
Abstract
Background
A variety of performance outputs are strongly determined by lower limbs volume and composition in children and adolescents. The current study aimed to examine the validity of thigh volume (TV) estimated by anthropometry in late adolescent female volleyball players. Dual-energy X-ray absorptiometry (DXA) measures were used as the reference method.
Methods
Total and regional body composition was assessed with a Lunar DPX NT/Pro/MD+/Duo/Bravo scanner in a cross-sectional sample of 42 Portuguese female volleyball players aged 14–18 years (165.2 ± 0.9 cm; 61.1 ± 1.4 kg). TV was estimated with the reference method (TV-DXA) and with the anthropometric method (TV-ANTH). Agreement between procedures was assessed with Deming regression. The analysis also considered a calibration of the anthropometric approach.
Results
The equation that best predicted TV-DXA was: -0.899 + 0.876 × log10 (body mass) + 0.113 × log10 (TV-ANTH). This new model (NM) was validated using the predicted residual sum of squares (PRESS) method (R2 PRESS = 0.838). Correlation between the reference method and the NM was 0.934 (95%CI: 0.880–0.964, Sy∙x = 0.325 L).
Conclusions
A new and accurate anthropometric method to estimate TV in adolescent female volleyball players was obtained from the equation of Jones and Pearson alongside with adjustments for body mass.
Similar content being viewed by others

Background
Human structure is commonly viewed as a hierarchy of organism, system, organ, tissue and cell [1, 2]. Consequently, body composition may be approached at different levels. Total body cannot be considered as a compositional level and the cellular level is of limited and specific interest. Taking these previous notes into account, the organizational system is often reduced into the chemical and the anatomical levels as proposed by Martin and Drinkwater [3].
Research dealing with body composition is often focused in the absolute quantity, percentage and distribution of body fat, in part, because of the apparent negative relationship of the fat component to health status. In the context of many sports, changing total and regional muscle component is a determinant factor in performance [4, 5] and the limited literature [6] suggests that total and appendicular lean soft tissue estimates have probably not received enough attention when compared to fat mass.
Lean soft tissue estimates derived from tissue-based models have been previously proposed [7–13]. A variety of fitness measures in youth were shown to be strongly determined by appendicular skeletal muscle mass [14–16]. Moreover, lower leg muscle [17] or thigh muscle volume [18] have been identified as preferable allometric scaling denominators to normalize VO2peak compared with body mass or either fat-free mass (FFM).
The method for determining body composition should be selected depending on research objectives. In general, methods have been developed with specific assumptions [2, 8, 9, 19] which limits is use to a certain group; such as males or females, general population or athletes, adults or children. At the organ and tissue level, imaging techniques such as computed axial tomography (CT) and multi-scan magnetic resonance imaging (MRI) are considered the “criterion” methods in assessing body composition [20, 21]. The image quality of CT is improving [22] but, compared to exposures of 2.5 mSv of typical natural environments, the effective radiation exposure is still ~10 mSv for a full body scan [21]. MRI, although safe, requires a high technical proficiency and is not cost-effective. Dual-energy X-ray absorptiometry (DXA) uses a relatively low dose of ionizing radiation (i.e., 1 mSv per scan) and is considered the safest and appropriate imaging modality to accesses body composition [23]. Still, the selection also needs to consider practical implications such as cost, operation, required technical skills, subject cooperation. Accessible, safe and cost-effective strategies are needed.
Water displacement leg volumetry offers a simple approach and was used for validation of lower limb volume derived from six truncated cone formulas in 32 young male and 15 adult females [24]. Studies on the validation of this anthropometric protocol in athletes are still limited to male rugby players [25]. In addition, in a sample of male adult cadavers midthigh girth was the best predictor of skeletal mass with a coefficient of correlation of 0.94 [9]. Therefore, the current study examines the validity of thigh volume (TV) estimated by anthropometry relative to estimates by DXA as the reference method in late adolescent female volleyball players. The analysis also considered a calibration of the anthropometric approach proposed by Jones and Pearson [24] by adding supplemental variables.
