
Abstract
Purpose
Quantitative analysis of vitreous inflammatory and angiogenic factors from patients with proliferative diabetic retinopathy (PDR) or diabetic macular edema (DME).
Materials and methods
Collection of undiluted vitreous samples from 20 diabetic patients: 13 with proliferative diabetic retinopathy (PDR) and 7 with diabetic macular edema (DME). DME patients had suboptimal response to anti-VEGF treatment. Samples from 11 control patients, with vitreomacular interface pathology such as idiopathic epiretinal membrane (iERM) (n = 4), vitreomacular traction syndrome (VMT) (n = 3) and full thickness macular hole (FTMH) (n = 3), were also collected. The levels of IL1b, IL6, IL8, IL27, TNFα, ICAM-1, VCAM, MCP-1, VEGFA and LCN2 were measured using cytometry flow analysis. Median values were compared with Mann–Whitney test since the distributions were skewed. Statistical analysis was performed with the Statistical Package for Social Sciences software (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.).
Results
The median concentration of LCN2, IL6, IL8, IL1b, IL27, ICAM, VCAM-1, MCP-1, TNFa and VEGFA was higher in PDR patients than in controls. Similarly, the median concentration of LCN2, IL6, IL8, IL27, ICAM, VCAM-1, TNFa and VEGFA was higher in DME patients than in controls. In particular, median LCN2 concentration in diabetic patients was 5,711 pg/ml (interquartile range [IR] = 2,534), while in controls was 2,586 pg/ml (IR = 2,345). Moreover, median LCN2 was 6,534 pg/ml in the DME group (IR = 6,850) and 4,785 pg/ml in the PDR group (IR = 2,608), (p = 0.025).
Conclusion
Various inflammatory and angiogenic factors are involved in the pathophysiology of PDR and DME. Elevated vitreous levels of LCN2 in PDR and especially in DME patients reveal a potential pathogenic association. More extended studies could verify LCN2 as an alternative therapeutic target.
Similar content being viewed by others


Introduction
Diabetes mellitus (DM) is a metabolic systemic disease affecting 422 million people worldwide [1]. Proliferative diabetic retinopathy (PDR) and diabetic macular edema (DME) are serious, vision threatening complications of DM [2]. There are approximately 17 million people with PDR and 28 million people with DME worldwide [3]. In the next years, the prevalence of these complications is expected to increase [4].
Both PDR and DME are considered consequences from diabetic retinopathy (DR), which is the result from a consecutive process between vascular alterations and inflammation [5,6,7,8,9].
Anti-vascular endothelial growth factor (anti-VEGF) agents remain the gold standard treatment for DME patients [10]. Yet, 30% of DME patients show suboptimal response with anti-VEGF therapy [11]. In clinical practice, the inflammatory component of DME can be addressed with steroids, such as dexamethasone implants [12,13,14]. Regarding PDR patients, recent studies have presented very favorable results with anti-VEGF agents (Protocol S, Clarity Study) [15, 16]. Yet, research is focusing on various factors as potential therapeutic targets for DME and PDR [7, 8, 17, 18].
Lipocalin-2 (LCN2), also described as neutrophil gelatinase-associated lipocalin (NGAL) [19], is a glycoprotein with a pleotropic action in different processes such as metabolism and inflammation [20]. It is also regarded as biomarker in various diseases, such as multiple sclerosis, acute kidney injury, lupus nephritis, cardiovascular disease and others [20]. Elevated serum LCN2 levels have been identified on patients with type 2 DM [21]. Serum LCN2 levels are also positively correlated with DR in these patients [22]. The role of LCN2 in neurological complications of diabetes has also been studied [23]. We have previously found a significant correlation between vitreous LCN2 and proliferative vitreoretinopathy (PVR) grade [24]. Recent data have shown upregulated vitreous NGAL in ocular sarcoidosis [25]. A significant increase of vitreous LCN2 and a correlation with VEGF has also been found in PDR patients [26]. Yet, the role of LCN2 in DME has not been studied thus far. The aim of our study was to investigate a potential association of LCN2 with DME or PDR in conjunction with other inflammatory and angiogenic factors.
