
Abstract
Background
Several epidemiological studies have investigated the association between ambient air pollution and age-related macular degeneration (AMD). However, a consensus has not yet been reached. Our meta-analysis aimed to clarify this association.
Methods
Databases, including PubMed, EMBASE, and Web of Science, were searched for relevant studies from 01 January 2000 to 30 January 2024. English-language, peer-reviewed studies using cross-sectional, prospective, or retrospective cohorts and case–control studies exploring this relationship were included. Two authors independently extracted data and assessed study quality. A random-effects model was used to calculate pooled covariate-adjusted odds ratios. Heterogeneity across studies was also tested.
Results
We identified 358 relevant studies, of which eight were included in the meta-analysis. Four studies evaluated the association between particulate matter less than 2.5 μm in diameter (PM2.5) and AMD, and three studies explored the relationship between nitrogen dioxide (NO2) or ozone (O3) and AMD. The pooled odds ratios were 1.16 (95% confidence interval [CI]: 1.11–1.21), 1.17 (95% CI: 1.09–1.25), and 1.06 (95% CI: 1.05–1.07), respectively.
Conclusion
Current evidence suggests a concomitant positive but not causal relationship between PM2.5, NO2, or O3 and AMD risk.
Similar content being viewed by others


Background
Age-related macular degeneration (AMD) is one of the leading causes of blindness in the aging population [1,2,3,4]. Late-onset AMD can be classified into dry and wet forms. Although intravitreal injection of anti-vascular endothelial growth factor agents is the first-line therapy for AMD, not all patients benefit from this treatment [5]. The underlying mechanism is multifactorial and remains unclear [6]. Recent evidence has suggested a potential influence of ambient air pollutants on AMD risk [7, 8]. Thus, further investigation of this correlation would be clinically meaningful.
Many compounds comprise ambient air pollution, including nitrogen dioxide (NO2), carbon monoxide (CO), sulphur dioxide (SO2), ozone (O3), and particulate matter less than 2.5 and 10 μm in diameter (PM2.5 and PM10, respectively) [9]. Air pollution is a major contributor to the global disease burden and associated with health hazards [10,11,12]. Prior epidemiological studies have demonstrated that ambient air pollution is a potential risk factor for AMD [13, 14]. For example, a national cross-sectional study in China reported a significant positive association between PM2.5 and AMD. For PM2.5, compared with the lowest quartile, the odds ratios (ORs) and 95% confidence intervals (CIs) across increasing quartiles were 0.828 (0.674, 1.018), 1.105 (0.799, 1.528), and 2.602 (1.516, 4.468) [14]. However, conflicting findings were observed on the association between AMD and NO2 or O3 [7, 13]. Further investigation is needed to clarify the correlation between ambient air pollution and AMD. Therefore, we conducted this meta-analysis to report a more robust and reliable outcome.
Methods
Search strategy
This meta-analysis was conducted following the Meta-Analysis of Observational Studies in Epidemiology guidelines. The PubMed, EMBASE, and Web of Science databases were searched for literature using the key words ‘ambient air pollution, particulate matter, ozone, sulphur dioxide, nitrogen dioxide, or carbon monoxide’ and ‘AMD or age-related macular degeneration’ from 01 January 2000 to 30 January 2024. Furthermore, references from original studies or relevant reviews were manually searched to identify other relevant studies. All included studies were epidemiological investigations; the language was restricted to English. Two investigators independently retrieved and reviewed the full texts and abstracts of all related literature. Conflicts were resolved through a full-text review and discussed by two independent reviewers until a consensus was reached.
Inclusion and exclusion criteria
The following inclusion criteria were applied: the studies (1) referred to the association between ambient air pollution and AMD; (2) contained calculable information, such as ORs, hazard ratios (HRs), the respective 95% CIs, and P-values; and (3) were English-only peer-reviewed studies using cross-sectional, prospective, or retrospective cohorts and case–control study designs. The exclusion criteria were as follows: (1) duplicate subjects; (2) abstracts, case reports, comments, reviews, and experimental study designs in laboratory settings; and (3) studies without necessary data.
Data extraction
Two independent investigators (Jiali Wu and Yuzhu Zhang) extracted data from the included studies. The following summary data were included: last author, year of publication, air pollutant(s), statistical model, main results, study cohort, and diagnostic criteria for AMD. If articles reported the OR and P-value instead of the 95% CI, they were manually calculated.
