
Abstract
Background
Cancer stage at diagnosis is an important prognostic indicator for patient outcomes, with detection at later stages associated with increased mortality and morbidity. The impact of cancer stage on patient-reported outcomes is poorly understood. This research aimed to understand symptom burden and health related quality of life (HRQoL) impact by cancer stage for ten cancer types: 1) ovarian, 2) lung, 3) pancreatic, 4) esophageal, 5) stomach, 6) head and neck, 7) colorectal, 8) anal, 9) cervical, and 10) liver and bile duct.
Methods
Ten narrative literature reviews were performed to identify and collate published literature on patient burden at different stages of disease progression. Literature searches were conducted using an AI-assisted platform to identify relevant articles published in the last five (2017–2022) or ten years (2012–2022) where articles were limited. Conference abstracts were searched for the last two years (2020–2022). The geographic scope was limited to the United States, Canada, Europe, and global studies, and only journal articles written in English were included.
Results
A total of 26 studies with results stratified by cancer stage at diagnosis (and before treatment) were selected for the cancer types of lung, pancreatic, esophageal, stomach, head and neck, colorectal, anal, and cervical cancers. Two cancer types, ovarian cancer, and liver and bile duct cancer did not return any search results with outcomes stratified by disease stage. A general trend was observed for worse patient-reported outcomes in patients with cancer diagnosed at an advanced stage of disease compared with diagnosis at an earlier stage. Advanced disease stage was associated with greater symptom impact including general physical impairments such as pain, fatigue, and interference with functioning, as well as disease/region-specific symptom burden. Poorer HRQoL was also associated with advanced disease with commonly reported symptoms including anxiety and depression.
Conclusions
Overall, the general trend for greater symptom burden and poorer HRQoL seen in late stage versus early-stage disease across the included cancer types supports the importance for early diagnosis and treatment to improve patient survival and decrease negative impacts on disease burden and HRQoL.
Similar content being viewed by others


Introduction
Cancer stage at diagnosis is an important prognostic indicator for patient outcomes, with detection at later stages associated with increased mortality and morbidity. An estimated 2,001,140 new cancer cases will occur in the United States in 2024 along with 611,720 cancer deaths [1]. Many cancers are diagnosed during late (distant) stage including 55% of ovarian cancer cases, 53% of lung cancer cases, 51% of pancreatic cancer cases, 38% of esophageal cancer cases, and 36% of stomach cancer cases [2]. Stage at diagnosis is an important predictor both for treatment efficacy and survival, but diagnosis times vary by cancer type [2].
The World Health Organization identified two strategies which allow for more effective cancer treatment: 1) diagnosing symptomatic cancer as early as possible, and 2) screening for asymptomatic cancer or pre-cancerous lesions in non-symptomatic target populations [3]. The US Preventive Services Task Force (USPSTF) recommends single cancer screening based on age and sex for lung (also risk-based), colon, and cervical cancers, among others [4,5,6,7,8]. For cancers with screening paradigms such as cervical cancer, most cases (43%) are diagnosed in early stage where 5-year survival rates are high (91.2%). However, for cancers without screening paradigms, such as pancreatic cancer, most cases (51%) are diagnosed in late stage, where 5-year survival rates are very low (3.2%) [2].
Currently, the level of invasiveness of cancer screening varies by cancer type and location, ranging from more invasive procedures such as colonoscopy for colorectal cancer and Papanicolaou test (pap smear) for cervical cancer, to less invasive procedures such as blood-based tests or imaging tests such as mammography or low-dose computed tomography. A key focus of current research for cancer screening is less invasive multi-cancer screening technologies, such as blood-based multi-cancer detection screening assays [9]. This multi-cancer early detection (MCED) approach has the potential to improve treatment outcomes through earlier diagnosis of a wide range of cancer types, in addition to improving health-related quality of life (HRQoL) for patients with a positive diagnosis.
Cancer type and cancer stage may be associated with specific symptomatology, with overall symptoms and symptom impact being greater in advanced disease stages [10]. Advanced cancer stage and increased symptoms are associated with worse HRQoL, which may be evaluated through patient reported outcome measures (PROMs). PROMs are self-reported questionnaires which provide a qualitative/quantitative measurement of various aspects of a patient’s health, including HRQoL, functional status, and symptoms and symptom burden, directly by the patient without clinician interpretation [11]. Inclusion of PROMs in clinical practice in oncology can be associated with benefits including improvements in care, prognosis, communication, patient safety, and risk identification such as symptom control and identification [12].
The purpose of this narrative review was to identify and collate published literature on symptom impact at different stages of disease progression for a range of 10 cancer types: 1) ovarian, 2) lung, 3) pancreatic, 4) esophageal, 5) stomach, 6) head and neck, 7) colorectal, 8) anal, 9) cervical, and 10) liver and bile duct. This will provide valuable information on symptom impact and HRQoL by cancer type and stage at diagnosis. In contrast to a systematic review, this narrative review was not intended to identify and report all the literature available for symptom impact but rather focused on the information most relevant to healthcare providers who are interested in understanding the burden of disease on patients with specific types of cancer.
