgent or a minor emergency. PC and ED visits were costed using data sourced from the Department of Health (Generalitat de Catalunya) [26]. Antibiotic and non-antibiotic medication costs were based on Spanish official prices. Considered were several classes of drugs currently in use: amoxicillin, amoxicillin-clavulanate, phenoxymethylpenicillin, and cefuroxime as antibiotics, and paracetamol and ibuprofen as non-antibiotic medication. Antibiotic and non-antibiotic medication costs were calculated from the number of packages needed to dose a 6-year-old child (the mean age of the included children). Doctor time to explain DAP and NAP strategy recommendations was calculated as equivalent to an additional 10% of the standard consultation time (i.e., 1 min per mean 10-min visit). No doctor time was counted for IAP as this strategy was considered the usual option.
In relation to adverse effects, we assumed that a rate of 10% in children treated with antibiotics, similar to the rate reported in the analysis by Coco et al. [20] and reflecting our RCT. We also assumed that adverse effects would always involve an additional visit and sometimes the prescription of non-antibiotic medication.
Non-healthcare direct and indirect costs
Direct costs calculated, using secondary information sources, were travel to healthcare institutions, parking, and outpatient consultation time for parents, while an indirect cost was time lost to work by parents (measured using a human capital approach), calculated from hourly wage data obtained from the Spanish National Statistics Institute (INE) [29]. Data on time lost to work were collected during the RCT. This cost was included, irrespective of who finally assumed it (the employer or the individual).
AMR cost
AMR was costed per prescription and per day using data published by the ECDPC [32] and the methodology of Oppong et al. [30]. Assuming that the Spanish population represents approximately 9% of the EU/EEA population and that prescriptions are made for seven days, we estimated 0.20 euros (2022) as the AMR cost per prescription over 30 days. The European average is similar to this value (0.15 pounds sterling, equivalent to 0.18 euros) according to Holmes et al. [31].
While AMR was included in our model as a cost, the cost of the reduction in antibiotic effectiveness assumed by society was not included, as is the usual practice in economic evaluations, due to the complexity of calculating this cost [30].
All costs were included in a deterministic sensitivity analysis (tornado diagram) whose low–high range is shown in Table 2.
Effectiveness estimates
Effectiveness estimates were calculated from quality-adjusted life-days (QALDs). QALD was used rather than quality-adjusted life year (QALY) because our time horizon was 30 days [20]. QALDs were calculated by multiplying days in each health state (moderate or severe specific symptoms, adverse effects, and days without symptoms), as collected during the RCT, by the associated utility value reflecting the child’s health-related quality of life at a given point in time.
Utility is normally scaled from 0 (= death) to 1 (= perfect health) and utility values for different health states in children with non-complicated RTIs are reported in the literature [20, 21, 23]. However, since, in our RCT, parents reported their children’s health state using a visual analogue scale (VAS), scored from 0 (= worst state) to 100 (= best state), the utility values used were based on those VAS scores.
The QALD value for a 30-day period for a child in perfect health is 30. Days of main moderate or severe specific symptoms and adverse effects indicated disutility, which we calculated as the difference between 1 and the average VAS score for each strategy. Data were collected to calculate utility as follows: on day 2, in relation to main severe specific symptoms, on day 7 in relation to main moderate specific symptoms, and on day 30 for no specific symptoms. Those days were chosen based on the mean duration in days for the main severe specific symptoms of 2.4 for DAP, 2.6 for IAP, and 2.6 for NAP, and for main moderate specific symptoms of 7 for DAP, 6.9 for IAP, and 6.9 for NAP.
For adverse effects, we calculated the number of days of adverse effects according to Coco et al. [20], and the associated disutility as reported by Shaikn et al. [21]. The disutility value for gastrointestinal adverse effects was 0.12, assuming that diarrhoea is a common, 2-day adverse effect, in 10% of children that used antibiotics [21]. In the case of hospitalization, disutility was rated as equivalent to the main severe symptoms and main moderate symptoms by consensus of the research team. Utility values and average days in each health state are reported in Table 3. A probabilistic sensitivity analysis was performed for these values.