Bias assessment
Two independent authors assessed the study risk using the Newcastle–Ottawa Scale (NOS). Cohort studies that scored ≥ 7, 4–6, and < 4 were considered to have a low, intermediate, and high risk, respectively, whereas cross-sectional studies that scored ≥ 7, 6, and ≤ 5 were considered to have a low, intermediate, and high risk, respectively.
Statistical analysis
Heterogeneity among studies was assessed using χ2-based Q-tests and inconsistency scores (I2). Heterogeneity was high, moderate, low, or none for I2 values ≥ 75%, 50–74%, 25–49%, and < 25%, respectively. Subsequently, random- and fixed-effect models were used based on the heterogeneity test results. The pooled ORs and 95% CIs were calculated to assess the risk of AMD due to ambient air pollution exposure. Regarding pooled outcome analyses, P < 0.05 was considered significant. All analyses were performed using RevMan 5.3. software (Review Manager, Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark).
Results
Study selection and characteristics
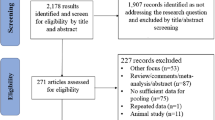
Figure 1 shows a flow diagram of the literature search. The initial search identified 358 articles from databases. After screening titles and abstracts combined with necessary full-text review, eight studies with 15,029,888 individuals were eligible for further analysis. Among these, four studies analysed PM2.5 [8, 13,14,15], and three examined NO2 [7, 13, 16] or O3 [16,17,18]. Two of the eight studies were longitudinal cohort studies [7, 8], while the rest were cross-sectional studies [13,14,15,16,17,18]. In the longitudinal cohort study that explored the association between the AMD risk and CO or NO2, 1,442 individuals among 39,819 AMD-free residents developed AMD during the study period of 11 years [7]. Moreover, 4,284,128 participants enrolled in the longitudinal cohort study evaluating the relationship between PM2.5 and AMD, and 12,095 AMD cases were identified during the 11-year follow-up [8].

Flow diagram of the included studies
The assessment and definition of AMD varied among studies. Among six studies applying standardised criteria for AMD diagnosis, grading was performed by at least two independent ophthalmologists to ensure the accuracy of diagnosis in three studies [8, 16, 17], whereas the other three did not describe the specific grading methodology [7, 14, 18]. Different from the standardised criteria, cases were diagnosed based on medical record review or self-reporting in two studies [13, 15]. Two AMD stages (early and late) were analysed separately in one study [16]. One study assessed AMD in patients with and without visual impairment [15]. One study explored the relationship of air pollution exposure with exudative and non-exudative AMD [18].
Table 1 summarizes the results of the individual studies in this meta-analysis. Liang et al. presented a single-pollutant model, proposing an increased risk of AMD among those exposed to the highest exposure quartile of CO (HR = 1.84; 95% CI: 1.57–2.15) and NO2 (HR = 1.91; 95% CI: 1.64–2.23). The risk did not increase in the second or third quartiles, indicating that moderate exposure did not lead to AMD [7]. Second, Freeman et al. reported that those exposed to higher PM2.5 levels were more likely to develop visually impaired AMD, as indicated by a single-pollutant regression model (OR = 1.52; 95% CI: 1.10–2.09). However, in a multipollutant model, higher exposure to PM2.5 merely showed a borderline association with visual impairment in AMD (OR = 1.41; 95% CI: 0.96–2.08, P = 0.08) [15]. In addition, single-pollutant model findings by Patel et al. demonstrated increased odds of AMD among participants exposed to higher levels of PM2.5 (OR = 1.08; 95% CI: 1.01–1.16). However, they did not find an association between exposure to PM10 (OR = 0.94; 95% CI: 0.86–1.02) or NO2 (OR = 0.99; 95% CI: 0.91–1.08) and AMD [13]. Furthermore, Choi et al. modelled air pollution within administrative division units, which suggested that NO2 (OR = 1.24; 95% CI: 1.05–1.46) and CO (OR = 1.22; 95% CI: 1.09–1.38) were risk factors for AMD, but O3 was associated with a decreased prevalence of AMD (OR = 0.8; 95% CI: 0.70–0.92). When air pollution was modelled as local/town units, the associations were slightly diminished. Besides, the study showed that higher levels of CO exposure led to higher prevalence of AMD [16]. However, the findings by Manookin et al., which were diametrically different from those by Choi et al., revealed that O3 was the only air pollution that statistically significant associated with any AMD (OR = 1.011; 95% CI: 1.003–1.019). It was demonstrated that NO2, SO2, CO and PM2.5 did not increase the AMD risk, whereas the exact effect size of them was not reported [18]. Both Hwang et al. and Yan et al. found a significant positive association between AMD and higher PM2.5 levels (HR = 1.19; 95% CI: 1.13–1.25 and OR = 2.602; 95% CI: 1.516–4.468, respectively) [8, 14]. Recently, multipollutant model findings by Sun et al. have revealed that the AMD risk was on a monotonic increasing trend with higher O3 concentration; the harmful effect increased rapidly after reaching a turning point of 110 μg/m3 (OR = 1.15; 95% CI: 1.13–1.16 and OR = 1.66; 95% CI: 1.63–1.69, respectively) increase [17]. Based on the results above, most studies revealed that higher concentrations of air pollution increased the AMD risk. However, no studies examined the correlation between the AMD risk and the exposure length.
