
Abstract
Background
This study aimed to apply near-infrared spectroscopy (NIRS) to monitor cerebral oxygen saturation (SrO2) level in neonates before and after the change of mechanical ventilation mode, and thus, the effects of the change of mechanical ventilator mode on SrO2 level in neonates were assessed.
Methods
This trial was designed as an observational study .A total of 70 neonates who were admitted to the Department of Neonatology of Beijing Luhe Hospital Affiliated to Capital Medical University (Beijing, China) between September 2019 and October 2021 and required respiratory support were included. The variations of SrO2 level before and after the change of mechanical ventilation mode, including changing from Synchronized intermittent mandatory ventilation (SIMV) to noninvasive ventilation (NIV, group 1), and from NIV to oxygen inhalation (group 2), were monitored by Enginmed EGOS-600 A. The changes of SrO2 level at 30 min before and 1 h after the change of ventilation mode were compared between the two groups.
Results
The SrO2 level in the group 1 30 min before, as well as 10 min, 30 min, and 1 h after the change of ventilation mode was 62.54 ± 3.36%, 65.43 ± 3.98%, 64.38 ± 4.23%, and 64.63 ± 3.71%, respectively. The SrO2 level at all the points after the change of ventilation mode increased compared with 30 min before the change (P < 0.05). The SrO2 level in the group 2 at each time point was 62.67 ± 4.69%, 64.61 ± 5.00%, 64.04 ± 4.48%, and 64.55 ± 4.32%, respectively. Compared with 30 min before ventilator weaning, the SrO2 level at all the points after ventilator weaning increased (P < 0.05). Peak inspiratory pressure (PIP) excluding Nasal Continuous Positive Airway Pressure (NCPAP)) in group 1 was lower than that before extubation, and the difference was statistically significant (P = 0) (Table 7).
Conclusions
SrO2 level showed an increasing trend after the change of ventilation mode, and the increase of SrO2 level at 10 min after the change of ventilation mode was the most prominent. From SIMV to NIV, increased SrO2 levels may be associated with decreased PIP.
Similar content being viewed by others


Background
Mechanical ventilation is an important tool for the treatment of neonatal respiratory failure, which increased neonates’ survival rate [1]. Due to the differences in conditions and devices used in neonatal intensive care unit (NICU), as well as the differences in disease conditions, the mode of mechanical ventilation could be different [2]. The different respiratory supporting modes potentially have different influences on hemodynamics, especially on cardiac output. Studies performed using echocardiography showed that the influences of ventilation modes on hemodynamics were different, while indicators (e.g., cardiac output or blood pressure) only reflect macroscopical circulation, rather than necessarily reflect the oxygenation in blood flow or microcirculation [3,4,5]. Therefore, although extensive physiological examinations have been performed on neonates undergoing mechanical ventilation, cerebral injury in neonates is still worthy of further investigation. Recently, near-infrared spectroscopy (NIRS) has been applied for noninvasive real-time bedside monitoring of mixed blood oxygen saturation in microcirculation, better reflecting the oxygenation in tissues [6,7,8]. Therefore, this study utilized the NIRS to investigate the effects of various modes of mechanical ventilation on cerebral oxygen saturation (SrO2) level in neonates.The objective of this study was to determine whether the change of ventilator pattern in neonates has any effect on the oxygen supply to the brain tissue. And what is the trend of cerebral oxygen saturation before and after different ventilator mode changes in neonates? The predefined hypothesis was that there was an increase in cerebral oxygen saturation before and after the change of invasive ventilation mode.
Methods
Subjects
This trial was designed as an observational study.
Neonates who were admitted to the NICU (with respiratory support) of the Beijing Luhe Hospital Affiliated to Capital Medical University (Beijing, China) between September 2019 and October 2021 were included. The study was approved by the Ethics Committee of the Beijing Luhe Hospital Affiliated to Capital Medical University, and written informed consent was acquired from neonates’ parents 6 h before planned change in ventilator setting. All neonates with respiratory diseases were investigated, in which the respiratory supporting mode changed from one mode to another mode according to the disease conditions.
The inclusion criteria were as follows: (1) age < 28 days; (2) neonates who required respiratory support for respiratory diseases; and (3) signing the informed consent from by neonates’ parents.