Methods
Study design and participants
The current cross-sectional study was part of a research project conducted in the Midlands of Portugal. Participants were recruited voluntarily from four competitive clubs covering three urban areas (Aveiro, Coimbra and Leiria). All volleyball players were from middle and high socio-economic status; considering parents educational background [26]. Adolescents were students in elementary and secondary schools. A total of 54 female adolescent volleyball players were assessed. The following inclusion criteria were considered: (i) chronological age >14.0 years and <17.9 years; (ii) based on self-reported information reaching menarche > 1 year (range: 1.5–6.4 years) before testing; (iii) having all data completed. The final sample of the current study was composed of 42 female volleyball players aged 14.0–17.9 years of European (Caucasian) ancestry.
Procedures
All research procedures were reviewed and approved by the Sports Science and Physical Education Faculty Scientific Committee of the University of Coimbra (CE/FCDEF-UC/00102014). Informed and formal written consent was acquired from all parents or legal guardians. During Easter breaks (i.e., 2-week period) of 2014 and 2015, coaches and athletes visited the laboratories in groups of 4–6 players during weekday afternoons. All measurements were taken in the same day. The anthropometric data was collected in standardized conditions by single and highly trained technician (MJCS), adopting recommended procedures [27]. DXA measurements were performed at the Department of Medical Imaging and Radiation Therapy at the School of Health and Technology of Coimbra. A single laboratory professional positioned the participants, performed the scans and executed the analysis according to the manufacturer’s manual.
Training history
Volleyball training years were obtained by individual interview at clubs and confirmed through the records at the Portuguese Volleyball Federation. Annual training volume for each player was daily recorded by the head coaches using standardized reporting forms of the research project. Players had ~3 training sessions per week of ~90 min∙session-1 and usually one game on Saturdays. Injuries and illnesses were accounted as nonattendances to training in the final annual training volume calculations.
Anthropometry
Stature (Harpenden stadiometer, model 98.603, HoltainLtd, Crosswell, UK), body mass (Seca electronic scale, model 770, Hamburg, Germany) and two skinfolds (Lange caliper, Beta Technology, Ann Arbor, MI, USA) were measured. Anterior and posterior skinfold measurement was performed on the right side of the body, to the nearest 0.1 mm, at the same level as mid-thigh circumference. The posterior thigh skinfold is not previewed in the above-cited standardized procedures but was already adopted in previous studies dealing with school children aged 10–13 years of both sexes [28, 29] and male adolescent rugby players [25]. Standing up, the participant places the right foot at the edge of the box with the knee bent at a right angle. The posterior skinfold site is then measured on the midline of the thigh with the technician kneeling and facing the left side of the participant.
Non-invasive estimation of thigh volume
Thigh volume estimated by anthropometry (TV-ANTH) of the right leg was determined from three circumferences and two partial lengths measured two times each and averaged for analysis. The technique was based on the procedures proposed by Jones and Pearson [24] in which the TV is fractioned into two portions, like two truncated cones: truncated cone 1 was determined from circumferences measured at the most proximal gluteal furrow and at one-third of the subischial height up from the tibial–femoral joint space; truncated cone 2 was similarly determined by using circumferences at the one-third of the subischial height up from the tibial–femoral joint space and at the transversal plan above the patella. Further details are provided in a clinical study [30]. In brief, volume was estimated from an equation derived from proximal (A 1) and distal (A 2) area sections that composed the truncated cones, and L is the length between the two transverse plans:
The areas A 1 and A 2 were derived from leg circumferences:
DXA
Whole-body DXA scans were performed with a Lunar DPX-PRO/NT/MD+ densitometer (Software Lunar Encore for Windows version 13.6, Waltham, MA, USA). Participants were positioned and examined according to the manufacturer’s manual. Regional composition of the lower limbs was sectioned following the same anatomic landmarks used in the anthropometric protocol. To derive thigh volume (TV-DXA), thigh lean soft tissue and bone were summed to obtain FFM in kilograms. Fat mass (FM) was also derived in kilograms. TV-DXA was calculated as:
The 1.1 g · mL-1 and the 0.9 g · mL-1, represents the mean density for FFM and FM, respectively [31].
Data quality
An independent sample of 20 late adolescent athletes from several sports was evaluated in all anthropometric dimensions two times within one week by the same technician (MJCS). Technical error of measurement (TEM; [32]) for stature and body mass were 0.32 cm and 0.21 kg, respectively. Corresponding values for front and posterior thigh skinfolds were 0.91 mm. For circumferences, TEM were 0.84 cm for proximal, 0.50 cm mid-thigh and 0.50 cm for distal. For the two partial lengths, TEM were 0.62 cm and 0.44 cm. The obtained errors of measurers are within the range of errors of a variety of field surveys [32]. Test-retest of DXA scans in 10 individuals displayed a coefficient of variation of 0.8% and 1.6% for lean soft tissue and percent of FM, respectively.
