
Abstract
Background
Hospitalisation resulting from complications of systemic therapy and radiotherapy places a substantial burden on the patient, society, and healthcare system. To formulate preventive strategies and enhance patient care, it is crucial to understand the connection between complications and the need for subsequent hospitalisation. This review aimed to assess the existing literature on complications related to systemic and radiotherapy treatments for cancer, and their impact on hospitalisation rates.
Methods
Data was obtained via electronic searches of the PubMed, Scopus, Embase and Google Scholar online databases to select relevant peer-reviewed papers for studies published between January 1, 2000, and August 30, 2023. We searched for a combination of keywords in electronic databases and used a standard form to extract data from each article. The initial specific interest was to categorise the articles based on the aspects explored, especially complications due to systemic and radiotherapy and their impact on hospitalisation. The second interest was to examine the methodological quality of studies to accommodate the inherent heterogeneity. The study protocol was registered with PROSPERO (CRD42023462532).
Findings
Of 3289 potential articles 25 were selected for inclusion with ~ 34 million patients. Among the selected articles 21 were cohort studies, three were randomised control trials (RCTs) and one study was cross-sectional design. Out of the 25 studies, 6 studies reported ≥ 10 complications, while 7 studies reported complications ranging from 6 to 10. Three studies reported on a single complication, 5 studies reported at least two complications but fewer than six, and 3 studies reported higher numbers of complications (≥ 15) compared with other selected studies. Among the reported complications, neutropenia, cardiac complications, vomiting, fever, and kidney/renal injury were the top-most. The severity of post-therapy complications varied depending on the type of therapy. Studies indicated that patients treated with combination therapy had a higher number of post-therapy complications across the selected studies. Twenty studies (80%) reported the overall rate of hospitalisation among patients. Seven studies revealed a hospitalisation rate of over 50% among cancer patients who had at least one complication. Furthermore, two studies reported a high hospitalisation rate (> 90%) attributed to therapy-repeated complications.
Conclusion
The burden of post-therapy complications is emerging across treatment modalities. Combination therapy is particularly associated with a higher number of post-therapy complications. Ongoing research and treatment strategies are imperative for mitigating the complications of cancer therapies and treatment procedures. Concurrently, healthcare reforms and enhancement are essential to address the elevated hospitalisation rates resulting from treatment-related complications in cancer patients.
Similar content being viewed by others

Introduction
Recent advances in cancer treatment [1], including systemic therapy and radiotherapy, have redefined the landscape of oncological care [2,3,4]. These treatment modalities, individually and in combination, have significantly improved patient outcomes and survival rates [5, 6]. While systemic therapy and radiotherapy have improved overall survival rates, they have also been linked to adverse events, such as neutropenia, thrombocytopenia, anaemia, sepsis, fever, mucositis, dehydration, and nausea and vomiting, some of which can result in hospitalisations [7,8,9,10]. There may be a complex relationship of treatment-related complications that can give rise to scenarios necessitating hospitalisation. This complex relationship between systemic therapy, radiotherapy, and subsequent hospitalisation has a profound impact on comprehensive cancer care [9].
A number of studies have examined the effectiveness of these treatments in terms of disease control and patient survivorship [11,12,13,14]. However, the impact of treatment-related complications and their correlative effects on hospitalisation rates have yet to be synthesised. This review seeks to address this knowledge gap, shedding light on the multifaceted relationship that shapes the trajectory of cancer care.
Systemic therapy includes a range of drug treatments or interventions, including chemotherapy, immunotherapy, and targeted therapy, each precisely tailored to the unique attributes of individual patients, the nature of their diseases, and the predominant treatment objectives [11, 13, 15,16,17,18]. Several complications occurring from systemic therapy and radiotherapy cover a diverse range [7,8,9,10], involving both immediate and long-term effects which have serious repercussions on the quality of life and survival outcomes [5, 19,20,21]. These complications are evidenced as haematological toxicities, neurological impairments, gastrointestinal perturbations, dermatological problems, and cardiopulmonary sequelae, among various others [9, 22, 23]. While certain complications can be effectively managed through outpatient healthcare services, others refer to a more significant impact, necessitating patients to hospitalisation for meticulous observation, intensive monitoring and specialised interventions.