Analyses
The three arms of the decision tree were compared in terms of cost per QALD using the ICER for the non-dominated alternatives. Cost-effectiveness analysis results were generated by summing direct health costs, non-healthcare direct and indirect costs, and AMR cost in euros per patient treated to obtain a total cost. Effectiveness was measured in gained QALDs, also per patient treated. The options, presented in order of costs (lowest to highest) were assumed to be mutually exclusive (a patient can only receive one intervention at a time). Dominated alternatives were excluded. Of the two dominance types, strict and extended, an alternative had strict dominance if it was less costly and yet more effective, and had extended dominance if its ICER was greater than the ICER of the next most effective alternative. We also calculated the net monetary benefit (NMB) [33] was also calculated as a better tool for decision making. Since the time horizon of the model was short (30 days), no discount rate over time was calculated.
We conducted a deterministic sensitivity analysis for all costs as listed in Table 2. The tornado analysis tested multi-way effects on the results of the model, reflecting the impact of variations in the ICER, which oscillated between low and high in a range from minus 15% to plus 15%.
We also conducted a probabilistic sensitivity analysis, in which all parameters were simultaneously and randomly varied across 10 000 Monte Carlo iterations in order to calculate cost-effectiveness probabilities for the three strategies. Distributions used were a beta distribution for utilities and probabilities, and a gamma distribution for costs [33].
An incremental cost-effectiveness plane and a cost-effectiveness acceptability curve were plotted to calculate the probability that an alternative may be cost-effective, given a threshold range of values (0–164.4 euros) for willingness-to-pay. The willingness-to-pay value was defined as the maximum cost that a society is willing to pay for one QALD gained in health. We considered a willingness-to-pay value of 82.2 euros per day, in accordance with the recommended 30 000 euros/QALY [21, 29].
TreeAge Pro 2021 (TreeAge, Williamstown, Massachusetts) statistical software was used for the analyses.
Results
Patients and clinical outcomes
A total of 422 paediatric patients were included in the trial. Mean (SD) age was 6.3 (3.0) years, and 216 (51.2%) were girls. Diagnoses were acute otitis media (n = 217; 51.4%), pharyngitis (n = 141; 33.4%), bronchitis (n = 39; 9.2%), and rhinosinusitis (n = 25, 5.9%). Most children (n = 382; 90.5%) had no respiratory comorbidities. Table 4 summarizes patient sociodemographic and clinical characteristics.
Note that of five ED visits, three were non-urgent and two were minor emergencies. A single DAP case of hospitalization for dehydration due to fever was considered an outlier because of its undue impact on the overall results (given its very high cost), and also because it had the same probability of occurring in any of three arms and mainly depended on risk factors such as the age of child. This case was therefore costed as a minor emergency.
Cost-effectiveness
The cost-effectiveness of each antibiotic strategy is shown in Table 5, ordered from least to most costly. The ICER calculation allowed us to determine which strategies were dominated or excluded.
Total costs in euros were 109.68 for IAP, 100.90 for DAP, and 97.48 for NAP. QALDs were 27.94 for DAP, 27.88 for IAP, and 27.82 for NAP. DAP was the most cost-effective strategy overall. IAP was more costly but equally as effective as DAP. NAP was both less costly and less effective than DAP (by 0.12 QALDs). Comparing DAP with NAP, the ICER was 28.84 euros per gained QALD for DAP. The NMB results confirmed that DAP should be the preferred strategy, although the difference between DAP and NAP was very small (6.33 euros). The very similar QALD results for the three strategies approximate our analysis to a cost minimization analysis (Table 5).
Deterministic sensitivity analysis
The cost of parental time lost to work, followed by the cost of PC visits, were the variables with the greatest impact on the ICER (Fig. 2). The relationship between time lost to work and impact on ICER was positive (in red to the right of the ICER value), while the relationship between PC visits and impact on ICER was negative (in blue to the right of the ICER value). Thus, any increase in time lost to work by parents increased the ICER value, while any increase in PC visits reduced the ICER value. This is explained by the fact that time lost to work affected DAP more than NAP, while PC visits affected NAP more than DAP.