Data analysis
Descriptive statistics for the total sample of female adolescent volleyball players were calculated and the Kolmogorov-Smirnov test was used to analyse the degree of normality. Log10-transformations were applied to reduce nonuniformity of errors. The interrelationship between body mass and estimates of TV (TV-DXA and TV-ANTH) were examined using Pearson Correlation. Years of training, annual number of training sessions, chronological age, age at menarche, log10 (stature), log10 (body mass), log10 (anterior thigh skinfold) and log10 (posterior thigh skinfold), were included in the stepwise regression model as potential independent variables with log10 (TV-DXA) as the dependent variable. To avoid collinearity a variance inflation factor < 10 and a tolerance > 0.10 was set [33]. Individual values of predicted TV were calculated by back-transformation of the values generated by the new model (TV-NM). The predicted residual sum of squares (PRESS) was used to validate the regression model [34]. Differences between estimated TV by the new predictive model and TV estimated by DXA were evaluated with paired-sample Student’s t-tests. Agreement between anthropometric estimates (practical approach) and volume based on DXA was assessed using Deming regressions [35]. This regression method was adopted since both x and y variables are subject to error. Limits of agreement between TV-NM and TV-DXA were assessed with Bland-Altman plots [36]. Alpha level was set at 0.05. Data analyses were completed using IBM SPSS v.23 for Mac OS.
Results
Descriptives for training experience, chronological age, estimated age at menarche, stature, body mass and appendicular skinfolds are summarized in Table 1. Body mass and posterior thigh skinfold did not fit the assumptions of normal distribution; all non-normally distributed variables were log transformed. All volleyball players attained menarche (ranged 10.8–15.7 years) and compete in organized and competitive volleyball (2-8 years). Mean statures and body masses (±SD) were 165.2 ± 0.9 cm and 61.1 ± 1.4 kg, respectively.
TV estimates derived from anthropometry and by DXA are summarized in Table 2. The means and standard deviation for TV-ANTH and TV-DXA were 4.91 ± 1.03 L and 5.55 ± 0.90 L, respectively. TV-ANTH did not fit the assumptions of normal distribution and were subsequently log-transformed.
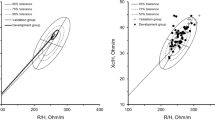
Relationships between body mass and estimates of TV (TV-ANTH; TV-DXA) are illustrated in Fig. 1. The correlation coefficients were 0.935 (95%CI: 0.882–0.965; 87.4% of variance in TV-DXA explained by body mass) and 0.815 (95%CI: 0.680–0.897; 66.5% of variance in TV-ANTH explained by body mass). The concurrent assessments of TV (TV-ANTH; TV-DXA) presented a large correlation (0.814; 95%CI: 0.678–0.896) with 66.37% of overlapping variance (Fig. 2). The slope coefficient was 0.850 (95%CI: 0.656–1.04) and was not considered different from the unit. The intercept was 1.620 (0.408–2.350) and was not significantly different from zero. A slope coefficient different from one reflects a proportional error while a systematic error corresponds to an intercept different from zero [35, 37, 38].

Regressions between body mass and estimates of thigh volume by anthropometry (TV-ANTH) and by dual X-ray absorptiometry (TV-DXA) in female volleyball players aged 14-18 years (n = 42). The standard error of estimation (Sy∙x), correlation (R) and coefficient of determination (R 2) are also presented

Deming regression between estimates of thigh volume by anthropometry (TV-ANTH) and by dual X-ray absorptiometry (TV-DXA) in female volleyball players aged 14-18 years (n = 42). The standard error of estimation (Sy∙x), correlation (R), confidence intervals for the correlation (CI) and coefficient of determination (R 2) are also presented
The regression model for TV prediction is given in Table 3. The correlation between the TV-NM including log10 (body mass), log10 (TV-ANTH) with TV-DXA was 0.922 (85.1% of overlapping variance). The prediction equation was as follows:
PRESS statistics were used to internally validate the TV-NM as presented in Table 3. The R 2 (0.838) was higher than R 2 presented in Fig. 2 (0.663) and SEE in Table 3 was low (0.027) which emphasized the accuracy of the model.