Quantitative synthesis
We used the data of single-pollutant models for effect estimates. Two articles calculated and divided air pollution concentrations into four quartiles; we used the data of the highest quartile in the meta-analysis [7, 14]. According to quantitative methods in the review of epidemiologic articles, we ignored the distinctions among the HRs and ORs and calculated the pooled OR [19].
Figure 2 illustrates the association between PM2.5 and AMD; the pooled OR was 1.16 (95% CI: 1.11–1.21, I2 = 82%, P = 0.0009). Figure 3 shows a forest plot of the outcomes of three studies on the relationship between NO2 and AMD; the pooled OR was 1.17 (95% CI: 1.09–1.25, I2 = 96%, P < 0.00001). Figure 4 illustrates the relationship between O3 and AMD; the pooled OR was 1.06 (95% CI: 1.05–1.07, I2 = 100%, P < 0.00001). All results demonstrated a positive relationship between ambient air pollution and AMD, as well as indicated high heterogeneity.

Forest plot of the association between PM2.5 and AMD risk. The pooled OR is 1.16 (95% CI: 1.11–1.21, I2 = 82%, P = 0.0009), demonstrating a positive relationship between PM2.5 and AMD. Abbreviations: PM2.5, particulate matter less than 2.5 μm in diameter; AMD, age-related macular degeneration; OR, odds ratio; CI, confidence interval; I2, inconsistency score

Forest plot of the association between NO2 and AMD risk. The pooled OR is 1.17 (95% CI: 1.09–1.25, I2 = 96%, P < 0.00001), indicating a positive relationship between NO2 and AMD. Abbreviations: NO2, nitrogen dioxide; AMD, age-related macular degeneration; OR, odds ratio; CI, confidence interval; I2, inconsistency score

Forest plot of the association between O3 and AMD risk. The pooled OR is 1.06 (95% CI: 1.05–1.07, I2 = 100%, P < 0.00001), indicating a positive relationship between O3 and AMD. Abbreviations: O3, ozone; AMD, age-related macular degeneration; OR, odds ratio; CI, confidence interval; I2, inconsistency score
Evidence evaluation
Due to the small number of studies eligible for analysis, a statistical evaluation of publication bias was not feasible [20]. NOS was used to assess the quality of the included studies (Additional file 1); one study was classified as having moderate quality [15], whereas the others were classified as having high quality [7, 8, 13, 14, 16,17,18].
Discussion
AMD is a progressive retinal disease associated with photoreceptor atrophy and degeneration of the retinal pigment epithelium with a high prevalence and limited therapeutic benefits [4, 5, 21, 22]. The mechanisms underlying AMD are multifactorial. Smoking is a detrimental factor for AMD [23, 24]. Thus, air pollutants, to which the outer eye segment is directly exposed, might also be potential risk factors for eye diseases. Previous studies have shown that air pollution has detrimental effects on ocular surface and increases the risk of dry eye disease and allergic conjunctivitis [25,26,27]. Recently, researchers have suggested that air pollution may also affect the inner eye segment. The relationships between air pollution and AMD, glaucoma, cataract, and diabetic retinopathy have also been investigated [28,29,30,31,32,33]. However, the results remain inconclusive. Therefore, we reviewed the existing studies and performed a meta-analysis to clarify this relationship. Notably, various studies have relatively consistently demonstrated a correlation between AMD and PM2.5. However, the results of individual studies exploring the exact association between AMD and NO2 or O3 are contradictory. Our meta-analysis indicated that three air pollutants increased the risk of AMD. Merely one study explored the relationship between SO2 and AMD. Additionally, two studies on the association between CO and AMD showed consistent findings that CO increased the AMD risk. For the reasons above, we did not analyse the association between the AMD risk and SO2 or CO.