Deterministic sensitivity analysis: tornado diagram. ICER: incremental cost-effectiveness ratio. DAP: delayed antibiotic prescription; NAP: no antibiotic prescription
The impact on the ICER was greater than the variation in the baseline value only in the case of time lost to work, with a variation of 15% in time lost to work having a 23% impact on the ICER (Table 6).
Probabilistic sensitivity analysis
Figure 3 shows the incremental cost-effectiveness scatterplot with 10 000 Monte Carlo iterations of the probabilistic model. DAP was more effective and more costly than NAP, as indicated by the 79.10% of iterations in quadrant I; however, the fact that ICER was below the willingness-to-pay value (82.2 euros) for 61.34% of the iterations in quadrant I indicates that DAP was the societally eligible strategy. Furthermore, DAP could be a dominated option in 20.77% of the iterations (represented in quadrant IV).

Probabilistic sensitivity analysis: cost-effectiveness plane. DAP: delayed antibiotic prescription; NAP: no antibiotic prescription; WTP: willingness-to-pay
Figure 4 depicts the cost-effectiveness acceptability curve for the probabilistic sensitivity analysis. As the willingness-to-pay value increased, DAP became more eligible, i.e., the probability of cost-effective iterations increased for the DAP strategy. For a willingness-to-pay value of 82.2 euros, DAP compared to NAP accounted for around 81.75% of cost-effectiveness iterations. For any willingness-to-pay value, IAP was dominated by one or both of the other alternatives.

Probabilistic sensitivity analysis: cost-effectiveness acceptability curve. DAP: delayed antibiotic prescription; IAP: immediate antibiotic prescription: NAP: no antibiotic prescription
Discussion
Main findings
DAP was the most cost-effective strategy for children aged 2–14 years attending PC centres with RTIs, whose paediatricians had reasonable doubt about the need to prescribe an antibiotic. NAP was less costly but less effective than DAP, although the difference was very small (0.12 QALDs). The ICER of DAP compared to NAP was 28.84 euros per gained QALD. The probabilistic sensitivity analysis showed that DAP was more cost-effective than NAP in 81.75% of the Monte Carlo iterations, with 82.2 euros as the willingness-to-pay value based on the recommended 30 000 euros/QALY. IAP was the dominated strategy, as it cost more and was equally as effective as DAP. The deterministic sensitivity analysis showed that time lost to work and PC visits were the costs with most impact on ICER values. Inclusion of the AMR cost in the analysis, referring to an interval of 30 days, did not change the results.
Results in context
Two previous studies [20, 21] have evaluated the cost-effectiveness of different antibiotic prescription strategies, including DAP. IAP in our study was more costly than DAP, as in the studies by Coco et al. [20] and Shaikh et al. [21] both of which also adopted a societal perspective. However, in our study, the cost difference between IAP and DAP (8.78 euros) was less than the 22.9 US dollars (DAP compared to IAP with 7–10 days of amoxicillin) for the Coco et al. study, and 36.37 US dollars (DAP compared to IAP with amoxicillin) for the Shaikh et al. study. The incremental gain in QALDs between strategies was very small in our study, as was the case in the above-mentioned two studies. Nevertheless, in those studies, IAP was the most cost-effective strategy, whereas in our study, DAP was the most cost-effective strategy. Our incremental gain in QALDs for DAP compared to IAP was 1.44 h, compared to the incremental gain in QALDs for IAP compared to DAP of 8.6 h in the Shaikh et al. study (IAP with amoxicillin), and 3.5 h in the Coco et al. study (IAP with 7–10 days of amoxicillin). Once the lower use of antibiotics and the lower adverse effects that can occur in DAP are considered, a possible explanation for the differences could be that our disutility values for the health status of children randomized to DAP, based on parent-reported VAS values, were lower than in previous studies.