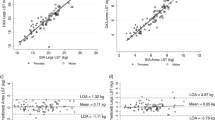
Deming repression analysis determined a nearly perfect correlation between TV-DXA and the TV-NM proposed in the current study for female adolescent volleyball: R = 0.934 and a Sy∙x = 0.325 (Fig. 3a). As reported in Fig. 3a, the intercept (-0.273) and slope (1.050) of the equation did not significantly differ from zero and one, respectively, rejecting the possibility of systematic or proportional bias. The measurement differences (error) relative to magnitude of TV were homoscedastic (r = 0.128; 95%CI: -0.183 to +0.416; Fig. 3b) with no significant mean differences between TV estimates by the ANTH-based NM and by DXA (Table 4).

Linear least product regressions between estimates of thigh volume and relationship between residuals and the mean of the concurrent estimates in female volleyball players aged 14-18 years (n = 42). Estimates of thigh volume by anthropometry-based new model (TV-NM) and by dual X-ray absorptiometry (TV-DXA, panel a). Differences between anthropometry-based new model (TV-NM) and reference given as dual X-ray absorptiometry (TV-DXA, panel b). The standard error of estimation (Sy∙x), correlation (R and r), coefficient of determination (R 2), upper limits of agreement (ULOA) and lower limits of agreement (LLOA) are also presented
Discussion
The present study developed and cross-validated an anthropometric equation for estimating TV based on DXA assessments in female late adolescent athletes. Estimated TV using the anthropometric equation [24] with adjustments for body mass among predictors increased the precision of the estimates relative to assessments by DXA which is considered a non-invasive imaging and reference technique. The data of the present study suggested that TV tended to be underestimated when derived from anthropometric models that combine the sum of two truncated cones compared to measurements derived from DXA assessments, although concurrent estimates were highly correlated (R = 0.814; 95%CI: 0.678–0.896). Among the limitations of this studies is the fact that DXA assumes constant density for all its components (i.e., skeletal mass tissue = 1.04 g · mL-1) and small errors into DXA estimates of skeletal mass may be introduced by the variability in actual skeletal mass density [12, 39]. Also, for the conversion of values of mass to volume, constant densities of FFM and FM values are used. It is known that actual densities may vary between different genders, ethnic groups and according to age [40].
Anthropometric equations for the prediction of total body lean soft tissue were developed in a large sample of nonobese and obese adults using MRI as the reference method [13]. These models are based in several assumptions: (i) lean soft tissue is theoretically in the shape of a cylinder; (ii) skinfolds can be used to correct measures of limb circumferences and provide reliable estimates of limb lean soft tissue circumferences; and, (iii) that the squared value of appendicular limb lean soft tissue circumferences generate estimates of lean soft tissue area. Though the accuracy of these models in predicting skeletal mass in adults exists [10], evidence of its applicability in young athletes is still lacking. In the current study, the difference between total body mass derived from scale mass and DXA was less than 1%. This value is within the range of under- or overestimation of whole-body FM using DXA due to extracellular fluid variations [41]. DXA-determined appendicular lean soft tissue has been validated against CT [31, 42]. This method was proposed as a reference imaging technique for the evaluation of limb lean soft tissue [10–13]. The method enables the identification of particular regions of interest and separates respective masses into bone mineral content plus two tissue compartments: fat and lean soft tissue [43].
The ordinary least squares method is generally used to obtain the slope and intercept of linearly related data. The technique presumes that the comparative method values are without error [44]. However, when random error affects both y and x values the least squares method may not be appropriate. Deming regression is a promising alternative because accommodates both y and x errors [25, 29, 45].
The sample of the current study was smaller than the 268 participants used in a previous study [6] but comparable with the study of rugby players aged 19.9 ± 2.2 years (n = 41) [25]. An appropriate participant-to-variable ratio is considered a relevant aspect while using multiple regressions, and it is recommended to maintain the critical proportion higher than 5:1 and preferably 20:1 [46]. In the current study, the baseline ratio was 5:1 with eight candidate predictors. The final model was based on a ratio of 21:1 with two significant predictors obtained from a sample of 42 female volleyball players. The PRESS method was used to avoid data splitting [34] which is a well-known method where the complete sample data are typically split into a fitting sample and a validation sample [37, 38]. The term PRESS corresponds to an acronym for predicted residual sum of squares. After obtaining a candidate model using multiple linear regressions analysis, the PRESS technique involves different prediction equations to obtain independent residuals since each case is left out of the respective model for estimation purposes.