Several potential mechanisms could explain these associations. As chemical components of air pollution, CO, NO2, O3, SO2, and PM2.5 share a common biological pathway known to induce oxidative stress and inflammation, which are recognised as AMD risk factors [34, 35]. Moreover, animal studies have demonstrated that PM2.5 can impair microvascular function [36]. In the eye, choroidal microcirculation deterioration plays a critical role in AMD [37]. Chua et al. also proposed that exposure to PM2.5 is associated with adverse retinal structural features, which may lead to AMD [13, 38]. In addition, PM2.5 can cause neurodegenerative diseases, including reduced cognitive function [39, 40], accelerated cognitive decline [41], Parkinson’s disease, and Alzheimer’s dementia [42]. Given that AMD is a neurodegenerative disease, these studies further justify the plausibility of a correlation between AMD and air pollution.
It should be noted that meterological variables have a significant effect on changes in air pollution. Yan et al. reported that combined exposure to PM2.5 and atmospheric pressure remarkably increased the risk of AMD, while temperature and humidity acted a weakly antagonistic effect on AMD [14]. Higher temperature is known to cause lower relative humidity. Moreover, both air temperature and atmospheric pressure affect the distribution and concentration of PM2.5 [14, 43]. At present, limited studies elucidate the joint effects of meterological factors and ambient air pollution on AMD. Therefore, further studies are needed to clarify this correlation.
Our meta-analysis has certain limitations. First, only a few studies were eligible for inclusion owing to the novelty of this topic. However, most of the included studies had large sample sizes and all were considered credible. Second, the standard definition of AMD was inconsistent among the studies. In addition, the measurement variability of the exposure assessment and the quantitative differences of the exposure extent could bias our findings. Moreover, we used the data of the highest quartile of two articles in the meta analysis and did not standardize the effect size across the studies. The small amount of studies for every air contaminant made subgroup analysis by the exposure level difficult. Finally, other pollutants can affect single-pollutant models. Multipollutant models are less likely to be affected by confounding factors but may be susceptible to other biases.
Conclusions
The current evidence suggests that ambient air pollutants, such as PM2.5, NO2, and O3, detrimentally affect AMD. Extensive studies are urgently required to investigate additional air pollution and their influence on AMD or other ocular diseases. Further strategies for reducing ambient air pollution exposure are essential for public health, which may ultimately mitigate AMD.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AMD:
-
Age-related macular degeneration
- CI:
-
Confidence interval
- CO:
-
Carbon monoxide
- HR:
-
Hazard ratio
- I2 :
-
Inconsistency score
- NO2 :
-
Nitrogen dioxide
- NOS:
-
Newcastle–Ottawa Scale
- OR:
-
Odds ratio
- O3 :
-
Ozone
- PM2.5 :
-
Particulate matter less than 2.5 μm in diameter
- PM10 :
-
Particulate matter less than 10 μm in diameter
- SO2 :
-
Sulphur dioxide
References
Apte RS. Age-related macular degeneration. N Engl J Med. 2021;385:539–47.
Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. Lancet. 2018;392:1147–59.
Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8.
Wong WL, Su X, Li X, Cheung CM, Klein R, Cheng CY, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2:e106–16.
Ammar MJ, Hsu J, Chiang A, Ho AC, Regillo CD. Age-related macular degeneration therapy: a review. Curr Opin Ophthalmol. 2020;31:215–21.
Fleckenstein M, Keenan TDL, Guymer RH, Chakravarthy U, Schmitz-Valckenberg S, Klaver CC, et al. Age-related macular degeneration. Nat Rev Dis Primers. 2021;7:31.
Chang KH, Hsu PY, Lin CJ, Lin CL, Juo SH, Liang CL. Traffic-related air pollutants increase the risk for age-related macular degeneration. J Investig Med. 2019;67:1076–81.