Two other studies have evaluated the cost-effectiveness of different antibiotic prescription strategies but without including the DAP option. Sun et al., [23] in a study which was also based on a societal perspective, applied a watchful waiting approach as recommended in American Academy of Pediatrics guidelines, i.e., an antibiotic is considered for prescription only after waiting to see if symptoms would self-resolve. On the basis that watchful waiting could be considered a similar strategy to DAP, our finding that DAP was the most cost-effective strategy corroborates that Sun et al. [23] finding that watchful waiting was the most cost-effective strategy. Gaboury et al. [22] evaluated the cost-effectiveness of different antibiotic prescription strategies, not including DAP; they reported a result that coincides with Coco et al. [20] and Shaikh et al. [21], namely, that IAP was more cost-effective than watchful waiting. However, in the Gaboury et al. study, and contrasting with our study and those by Coco et al. and Shaikh et al. (adopting a societal perspective), watchful waiting compared to IAP with amoxicillin cost 9.48 Canadian dollars more.
Accounting for the AMR cost, to some extent our results coincide with the Oppong et al. [30] study that evaluated the cost-effectiveness of amoxicillin compared to placebo for adults with lower-RTIs attending PC centres. That study found that the dominant strategy did not change when AMR cost was included, but only for European data, i.e., not for data from other regions. Amoxicillin was the dominant strategy for those European data, while DAP was the cost-effective strategy in our study. Note, however, that the Oppong et al. study did not adopt, as we did, a societal perspective.
However, in comparisons between our findings and those of the above-cited studies, similarities and differences must be interpreted with care, both because of the variety of methods used and because those studies were carried out in the USA or Canada with their different health system models and healthcare costs.
Limitations and strengths
Our study has several possible limitations. First, we approximated health status utility using a VAS instead of measuring health status using standard gamble or time-trade off, or classifying health status using a questionnaire like the EuroQoL-5D [34]. Nevertheless, our findings can be considered reliable, as the QALDs were based on RCT data, and largely corroborate those of the meta-analysis by Oh [35]. Second, while the 30-day time horizon is sufficient for certain conditions, including RTIs, it is insufficient to assess the benefits of reduced antibiotic consumption in relation to reduced AMR. Third, we did not take into account private medical consultations, even though 12.6% of the Spanish population has private health insurance [36]. However, this limitation was likely to have had a similar impact on all three strategies. The trial was underpowered for two important cost drivers, namely, re-consultations and hospital admissions (included as complications), and wider individual-patient-data evidence [19] suggests that these are both higher with NAP compared to DAP; we therefore may have underestimated the cost-effectiveness of DAP. Fourth, the study was conducted in a pre-COVID-19 pandemic scenario, i.e., before the introduction of new rapid tests that could reduce diagnostic uncertainty. The cost of such tests were not considered but, as a fixed cost, it would not modify the results.
Our study also has some strengths. The main ones are that the study was based on a pragmatic RCT and, in analysing the cost-effectiveness of different antibiotic prescription strategies for children with RTIs, is the first such study performed outside North America. Our study, based on previous literature and a time horizon of 30 days, also considers AMR cost, a key issue not included in previous studies [20,21,22,23]. Finally, included also was the impact of non-healthcare direct and indirect costs in our study, reflecting a societal perspective.
Implications for practice and research
DAP is the most cost-effective strategy, although the difference with NAP is very small and the alternative IAP is a dominated strategy. For this reason, when panels consider the reduction of AMR a critical outcome, guideline panels are likely to recommend DAP strategies in those cases in which clinicians have doubts about whether it is necessary to administer an antibiotic to children with RTI.
Future studies should focus on more accurate analyses of the cost of AMR over a longer time period, and should consider the consequences of taking antibiotics not only in terms of costs, but also in terms of disutility of different health states, including re-consultations and complications.
Conclusions
When clinicians are in doubt about whether an antibiotic is needed for children with RTIs attending PC centres, those treated with the DAP strategy will have slightly better efficiency outcomes than those treated with IAP because its costs are lower than those of IAP. DAP is also the most cost-effective strategy over a time horizon of 30 days if AMR is considered, despite higher short-term costs than NAP. However, if in the long term the costs of AMR are larger than estimated, NAP could also be an alternative strategy.