The exclusion criteria were as follows: (1) neonates with severe intracranial hemorrhage (grade III or IV); (2) neonates with congenital heart disease or congenital cranial dysinnervation disorders; (3) neonates with severe anemia, severe asphyxia, inherited metabolic diseases, or ischemic or hypoxic cerebral diseases; (4) neonates with incomplete data that could not be used for statistical analysis; and (5) abandoning treatment by neonates’ parents and asking for ventilator weaning.
Material
The Enginmed EGOS-600 A was used to monitor the SrO2 level from 30 min before the change of ventilation mode until 1 h after the change. Spatially resolved NIRS was used in this trial.
The step down in the ventilation strategy from SIMV to non-invasive assisted ventilation including NCPAP/NIPPV/Bilevel positive airway pressure (BiPAP) was denoted as group 1”, and the Noninvasive assisted ventilation (including NCPAP/NIPPV/BiPAP)to oxygen inhalation were denoted as group 2.In addition, the multifunctional electrocardiogram (ECG) monitoring was applied to concurrently monitor clinical indicators, including heart rate, blood pressure, and respiration rate. We then recorded NIRS data for the 30 min before ventilator change and 60 min after ventilator change,then we compared SrO2 data for a 30-minute epoch prior to the change (eg-30 to 0 min, where ventilator change was designated time 0 ) with a 60-minute epoch after the change (e.g. 0 to + 60 min). NIRS saturation data were averaged within 1-minute (NIRS records data every 2 s).The average of SrO2 level was calculated every 10 min, and the time-SrO2 tendency chart was plotted (Fig. 1). The trend of SrO2 level was evaluated. In addition, the time point with a relatively substantial change of SrO2 level was selected for statistical analysis. Besides, the influences of gestational age, gender, delivery mode, birth weight, hemoglobin (Hb) level, 1-min Apgar score, and blood-gas indicators (PH, PCO2, PO2, HCO3, SO2, and Hb) on variation of SrO2 level were investigated. Furthermore, the associations of heart rate, respiration, and blood pressure with variation of SrO2 level were explored.

Tendency of changes of SrO2 level, respiration, and heart rate with time
Statistical analysis
Normally distributed quantitative data were described as mean and standard deviation. The comparisons of SrO2 level at different time points within group were performed by the analysis of variance (ANOVA) for repeated measurements, and the Fisher’s least significant difference (LSD) test was used for making comparison between the two groups. The variation of SrO2 level in neonates at 10 min after ventilator weaning was used as the dependent variable, and gestational age, birth weight, Hb level, 1-min Apgar score, and blood-gas indicators (PH, PCO2, PO2, HCO3, SO2, and Hb) were used as the independent variables, and then, the multivariate logistic regression model was established.The paired T-test was used to compare the changes of parameters before and after the change of ventilator mode. The vital signs at different time points were compared by ANOVA for repeated measurements. P < 0.05 was considered statistically significant.
Results
General characteristics
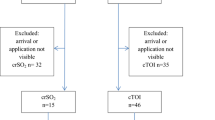
Totally, 75 neonates met the inclusion criteria, of whom 5 neonates were excluded. Specifically, 1 neonate with ischemic or hypoxic cerebral disease was excluded, 2 neonates were excluded for the incomplete data of SrO2 monitoring, and 2 neonates with congenital heart disease were excluded. Therefore, 70 neonates were finally included in this study, in which the gestational age ranged from 26 + 2 to 40 + 2 weeks, and the mean body weight was 2122.5 ± 800.2 g (Table 1).
Influences of clinical characteristics on SrO2 level
The multivariate logistic regression analysis showed that birth weight, gestational age, 1-min Apgar score, Hb level, blood-gas indicators (PH, PCO2, PO2, HCO3, SO2, and Hb), age (d) of ventilator weaning, gender, and delivery mode had no significant influence on variation of SrO2 level (P > 0.05) (Table 2).