Methods
Search strategy
Ten narrative literature reviews were performed to identify and collate published literature on patient burden at different stages of disease progression for the following cancer types: 1) ovarian, 2) lung, 3) pancreatic, 4) esophageal, 5) stomach, 6) head and neck, 7) colorectal, 8) anal, 9) cervical, and 10) liver and bile duct. Disease terms for each cancer type were run in an artificial intelligence (AI)-assisted platform (EVID PRO) [13] to identify relevant articles published within the last 5 years (January 2017—December 2022). Where the number of articles identified for a specific cancer type were limited to less than 10 articles, in the case of ovarian, esophageal, stomach, anal, cervical, and liver and bile duct cancers, this was extended to 10 years (January 2012—December 2022). The geographic scope was limited to the United States (U.S.), Canada, Europe and global studies, and only journal articles written in English were included. The EVID PRO tool automatically scans and pulls articles with any specific acronyms, scales, and/or PRO instruments. Electronic searches were supplemented with grey literature searches of relevant conference meeting abstracts restricted to the last 2 years (2020–2022). Congresses included: American Society of Clinical Oncology (ASCO), European Society for Medical Oncology (ESMO), and Professional Society for Health Economics and Outcomes Research (ISPOR) (for all indications), Digestive Disease Week (DDW) (GI cancers only), European Respiratory Society (ERS) (lung cancer), and American Head and Neck Society (AHNS) (head and neck).
Study selection
For each literature review, an initial screening was performed on the title and abstract of the identified articles followed by a full-text review of articles considered relevant. The PICOS (Population, Intervention, Comparison, Outcomes, Study Design) criteria are shown in Table 1. Studies were considered for inclusion if patient staging information was reported; outcomes included impact of cancer-related symptoms by cancer type (by stage of disease preferred), as assessed by standardized/ validated instruments (e.g., EORTC QLQ-C30, MDASI); and met the geographic and language limits described above. Studies were excluded if the study population was pretreated (treatment may affect HRQoL/PRO and thus not reflect cancer specific symptoms/impact), if studies were conducted outside US/Europe (unless global), if outcomes reported were related to treatment or were only reported post intervention (no baseline scores), and if only instruments not previously validated were implemented.
Data extraction
Following selection of relevant literature from screening and full text review, data from publications meeting the PICOS elements were extracted into standardized extraction tables in an Excel workbook by one reviewer. A second author reviewed all data extractions for completeness and accuracy. Any discrepancies encountered were discussed and resolved by a third independent reviewer.
Results
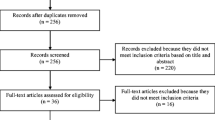
Across all cancer types, 150 articles reporting PRO data that included information on disease staging were selected. In most of these studies PRO data were not reported with results stratified by disease stage, and instead reported outcomes with patients of varying disease stages grouped together (n = 54) or included patients within a particular disease stage (n = 70). After excluding these studies, 26 studies across 8 cancer types reporting PRO results stratified by disease stage were selected for inclusion. Two cancer types, liver and bile duct, and ovarian did not return any search results with outcomes stratified by disease stage.
Descriptions of the PRO instruments used in the 26 included studies are provided in Table 2 [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. For each study across the 8 cancer types with results stratified by disease stage, a description including study design, PRO instruments and results, and any statistical analyses performed is presented in Table 3. The results for these 8 cancer types are organized by the primary stage at which each cancer type is most often diagnosed according to the National Cancer Institute SEER statistics: 1) late stage/distant, 2) regional stage, and 3) early stage/localized [34]. SEER statistics for the 10 cancer types included in the original scope of this review are presented in Table 4.
Disease staging varied throughout the 26 included studies and is reported as described in each study. Disease staging may have been described descriptively (ex. early-stage vs advanced stage) or according to a staging system such as the TNM Classification of Malignant Tumors (TNM) developed by the Union for International Cancer Control (UICC). The TNM is used for describing cancer based on: 1) tumor size and tissue location (T0 indicating no evidence of a tumor and T1-T4 describing the progressive size and invasiveness), 2) spread to lymph nodes (N0 indicating no regional nodal spread and N1-N3 indicating progressively distal nodal spread), and 3) presence of metastases (M0 indicating no metastases and M1 indicating presence of metastases) [58]. The combination of these 3 factors from the TNM system can then be used for simplified cancer staging (Stages I, II, III, and IV) [58]. While categorization as early or advanced disease based on staging varies between cancer types, generally Stage I indicates localized cancer (T1-T2, N0, M0), stage II indicates early-stage locally advanced cancer (T2-T4, N0, M0), stage III indicates late-stage locally advanced cancer (T1-T4, N1-N3, M0), and stage IV indicates metastatic cancer (T1-T4, N1-N3, M1) [58].
Cancers predominantly diagnosed at distant stage
Lung cancer
The primary stage of diagnosis for lung cancer is at a distant stage, accounting for 53% of diagnoses [34]. For lung cancer, HRQoL and symptom burden by disease stage was reported using PRO instruments including Patient-Reported Outcomes Measurement Information System (PROMIS) [35], Short-Form Survey-8 (SF-8) [36], 12-item anorexia/cachexia scale (A/CS-12) [37], Short-Form Survey-12 (SF-12) [38], Revised Psychosocial Screen for Cancer (PSSCAN-R) [39], MD Anderson Symptom Inventory (MDASI) [40], and quality of life (QoL) single item scales [40]. Overall, findings suggested that both physical and mental HRQoL were impaired in advanced stages compared with early-stage disease.
Patients with stage III or IV disease reported significantly poorer physical and mental HRQoL versus patients with stage I disease [38]. Physical HRQoL scores were 41.16 and 37.74 in patients with stage III or IV disease and 43.9 in patients with stage I disease (SF-12, P for trend < 0.001). Mental HRQoL scores were 46.26 and 45.22 in patients with stage III or IV disease and 49.28 in patients with stage I disease (SF-12, p for trend < 0.001). Additionally, between patients with advanced versus early stage disease, poorer HRQoL measured using single-item QoL scales was reported for emotional well-being (6.5 vs 7.1, P < 0.03), physical well-being (5.7 vs 6.6, P < 0.002), and overall QoL (6.3 vs 7.2, P < 0.001) [40].