Availability of data and materials
Study data and materials not included in this article are available from the corresponding authors on reasonable request.
Abbreviations
- AMR:
-
Antimicrobial resistance
- CREC:
-
Clinical research ethics committee
- DAP:
-
Delayed antibiotic prescription
- ED:
-
Emergency department
- IAP:
-
Immediate antibiotic prescription
- ICER:
-
Incremental cost-effectiveness ratio
- NAP:
-
No antibiotic prescription
- NMB:
-
Net monetary benefit
- PC:
-
Primary care
- QALD:
-
Quality-adjusted life day
- QALY:
-
Quality-adjusted life year
- RCT:
-
Randomized clinical trial
- RTI:
-
Respiratory tract infection
- VAS:
-
Visual analogue scale
References
Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128(6):1053–61.
Hollinghurst S, Gorst C, Fahey T, Hay AD. Measuring the financial burden of acute cough in pre-school children: a cost of illness study. BMC Fam Pract. 2008;9:10.
Kronman MP, Zhou C, Mangione-Smith R. Bacterial prevalence and antimicrobial prescribing trends for acute respiratory tract infections. Pediatrics. 2014;134(4):e956–65. Available from: https://www.ncbi.nlm.nih.gov/pubmed/25225144. 2014/09/15.
Andrade JV, Vasconcelos P, Campos J, Camurça T. Antibiotic Prescribing in Ambulatory Care of Pediatric Patients with Respiratory Infections TT - Prescrição Antibiótica no Ambulatório em Doentes Pediátricos com Patologia Respiratória. Acta Med Port. 2019;32(2):101–10. Available from: https://www.ncbi.nlm.nih.gov/pubmed/30896390. 2019/02/28.
Malo S, Bjerrum L, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Antibiotic prescribing in acute respiratory tract infections in general practice. An Pediatr (Barc). 2015;82(6):412–6.
Whaley LE, Businger AC, Dempsey PP, Linder JA. Visit complexity, diagnostic uncertainty, and antibiotic prescribing for acute cough in primary care: a retrospective study. BMC Fam Pract. 2013;14:120.
Lucas PJ, Cabral C, Hay AD, Horwood J. A systematic review of parent and clinician views and perceptions that influence prescribing decisions in relation to acute childhood infections in primary care. Scand J Prim Health Care. 2015;33(1):11–20.
Horwood J, Cabral C, Hay AD, Ingram J. Primary care clinician antibiotic prescribing decisions in consultations for children with RTIs: a qualitative interview study. Br J Gen Pract. 2016;66(644):e207–13.
Petursson P. GPs’ reasons for “non-pharmacological” prescribing of antibiotics. A phenomenological study. Scand J Prim Health Care. 2005;23(2):120–5.
Little P, Dorward M, Warner G, Stephens K, Senior J, Moore M. Importance of patient pressure and perceived pressure and perceived medical need for investigations, referral, and prescribing in primary care: nested observational study. BMJ. 2004;328(7437):444.
Little P, Williamson I, Warner G, Gould C, Gantley M, Kinmonth AL. Open randomised trial of prescribing strategies in managing sore throat. BMJ. 1997;314(7082):722–7.
Little P, Gould C, Williamson I, Warner G, Gantley M, Kinmonth AL. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. BMJ. 1997;315(7104):350–2. Available from: https://www.ncbi.nlm.nih.gov/pubmed/9270458.
Clavenna A, Bonati M. Adverse drug reactions in childhood: a review of prospective studies and safety alerts. Arch Dis Child. 2009;94(9):724–8. Available from: https://www.ncbi.nlm.nih.gov/pubmed/19531524. 2009/06/15.
Goossens H, FerechvanderStichele R, Elseviers M. M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–87.
WHO. Global action plan on antimicrobial resistance. World Health Organization, editor. Geneve: World Health Organization. 2015. Available from: https://apps.who.int/iris/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1.