The evolution of cancer care has gone beyond the boundaries of the clinic, reflecting shifts in outpatient-centred care models, and augmented supportive care strategies. Reducing hospitalisations has been a significant improvement in patient experience, meeting the patient's desire to maintain their health status. However, hospitalisation due to complications of systemic therapy and radiotherapy can have a significant burden on the patient, society, and the healthcare system. These hospitalisations can lead to interruptions in treatment and adversely affect the patient's response to treatment. Furthermore, complications resulting in hospitalisations can also result in treatment interruptions and negatively affect the patient's response to treatment. Although some review studies have attempted to capture post-therapy complications due to systemic therapy and/or radiotherapy, most of these studies have focused on a single type of cancer or a specific type of complication [24,25,26,27,28,29]. Unfortunately, there has been little effort to conduct a comprehensive review study that provides extensive data on all types of complications, any type of cancer, various types of therapy, and their subsequent hospitalisation.
The increasing concern about the burden of hospitalisation due to treatment-related complications has made it crucial to understand the link between complications and hospitalisation. This knowledge is essential for the development of preventive strategies and the improvement of patient care. Therefore, the primary objective of this systematic review is to analyse the available ongoing literature to investigate the relationship between systemic therapy and radiotherapy-related complications, and how they affect hospitalisation rates. This review presents a comprehensive analysis of the existing literature on complications related to systemic and radiotherapy treatments for cancer, and their impact on hospitalisation rates. The review highlights that hospitalisations due to treatment complications pose a significant burden on the healthcare system. When many patients require hospitalisation due to complications, it can reduce the availability of resources for other patients in need, limiting access to care. Moreover, increased hospitalisations can lead to additional demands on healthcare professionals, potentially increasing their workload and affecting patient care quality. Policymakers and clinicians can use this evidence to revisit existing clinical policies, regulations, and strategies, while patients can make better-informed decisions regarding their cancer therapies. This review can serve as a guide for future intervention efforts and contribute to a better scientific understanding of the issue.
By analysing a diverse range of studies, the objective of this review is to achieve the following goals:
-
1)
Identify the types and frequencies of complications associated with systemic therapy and radiotherapy.
-
2)
Quantify the proportion of patients who require hospitalisation due to complications arising from these treatments.
-
3)
Investigate potential predictors of hospitalisation, such as patient demographics, treatment modalities, and complication severity.
-
4)
Discuss the implications of treatment-related complications for healthcare resource allocation, patient well-being, and treatment decision-making.
Methods
This systematic review was registered under International Prospective Register of Systematic Reviews (PROSPERO) with the registration number of CRD42023462532. This review adopted the PICOS framework for structing and designing this study [30].
PICOS | Population (P): All patients undergoing systemic therapy and/or radiotherapy for cancer treatment |
Interventions (I): Systemic therapy and/or radiotherapy for cancer treatment | |
Comparison (C): No specific comparison is required for this systematic review since the focus is on the relationship between treatment complications and subsequent hospitalisation rates | |
Outcomes (O): o Types and frequencies of complications associated with systemic therapy and radiotherapy o Proportion of patients experiencing complications that lead to hospitalisation o Variation in hospitalisation rates across different cancer types and treatment contexts o Implications of treatment-related complications for healthcare resource allocation, patient well-being, and treatment decision-making | |
Study Design (S): This review comprehensively analyses the impact of systemic therapy and radiotherapy complications on hospitalisation rates, using various study designs including randomized controlled trials, cohort studies, and cross-sectional observational studies |
Eligibility criteria
This review added a published peer-review publication provided it fulfilled all the following criteria. In this review, inclusion and exclusion criteria were defined based on the research objectives, study population, interventions, comparisons, and outcomes (PICOS framework) [31]. An eligible article was selected based on the following criteria:
Inclusion criteria
-
1)
All patients underwent systemic therapy and/or radiotherapy for cancer treatment.