A correlation between advanced disease stage and poorer mental health was also reported in studies using other PRO instruments. Advanced disease stage was significantly associated with an increased prevalence of emotional problems (SF-8, P < 0.001) [36]. Additionally, anxiety was more prevalent in patients with metastases versus those without metastases (PSSCAN-R, Odds Ratio (OR): 1.46, P < 0.001), although this association was not found for depression (Odds Ratio (OR): 1.10, P = 0.196) [39].
Greater symptom prevalence and impact were also associated with patients with advanced disease. Patients with stage III/IV disease reported worse fatigue versus patients with stage I/II disease (PROMIS, 54.6 vs 58.2) based on a clinically meaningful difference of 3 points (as defined by the study authors for the PROMIS instrument) [35]. Social function was also worse in patients with stage III/IV disease (47.2 vs 43.7), indicating that the higher symptom burden reported by patients with advanced disease also has a broader impact on patient functioning [35]. These results are supported by a second study that reported a greater prevalence of both physical and emotional symptoms (measured using the MDASI) in patients with advanced disease compared with patients with early-stage disease [40]. Symptoms significantly associated with advanced disease included sleep problems (3.5 vs 2.5, P < 0.001), drowsiness (2.6 vs 1.6, P < 0.001), fatigue (3.9 vs 2.2, P < 0.001), sadness (2.9 vs 1.9, P < 0.002), pain (3.5 vs 2.1, P < 0.001), shortness of breath (3.2 vs 2.2, P < 0.001), lack of appetite (2.1 vs 1.3, P < 0.001), and dry mouth (1.9 vs 1.2, P < 0.008). Advanced disease was also associated with increased symptom interference for the domains of work (4.4 vs 2.3, P < 0.001), enjoying life (3.8 vs 2.3, P < 0.001), general activity (3.9 vs 2.0, P < 0.001), mood (3.4 vs 2.3, P < 0.001), walking (3.4 vs 1.8, P < 0.001), and relationships with others (2.2 vs 1.2, P < 0.001). Risk for anorexia/cachexia was not significantly associated with disease stage (A/CS-12, P = 0.09) [37].
Pancreatic cancer
The primary stage of diagnosis for pancreatic cancer is at distant stage, accounting for 51% of diagnoses [34]. HRQoL and symptom outcomes in patients with pancreatic cancer were evaluated using the SF-12 [41] and MDASI [42]. Worse physical HRQoL was associated with advanced tumor stage (I-IV) (SF-12, P for trend < 0.001), although this association was not significant for mental HRQoL (SF-12, P for trend 0.16) [41]. Additionally, patients in stage III/IV had higher symptom scores compared with patients in stage II/III (MDASI, 51.8 vs 47.3), indicating worse symptom severity, although no statistical tests or P values were reported [42].
Esophageal cancer
The primary stage of diagnosis for esophageal cancer is at distant stage, accounting for 38% of diagnoses [34]. For esophageal cancer, results stratified by disease stage were reported for the instruments Functional Assessment of Cancer Therapy-General (FACT-G) [43], FACT-Esophageal (FACT-E) [43, 44], FACT-Esophageal Cancer Subscale (FACT-ECS) [43, 44], and European Quality of Life Five Dimension questionnaire (EQ-5D-3L) [43].
Better HRQoL was reported in patients with stage II/III disease versus patients in stage IV [43]. Patients with stage II/ III disease reported a mean (SD) EQ-5D baseline utility score of 0.82 (0.13) compared with a score of 0.72 (0.18) in patients with stage IV or recurrent disease. Given a minimally important difference in EQ-5D Health Utility Score (HUS) of 0.07, this indicates that patients with stage IV or recurrent disease have clinically meaningful impaired HRQoL compared with patients with early-stage disease [43]. Poorer HRQoL with advanced disease stage was also reported using disease specific instruments. Patients in stage IV showed directionally poorer scores versus patients in stage II/III for symptoms associated with esophageal cancer (FACT-ECS, 40.2 vs 46.0) and HRQoL subscales such as emotional well-being (FACT-E, 13.6 vs 17.0). However, p values were not reported for these comparisons [43]. A statistically significant trend between higher T-stage and worse HRQoL was reported between patients with T4 disease versus T1 (FACT-ECS, 44.5 vs 58.7, P < 0.002), however this trend was not significant for all instruments (FACT-E, P = 0.65) [44].
Stomach cancer
The primary stage of diagnosis for stomach cancer is at distant stage, accounting for 36% of diagnoses [34]. A significantly greater prevalence of reported cancer symptoms was associated with advanced disease stage, with results stratified by both T stage (1–4) and UICC stage (I-IV) [45]. A higher prevalence of alarm symptoms (dysphagia, weight loss, bleeding, vomiting) was reported by patients with T-stage 3/4 versus T-stage 1/2 (OR: 2.54, P < 0.0001), and for patients with UICC stage III/IV versus UICC stage I/II (OR: 3.02, P < 0.0001).
Cancers predominately diagnosed at regional stage
Head and neck cancer
The primary stage of diagnosis for head and neck cancer is at regional stage, accounting for 51% of diagnoses [34]. For head and neck cancer, results stratified by disease stage were reported for the PRO instruments National Comprehensive Cancer Network Distress Thermometer (NCCN DT) [47], Pittsburgh Sleep Quality Index (PSQI) [49], Apnea/Hypopnea Index (AHI) [48], and Eating Assessment Tool-10 (EAT-10) [46]. There was a significant correlation between advanced disease (higher T stage) and problems with swallowing (i.e., increased severity of swallowing impairment; EAT-10, P < 0.02) [46]. No statistically significant differences based on disease stage were reported for distress (NCCN DT) [47], sleep quality [49], or apnea and hypoxia [48].