Cassini A, Högberg LD, Plachouras D, Quattrocchi A, Hoxha A, Simonsen GS, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66.
Tan T, Little P, Stokes T, Group GD. Antibiotic prescribing for self limiting respiratory tract infections in primary care: summary of NICE guidance. BMJ. 2008;337:a437–a437. Available from: https://www.ncbi.nlm.nih.gov/pubmed/18650239.
American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113(5):1451–65.
Stuart B, Hounkpatin H, Becque T, Yao G, Zhu S, Alonso-Coello P, et al. Delayed antibiotic prescribing for respiratory tract infections: individual patient data meta-analysis. BMJ. 2021;373:n808.
Coco AS. Cost-effectiveness analysis of treatment options for acute otitis media. Ann Fam Med. 2007;5(1):29–38.
Shaikh N, Dando EE, Dunleavy ML, Curran DL, Martin JM, Hoberman A, et al. A Cost-Utility Analysis of 5 Strategies for the Management of Acute Otitis Media in Children. J Pediatr. 2017;189:54-60.e3.
Gaboury I, Coyle K, Coyle D, Le Saux N. Treatment cost effectiveness in acute otitis media: A watch-and-wait approach versus amoxicillin. Paediatr Child Health. 2010;15(7):e14–8.
Sun D, McCarthy TJ, Liberman DB. Cost-Effectiveness of Watchful Waiting in Acute Otitis Media. Pediatrics. 2017;139(4):e20163086.
Mas-Dalmau G, Villanueva López C, Gorrotxategi Gorrotxategi P, Argüelles Prendes E, Espinazo Ramos O, Valls Duran T, et al. Delayed Antibiotic Prescription for Children With Respiratory Infections: A Randomized Trial. Pediatrics. 2021;147(3):e20201323.
Vademecum Spain. Available from: https://www.vademecum.es. Cited 20 Apr 2022.
Generalitat de Catalunya. ORDRE SLT/63/2020, de 8 de març, per la qual s’aproven els preus públics de Servei Català de la Salut. Diari Oficial de la Generalitat de Catalunya. 2020;8134:1–173.
Travel Manager International. Revista profesional de viajes de negocio. Informe Captio 2021: ¿A cuánto se paga el kilometraje en España? Available from: https://revistatravelmanager.com/a-cuanto-se-paga-el-kilometraje-en-espana-2021/. Cited 27 Abr 2022.
Parkimeter. Available from: https://parkimeter.com/en. Cited 22 Apr 2022.
Spanish national institute of statistics. Salary structure survey. 2021. Available from: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177025&menu=ultiDatos&idp=1254735976596. Cited 3 Mar 2022.
Oppong R, Smith RD, Little P, Verheij T, Butler CC, Goossens H, et al. Cost effectiveness of amoxicillin for lower respiratory tract infections in primary care: an economic evaluation accounting for the cost of antimicrobial resistance. Br J Gen Pract. 2016;66(650):e633–9.
Holmes EAF, Harris SD, Hughes A, Craine N, Hughes DA. Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care. Antibiotics (Basel). 2018;7(4):106.
ECDC. Antimicrobial consumption in the EU/EEA – Annual Epidemiological Report 2019. 2020;1–25.
Briggs A, Claxton K, Sculpher M. Decision Modelling for Health Economic Evaluation. Oxford: OUP, editor. Int J Epidemiol. 2011.
Prieto L, Sacristán JA, Pinto JL, Badia X, Antoñanzas F, del Llano J. Analysis of costs and results of the economic assessment of health interventions. Med Clin (Barc). 2004;122(11):423–9.
Oh PI, Maerov P, Pritchard D, Knowles SR, Einarson TR, Shear NH. A cost-utility analysis of second-line antibiotics in the treatment of acute otitis media in children. Clin Ther. 1996;18(1):160–82.
Ministerio de Sanidad y Consumo. National Health Survey. 2017. Modalidad de la cobertura sanitaria. Available from: https://www.ine.es/dynt3/inebase/es/index.htm?type=pcaxis&path=/t15/p419/a2017/p05/&file=pcaxis.