Liang CL, Wang CM, Jung CR, Chang YC, Lin CJ, Lin YT, et al. Fine particulate matter measured by satellites predicts the risk of age-related macular degeneration in a longitudinal cohort study. Environ Sci Pollut Res Int. 2022;29:51942–50.
Goshua A, Akdis CA, Nadeau KC. World health organization global air quality guideline recommendations: executive summary. Allergy. 2022;77:1955–60.
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet. 2017;389:1907–18.
Christiani DC. Ambient air pollution and lung cancer: nature and nurture. Am J Respir Crit Care Med. 2021;204:752–3.
Mannucci PM, Harari S, Franchini M. Novel evidence for a greater burden of ambient air pollution on cardiovascular disease. Haematologica. 2019;104:2349–57.
Chua SYL, Warwick A, Peto T, Balaskas K, Moore AT, Reisman C, et al. Association of ambient air pollution with age-related macular degeneration and retinal thickness in UK Biobank. Br J Ophthalmol. 2022;106:705–11.
He J, Liu Y, Zhang A, Liu Q, Yang X, Sun N, et al. Joint effects of meteorological factors and PM2.5 on age-related macular degeneration: a national cross-sectional study in China. Environ Health Prev Med. 2023;28:3.
Grant A, Leung G, Aubin MJ, Kergoat MJ, Li G, Freeman EE. Fine particulate matter and age-related eye disease: the Canadian longitudinal study on aging. Invest Ophthalmol Vis Sci. 2021;62:7.
Ju MJ, Kim J, Park SK, Kim DH, Choi YH. Long-term exposure to ambient air pollutants and age-related macular degeneration in middle-aged and older adults. Environ Res. 2022;204: 111953.
Jia H, Guo Y, Luo H, Meng X, Zhang L, Yu K, et al. Association of long-term ozone air pollution and age-related macular degeneration in older Chinese population. Sci Total Environ. 2024;912: 169145.
Hunt MS, Chee YE, Saraf SS, Chew EY, Lee CS, Lee AY, et al. Association of environmental factors with age-related macular degeneration using the intelligent research in sight registry. Ophthalmol Sci. 2022;2(4):100195.
Greenland S. Quantitative methods in the review of epidemiologic literature. Epidemiol Rev. 1987;9:1–30.
Grant A, Leung G, Freeman EE. Ambient air pollution and age-related eye disease: A systematic review and meta-analysis. Invest Ophthalmol Vis Sci. 2022;63:17.
Feigl B. Age-related maculopathy-linking aetiology and pathophysiological changes to the ischaemia hypothesis. Prog Retin Eye Res. 2009;28:63–86.
Stahl A. The diagnosis and treatment of age-related macular degeneration. Dtsch Arztebl Int. 2020;117:513–20.
Saunier V, Merle BMJ, Delyfer MN, Cougnard-Grégoire A, Rougier MB, Amouyel P, et al. Incidence of and risk factors associated with age-related macular degeneration: four-year follow-up from the ALIENOR Study. JAMA Ophthalmol. 2018;136:473–81.
Wang Y, Zhong Y, Zhang L, Wu Q, Tham Y, Rim TH, et al. Global incidence, progression, and risk factors of age-related macular degeneration and projection of disease statistics in 30 years: a modeling study. Gerontology. 2022;68:721–35.
Mo Z, Fu Q, Lyu D, Zhang L, Qin Z, Tang Q, et al. Impacts of air pollution on dry eye disease among residents in Hangzhou, China: a case-crossover study. Environ Pollut. 2019;246:183–9.
Hwang SH, Choi YH, Paik HJ, Wee WR, Kim MK, Kim DH. Potential importance of ozone in the association between outdoor air pollution and dry eye disease in South Korea. JAMA Ophthalmol. 2016;134:503–10.
Lu CW, Fu J, Liu XF, Chen WW, Hao JL, Li XL, et al. Air pollution and meteorological conditions significantly contribute to the worsening of allergic conjunctivitis: a regional 20-city, 5-year study in Northeast China. Light Sci Appl. 2021;10:190.
Sun HY, Luo CW, Chiang YW, Yeh KL, Li YC, Ho YC, et al. Association between PM2.5 exposure level and primary open-angle glaucoma in Taiwanese adults: a nested case-control study. Int J Environ Res Public Health. 2021;18(4):1714.