Materials and methods
Study design
This study was conducted at the University Hospital of Ioannina, Greece, between March and September 2019. Approval was received from the hospital’s ethics committee “Scientific Board” (March 2019). All patients were recruited and examined at the University Ophthalmology Clinic. Written informed consent was obtained from each patient during the recruitment period and before the operation. The study is adherent to the tenets of the Declaration of Helsinki.
In this study, we have collected vitreous samples from 20 diabetic and 10 control patients. From diabetic patients, 13 had PDR and 7 DME. The control group included 4 patients with idiopathic epiretinal membrane (iERM), 3 with vitreomacular traction syndrome (VMT) and 3 with full-thickness macular hole (FTMH). In all patients, complete ophthalmic examination, including optical coherence tomography (OCT) and fluorescein angiography (FA) was performed. All DME patients had previously received anti-VEGF treatment (Ranibizumab or Aflibercept) with a suboptimal response. These eyes had OCT-central subfield thickness (OCT-CST) of 250 μm for a period of 24 weeks and received at least 4 intravitreal anti-VEGF injections [27]. We did not notice anatomical improvement after switching between Ranibizumab and Aflibercept. No significant vitreoretinal interface pathology (such as ERM) was confirmed by OCT in DME cases. Fundoscopy revealed no tractional component in all diabetic patients, while in cases of vitreous hemorrhage (VH) coexistence, ultrasonography (US) was performed in order to exclude any tractional retinal detachment. Apart from panretinal photocoagulation (PRP), no other treatment had been applied to PDR patients. Diabetic patients were divided in two groups (PDR and DME) because they have received different treatment (intravitreal injections or PRP). DME patients did not had proliferative disease. The exclusion criteria included ocular trauma history, prior ophthalmic surgery other than phacoemulsification, ocular or systemic inflammation and malignancy.
Each operation was performed by the same vitreoretinal surgeon and included standard 25G pars plana vitrectomy with Alcon Constellation system. Each sample (0.5 ml of core vitreous) was collected before opening the infusion cannula and stored at -80 ̊C. Then, all samples were analyzed with cytometry flow for the quantification of IL1b, IL6, IL8, IL27, TNFα, ICAM-1, VCAM, MCP-1, VEGFA and LCN2 (NGAL). According to literature, these factors are implicated in the pathophysiology of PDR or DME development [26, 28,29,30], thus a potential correlation with LCN2 concentration could highlight an inflammatory or angiogenic pathway association. In DME patients, vitrectomy was performed in order to achieve better oxygenation and removal of the angiogenic and inflammatory factors from the macular area [31]. Moreover, in order to achieve complete vitreous cortex removal [31] and avoid postoperative ERM development [32] peeling of the internal limiting membrane (ILM) using brilliant blue dye was performed. No postoperative complications were noticed in all cases.
Cytometry flow analysis
Vitreous samples were tested with the AimPlex multiplex assay in a FACSCalibur (Becton–Dickinson) cytometer. Results were analyzed with the CellQuest software (Becton–Dickinson). The technology of AimPlex multiple analysis works by using multiple populations of beads that differentiate in size and level of fluorescence intensity. In this way, multiple molecules can be measured during the same reaction. Cytometric bead array is based on the same principle as sandwich ELISA. Every bead population is conjugated with a specific antibody, which can bind with the target analyte (cytokine).
Concentrations were obtained from the measured fluorescent intensity after comparison with the fluorescent signal of a standard curve. The standard curve corresponds to 8 measurements from a solution with a known analyte concentration (cytokine) (Fig. 1). Results were expressed as picograms per milliliter (pg/ml). The first step of the test included the incubation of the antibody bearing beads with the antigen for 60 min, which was followed by the biotinylated antibody incubation for 30 min. The last step included the streptavidin phycoerythrin incubation for 20 min. Figure 2 illustrates the dot-plot diagrams of the measured factors, from a DME case.