Acknowledgements
We would like to thank the parents and children included in the study for their participation. We would also like to thank Cristina Puchol Sánchez for help with data collection and Ailish Maher for assistance with language editing of a version of the manuscript.
Delayed Antibiotic Prescription (DAP) Pediatrics Group
Members
Gemma Mas-Dalmau1,2 María José Pérez-Lacasta3–5 Pablo Alonso-Coello1,6* Pedro Gorrotxategi-Gorrotxategi7 Emma Argüelles-Prendes8 Oscar Espinazo-Ramos9 Josefa Manuel-Enguidanos9 Teresa Valls-Duran10 María Encarnación Gonzalo-Alonso11–13 María Pilar Cortés-Viana14 Tatiana Menéndez-Bada15 Marta Esther Vázquez-Fernández16 Ana Isabel Pérez-Hernández17 Laura Muñoz-Ortiz18 Carmen Villanueva-López19 Natividad Herrero-Torres19 Paul Little20 Mariam de la Poza-Abad21 Misericòrdia Carles-Lavila3–5* Lorena Martínez-Villamizar1 Carme Palassí-Bargalló22 Maria Amor Peix-Galito22 Francesca Camps-Serra23 Rosa Mené-Bergara23 Paloma Ramírez-Álvarez24 Marisa Pietrafesa-Barreiro25 Pilar Ortiz-Ros26 Virgina del Rey-Márquez26 Lucía Barahona-Rondón27 María Rosario Benítez-Rubio28 Ana María Valero-Marugán28 María Laura Casado-Sánchez29 Ángeles de Pando-Bravo30 Miren Arrate Bengoa-Gorosabe31 Carmen Callén-Blecua32 Inés Hernández-Salvador33 Irene Ozcoidi-Erro34 Javier Eduardo Blanco-González35 Carmelo Gutiérrez-Abad36
Affiliations
1Department of Epidemiology and Public Health - Iberoamerican Cochrane Centre, Hospital de la Santa Creu i Sant Pau - Biomedical Research Institute Sant Pau (IIB Sant Pau), Barcelona, Spain; 2Nursing Care Research Group, IIB Sant Pau, Barcelona, Spain; 3Department of Economics, Universitat Rovira i Virgili, Reus, Spain; 4Economic Challenges for the Next Generation (ECO-NEXT: SGR2021-00729), Reus, Spain; 5Research Centre on Economics and Sustainability (ECO-SOS), Reus, Spain; 6CIBER Epidemiology and Public Health (CIBERESP), Madrid, Spain; 7Pasai San Pedro Primary Care Centre, Pasaia, Spain; 8Ribadesella Primary Care Centre, Ribadesella, Spain; 9Las Matas Primary Care Centre, Las Rozas de Madrid, Spain; 10Val Miñor Primary Care Centre, Nigrán, Spain; 11Ugao Miraballes Primary Care Centre, Ugao Miraballes, Spain; 12Arrigorriaga Primary Care Centre, Arrigorriaga, Spain; 13Ariz–Basauri Primary Care Centre, Basauri, Spain; 14Maragall Primary Care Centre, Barcelona, Spain; 15Iruña de Oca Primary Care Centre, Nanclares de la Oca, Spain; 16Arturo Eyries Primary Care Centre, Valladolid, Spain; 17Torrelodones Primary Care Centre, Torrelodones, Spain; 18Catalan Agency for Health Quality and Assessment (AQuAS), Barcelona, Spain; 19Manso Primary Care Centre, Barcelona, Spain; 20Aldermoor Primary Care Centre, Southampton, UK; 21Dr Carles Ribas Primary Care Centre, Barcelona, Spain; 22Sardenya Primary Care Centre, Barcelona, Spain; 23Río de Janeiro Primary Care Centre, Barcelona, Spain; 24Sants Primary Care Centre, Barcelona, Spain; 25Bordeta-Magòria Primary Care Centre, Barcelona, Spain; 26Dos de Mayo Primary Care Centre, Móstoles, Spain; 27Valleaguado Primary Care Centre, Coslada, Spain; 28Miraflores Primary Care Centre, Alcobendas, Spain; 29San Blas Primary Care Centre, Parla, Spain; 30Villanueva de la Cañada Primary Care Centre, Villanueva de la Cañada, Spain; 31Bergara Primary Care Centre, Bergara, Spain; 32Bidebieta Primary Care Centre, San Sebastián, Spain; 33Alango Primary Care Centre, Getxo, Spain; 34Amara Berri Primary Care Centre, San Sebastián, Spain;35El Casar de Talamanca Primary Care Centre, El Casar, Spain; 36Las Huegas Primary Care Centre, Burgos, Spain.