A previous study with Portuguese adolescents athletes [6] was the first to present anthropometric-based equations to estimate limbs lean soft tissue with DXA as the reference method. Body mass was the strongest predictor of DXA-measured appendicular lean soft tissue, explaining 83% of the variation in appendicular lean soft tissue, while sex and stature contributed with 5% and 3% of additional explained variance. Chronological age only added 0.4% of the explained inter-individual variability. Among 65 boys and girls below stage 5 of sexual maturation, it was demonstrated that the stages of sexual maturation failed to contribute in the prediction of skeletal muscle after including body weight [11]. However, it should be noted that sexual maturation was determined by combining self-assessed stages of breast and pubic hair development, which could lead to misclassification between genders [40]. It is believed that appendicular fat tissue and appendicular lean soft tissue may be differently affected by inter-individual variability of biological maturation [47], since, on average, boys linearly increase muscle mass whereas girls attain a plateau in muscle mass and accumulate larger amounts of fat mass, particularly in the extremities. A recent study in healthy circumpubertal boys [29], used predicted mature (adult) stature as a non-invasive maturity status and identified a positive and significant contribution of this variable to explain inter-individual differences in lower limbs lean soft tissue. Additional studies are necessary to check for the adequacy of sex-specific models, while also using a valid assessment of biological maturity.
The allometric modelling procedures of the present study did not identified a significant contribution of years of training, annual number training sessions, chronological age, age at menarche, stature or posterior thigh skinfold to predict TV. Years of training are strongly correlated with chronological age and both variables presented a small range of variability and normal distribution. On the other hand, annual number of training sessions does not represent specify and intensity of the training activities. Similarly to previous studies [6, 25, 28, 29], body mass (R = 0.810) explained most of the variance of the TV-NM proposed in the current study for female adolescent volleyball players. The estimated TV using the anthropometric equation [24] added little explained variance (R = 0.138). Other approaches to estimate appendicular volume without the inclusion of TV-ANTH should be explored.
The available literature was lacking in non-invasive models to estimate appendicular size descriptors for female adolescent athletes. Estimates of lower limbs soft tissue or volume [16–18] are highly and positively associated with a multiplicity of ergometer and fitness assessments. Also, they have been shown to be more suitable scaling denominators than body mass or FFM to predict peak oxygen uptake in adolescent (14.5–16.5 years) male roller hockey players [16] and to predict outputs resulting from short-term power assessments in adolescent (14.0–16.0 years) male basketball players [5]. The equation derived from the present study is a useful analytical tool for the critical interpretation of variation of TV within and between individuals and presented similar internal validity to other available studies for similar proposes [6, 25, 28, 29].
It was possible to obtain an acceptable and nonbiased method to accurately predict thigh volume in female volleyball players aged 14–18 years. Strengths of the present study include the analysis of agreement between thigh volume predicted by a new anthropometry based model and estimated with DXA; which indicated no proportional bias between methods (see Fig. 2). Also, conclusions of the present study cumulatively emerged from the PRESS statistics combined with the analysis of mean differences and also from the plot of individual differences by mean scores of the measurements defining upper and lower limits of agreement. A substantial percentage of variance was explained by the new predictive model (R 2 = 0.872) and body mass was a relevant and additional predictor. The current investigation is not without limitations. The study was limited to a relatively small sample of 42 female volleyball players from a narrow age range. Moreover, prediction equations tend to be population specific and additional validation studies in female adolescent volleyball players are required to validate this model.
Conclusions
The current study clearly identified a new anthropometric-based model to estimate TV in research dealing with female late adolescent athletes. The model is based on procedures proposed by Jones and Pearson [24] with the addition of simple body mass measures. It was internally cross-validated with suitable statistical procedures, ensuring its applicability to similar samples. This equation represents an accurate and practical alternative to quantify TV in late adolescent female volleyball players.