Standard curves of LCN2 (a) and VEGFA (b). The horizontal axis corresponds to the concentration in pg/ml and the vertical axis the mean fluorescence intensity (MFI)

Dot-plot diagrams of the measured factors from a DME case. The horizontal axis (FL2) represents the fluorescent intensity related to the concentration of each measured factor (IL1b, IL6, IL8, I-CAM, V-CAM, MCP-1, TNFa, VEGF, NGAL) framed in a box. The vertical axis (FL4) represents the fluorescent intensity serving for distinguishing each factor, by allocating them on different sites in the plot
Statistical analysis
Continuous variables are presented as mean, standard deviation, median, interquartile range, minimum value and maximum value, while categorical variables are presented as percentages (frequencies). Continuous variables did not follow the normal distribution and thus nonparametric methods were used. For continuous variables, differences between the two groups were evaluated with Mann–Whitney U test. Variability between the DR and the control group in terms of age and gender was assessed with independent-samples t-test and chi-square test respectively. A two tailed p-value of less than 0.05 was considered statistically significant. Statistical analysis was performed with the Statistical Package for Social Sciences software (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.).
Results
There were no differences in age and gender between diabetic patients and controls. In particular, mean age in the diabetic patients group was 67.6 years (standard deviation [SD] = 11.9, minimum value = 33, maximum value = 87) while in the control group was 68.4 years (SD = 10.5, minimum value = 51, maximum value = 84) (t = 0.2, p = 0.9). Mean age for the DME group was 70.6 years (SD = 8.9, minimum value = 57, maximum value = 87) while for the PDR group was 65.1 (SD = 13.7, minimum value = 33, maximum value = 86). In diabetic patients group 55% (n = 11) were males, while 30% (n = 3) of controls were males (x2 = 1.7, p = 0.26). Mean HbA1c for DME was 7.4% (SD = 2.1%, median = 6.8%, minimum value = 5.1%, maximum value = 12%), while for PDR was 9.5% (SD = 1.6%, median = 10%, minimum value = 7%, maximum value = 12%), (t = 2.5, p = 0.02).
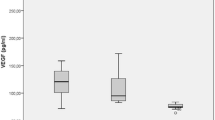
Relations between measured factors and patients are shown in Table 1. The median concentration of LCN2, IL6, IL8, IL1b, IL27, ICAM, VCAM-1, MCP-1, TNFa and VEGFA was higher in PDR patients than in controls. Also, the median concentration of LCN2, IL6, IL8, IL27, ICAM, VCAM-1, TNFa and VEGFA was higher in DME patients than in controls. In particular, median LCN2 concentration in in diabetic patients was 5,711 pg/ml (interquartile range [IR] = 2,534), while in the controls was 2,586 pg/ml (IR = 2,345). Also, median LCN2 was 6,534 pg/ml in the DME group (IR = 6,850) and 4,785 pg/ml in the PDR group (IR = 2,608). LCN2 levels of the patients and the controls are shown in Fig. 3. There were no outliers.

LCN2 levels of the controls, DME and PDR patients
Median LCN2 was higher in DME group than PDR group (p = 0.025), while median IL8 was higher in PDR group than DME group (p = 0.02). Medians’ LCN2 difference between DME and controls (3,948) was almost twice higher than medians’ LCN2 difference between PDR and controls (2,199). Also, medians’ IL8 difference between PDR and controls (594.5) was almost three times higher than medians’ IL8 difference between DME and controls (207.7).
Discussion
In this study, we found elevated LCN2 levels in the vitreous of diabetic patients. Median LCN2 concentration was higher in PDR and markedly higher in DME group as compared to controls. To our knowledge, this observation has not been reported to the literature so far.
Numerous angiogenic and inflammatory factors are implicated in the pathogenesis of DR, and therefore in DME and PDR [5, 6, 8]. The NF-κβ pathway is a key element in the development of vascular complications caused in DM and DR and it is related to the expression of IL1b, IL6, IL8, TNFa, I-CAM and MCP-1 [33]. In a recent study, it has been proposed that intravitreal LCN2 can suppress ocular inflammation (in rat models) by inhibiting the activation of NF-κβ pathway [34]. The anti-inflammatory role of LCN2 in macrophages and NF-κβ pathway has also been reported before [35].
The vascular alterations in DR are accompanied by blood retinal barrier (BRB) breakdown leading to DME development [36]. The BRB breakdown can develop, due to the junctional protein damage and the vascular endothelial cell dysfunction [37]. The role of LCN2 in vascular endothelial cell function has been studied in the cerebrovascular system [38]. It has been proposed that LCN2 might reduce the damage to endothelial junctional proteins (ZO-1, VE-cadherin) after ischemic brain stroke, acting as an endogenous ‘help me signal’ and thus maintaining the blood brain barrier (BBB) integrity [38]. On the other hand, LCN2 can also promote angiogenesis [39, 40]. For this reason, the specific role of LCN2 in both PDR and DME needs to be elucidated with further studies; in fact, its role in modulating pro- and anti-inflammatory responses is still under research [41].