Colorectal cancer
The primary stage of diagnosis for colorectal cancer is at regional stage, accounting for 36% of diagnoses [34]. In colorectal cancer, HRQoL and symptom burden by disease stage was reported using a range of PRO assessments including SF-12 [50, 51], PROMIS [35], FACT-Colorectal (FACT-C) and NSABP Symptom Checklist (SCL-17) [52], PERFORM fatigue questionnaire [53], and Hospital Anxiety and Depression Scale (HADS) [54]. Across all PRO assessments, advanced stage disease was generally associated with poorer HRQoL and increased symptomology and burden.
Significantly poorer physical and mental HRQoL was reported for patients with late-stage versus early-stage disease [50]. Comparing between patients in stage IV versus stage I, advanced disease was associated with significantly lower scores (poorer HRQoL) for both physical HRQoL (SF-12 PCS, 40.8 vs 46.9, P < 0.001) and mental HRQoL (SF-12, 46.0 vs 50.1, P < 0.001). Additionally, another study also evaluated ethnicity (white, black, or Hispanic) as a factor in HRQoL outcomes [51]. While advanced disease stage in all ethnicities was significantly associated with poorer physical HRQoL (SF-12 PCS, P < 0.05, for all), worse mental HRQoL with advanced disease was not observed, regardless of ethnicity. In comparing HRQoL in patients with stage II vs stage III cancer, significantly poorer HRQoL was reported in patients with stage III cancer (FACT-C TOI, 66.1 vs 64.0, P < 0.004) [52].
An increase in symptoms and the impact of symptoms on functioning were also associated with advanced stage disease. Clinically meaningful differences (defined by the study authors as a difference of 3 points for the PROMIS instrument) were reported in patients with stage IV and stage III cancer versus stage I/II across a range of functions and symptoms. Poorer functioning was reported in patients with stage III and IV disease versus patients with stage I/II for physical (41.8 and 43.4 vs 46.5), social (45.4 and 48.0 vs 51.2), and cognitive function (49.1 and 49.7 vs 52.9) [35]. Symptoms of pain (56.5 vs 52.1, stage IV vs stage I/II) and fatigue (56.5 vs 50.8, stage IV vs stage I/II) were also clinically worse in patients with advanced disease [35]. However, other studies reported no significant difference in fatigue between early and advanced-stage disease using other PRO instruments (SF-36 vitality subscale [52] and PERFORM 12-item scale [53]). Symptom impact was also significantly associated with advanced disease stage. Patients with stage III reported greater symptom impact (pain, vision and hearing problems, and GI problems) compared with patients with stage II cancer (SCL-17, 8.5 vs 7.2, P < 0.001) [52]. Additionally, depression was significantly more prevalent in patients with metastatic disease versus those without (HADS, 31% vs 23%, P < 0.015), although this association was not statistically significant when comparing patients based on T stage or N stage [54].
Cancers predominately diagnosed at localized stage
Anal cancer
The primary stage of diagnosis for anal cancer is at localized stage, accounting for 43% of diagnoses [34]. For anal cancer, symptom burden was described stratified by T-stage (T 1–4) [55]. Overall, the most common symptoms reported by patients with anal cancer were anal bleeding (78%), anal/perianal pain (29% and 24%, respectively), weight loss (31%), tumor on self-examination (26%), and foreign body sensation (22%). Patients with locally advanced cancer (T3/T4) reported significantly greater prevalence of constipation and abdominal pain (P < 0.02), and perianal pain and weight loss (P < 0.01). Meanwhile, pruritus was significantly more frequent in patients with early T stages (P < 0.01). Patients with more advanced disease reported significantly more symptoms than those with less advanced tumors (average total number of symptoms for T1 vs T4, 2.1 vs 4.4, P < 0.01) indicating overall poorer HRQoL.
Cervical cancer
The primary stage of diagnosis for cervical cancer is at localized stage, accounting for 43% of diagnoses [34]. For cervical cancer, results stratified by disease stage were reported for the PRO instruments European Organization For Research And Treatment Of Cancer Core Quality of Life questionnaire (EORTC QLQ-C30) and EORTC cervical cancer questionnaire (EORTC QLQ-CX24) [56], PROMIS [35], and HADS [56, 57]. In terms of global HRQoL (measured using EORTC QLQ-C30), there was no statistically significant association between cancer stage, early vs locally advanced, and global score (72.9 vs 76.1, P = 0.264). Symptom burden was assessed through the PRO instruments, PROMIS, and HADS, and the disease-specific EORTC QLQ-CX24 instrument. Patients with locally advanced cancer reported significant impairments versus patients with early stage for sexual activity (EORTC QLQ-CX24, 9.1 vs 17.1, P < 0.004) and sexual enjoyment (EORTC QLQ-CX24, 22.9 vs 52.1, P < 0.006) [56]. Poorer mental and physical HRQoL was reported between patients with stage I cancer versus stage II/III/IV cancer for the PROMIS domains of pain interference (51.1 vs 56.1), fatigue (51.8 vs 56.6), anxiety (51.5 vs 54.9), depression (50.0 vs 53.6), physical function (48.4 vs 41.2), social function (52.6 vs 46.9), and cognitive function (51.7 vs 47.9) [35]. Depression and anxiety were evaluated based on FIGO staging in two studies [56, 57]. No significant differences were reported for either anxiety or depression, although one study noted a directional trend of more patients with locally advanced disease reporting anxiety compared with patients with early-stage disease (HADS, 63% vs 53%) [56].
Discussion
In this narrative literature review of patient reported outcomes assessing symptom impact and health-related quality of life across 10 different cancer types, a general trend was observed for worse PRO results in patients with cancer diagnosed at an advanced stage of disease versus patients diagnosed at an earlier stage. Advanced disease stage was associated with greater prevalence of symptoms and increased symptom impact including general physical impairments such as pain, fatigue, and interference with functioning, as well as disease/region-specific symptom burden. Poorer HRQoL was also associated with advanced disease with commonly reported symptoms including anxiety and depression.