Abbreviations
- A:
-
Area sections
- C:
-
Circumferences
- CT:
-
Computed axial tomography
- DXA:
-
Dual-energy X-ray absorptiometry
- FFM:
-
Fat-free mass
- FM:
-
Fat mass
- MRI:
-
Magnetic resonance imaging
- PRESS:
-
Predicted residual sum of squares
- TEM:
-
Technical errors of measurement
- TV:
-
Thigh volume
- TV-ANTH:
-
Thigh volume estimated by anthropometry
- TV-DXA:
-
Thigh volume estimated by DXA
- TV-NM:
-
Thigh volume estimated by anthropometry-based new model
References
Wang ZM, Ma R, Pierson RN, Heymsfield SB. Five-level model: reconstruction of body weight at atomic, molecular, cellular, and tissue-system levels from neutron activation analysis. Basic Life Sci. 1993;60:125–8.
Eston R, Hawes M, Martin A, Reilly T. Human Body composition. In: Eston R, Reilly T, editors. Kinanthropometry – tests, procedures and data. Abingdon, Oxon: Routledge; 2009.
Martin AD, Drinkwater DT. Variability in the measures of body fat: Assumptions or technique? Sports Med. 1991;11:277–88.
Coelho-e-Silva MJ, Figueiredo AJ, Carvalho HM, Malina RM. Functional capacities and sport-specific skills of 14-to 15-year-old male basketball players: Size and maturity effects. Eur J Sport Sci. 2008;8(5):277–85.
Carvalho HM, Coelho-e-Silva MJ, Figueiredo AJ, Goncalves CE, Philippaerts RM, Castagna C, et al. Predictors of maximal short-term power outputs in basketball players 14-16 years. Eur J Appl Physiol. 2011;111(5):789–96.
Quiterio AL, Carnero EA, Silva AM, Bright BC, Sardinha LB. Anthropometric models to predict appendicular lean soft tissue in adolescent athletes. Med Sci Sports Exerc. 2009;41(4):828–36.
Matiegka J. The testing of physical efficiency. Am J Phys Anthropol. 1921;4:223–30.
Heymsfield SB, McManus C, Smith J, Stevens V, Nixon DW. Anthropometric measurement of muscle mass: revised equations for calculating bone-free arm muscle area. Am J Clin Nutr. 1982;36(4):680–90.
Martin AD, Spenst LF, Drinkwater DT, Clarys JP. Anthropometric estimation of muscle mass in men. Med Sci Sports Exerc. 1990;22(5):729–33.
Kim J, Heshka S, Gallagher D, Kotler DP, Mayer L, Albu J, et al. Intermuscular adipose tissue-free skeletal muscle mass: estimation by dual-energy X-ray absorptiometry in adults. J Appl Physiol (1985). 2004;97(2):655–60.
Kim J, Shen W, Gallagher D, Jones A, Wang Z, Wang J, et al. Total-body skeletal muscle mass: estimation by dual-energy X-ray absorptiometry in children and adolescents. Am J Clin Nutr. 2006;84(5):1014–20.
Kim J, Wang Z, Heymsfield SB, Baumgartner RN, Gallagher D. Total-body skeletal muscle mass: estimation by a new dual-energy X-ray absorptiometry method. Am J Clin Nutr. 2002;76(2):378–83.
Lee RC, Wang Z, Heo M, Ross R, Janssen I, Heymsfield SB. Total-body skeletal muscle mass: development and cross-validation of anthropometric prediction models. Am J Clin Nutr. 2000;72(3):796–803.
Davies CT, Barnes C, Godfrey S. Body composition and maximal exercise performance in children. Hum Biol. 1972;44(2):195–214.
Docherty D, Gaul CA. Relationship of body size, physique, and composition to physical performance in young boys and girls. Int J Sports Med. 1991;12(6):525–32.
Valente-Dos-Santos J, Sherar L, Coelho-e-Silva MJ, Pereira JR, Vaz V, Cupido-Dos-Santos A, et al. Allometric scaling of peak oxygen uptake in male roller hockey players under 17 years old. Appl Physiol Nutr Metab. 2013;38(4):390–5.
Tolfrey K, Barker A, Thom JM, Morse CI, Narici MV, Batterham AM. Scaling of maximal oxygen uptake by lower leg muscle volume in boys and men. J Appl Physiol (1985). 2006;100(6):1851–6.
Welsman JR, Armstrong N, Kirby BJ, Winsley RJ, Parsons G, Sharpe P. Exercise performance and magnetic resonance imaging-determined thigh muscle volume in children. Eur J Appl Physiol Occup Physiol. 1997;76(1):92–7.