Shan A, Chen X, Yang X, Yao B, Liang F, Yang Z, et al. Association between long-term exposure to fine particulate matter and diabetic retinopathy among diabetic patients: a national cross-sectional study in China. Environ Int. 2021;154: 106568.
Yang X, Yang Z, Liu Y, Chen X, Yao B, Liang F, et al. The association between long-term exposure to ambient fine particulate matter and glaucoma: a nation-wide epidemiological study among Chinese adults. Int J Hyg Environ Health. 2021;238: 113858.
Saha A, Kulkarni PK, Shah A, Patel M, Saiyed HN. Ocular morbidity and fuel use: an experience from India. Occup Environ Med. 2005;62:66–9.
Pokhrel AK, Bates MN, Shrestha SP, Bailey IL, Dimartino RB, Smith KR. Biomass stoves and lens opacity and cataract in Nepalese women. Optom Vis Sci. 2013;90:257–68.
Sehgal M, Rizwan SA, Krishnan A. Disease burden due to biomass cooking-fuel-related household air pollution among women in India. Glob Health Action. 2014;7:25326.
Riggs DW, Zafar N, Krishnasamy S, Yeager R, Rai SN, Bhatnagar A, et al. Exposure to airborne fine particulate matter is associated with impaired endothelial function and biomarkers of oxidative stress and inflammation. Environ Res. 2020;180: 108890.
Delfino RJ, Staimer N, Vaziri ND. Air pollution and circulating biomarkers of oxidative stress. Air Qual Atmos Health. 2011;4:37–52.
Nurkiewicz TR, Porter DW, Barger M, Castranova V, Boegehold MA. Particulate matter exposure impairs systemic microvascular endothelium-dependent dilation. Environ Health Perspect. 2004;112:1299–306.
Lipecz A, Miller L, Kovacs I, Czakó C, Csipo T, Baffi J, et al. Microvascular contributions to age-related macular degeneration: from mechanisms of choriocapillaris aging to novel interventions. Geroscience. 2019;41:813–45.
Chua SYL, Khawaja AP, Dick AD, Morgan J, Dhillon B, Lotery AJ, et al. Ambient air pollution associations with retinal morphology in the UK Biobank. Invest Ophthalmol Vis Sci. 2020;61:32.
Gatto NM, Henderson VW, Hodis HN, St John JA, Lurmann F, Chen JC, et al. Components of air pollution and cognitive function in middle-aged and older adults in Los Angeles. Neurotoxicology. 2014;40:1–7.
Ranft U, Schikowski T, Sugiri D, Krutmann J, Krämer U. Long-term exposure to traffic-related particulate matter impairs cognitive function in the elderly. Environ Res. 2009;109:1004–11.
Weuve J, Puett RC, Schwartz J, Yanosky JD, Laden F, Grodstein F. Exposure to particulate air pollution and cognitive decline in older women. Arch Intern Med. 2012;172:219–27.
Kioumourtzoglou MA, Schwartz JD, Weisskopf MG, Melly SJ, Wang Y, Dominici F, et al. Long-term PM2.5 exposure and neurological hospital admissions in the Northeastern United States. Environ Health Perspect. 2016;124:23–9.
Wang S, Gao J, Guo L, Nie X, Xiao X. Meteorological influences on spatiotemporal variation of PM2.5 concentrations in atmospheric pollution transmission channel cities of the Beijing-Tianjin-Hebei region, China. Int J Environ Res Public Health. 2022;19:1607.
Acknowledgements
We thank all authors for their contributions to this article.
Funding
Chinese National Nature Science Foundation (Project number 81600778).
Author information
Authors and Affiliations
Contributions
Jiali Wu contributed to the analysis design, literature search, literature reviews, and data analysis. Yuzhu Zhang contributed to the literature search, literature reviews, data analysis, and drafting of the manuscript. Xian Xu, Yuzhu Zhang, and Jiali Wu reviewed the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Newcastle-Ottawa Scale for assessing the quality of studies in the meta-analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, J., Zhang, Y. & Xu, X. Association between ambient air pollution and age-related macular degeneration: a meta-analysis. BMC Ophthalmol 24, 202 (2024). https://doi.org/10.1186/s12886-024-03465-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-024-03465-y