-
2)
Original research articles using quantitative study designs (e.g., cohort, longitudinal, case–control, cross-sectional, and randomised controlled trials),
-
3)
Studies reported complications or side effects associated with systemic therapy and/or radiotherapy.
-
4)
Studies stated the proportion of patients experiencing complications that require hospitalisation.
-
5)
Studies that provided sufficient data for the synthesis of outcomes.
-
6)
Studies published in English and published between January 1, 2000 to August 30, 2023.
Exclusion criteria
This review excluded these publications, including reviews, perspectives, opinion speech of papers, commentaries, editorials, letters, conference abstracts, reports, grey literature, unpublished research, studies without primary data, animal studies, laboratory studies, and in vitro studies.
Information sources
A search strategy was developed to search Medline via the PubMed interface, Scopus, Embase, and Google Scholar online databases to identify relevant original peer-reviewed papers for our systematic review. In addition to the database search, we explored references of selected studies and previously published article on similar topics (backward and/or forward reference searching) to incorporate all potential pertinent articles to construct our summary estimates. A snowball method was applied to ensure completeness.
Search strategy
This systematic review was conducted to identify literature that reported on complications due to systemic and radiotherapy and their impact on hospitalisation. The search strategy was comprised of three concepts: (i) systemic therapy and radiotherapy as part of cancer treatment; (ii) complications or side effects associated with systemic therapy and/or radiotherapy; (iii) hospitalisation due to therapy-related complications. This review screened quantitative studies focused on cancer diseases. This review search included articles published in English language between January 1, 2000, and August 30, 2023, to capture the most relevant and update articles on this topic. A combination of keywords, MeSH and Boolean operators’ terms were applied to develop the search terms. A description of search terms is given in Appendix Table A1.
Data collection process
The four reviewers (RAM, MS, PKD, and MPM) screened the titles and abstracts of retrieved studies against the predefined inclusion and exclusion criteria. After settling any differences, the reviewers independently extracted the data, discussed the inputs, and revised the extracted data. Unresolved issues were resolved by involving two reviewers (OW and MEH). Excluded studies did not meet the eligibility criteria.
Data items
This review considered the following outcomes according to the study objectives:
-
Types and frequencies of complications associated with systemic therapy and radiotherapy.
-
Proportion of patients experiencing complications that lead to hospitalisation.
-
Variation in hospitalisation rates across different cancer types and treatment contexts.
Data extractions
Using EndNote libraries, four independent reviewers screened the articles. They created a data-extraction form to establish the type of information to be extracted. The reviewers recorded relevant data on the name of the first author, study settings (country), publication year, study design, number of study participants, time horizon /follow-up periods, demographics (e.g., average age/age group, gender), cancer types, cancer stages, systemic and radiotherapy, intervention, comparators, list of complications and associated hospitalisations. We further inputted data on hospitalisations (length of stay in days, and/or percentage of hospitalised patients). In addition, they documented studies’ description of analytical models/methods, internal validity checks or robustness of findings, description of handling missing data, and funding sources. Unresolved issues were resolved by involving a reviewer (OW).
Quality assessment
Considering the diverse range of study designs including randomised controlled trials (RCTs) [32], cohort, and cross-sectional studies [33], three distinct quality assessment tools were employed to accommodate the inherent heterogeneity. Reviewers assessed the quality of the included studies, and the discrepancies were resolved with discussion with the reviewer (OW). The critical appraised tools utilised in this study were constructed by the Joanna Briggs Institute (JBI) [33]. These tools are widely adopted in academic studies [34, 35] and provide a nuanced evaluation of the risk of bias, categorised as low, moderate, or high [35]. Study quality impacts future research confidence. High-quality studies assure conclusions, while low-quality studies raise replication doubts.
Synthesis of results
The reviewers used a narrative synthesis approach for synthesis of results that integrated the quantitative findings with the qualitative insights. This approach facilitated a comprehensive understanding of the relationships between systemic therapy, radiotherapy, complications, and hospitalisation rates. Using this approach, the reviewers observed the patterns, trends, and consistencies across studies within this qualitative synthesis. The reviewers used Microsoft Excel to manage synthesis data and analyse data. To present the relationship between post-therapy complications and the reporting studies, a heatmap was generated using the statistical software R (v4.3.1).