Matrix Metalloproteinase-9 (MMP-9) has a key role in the pathogenesis of DR and progression to PDR [42,43,44,45,46]. MMP-9 also correlates both with the DME development [47] and the structural damage caused by chronic DME [47]. At the same time, LCN2 modulates the activity of MMP-9 [48,49,50,51], highlighting the rationale for further investigation in this field.
We have also found a significant elevation of IL27 in DME and PDR patients as compared to controls. Elevated IL27 levels have been previously measured in the aqueous humor of patients with diabetic retinopathy [29]. The anti-inflammatory role of IL27 in ocular inflammation has also been described [52]. VEGFA is a potent angiogenic factor, which can also act as a chemoattractant to macrophages and granulocytes, or can induce vasodilation [53]. Q Zhang et al. reported that IL27 can suppress the VEGFA production in macrophages on patients with diabetic retinopathy [54].
To date, there is limited evidence concerning the role of LCN2 in DM. Conceivably, this information is be considered relevant for clinical practice, as this glycoprotein could serve as a predicting factor for the prognostication in diabetic patients and as a potential therapeutic target. The aforementioned parameters along with our observation concerning increased levels of LCN2 in DME may add strength to our study. In any case, our study contributes to a little-studied issue that warrants further investigation.
Undoubtedly, the results of the present study should be interpreted with certain limitations. Firstly, our study sample consists of a small number of recruited patients. However, this sample size enabled significant differences. The patients with DME without concurrent vitreoretinal pathology (such as ERM) and indication for vitrectomy are rare cases. Thus, even with few recruited patients, this study provides very useful information for clinical practice. Undoubtedly, the small sample does not allow us to conclude if the LCN2 concentration differences can be attributed to the different treatment strategies in each group (either PRP in PDR or anti-VEGF in DME). Another limitation concerns the levels of VEGFA at the patients with DME. All patients with DME had received anti-VEGF treatment before. This is because one of the study aims was to investigate alternative therapeutic targets in cases that are refractory to anti-VEGF treatment. Lastly, caution is needed in the interpretation of results concerning the quantification of VEGF (with antibody based assays) in the presence of antibody-based anti-VEGF agents, such as Ranibizumab or Aflibercept [55, 56].
In conclusion, we have found elevated vitreous LCN2 levels in patients with PDR and in patients with DME refractory to anti-VEGF treatment. These findings are accentuating the role of LCN2 in the pathogenesis of PDR and DME, adding further information to previous studies. Larger longitudinal studies are needed, in order to determine the significance of LCN2 as biomarker or therapeutic target.
Availability of data and materials
The datasets used and analyzed in the current study are available from the corresponding author on reasonable request.
References
WHO. https://www.who.int/health-topics/diabetes#tab=tab_1, 2020.
Wong TY, Sun J, Kawasaki R, et al. Guidelines on Diabetic Eye Care: The International Council of Ophthalmology Recommendations for Screening, Follow-up, Referral, and Treatment Based on Resource Settings. Ophthalmology. 2018;125:1608–22. Research Support, Non-U.S. Gov't Review 2018/05/20.
Yau JW, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes care. 2012;35:556–64. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't Review Systematic Review 2012/02/04.
Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis (Lond). 2015;2:17. Review 2015/11/26.
Rubsam A, Parikh S, Fort PE. Role of Inflammation in Diabetic Retinopathy. Int J Mol Sci. 2018;19:942. Review 2018/03/23.
Romero-Aroca P, Baget-Bernaldiz M, Pareja-Rios A, et al. Diabetic Macular Edema Pathophysiology: Vasogenic versus Inflammatory. J Diabetes Res. 2016;2016:2156273. Review 2016/10/21.
Barot M, Gokulgandhi MR, Patel S, et al. Microvascular complications and diabetic retinopathy: recent advances and future implications. Future Med Chem. 2013;5:301–14. Research Support, N.I.H., Extramural Review 2013/03/08.