HRQoL, measured using generic PRO instruments, was worse in patients with advanced stage disease compared with patients with early-stage disease across cancer types. A range of generic instruments were used to measure HRQoL including the SF-12, reported in 4 studies [36, 39, 46, 48]. Clinically meaningful differences in HRQoL and symptoms were also reported for other PRO instruments such as PROMIS, with patients with advanced stage disease reporting worse HRQoL and more symptoms than patients with early stage disease [35]. Increased prevalence and/or interference of pain was correlated with advanced disease stage for colorectal cancer [35], lung cancer [35, 40], cervical cancer [35], and anal cancer [55]. This included both general pain [35, 40], and cancer type/site-specific pain such as perianal and abdominal pain in anal cancer [55]. Other general symptoms correlated with advanced disease included fatigue and sleep disturbances in lung, colorectal, and cervical cancers [35, 40], impairments in physical and cognitive function in colorectal and cervical cancer [35], nausea, lack of appetite, or anorexia and cachexia for lung cancer [37] and anal cancer [55].
The results of this review also highlight the increased burden of disease-specific symptoms in patients with advanced stage disease. Results from cancer-type specific PRO instruments were reported for the cancer types of colorectal (FACT-C TOI), cervical (EORTC QLQ-CX24), and esophageal (FACT-ECS) cancers. For both colorectal and esophageal cancer, a statistically significant association was reported between advanced cancer stage and worse HRQoL scores, as measured by the relevant disease-specific PRO instrument [44, 52]. For cervical cancer, advanced cancer stage was associated with statistically significant impairments in sexual activity and enjoyment [56]. In addition, disease-specific symptoms that correlated with advanced stage disease were seen in stomach cancer for alarm symptoms (dysphagia, weight loss, bleeding, vomiting) [45], and in head and neck cancer with trouble swallowing [46]. Together, these findings highlight the importance of using disease-specific PRO instruments to assess HRQoL and support the previously published observation that disease specific instruments are likely more sensitive to detect differences both between therapies [59, 60], but also, in the case of this review, when comparing between patients in different disease stages [59, 60].
Increased symptom burden can also impact a patient’s functional status, such as physical, emotional, or social functioning. Findings from this review show that advanced disease was associated with increased symptom interference in multiple areas including ability to work, walk, and general activity in lung cancer [40], and greater overall symptom burden in colorectal cancer [52] and anal cancer [55]. Increased prevalence or severity of emotional problems with more advanced disease was reported for multiple cancer types. Increased prevalence of emotional problems was correlated with advanced cancer stage for colorectal cancer [35, 50, 54], lung cancer [36, 38,39,40], and cervical cancer [35]. Statistically significant trends for worse mental HRQoL with advanced disease stage were also reported for colorectal cancer [46] and lung cancer [36]. Additionally, there was a statistically significant association between metastatic disease in colorectal cancer and prevalence of depression, although results were non-significant when stratified by T-stage or N-stage [52]. However, in cervical cancer, a statistically significant association was not found between advanced disease stage and prevalence of anxiety or depression [54, 55].
Across the 10 cancer types assessed in this review, 8 cancer types reported PRO results stratified by disease stage, while no studies were identified for the cancer types of liver and bile duct, or ovarian cancer. The number of studies found with results stratified by disease stage varied between cancer types and this is likely impacted by multiple variables including cancer prevalence and incidence, screening availability, distribution of cancer stage at diagnosis, treatment options, and efficacy and survival rates. The greatest number of studies found were for lung and colorectal cancer, returning 6 results each. Perhaps unsurprisingly, these cancers are the most prevalent of the 10 cancers included in the scope of this review: 1,388,422 for colorectal cancer, and 603,989 for lung cancer (Table 4) [34]. In contrast, no studies with results stratified by disease stage were found for the cancer types liver and bile duct, and ovarian, despite relatively high U.S. prevalence rates, 105,765 and 236,511, respectively (Table 4) [34]. The lack of results for these two cancers may be due to the lack of screening paradigms available for these cancers, thus resulting in the majority of cases being detected in later stages. Among the 10 cancers included in the scope of this narrative literature review, the stage at which each cancer type is primarily diagnosed varies. While stage distribution at diagnosis for colorectal cancer is more evenly distributed between early/localized stage (35% of cases), regional stage (36% of cases), and late/distant stage (23% of cases), other cancers are more highly skewed towards diagnosis at the advanced (distant) stage, including lung (53% of cases), pancreatic (51% of cases), esophageal (38% of cases), stomach (36% of cases), and ovarian (55% of cases) (Table 4) [34]. In general, 5-year survival rates are greater for those cancers that are more often diagnosed in earlier stages, although exceptions apply (e.g., liver and bile duct) [2]. Overall, data support the importance of early diagnosis and treatment to improve survival rates and reduce the negative impact of late diagnosis on patient symptom burden and HRQoL.
A few key limitations are present in this narrative literature review. First, while database searches were conducted in a systematic manner, this work was not intended to be a systematic review. Therefore, the studies selected are considered to be of most relevance to the question being addressed but may not include all relevant references. While the primary objective of this narrative literature review was to identify and collate published literature on patient burden at different stages of disease progression for the ten selected cancers, the secondary objective was to evaluate HRQoL based on cancer type and stage, within and between different cancer types. However, selected literature was heterogenous in terms of patient populations and study design. This review included both prospective and retrospective studies, the latter of which carries additional limitations including the potential for bias due to missing or misreported data. Also, while this review was focused on identifying patients with PRO assessments at the time of diagnosis and prior to treatment, the nature of retrospective claims analyses means that it is sometimes difficult to determine if patients may have previously received treatment. Additionally, studies may not have been powered for PRO endpoints. Statistical comparisons were not reported in all studies and few studies reported minimally important differences. Taken together, these factors limited the ability to draw strong conclusions.