Synthesis methods
Data were systematically presented and tabulated to encompass population demographics and study characteristics. Within the scope of descriptive analysis, categorical variables' attributes were interpreted through frequencies (n) and percentages (%), which were employed to convey the continuous nature of quantitative data. The comprehensive account of systemic and radiotherapy-related complications was outlined, categorised by cancer types, stages, and study designs. Pertaining to hospitalisation, data stemming from complications due to systemic and radiotherapy were demonstrated in terms of descriptive statistics, including mean length of stay (in days) or hospitalisation rates expressed as a percentage, as appropriate to the context.
Results
Data selection and process
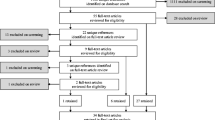
The eligibility of studies included was determined following a three-steps screening process. Firstly, EndNote software was used to eliminate duplicates from all retrieved studies or documents. Secondly, the reviewers examined the articles by reading the titles and abstracts to determine their relevance to our study. Finally, the third stage necessitated reading of full texts of all possibly relevant articles identified by our searches as reflected in the PRISMA flow diagram Fig. 1.

PRISMA flow diagram
Description of studies included
The initial search retrieved 3289 studies from the electronic databases. After excluding the duplicates and irrelevance or absence of required information, we screened the titles and abstracts for a further selection of eligible articles (Fig. 1). Subsequently, we selected 80 articles based on eligibility criteria for full-text review. After excluding 55 studies in the full-text review, finally, 25 studies with a total of approximately 33.82 million patients were included in the systematic review [7,8,9,10, 15, 18, 21, 36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53]. A total of 55 studies were excluded for various reasons: 12 were editorial, opinion pieces, commentary, or letters to the editor; 9 were review papers; and 34 did not provide sufficient or complete outcome-related data.
Characteristics of the studies
Table 1 shows the characteristics of the included studies in our review. Approximately 52% studies (12 out 25 studies) were in the USA (n = 13) [7, 9, 10, 15, 18, 37, 38, 40, 45, 46, 49, 51, 53], followed by 28% studies in Australia (n = 7) [8, 21, 36, 39, 41, 42, 44]. In terms of study participants, the selected studies exhibited a wide range, with participant numbers varying from 60 to 29,546,02 participants. 56% of the studies (14 out of 25 studies) involved 1000 or more participants [9, 10, 15, 18, 37, 38, 40, 42, 44,45,46, 48, 51, 53], while approximately one-third of the selected studies (7 out of 25 studies) had participants number ranging from 100 to 500 [7, 8, 21, 36, 41, 50, 52]. One study had a comparatively smaller participants number (< 100 participants) compared with others [39]. Furthermore, most selected studies (21 out of 25 studies) adopted a cohort study design [7,8,9,10, 21, 36,37,38,39, 41,42,43,44,45,46, 48, 49, 51,52,53,54], three RCTs [47, 49, 52] and one study using a cross-sectional study design [40].
A higher number of selected studies (60%, 15 out of 25) included both male and female populations. Seven studies (28%) exclusively focused on female participants, while three studies included male participants only (Table 1). Most of the selected studies (96%, 24 out of 25) featured adult (> 18 years) participants, while one study solely focused on child participants [43]. Considering the trend of relevant publications, eight of the selected studies (32%) were published between 2002 and 2011, while 17 studies (68%) were published between 2012 and 2022 (Table 1).