Gologorsky D, Thanos A, Vavvas D. Therapeutic interventions against inflammatory and angiogenic mediators in proliferative diabetic retinopathy. Mediators Inflamm. 2012;2012:629452. Review 2012/10/03.
Adamis AP. Is diabetic retinopathy an inflammatory disease? Br J Ophthalmol. 2002;86:363–5. Editorial 2002/03/27.
Takamura Y, Ohkoshi K, Murata T. New Strategies for Treatment of Diabetic Macular Edema. J Ophthalmol. 2018;2018:4292154. Editorial 2018/09/14.
Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372:1193–203. Comparative Study Multicenter Study Randomized Controlled Trial Research Support, N.I.H., Extramural 2015/02/19.
Zur D, Iglicki M, Loewenstein A. The Role of Steroids in the Management of Diabetic Macular Edema. Ophthalmic Res. 2019;62:231–6. Review 2019/05/03.
Gillies MC, Lim LL, Campain A, et al. A randomized clinical trial of intravitreal bevacizumab versus intravitreal dexamethasone for diabetic macular edema: the BEVORDEX study. Ophthalmology. 2014;121:2473–81. Clinical Trial, Phase II Multicenter Study Randomized Controlled Trial Research Support, Non-U.S. Gov't 2014/08/27.
Dutra Medeiros M, Alkabes M, Nucci P. Effectiveness of the Dexamethasone Intravitreal Implant for Treatment of Patients with Diabetic Macular Oedema. Eur Endocrinol. 2014;10:111–6. Review 2014/08/01.
Sivaprasad S, Prevost AT, Vasconcelos JC, et al. Clinical efficacy of intravitreal aflibercept versus panretinal photocoagulation for best corrected visual acuity in patients with proliferative diabetic retinopathy at 52 weeks (CLARITY): a multicentre, single-blinded, randomised, controlled, phase 2b, non-inferiority trial. Lancet. 2017;389:2193–203. Clinical Trial, Phase II Comparative Study Multicenter Study Randomized Controlled Trial 2017/05/13.
Gross JG, Glassman AR, Jampol LM, et al. Panretinal Photocoagulation vs Intravitreous Ranibizumab for Proliferative Diabetic Retinopathy: A Randomized Clinical Trial. Jama. 2015;314:2137–46. Multicenter Study Randomized Controlled Trial Research Support, N.I.H., Extramural 2015/11/14.
Urias EA, Urias GA, Monickaraj F, et al. Novel therapeutic targets in diabetic macular edema: Beyond VEGF. Vision Res. 2017;139:221–7. Review 2017/10/11.
Safi SZ, Qvist R, Kumar S, et al. Molecular mechanisms of diabetic retinopathy, general preventive strategies, and novel therapeutic targets. BioMed Res Int. 2014;2014:801269. Research Support, Non-U.S. Gov't Review 2014/08/12.
Kjeldsen L, Cowland JB, Borregaard N. Human neutrophil gelatinase-associated lipocalin and homologous proteins in rat and mouse. Biochim Biophys Acta. 2000;1482:272–83. Research Support, Non-U.S. Gov't Review 2000/11/04.
Abella V, Scotece M, Conde J, et al. The potential of lipocalin-2/NGAL as biomarker for inflammatory and metabolic diseases. Biomarkers. 2015;20:565–71 Research Support, Non-U.S. Gov't Review 2015/12/17.
Elkhidir AE, Eltaher HB, Mohamed AO. Association of lipocalin-2 level, glycemic status and obesity in type 2 diabetes mellitus. BMC Res Notes. 2017;10:285. 2017/07/16.
Chung JO, Park SY, Cho DH, et al. Plasma neutrophil gelatinase-associated lipocalin levels are positively associated with diabetic retinopathy in patients with Type 2 diabetes. Diabet Med. 2016;33:1649–54. 2016/04/22.
Bhusal A, Lee WH, Suk K. Lipocalin-2 in Diabetic Complications of the Nervous System: Physiology, Pathology, and Beyond. Front Physiol. 2021;12(638112):20210205.
Batsos G, Christodoulou E, Vartholomatos G, et al. Vitreous levels of Lipocalin-2 on patients with primary rhegmatogenous retinal detachment. PLoS One. 2019;14:e0227266. 2020/01/01.
Moseley I. Interpreting the skull X-ray. Br J Hosp Med. 1987;37:340–8.