Correlation analysis showed that with the change of mechanical ventilation mode, heart rate, respiration rate, and SrO2 level also changed concurrently (Fig. 1). Blood pressure monitoring showed that both systolic blood pressure (SBP) and diastolic blood pressure (DBP) increased after than before ventilator weaning. Therefore, with the change of ventilation mode, the heart rate, respiration rate, and blood pressure all slightly increased concurrently with the SrO2 level; however, ANOVA for repeated measurements showed that the changes were not statistically significant (P > 0.05) (Table 3).
Influences of changing from SIMV to noninvasive ventilation (NIV) mode on SrO 2 level
A chart was plotted to illustrate the tendency of change of SrO2 level with time in the group 1, which showed that the SrO2 level tended to increase after ventilator weaning, reached the peak at 10 min after ventilator weaning, and then started to decrease, while the SrO2 level was still higher than that before ventilator weaning (Fig. 2). The linear analysis of the change of SrO2 level with time in the group 1 showed that the change had a linear tendency (F = 10.796, P = 0.002) (Table 4). The SrO2 level in neonates before ventilator weaning was 62.54 ± 3.36% in the group 1, and the ANOVA for repeated measurements showed that the SrO2 levels at the 4 time points were statistically significant (P < 0.001). The SrO2 level at 10 min after ventilator weaning (65.43 ± 3.98%) was significantly higher than that before ventilator weaning (P < 0.001); however, the SrO2 level at 30 min (P < 0.001) and 1 h (F = 10.524, P < 0.001) after ventilator weaning decreased gradually (Fig. 2).

Tendency of the impact of the change of mechanical ventilation mode on SrO2 level. SrO2 level tended to increase after the change of mechanical ventilation mode in the group 1 and group 2, which reached the peak at 10 min after the change. The variation of SrO2 level in the group 1 was more prominent, and the change was larger
Influences of changing from NIV to oxygen inhalation on SrO2 level
A chart was plotted to illustrate the tendency of the change of SrO2 level with time in the group 2, which showed that the SrO2 level also tended to increase after ventilator weaning. The SrO2 level reached the peak at 10 min after ventilator weaning and then started to decrease, while the SrO2 level was still higher than that before ventilator weaning (Fig. 2). The linear analysis of the change of SrO2 level with time in the group 2 also showed that the change had a linear tendency (F = 7.717, P = 0.009) (Table 5). The SrO2 level in neonates before ventilator weaning was approximately 62.67 ± 4.69% in the group 2, which significantly increased to 64.61 ± 5.00% at 10 min after ventilator weaning (P = 0.002), and then, started to decrease gradually 10 min later and stabilized at 30 min after ventilator weaning. However, the SrO2 level (64.55 ± 4.32%) was still significantly higher than that before the ventilator weaning (P = 0.003) (Table 6).
Comparison of ventilator parameters
PEEP in group 1 was lower than that before extubation, and FiO2 was higher than that before extubation, but the differences were not statistically significant (P = 0.34,P = 0.156). However, PIP (excluding NCPAP) in group 1 was lower than that before extubation, and the difference was statistically significant (P = 0) (Table 7). FiO2 in group 2 was higher than that before ventilator weaning,but the differences were not statistically significant (P = 0.148) (Table 7).
Discussion
The findings of this study demonstrated SrO2 level increased in both groups after the change of mechanical ventilation mode.Birth weight, gestational age, 1-min Apgar score, Hb level, and blood-gas indicators had no significant influence on neonatal SrO2 level. From SIMV to NIV, increased SrO2 levels may be associated with decreased PIP.
Influences of changing from SIMV to NIV on SrO2 level
The findings of the present study showed that after the change of mechanical ventilation mode, including from SIMV to NIV, neonatal SrO2 level increased compared with before the change, which reached the peak at 10 min after the change, and then gradually stabilized at 1 h after the change.