Conclusions
The findings of this narrative literature review support the search for improvements in cancer screening and earlier detection and treatment. Studies with results stratified by disease stage were limited, likely due to some cancers primarily being detected at advanced stages. Although the HRQoL data lacked consistent stratification by cancer stage, advanced stage cancer at diagnosis and prior to treatment was generally associated with worse HRQoL. This observation was expected due to stage or spread of disease likely playing a significant role in symptom impact burden. Overall, this supports the importance of detecting and treating cancer at earlier stages when patients may be asymptomatic or have lower symptom burden to minimize the increased negative impact on HRQoL and functional status observed in cancers diagnosed in advanced stage.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- A/CS-12:
-
12-Item anorexia/cachexia scale
- AHI:
-
Apnea/Hypopnea Index
- AHNS:
-
American Head and Neck Society
- ASCO:
-
American Society of Clinical Oncology
- DDW:
-
Digestive Disease Week
- EAT-10:
-
Eating Assessment Tool-10
- EORTC QLQ-C30:
-
European Organization For Research And Treatment Of Cancer Core Quality of Life questionnaire
- EORTC QLQ-CX24:
-
EORTC cervical cancer questionnaire
- EQ-5D-3L:
-
European Quality of Life Five Dimension questionnaire
- ERS:
-
European Respiratory Society
- ESMO:
-
European Society for Medical Oncology
- FACT-C:
-
Functional Assessment of Cancer Therapy-Colorectal
- FACT-E:
-
Functional Assessment of Cancer Therapy-Esophageal
- FACT-ECS:
-
Functional Assessment of Cancer Therapy-Esophageal Cancer Subscale
- FACT-G:
-
Functional Assessment of Cancer Therapy-General
- FIGO:
-
International Federation of Gynecology and Obstetrics
- HADS:
-
Hospital Anxiety and Depression Scale
- HRQoL:
-
Health-related quality of life
- HUS:
-
Health Utility Score
- ISPOR:
-
Professional Society for Health Economics and Outcomes Research
- MCED:
-
Multi-cancer early detection
- MCS:
-
Mental Component Summary
- MDASI:
-
MD Anderson Symptom Inventory
- NCCN DT:
-
National Comprehensive Cancer Network Distress Thermometer
- OR:
-
Odds Ratio
- PCS:
-
Physical Component Summary
- PICOS:
-
Population, Intervention, Comparison, Outcomes, Study Design
- PROMIS:
-
Patient-Reported Outcomes Measurement Information System
- PROMs:
-
Patient reported outcome measures
- PSQI:
-
Pittsburgh Sleep Quality Index
- PSSCAN-R:
-
Revised Psychosocial Screen for Cancer
- SCL-17:
-
National Surgical Adjuvant Breast and Bowel Project (NSABP) Symptom Checklist
- SF-12:
-
Short-Form Survey-12
- SF-36:
-
Short-Form Survey-36
- SF-8:
-
Short-Form Survey-8
- TOI:
-
Trial Outcome Index
- UICC:
-
Union for International Cancer Control
- USPSTF:
-
US Preventive Services Task Force
References
Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49.
Incidence and relative survival by stage at diagnosis for common cancers. https://www.cdc.gov/cancer/uscs/about/data-briefs/no25-incidence-relative-survival-stage-diagnosis.htm. Accessed 2 Oct 2023.
World Health Organization. Guide to cancer early diagnosis. Geneva: World Health Organization; 2017.
U.S. Preventive Services Task Force. Screening for lung cancer: US preventive services task force recommendation statement. JAMA. 2021;325(10):962–70.
U.S. Preventive Services Task Force. Screening for breast cancer: US preventive services task force recommendation statement. Ann Intern Med. 2016;164(4):279–96.
U.S. Preventive Services Task Force. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA. 2021;325(19):1965–77.
U.S. Preventive Services Task Force. Screening for prostate cancer: US preventive services task force recommendation statement. JAMA. 2018;319(18):1901–13.
U.S. Preventive Services Task Force. Screening for cervical cancer: US preventive services task force recommendation statement. JAMA. 2018;320(7):674–86.
Klein EA, Richards D, Cohn A, Tummala M, Lapham R, Cosgrove D, Chung G, Clement J, Gao J, Hunkapiller N, et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Ann Oncol. 2021;32(9):1167–77.
Koo MM, Swann R, McPhail S, Abel GA, Elliss-Brookes L, Rubin GP, Lyratzopoulos G. Presenting symptoms of cancer and stage at diagnosis: evidence from a cross-sectional, population-based study. Lancet Oncol. 2020;21(1):73–9.
Cella D, Hahn E, Jensen S, Butt Z, Nowinski C, Rothrock N, Lohr K. Patient-reported outcomes in performance measurement. 2015.
Silveira A, Sequeira T, Goncalves J, Lopes Ferreira P. Patient reported outcomes in oncology: changing perspectives-a systematic review. Health Qual Life Outcomes. 2022;20(1):82.
Michelson M, Chow T, Mahida S, Manson S, Park J. PCN308 natural language processing to understand the landscape of patient-reported outcomes in a specific disease area. Value Health. 2020;23:S477.
Ribaudo JM, Cella D, Hahn EA, Lloyd SR, Tchekmedyian NS, Von Roenn J, Leslie WT. Re-validation and shortening of the Functional Assessment of Anorexia/Cachexia Therapy (FAACT) questionnaire. Qual Life Res. 2000;9(10):1137–46.
Guilleminault C, Tilkian A, Dement WC. The sleep apnea syndromes. Annu Rev Med. 1976;27:465–84.
Belafsky PC, Mouadeb DA, Rees CJ, Pryor JC, Postma GN, Allen J, Leonard RJ. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann Otol Rhinol Laryngol. 2008;117(12):919–24.