Wang H, Lou H, Li Y, et al. Elevated vitreous Lipocalin-2 levels of patients with proliferative diabetic retinopathy. BMC Ophthalmol. 2020;20(260):20200630.
Bressler SB, Ayala AR, Bressler NM, et al. Persistent Macular Thickening After Ranibizumab Treatment for Diabetic Macular Edema With Vision Impairment. JAMA Ophthalmol. 2016;134:278–85.
Deuchler S, Schubert R, Singh P, et al. Vitreous expression of cytokines and growth factors in patients with diabetic retinopathy-An investigation of their expression based on clinical diabetic retinopathy grade. PLoS One. 2021;16(e0248439):20210519.
Houssen ME, El-Hussiny MAB, El-Kannishy A, et al. Serum and aqueous humor concentrations of interleukin-27 in diabetic retinopathy patients. Int Ophthalmol. 2018;38(1817–1823):20170724.
Srividya G, Jain M, Mahalakshmi K, et al. A novel and less invasive technique to assess cytokine profile of vitreous in patients of diabetic macular oedema. Eye (Lond). 2018;32(820–829):20180105.
Bonnin S, Sandali O, Bonnel S, et al. Vitrectomy with internal limiting membrane peeling for tractional and nontractional diabetic macular edema: long-term results of a comparative study. Retina. 2015;35:921–8.
Ivastinovic D, Haas A, Weger M, et al. Vitrectomy for diabetic macular edema and the relevance of external limiting membrane. BMC Ophthalmol. 2021;21(334):20210915.
Suryavanshi SV, Kulkarni YA. NF-kappabeta: A Potential Target in the Management of Vascular Complications of Diabetes. Front Pharmacol. 2017;8:798. Review 2017/11/23.
Tang W, Ma J, Gu R, et al. Lipocalin 2 Suppresses Ocular Inflammation by Inhibiting the Activation of NF-kappabeta Pathway in Endotoxin-Induced Uveitis. Cell Physiol Biochem. 2018;46:375–88. 2018/03/29.
Guo H, Jin D, Chen X. Lipocalin 2 is a regulator of macrophage polarization and NF-kappaB/STAT3 pathway activation. Mol Endocrinol. 2014;28:1616–28. Research Support, N.I.H., Extramural 2014/08/16.
Bandello F, Lattanzio R, Zucchiatti I, et al. Pathophysiology and treatment of diabetic retinopathy. Acta diabetologica. 2013;50:1–20. Review 2013/01/02.
Diaz-Coranguez M, Ramos C, Antonetti DA. The inner blood-retinal barrier: Cellular basis and development. Vision research. 2017;139:123–37. Review 2017/06/18.
Du Y, Li W, Lin L, et al. Effects of lipocalin-2 on brain endothelial adhesion and permeability. PloS One. 2019;14:e0218965. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't 2019/07/04.
Wu L, Du Y, Lok J, et al. Lipocalin-2 enhances angiogenesis in rat brain endothelial cells via reactive oxygen species and iron-dependent mechanisms. J Neurochem. 2015;132(622–628):20150129.
Yang J, McNeish B, Butterfield C, et al. Lipocalin 2 is a novel regulator of angiogenesis in human breast cancer. FASEB J. 2013;27(45–50):20120914.
Ferreira AC, Da Mesquita S, Sousa JC, et al. From the periphery to the brain: Lipocalin-2, a friend or foe? Prog Neurobiol. 2015;131(120–136):20150706.
Kowluru RA, Zhong Q, Santos JM. Matrix metalloproteinases in diabetic retinopathy: potential role of MMP-9. Expert Opin Investig Drugs. 2012;21:797–805. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't Review 2012/04/24.
Mohammad G, Kowluru RA. Diabetic retinopathy and signaling mechanism for activation of matrix metalloproteinase-9. J Cell Physiol. 2012;227:1052–61. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't 2011/05/14.
Giebel SJ, Menicucci G, McGuire PG, et al. Matrix metalloproteinases in early diabetic retinopathy and their role in alteration of the blood-retinal barrier. Lab Invest. 2005;85:597–607 Research Support, N.I.H., Extramural Research Support, U.S. Gov't, P.H.S. 2005/02/16.