Schwaberger et al. have shown an influence of respiratory support on cerebral hemodynamics (cerebral blood volume, cerebral oxygenation) [9, 10]. The effect of invasive ventilation on SrO2 could be associated with the increase of intrathoracic pressure caused by the ventilation, which induced cerebral venous stasis and cardiac venous return impairment, and could consequently influence the cerebral blood volume [11]. In addition, invasive procedures changed the anatomical structures of the respiratory tract; the neonate-machine interaction could also induce the variation of arterial blood pressure and cerebral blood flow velocity, and could consequently lead to the variation of SrO2 level [12, 13]. Govindan et al. continuously monitored the mean arterial pressure (MAP) and cerebral blood flow in neonates who underwent positive pressure ventilation by NIRS, and found that the variation of ventilator-related cerebral blood volume in neonates could further induce the passive change of cerebral oxygen metabolism, and consequently induce cerebral injuries in neonates [14]. Several studies have recently compared the effects of different invasive ventilation modes on cerebral oxygen. In a study performed by Mrozek et al. [15], intermittent mandatory ventilation, synchronized intermittent mandatory ventilation, and assist/control (A/C) mode of mechanical ventilation were used for neonates with respiratory stress syndrome within 6 h after the application of a surfactant, and the findings showed that neonate-machine interaction could induce arterial pressure variation, and further induce cerebral blood flow instability, thereby inducing severe intraventricular hemorrhage. Schwaberger B et al. found that the oxygen supply for brain increased within 15 min after birth in healthy neonates, which induced the contraction of cerebral blood vessels and reduced cerebral blood volume [9, 16]. The present study compared neonates who underwent mechanical ventilation and those who did not undergo mechanical ventilation, and found that the blood volume in both groups decreased continuously within 15 min after birth, while the amplitude of reduction in neonates who underwent mechanical ventilation was relatively low within the first 7 min [9]. However, there are still debates on whether the reduction of cerebral blood volume can be induced by mechanical ventilation or the pathological states in neonates.
Influences of changing from NIV to oxygen inhalation on SrO2 level
The findings showed that in the noninvasive-oxygen inhalation group (group 2), neonatal SrO2 level increased compared with before ventilator weaning, which reached the peak at 10 min after the ventilator weaning and then gradually stabilized.
Theoretically, the influence of changing from NIV to oxygen inhalation on SrO2 level could be associated with the disappear of pressure from assisted ventilation, which induced the reduction of intrathoracic positive pressure, increased venous return and cardiac output, and consequently increased the cerebral blood flow and induced the elevation of SrO2 level [17, 18]. However, Schwaberger et al. have shown that respiratory support immediately after birth by using sustained lung inflations in preterm infants did not show significant differences in CBV and cTOI compared to not using RS [19].Zhong et al. [4]investigated 26 neonates (born at the gestational age of 25–37 weeks), and found that the mean cerebral oxygenation in neonates on positive airway pressure ventilation was not significantly different from that in the normal control group; however, mean cerebral fractional oxygen extraction (FOE) in neonates increased from 0.22 ± 0.10 to 0.28 ± 0.13 (P = 0.002) with the increase of time of positive airway pressure ventilation, indicating the increasing tendency of SrO2 level.
Conclusions
In summary, SrO2 level increased in neonates after changing from SIMV to NIV mode, which reached the peak at 10 min after the change of mode and then gradually stabilized at 30 min after the change. The SrO2 level also increased in neonates after changing from NIV to oxygen inhalation, which peaked 10 min after the change and then gradually stabilized at 10 min after the change. The change of SrO2 level from SIMV to NIV may be associated with decreased PIP. .
Data Availability
All data generated or analysed during this study are included in this article.
Abbreviations
- NIRS:
-
Near-infrared spectroscopy
- SrO2:
-
Cerebral oxygen saturation
- CMV:
-
Conventional mechanical ventilation
- SIMV:
-
Synchronized intermittent mandatory ventilation
- NIPPV:
-
Nasal intermittent positive pressure ventilation
- BiPAP:
-
Bilevel mask positive airway pressure
- NCPAP:
-
Nasal continuous positive airway pressure
- NICU:
-
Neonatal intensive care unit
- ECG:
-
Electrocardiogram
- Hb:
-
Hemoglobin
- ANOVA:
-
Analysis of variance
- LSD:
-
Least significant difference
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
References
Nasef N, Rashed HM, Aly H. Practical aspects on the use of non-invasive respiratory support in preterm infants. Int J Pediatr Adolesc Med. 2020;7:19–25.
[Routine of mechanical ventilation in neonates]. Zhonghua Er Ke Za Zhi. 2015;53:327–30.