Gemma Mas-Dalmau is a doctoral candidate in Methodology of Biomedical Research and Public Health, attached to the Paediatrics, Obstetrics and Gynaecology and Preventive Medicine Department, Universitat Autònoma de Barcelona, Barcelona, Spain.Pablo Alonso-Coello is a researcher included in the CERCA Programme of the Generalitat de Catalunya.
Funding
The study was funded by Instituto de Salud Carlos III under a 2016 grant call (Acción Estratégica en Salud 2013–2016: Programa de Investigación Orientada a los Retos de la Sociedad) within the framework of the Spanish National Plan for Scientific and Technical Research and Innovation 2013–2016 (PI11/02192), co-funded by the EU through the ERDF and the Spanish Ministry of Health, Social Services, and Equality (EC11-339).
Author information
Authors and Affiliations
Consortia
Contributions
Gemma Mas Dalmau (GMD): Conceptualization, Methodology, Data curation, Investigation, Writing – original draft, Project administration. María José Pérez Lacasta (MPL), Misericòrdia Carles Lavila (MCL): Conceptualization, Methodology, Formal analysis, Data curation, Writing – review and editing, Supervision. Pablo Alonso Coello (PAC): Conceptualization, Methodology, Writing – review and editing, Supervision, Funding acquisition. Pedro Gorrotxategi Gorrotxategi (PGG): Conceptualization, Methodology, Acquisition of data, Writing – review and editing. Emma Argüelles Prendes (EAP), Oscar Espinazo Ramos (OER), Teresa Valls Duran (TVD), María Encarnación Gonzalo Alonso (MGA), María Pilar Cortés Viana (MCV), Tatiana Menéndez Bada (TMB), Marta Esther Vázquez Fernández (MVF), Ana Isabel Pérez Hernández (APH): Acquisition of data, Writing – review and editing. Laura Muñoz Ortiz (LMO): Formal analysis, Writing – review and editing. Carmen Villanueva López (CVL): Conceptualization, Acquisition of data, Writing – review and editing. Paul Little (PL): Conceptualization, Writing – review and editing, Supervision. Mariam de la Poza Abad (MPA): Conceptualization, Methodology, Writing – review and editing, Funding acquisition.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the IDIAPJGol Clinical Research Ethics Committee (CREC) (reference committee), CREC Consorci Sanitari del Maresme, CREC Hospital General Universitario Gregorio Marañón, CREC Euskadi, CREC Asturias, CREC Hospital Universitario de Burgos, CREC León, CREC Valladolid Área Oeste, CREC Área de salud de Segovia, CREC Aragón, CREC Hospital Virgen del Rocío, CREC Hospital Universitario de Guadalajara, CREC Corporativo de Atención Primaria en la Comunidad Valenciana, CREC Galicia, and by the Spanish Medicines Agency (AEMPS). All study procedures were in accordance with the ethical standards of the Declaration of Helsinki. All parents and included children aged 12 and older signed an informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mas-Dalmau, G., Pérez-Lacasta, M. ., Alonso-Coello, P. et al. A trial-based cost-effectiveness analysis of antibiotic prescription strategies for non-complicated respiratory tract infections in children. BMC Pediatr 23, 497 (2023). https://doi.org/10.1186/s12887-023-04235-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-04235-3