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–76.
Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–43.
Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, Silberman M, Yellen SB, Winicour P, Brannon J, et al. The functional assessment of cancer therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11(3):570–9.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Cleeland CS, Mendoza TR, Wang XS, Chou C, Harle MT, Morrissey M, Engstrom MC. Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer. 2000;89(7):1634–46.
National Comprehensive Cancer Network. NCCN practice guidelines for the management of psychosocial distress. National Comprehensive Cancer Network. Oncology (Williston Park). 1999;13(5a):113–47.
Baro E, Carulla J, Cassinello J, Colomer R, Mata JG, Gascon P, Gasquet JA, Herdman M, Rodriguez CA, Sanchez J, et al. Development of a new questionnaire to assess patient perceptions of cancer-related fatigue: item generation and item reduction. Value Health. 2009;12(1):130–8.
Cella D, Yount S, Rothrock N, Gershon R, Cook K, Reeve B, Ader D, Fries JF, Bruce B, Rose M, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): progress of an NIH Roadmap cooperative group during its first two years. Med Care. 2007;45(5 Suppl 1):S3–11.
Linden W, Yi D, Barroetavena MC, MacKenzie R, Doll R. Development and validation of a psychosocial screening instrument for cancer. Health Qual Life Outcomes. 2005;3:54.
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213.
Kopec JA, Yothers G, Ganz PA, Land SR, Cecchini RS, Wieand HS, Lembersky BC, Wolmark N. Quality of life in operable colon cancer patients receiving oral compared with intravenous chemotherapy: results from National Surgical Adjuvant Breast and Bowel Project Trial C-06. J Clin Oncol. 2007;25(4):424–30.
Turner-Bowker DM, Bayliss MS, Ware JE, Kosinski M. Usefulness of the SF-8™ health survey for comparing the impact of migraine and other conditions. Qual Life Res. 2003;12(8):1003–12.
Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33.
Ware JE, Kosinski M, Keller SD. SF-36 physical and mental health summary scales: a user’s manual. Boston: Health Assessment Lab; 1994.
Greimel ER, Kuljanic Vlasic K, Waldenstrom AC, Duric VM, Jensen PT, Singer S, Chie W, Nordin A, Bjelic Radisic V, Wydra D, et al. The European Organization for Research and Treatment of Cancer (EORTC) quality-of-life questionnaire cervical cancer module: EORTC QLQ-CX24. Cancer. 2006;107(8):1812–22.
Wendy LW, Elizabeth AH, Fei M, Hernandez L, David ST, Cella D. Reliability and validity of the Functional Assessment of Cancer Therapy-Colorectal (FACT-C) quality of life instrument. Qual Life Res. 1999;8(3):181–95.
Darling G, Eton DT, Sulman J, Casson AG, Celia D. Validation of the functional assessment of cancer therapy esophageal cancer subscale. Cancer. 2006;107(4):854–63.
SEER*Explorer: an interactive website for SEER cancer statistics. https://seer.cancer.gov/statistics-network/explorer/.
Jensen RE, Potosky AL, Moinpour CM, Lobo T, Cella D, Hahn EA, Thissen D, Smith AW, Ahn J, Luta G, et al. United States population-based estimates of patient-reported outcomes measurement information system symptom and functional status reference values for individuals with cancer. J Clin Oncol. 2017;35(17):1913–20.
Morrison EJ, Novotny PJ, Sloan JA, Yang P, Patten CA, Ruddy KJ, Clark MM. Emotional problems, quality of life, and symptom burden in patients with lung cancer. Clin Lung Cancer. 2017;18(5):497–503.
Berry DL, Blonquist T, Nayak MM, Roper K, Hilton N, Lombard H, Hester A, Chiavacci A, Meyers S, McManus K. Cancer anorexia and cachexia: screening in an ambulatory infusion service and nutrition consultation. Clin J Oncol Nurs. 2018;22(1):63–8.
Pierzynski JA, Ye Y, Lippman SM, Rodriguez MA, Wu X, Hildebrandt MAT. Socio-demographic, clinical, and genetic determinants of quality of life in lung cancer patients. Sci Rep. 2018;8(1):10640.
Leung B, Laskin J, Wu J, Bates A, Ho C. Assessing the psychosocial needs of newly diagnosed patients with nonsmall cell lung cancer: Identifying factors associated with distress. Psychooncology. 2019;28(4):815–21.
Mendoza TR, Kehl KL, Bamidele O, Williams LA, Shi Q, Cleeland CS, Simon G. Assessment of baseline symptom burden in treatment-naive patients with lung cancer: an observational study. Support Care Cancer. 2019;27(9):3439–47.
Deng Y, Tu H, Pierzynski JA, Miller ED, Gu X, Huang M, Chang DW, Ye Y, Hildebrandt MAT, Klein AP, et al. Determinants and prognostic value of quality of life in patients with pancreatic ductal adenocarcinoma. Eur J Cancer. 2018;92:20–32.
Ambai VT, Singh V, Boorman DW, Neufeld NJ. Celiac plexus neurolysis for abdominal cancers: going beyond pancreatic cancer pain. Pain Rep. 2021;6(1):e930.
Doherty MK, Leung Y, Su J, Naik H, Patel D, Eng L, Kong QQ, Mohsin F, Brown MC, Espin-Garcia O, et al. Health utility scores from EQ-5D and health-related quality of life in patients with esophageal cancer: a real-world cross-sectional study. Dis Esophagus. 2018;31(12):1–9.
Kidane B, Ali A, Sulman J, Wong R, Knox JJ, Darling GE. Health-related quality of life measure distinguishes between low and high clinical T stages in esophageal cancer. Ann Transl Med. 2018;6(13):270.