Tana M, Polglase GR, Cota F, et al. Determination of lung volume and hemodynamic changes during high-frequency ventilation recruitment in Preterm neonates with respiratory distress syndrome. Crit Care Med. 2015;43:1685–91.
Zhong J, Lui K, Schindler T. The effect of continuous positive Airway pressure on cerebral and splanchnic oxygenation in Preterm Infants. Neonatology. 2019;116:363–8.
Brew N, Walker D, Wong FY. Cerebral vascular regulation and brain injury in preterm infants. Am J Physiol Regul Integr Comp Physiol. 2014;306:R773–86.
Booth EA, Dukatz C, Sood BG, et al. Near-infrared spectroscopy monitoring of cerebral oxygen during assisted ventilation. Surg Neurol Int. 2011;2:65.
Kenosi M, Naulaers G, Ryan CA, et al. Current research suggests that the future looks brighter for cerebral oxygenation monitoring in preterm infants. Acta Paediatr. 2015;104:225–31.
Kooi EMW, Verhagen EA, Elting JWJ, et al. Measuring cerebrovascular autoregulation in preterm infants using near-infrared spectroscopy: an overview of the literature. Expert Rev Neurother. 2017;17:801–18.
Schwaberger B, Pichler G, Binder-Heschl C, et al. Cerebral blood volume during neonatal transition in term and Preterm Infants with and without respiratory support. Front Pediatr. 2018;6:132.
Schwaberger B, Pichler G, Avian A, Binder-Heschl C, Baik N, Urlesberger B. Do sustained lung inflations during neonatal resuscitation affect cerebral blood volume in Preterm Infants? A Randomized Controlled Pilot Study. PLoS ONE. 2015;10(9):e0138964–4.
Rhee CJ, da Costa CS, Austin T, et al. Neonatal cerebrovascular autoregulation. Pediatr Res. 2018;84:602–10.
Su X, He Y. [Factors influencing ventilator weaning and predictive value of weaning criteria in children]. Zhonghua Er Ke Za Zhi. 2014;52:783–7.
Junhasavasdikul D, Telias I, Grieco DL, et al. Expiratory Flow Limitation during Mechanical Ventilation. Chest. 2018;154:948–62.
Govindan V, Govindan R, Massaro AN, et al. Cerebral venous volume changes and pressure autoregulation in critically ill infants. J Perinatol. 2020;40:806–11.
Bugiera M, Szczapa T, Sowińska A, et al. Cerebral oxygenation and circulatory parameters during pressure-controlled vs volume-targeted mechanical ventilation in extremely preterm infants. Adv Clin Exp Med. 2020;29:1325–9.
Schwaberger B, Pichler G, Binder-Heschl C, Baik N, Avian A, Urlesberger. B.Transitional changes in cerebral blood volume at Birth. Neonatology. 2015;108(4):253–8. https://doi.org/10.1159/000437347.
Wilkinson D, Andersen C, O’Donnell CP, et al. High flow nasal cannula for respiratory support in preterm infants. Cochrane Database Syst Rev. 2016;2:Cd006405.
Sadeghnia A, Foroshani MZ, Badiei Z. A comparative study of the Effect of nasal intermittent positive pressure ventilation and nasal continuous positive Airway pressure on the Regional Brain tissue oximetry in premature Newborns weighing < 1500 g. Int J Prev Med. 2017;8:41.
Schwaberger B, Pichler G, Binder C, et al. O-025Do sustained Lung Inflations during resuscitation of Preterm Infants affect cerebral blood volume and cerebral Regional Oxygen Saturation?[J]. Arch Dis Child. 2014;99(Suppl 2):A31–1.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Lihua Li conceived and supervised the study; Lihua Li and Jingjing Zhao designed experiments; Jingjing Zhao and Manman Li analysed data; Jingjing Zhao,Wei Wang and Wei Liu wrote the manuscript; Lihua Li and Rong Wu made manuscript revisions. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Beijing Luhe Hospital Affiliated to Capital Medical University(2021-LHKY-089-02). All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was acquired from neonates’ parents.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, J., Wu, R., Liu, W. et al. Effect of the change of mechanical ventilation mode on cerebral oxygen saturation level in neonates. BMC Pediatr 23, 231 (2023). https://doi.org/10.1186/s12887-023-04036-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-04036-8