Cancer and diagnosis related information
Table 2 shows the participants' cancer-related characteristics. Out of the 25 studies reviewed, 15 of them focused on patients with a single type of cancer (breast, lung or other) [8, 15, 21, 36, 37, 39, 42, 43, 47,48,49,50,51,52,53], while the remaining 10 studies included individuals with multiple types of cancers [7, 9, 10, 38, 40, 41, 44,45,46]. Furthermore, five studies were conducted solely on breast cancer patients, and six focused on lung cancer patients. Approximately 62% of the studies (15 out of 25) reported on patients with cancer at all stages, from stage I to IV. Nine studies focused on patients with advanced-stage cancer (stage III or IV), while one study reported early-stage cancer (stage I or II). In terms of the treatment modalities used in the studies, 9 out of 25 studies (55%) employed a combination of therapies, such as chemotherapy, radiotherapy, hormonal therapy, and/or antibiotic therapy for cancer treatment. On the other hand, 16 out of 25 studies reported that patients received a single therapy, either chemotherapy or radiotherapy. The details are presented in Table 2.
Reported therapy-related complication and impact on hospitalisation
Table 3 presents data on complications related to therapy and resulting hospitalisations. Most studies (19 out 25 studies) reported multiple complications, but three studies focused on a single complication [21, 36, 39]. Out of the 25 studies, six studies reported 10 or more complications [7,8,9,10, 37, 47], while seven studies reported complications ranging from six to ten (Table 3). Five studies reported at least two complications but fewer than six [38, 42, 43, 50, 51], and three studies reported significantly higher numbers of complications (15 or more) compared with other selected studies. Furthermore, four studies reported between nine to eleven complications. However, three out 25 studies concentrated on a single complication [21, 36, 39], including weight loss, fatigue, and reduced lymphovascular invasion.
In this study, we investigated the reported post-therapy complications to generalize the disease patterns. Compiling the adverse events, we have classified and found 49 different complications based on reported complication types and characteristics (Supplementary File S1). Among the reported complications, neutropenia, any types of infections, cardiac complications, vomiting, fever, and kidney/renal injury were the top-most post-therapy complications (Fig. 2). Moreover, anemia, mental/neural complications, and respiratory complications were also reported by the included studies as post-therapy complications.

The distribution and relationship between the post-therapy complications and the selected studies. Note: The complications were plotted in the y-axis corresponding to the included studies in the x-axis. The orange boxes mean the presence (value = 1) of that type of complication reported by the corresponding studies and the grey boxes mean the absence (value = 0) of that type of complication. AST = aspartate aminotransferase and ALT = alanine aminotransferase
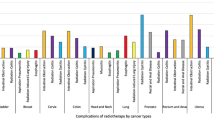
Figure 3 shows that the severity of post-therapy complications varied depending on the type of therapy. For example, studies indicate that patients treated with combination therapy had a higher number of post-therapy complications across the selected studies. This suggests that combination therapy is associated with a higher number of post-therapy complications.

Number of post-therapy complications by therapy. Note: Combination therapy involves using two or more treatment methods simultaneously. This could include chemotherapy and radiotherapy; chemotherapy, radiation therapy, and hormonal therapy; or chemotherapy and antibiotic therapy. On the other hand, single therapy refers to using only one method of treatment modality, such as chemotherapy, radiotherapy, or hormonal therapy
In the investigation of hospitalisations resulting from therapy-related complications, 20 studies (80%) reported the overall rate of hospitalisation among patients [7, 9, 15, 18, 21, 38,39,40,41,42,43, 45,46,47,48,49,50,51,52,53]. Of these, four studies provided data on the average length of stay (ALOS) [8, 10, 36, 44], while two studies reported both the overall hospitalisation rate and ALOS [37, 45]. Of the studies which reported ALOS, three out six studies showed a hospitalisation ALOS of 9 days, [10, 36, 44] whereas one study was reported an ALOS of 12 days [8]. Seven out of 25 studies revealed a hospitalisation rate of over 50% among cancer patients who had at least one complication [9, 15, 37,38,39,40, 43]. Furthermore, two studies reported an exceptionally high hospitalisation rate (> 90%) attributed to therapy-repeated complications [9, 38].
Quality of included studies
Based on the review, it was found that all 21 cohort studies analysed were deemed reliable due to their high-quality standards [7,8,9,10, 21, 36,37,38,39, 41,42,43,44,45,46, 48, 49, 51,52,53,54]. Furthermore, three RCTs [47, 49, 52] and single cross-sectional study were assessed to be of high quality, indicating that they adhered to the JBI quality assessment criteria [40]. It's worth noting that no studies were excluded based on poor quality assessment scores (more details Appendix Table A2-A4).