Drinkwater DT, Martin AD, Ross WD, Clarys JP. Validation by cadaver dissection of Matiegka’s equations for the anthropometric estimation of ana tomical body composition in adult humans. In: Day JA, editor. The 1984 Olympic Scientific Congress Proceedings. Champaign, Illinois: Perspectives in Kinanthropometry; 1984.
Lee SY, Gallagher D. Assessment methods in human body composition. Curr Opin Clin Nutr Metab Care. 2008;11(5):566–72.
Seabolt LA, Welch EB, Silver HJ. Imaging methods for analyzing body composition in human obesity and cardiometabolic disease. Ann N Y Acad Sci. 2015;1353:41–59.
Prado CM, Heymsfield SB. Lean tissue imaging: a new era for nutritional assessment and intervention. JPEN J Parenter Enteral Nutr. 2014;38(8):940–53.
Albanese CV, Diessel E, Genant HK. Clinical applications of body composition measurements using DXA. J Clin Densitom. 2003;6(2):75–85.
Jones PR, Pearson J. Anthropometric determination of leg fat and muscle plus bone volumes in young male and female adults. J Physiol. 1969;204(2):63P–6P.
Carvalho HM, Coelho-e-Silva MJ, Figueiredo AJ, Tavares OM, Ferry B, Hidalgo-Hermanni I, et al. Agreement between anthropometric and dualenergy X-ray absorptiometry assessments of lower-limb volumes and composition estimates in youth-club rugby athletes. Appl Physiol Nutr Metab. 2012;37:463–71.
Machado-Rodrigues AM, Coelho-e-Silva MJ, Mota J, Cumming SP, Riddoch C, Malina RM. Correlates of aerobic fitness in urban and rural Portuguese adolescents. Ann Hum Biol. 2011;38(4):479–84.
Lohman TG, Roche AF, Martorell R. Anthropometric standardization reference manual. Champaign, Illinois: Human Kinetics; 1988.
Coelho-e-Silva MJ, Malina RM, Simoes F, Valente-Dos-Santos J, Martins RA, Vaz V, et al. Determination of thigh volume in youth with anthropometry and DXA: agreement between estimates. Eur J Sport Sci. 2013;13(5):527–33.
Valente-dos-Santos J, Coelho-e-Silva MJ, Machado-Rodrigues AM, Elferink-Gemser MT, Malina RM, Petroski EL, et al. Prediction equation for lower limbs lean soft tissue in circumpubertal boys using anthropometry and biological maturation. PLoS ONE. 2014;9(9):e107219.
Villaca DS, Lerario MC. dal Corso S, Napolis L, de Albuquerque AL, Lazaretti-Castro M, et al. Clinical value of anthropometric estimates of leg lean volume in nutritionally depleted and non-depleted patients with chronic obstructive pulmonary disease. Br J Nutr. 2008;100(2):380–6.
Visser M, Fuerst T, Lang T, Salamone L, Harris TB. Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg musclemass. Health, aging, and body composition study-dual-energy x-ray absorptiometry and body composition working group. J Appl Physiol. 1999;87:1513–20.
Malina RM. Anthropometry. In: Maud PJ, Foster C, editors. Physiological assessment of human fitness. Champaign, Illinois: Human Kinetics; 1995. p. 205–19.
Slinker BK, Glantz SA. Multiple regression for physiological data analysis: the problem of multicollinearity. Am J Physiol. 1985;249(1Pt2):R1–R12.
Holiday DB, Ballard JE, McKeown BC. PRESS-related statistics: regression tools for cross-validation and case diagnostics. Med Sci Sports Exerc. 1995;27(4):612–20.
Ricker WE. Linear regressions in fishery research. J Fish Res Board Can. 1973;30:409–34.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–10.
Snee RD. Validation of regression models: methods and examples. Tecnhometrics. 1977;19:415–28.
Jackson AS, Pollock ML, Ward A. Generalized equations for predicting body density of women. Med Sci Sports Exerc. 1980;12(3):175–81.
Snyder WS, Cook MJ, Nasset ES, Karhansen LR, Howells GP, Tipton IH. Report of the task group on reference men. Oxford, United Kingdom: Pergamon Press; 1975.