Lee CZ, Xue Z, Zhu Y, et al. Matrix metalloproteinase-9 inhibition attenuates vascular endothelial growth factor-induced intracerebral hemorrhage. Stroke. 2007;38:2563–8. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't 2007/08/04.
Navaratna D, McGuire PG, Menicucci G, et al. Proteolytic degradation of VE-cadherin alters the blood-retinal barrier in diabetes. Diabetes. 2007;56:2380–7. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't 2007/05/31.
Kwon JW, Choi JA, Jee D. Matrix Metalloproteinase-1 and Matrix Metalloproteinase-9 in the Aqueous Humor of Diabetic Macular Edema Patients. PloS One. 2016;11:e0159720. 2016/07/29.
Kobayashi T, Kim H, Liu X, et al. Matrix metalloproteinase-9 activates TGF-beta and stimulates fibroblast contraction of collagen gels. Am J Physiol Lung Cell Mol Physiol. 2014;306:L1006-1015. Research Support, N.I.H., Extramural Research Support, Non-U.S. Gov't 2014/04/08.
Hofmaier F, Hauck SM, Amann B, et al. Changes in matrix metalloproteinase network in a spontaneous autoimmune uveitis model. Invest Ophthalmol Vis Sci. 2011;52:2314–20. Research Support, Non-U.S. Gov't 2011/01/14.
Kubben FJ, Sier CF, Hawinkels LJ, et al. Clinical evidence for a protective role of lipocalin-2 against MMP-9 autodegradation and the impact for gastric cancer. Eur J Cancer. 2007;43:1869–76. 2007/07/03.
Yan L, Borregaard N, Kjeldsen L, et al. The high molecular weight urinary matrix metalloproteinase (MMP) activity is a complex of gelatinase B/MMP-9 and neutrophil gelatinase-associated lipocalin (NGAL). Modulation of MMP-9 activity by NGAL. J Biol Chem. 2001;276:37258–65. Research Support, Non-U.S. Gov't 2001/08/04.
Lee YS, Amadi-Obi A, Yu CR, et al. Retinal cells suppress intraocular inflammation (uveitis) through production of interleukin-27 and interleukin-10. Immunology. 2011;132:492–502. Research Support, N.I.H., Intramural 2011/02/08.
Bardach J. The influence of cleft lip repair on facial growth. The Cleft palate journal. 1990;27:76–8 . 1990/01/01.
Zhang Q, Cunha APD, Li S, et al. IL-27 regulates HIF-1alpha-mediated VEGFA response in macrophages of diabetic retinopathy patients and healthy individuals. Cytokine. 2019;113:238–47. Clinical Trial Comparative Study 2018/07/17.
Sumner G, Georgaros C, Rafique A, et al. Anti-VEGF drug interference with VEGF quantitation in the R&D systems human quantikine VEGF ELISA kit. Bioanalysis. 2019;11:381–92. 2019/03/21.
Takahashi H, Nomura Y, Nishida J, et al. Vascular Endothelial Growth Factor (VEGF) Concentration Is Underestimated by Enzyme-Linked Immunosorbent Assay in the Presence of Anti-VEGF Drugs. Invest Ophthalmol Vis Sci. 2016;57:462–6. Research Support, Non-U.S. Gov't 2016/02/13.
Acknowledgements
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Funding
No funding or sponsorship was received for this study.
Author information
Authors and Affiliations
Contributions
GB collected and interpreted data, drafted and wrote the main manuscript. EC collected and interpreted data, contributed to writing and reviewed the manuscript. EEC contributed to writing and reviewed the manuscript. PG made the statistical analysis, contributed to writing and reviewing the manuscript. AK interpreted data and reviewed the manuscript. LL interpreted data and reviewed the manuscript. MS interpreted data, reviewed the manuscript, conceived and supervised the study. All authors have read, critically revised and approved the current version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted at the Department of Ophthalmology of the University Hospital of Ioannina, Greece after receiving approval from the institutional ethics committee and adhered to the tenets of the declaration of Helsinki. Written informed consent was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Batsos, G., Christodoulou, E., Christou, E.E. et al. Vitreous inflammatory and angiogenic factors on patients with proliferative diabetic retinopathy or diabetic macular edema: the role of Lipocalin2. BMC Ophthalmol 22, 496 (2022). https://doi.org/10.1186/s12886-022-02733-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-022-02733-z