Franck C, Zimmermann N, Goni E, Lippert H, Ridwelski K, Kruschewski M, Kreuser N, Lingohr P, Schildberg C, Vassos N, et al. Different prevalence of alarm, dyspeptic and reflux symptoms in patients with cardia and non-cardia gastric cancer. J Gastrointestin Liver Dis. 2021;30(4):431–7.
Amin JD, Rodriggs T, Weir KA, Snider JW, Hatten KM. Prospective evaluation of swallowing symptoms in human papillomavirus-associated oropharynx cancer. Dysphagia. 2022;37(1):58–64.
Brauer ER, Lazaro S, Williams CL, Rapkin DA, Madnick AB, Dafter R, Cheng G, Porter A, Abemayor E, Chai-Ho W, et al. Implementing a tailored psychosocial distress screening protocol in a head and neck cancer program. Laryngoscope. 2021;132(8):1600–8.
Huppertz T, Horstmann V, Scharnow C, Ruckes C, Bahr K, Matthias C, Gouveris H. OSA in patients with head and neck cancer is associated with cancer size and oncologic outcome. Eur Arch Otorhinolaryngol. 2021;278(7):2485–91.
Santoso AMM, Jansen F, Lissenberg-Witte BI, Baatenburg de Jong RJ, Langendijk JA, Leemans CR, Smit JH, Takes RP, Terhaard CHJ, van Straten A, et al. Poor sleep quality among newly diagnosed head and neck cancer patients: prevalence and associated factors. Support Care Cancer. 2021;29(2):1035–45.
Reyes ME, Ye Y, Zhou Y, Liang A, Kopetz S, Rodriquez MA, Wu X, Hildebrandt MA. Predictors of health-related quality of life and association with survival may identify colorectal cancer patients at high risk of poor prognosis. Qual Life Res. 2017;26(2):319–30.
Belachew AA, Reyes ME, Ye Y, Raju GS, Rodriguez MA, Wu X, Hildebrandt MAT. Patterns of racial/ethnic disparities in baseline health-related quality of life and relationship with overall survival in patients with colorectal cancer. Qual Life Res. 2020;29(11):2977–86.
Ganz PA, Hays RD, Spritzer KL, Rogatko A, Ko CY, Colangelo LH, Arora A, Hopkins JO, Evans TL, Yothers G. Health-related quality of life outcomes after neoadjuvant chemoradiotherapy for rectal cancer in NRG Oncology/NSABP R-04. Cancer. 2022;128(17):3233–42.
Ruiz-Casado A, Franco FF, Romero-Elias M, Fiuxa C, Gutiérrez Sanz L, Alvarez-Bustos A, Sanchez Ruiz A, Garcia Gonzalez D, Gonzalez-Cutre D, Cebolla H. 1564P Cancer-related fatigue in colorectal cancer patients at the time of diagnosis. Ann Oncol. 2022;33:S1263.
Varela-Moreno E, Rivas-Ruiz F, Padilla-Ruiz M, Alcaide-Garcia J, Zarcos-Pedrinaci I, Tellez T, Fernandez-de Larrea-Baz N, Bare M, Bilbao A, Sarasqueta C, et al. Influence of depression on survival of colorectal cancer patients drawn from a large prospective cohort. Psychooncology. 2022;31(10):1762–73.
Sauter M, Keilholz G, Kranzbuhler H, Lombriser N, Prakash M, Vavricka SR, Misselwitz B. Presenting symptoms predict local staging of anal cancer: a retrospective analysis of 86 patients. BMC Gastroenterol. 2016;16:46.
Ferrandina G, Mantegna G, Petrillo M, Fuoco G, Venditti L, Terzano S, Moruzzi C, Lorusso D, Marcellusi A, Scambia G. Quality of life and emotional distress in early stage and locally advanced cervical cancer patients: a prospective, longitudinal study. Gynecol Oncol. 2012;124(3):389–94.
Mantegna G, Petrillo M, Fuoco G, Venditti L, Terzano S, Anchora LP, Scambia G, Ferrandina G. Long-term prospective longitudinal evaluation of emotional distress and quality of life in cervical cancer patients who remained disease-free 2-years from diagnosis. BMC Cancer. 2013;13:127.
TNM Classification. https://www.ncbi.nlm.nih.gov/books/NBK553187/. Accessed 31 Oct 2023.
Patrick DL, Deyo RA. Generic and disease-specific measures in assessing health status and quality of life. Med Care. 1989;27(3 Suppl):S217-232.
McKenna SP. Measuring patient-reported outcomes: moving beyond misplaced common sense to hard science. BMC Med. 2011;9:86.
Acknowledgements
Medical writing support was provided by Henry Blanton, an employee of Genesis Research Group.
Funding
This review was conducted by Genesis Research Group with funding provided by GRAIL, Inc.
Author information
Authors and Affiliations
Contributions
K.C.C., A.M., G.G.G., M.R.W., and A.E.B. contributed to research design, synthesis and interpretation of findings. G.G.G. and M.R.W. contributed to acquisition, analysis, and interpretation of review data. K.C.C., G.G.G., A.E.B. and D.L.P. contributed to synthesis and interpretation of findings and critically reviewed draft manuscripts. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
K.C.C. is an employee of GRAIL, Inc. with stock ownership in Illumina, Bristol Myers Squibb, Gilead, Baxter, and Bayer. A.E.B. and G.G.G. are current employees of Genesis Research Group, A.M. and M.R.W. are former employees of Genesis Research Group. D.L.P. provides consulting to GRAIL, Inc.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chung, K.C., Muthutantri, A., Goldsmith, G.G. et al. Symptom impact and health-related quality of life (HRQoL) assessment by cancer stage: a narrative literature review. BMC Cancer 24, 884 (2024). https://doi.org/10.1186/s12885-024-12612-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12612-z