Lohman TG. Applicability of body composition techniques and constants for children and youths. Exerc Sport Sci Rev. 1986;14:325–57.
Pietrobelli A, Formica C, Wang Z, Heymsfield SB. Dual-energy X-ray absorptiometry body composition model: review of physical concepts. Am J Physiol. 1996;271:E941–51.
Wang ZM, Visser M, Ma R, Baumgartner RN, Kotler D, Gallagher D, et al. Skeletal muscle mass: evaluation of neutron activation and dual-energy X-ray absorptiometry methods. J Appl Physiol (1985). 1996;80(3):824–31.
Shih R, Wang Z, Heo M, Wang W, Heymsfield SB. Lower limb skeletal muscle mass: development of dual-energy X-ray absorptiometry prediction model. J Appl Physiol (1985). 2000;89(4):1380–6.
Martin RF. General deming regression for estimating systematic bias and its confidence interval in method-comparison studies. Clin Chem. 2000;46(1):100–4.
Ludbrook J. Comparing methods of measurements. Clin Exp Pharmacol Physiol. 1997;24(2):193–203.
Vincent WJ. Statistics in Kinesiology. Champaign, Illinois: Human Kinetics; 2005.
Malina RM, Bar-Or O, Bouchard C. Growth maturation and physical activity. Champaign, Illinois: Human Kinetics; 2004.
Acknowledgments
The authors gratefully acknowledge the early contribution of Filipe Simões (†2013). Our thanks also go to Alexandra Silva, Nuno Amado and Shirley Souza for the input in the collection of the data.
Funding
JVdS (SFRH/BPD/100470/2014) and JPD (SFRH/BD/101083/2014) were partially supported by FCT. No other current funding sources for this study. The funder played no role in the design, collection, analysis or interpretation of the data, nor in the preparation of the manuscript or decision to submit the manuscript for publication.
Availability of data and materials
The dataset supporting the conclusions of this article is fully available without restriction and is included in the additional file 1.
Authors’ contributions
Conceived and designed the experiments: OMT DAM JMC DC MJCS. Performed the experiments: OMT JPD MJCS. Analyzed the data: JVdS JPD LAG RAF LBS MJCS. Data interpretation: JVdS JPD SCP LAG RAF DAM JMC LBS MJCS. Wrote the paper: OMT JVdS JPD DC MJCS. Revised manuscript content: SCP LAG RAF DAM JMC LBS. Approved final version of manuscript: OMT JVdS JPD SCP LAG RAF DAM JMC LBS DC MJCS.
Competing interests
The authors declare that they have no competing interest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was approved the Sports Science and Physical Education Faculty Scientific Committee of the University of Coimbra (CE/FCDEF-UC/00102014) and was conducted in accordance with the Declaration of Helsinki for human studies by the World Medical Association. Informed and formal written consent was acquired from all parents or legal guardians.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1186/s12887-017-0818-8.
Additional file
Additional file 1:
Dataset used in this Research. YT: years of training; ANS: annual number of training sessions; ANG: annual number of games; BM: body mass; H: stature; SKTA: anterior mid-thigh skinfold; SKTP: posterior mid-thigh skinfold; PTL: proximal thigh length; DTL: distal thigh length; TTL: total thigh length; CGF: circumference at the most proximal gluteal furrow (highest possible horizontal circumference); CMT: circumference at the one-third of the subischial height up from the tibial–femoral joint space; CMTC: circumference at the one-third of the subischial height up from the tibial–femoral joint space corrected for subcutaneous adipose tissue thickness; CDT: circumference at the minimum circumference above the patella (distal thigh); TVANTH: thigh volume based on Jones and Pearson; TVANTHFF: fat free volume in the thigh calculated based on Jones and Pearson; TVANTHF: fat volume in the thigh based on Jones and Pearson; DXATV: thigh volume estimated by DXA; DXATVFF: fat free volume in the thigh estimated by DXA; DXATVF: fat volume in the thigh estimated by DXA. (XLSX 21 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tavares, Ó.M., Valente-dos-Santos, J., Duarte, J.P. et al. Concurrent agreement between an anthropometric model to predict thigh volume and dual-energy X-Ray absorptiometry assessment in female volleyball players aged 14-18 years. BMC Pediatr 16, 190 (2016). https://doi.org/10.1186/s12887-016-0730-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-016-0730-7