Discussion
This study analysed data from 25 studies that involved approximately 33.8 million cancer patients, providing a summarised relationship between systemic therapy and radiotherapy complications and their impact on hospitalisation rates. This review identified all studies were conducted in high-income countries such as the United States, Australia, and Canada. However, there is a lack of evidence on cancer therapy-related post-complication complications and associated hospitalisations, specifically in low- and lower-middle-income countries. The study revealed that approximately half of the included studies used combination therapies, such as chemotherapy and radiotherapy and/or hormonal therapy or antibiotic therapy) as the prevailing treatment modalities among cancer patients. This study found that a combination therapy is associated with a higher complication rate. Regarding post-therapy complications due to systemic therapy and radiotherapy, two-thirds of the included studies’ participants reported multiple complications related to therapy, with most studies reporting that around 80% of hospitalisations were associated with these complications. These findings varied depending on the type of cancer diagnosis, disease severity, and study design. For instance, among the selected studies conducted among breast or lung cancer patients, three or more complications were reported. Most of the selected studies adopted a cohort study design to generate this evidence, followed by randomised control trials. Our review identified that the majority of the cancer patients were from all stages (i.e., I to IV), however, minority studies included the advanced (III/IV) and early stages (I/II) of patients. A previous systematic review, focused on endometrial cancer, reported that severe adverse effects in the advanced stages were common [55]. Further, another study illustrated that chemotherapy and radiotherapy for all types of cancers induced changes which may present complications, leading to hospitalisations of the patients [16]. As such, cancers at advanced stages are vulnerable to treatment-related complications that could lead to hospitalisations. These emphasise the critical need for early diagnosis and tailored therapeutic approach especially in the advanced stages, including proactive management of treatment related adverse effects to reduce the rate of hospitalisation.
Similar to the studies conducted in previous [11, 13, 20], our review found that more than 50% of treatment modalities were a combination of chemotherapy and radiotherapy for cancer treatment which might lead to complications [56, 57]. We found that a combination therapy is associated with a higher complication rate. Using multiple therapeutic methods at the same time can lead to an increase in adverse events and complications. A study on advanced pancreatic ulcers highlighted that though combination treatment strategies increased the side effects, had the potential to improve the treatment outcomes [57]. This highlights the need to carefully weigh the potential benefits and risks of combining different treatments. Although combination therapy can have promising outcomes, the higher complication rate underscores the importance of considering the risk–benefit ratio when making clinical decisions. Future research should focus on understanding the mechanisms behind these complications to refine treatment protocols, improve patient safety, and ultimately enhance the effectiveness of combination therapies in managing this specific condition.
Our review reports the data on the therapy-related adverse effects and patient hospitalisation rates as a major outcome, illustrating multiple complications that might lead to higher hospitalisations rate and longer hospital stay. Some previous studies reported that therapy-related treatment modalities for cancer have higher complications, these lead to higher emergency visits and length of hospital stay [9, 58, 59]. These might be due to the toxicity of treatment, weak immune system, and patient with other co-morbidities. In addition, sepsis, pneumonia and aspiration pneumonitis were associated with longer hospital stays [9, 45]. These results underscore the needs of identification and management of potential side effects related to cancer therapies. The findings also suggest the importance of a multidisciplinary approach to cancer care, involving oncologists, nurses, or other health professionals to minimise the adverse events and reduce hospitalisation rates. Therefore, the authors suggest future clinical research on refining the treatment modalities.
This review has some limitations. Firstly, most of the included studies are from developed countries, which could limit the generalisability of our findings to the low- and lower-middle-income countries, where healthcare systems and patient populations may differ substantially. Secondly, there is a paucity of uniformity in the research methodologies applied across studies. However, the majority are cohort studies, and one cross-sectional study design and this variation can affect the level of casual inferences that can be drawn from the findings. Thirdly, this review revealed variations in the follow-up periods used in the included studies. This variability can impact decision-making, potentially leading to confusion among audience regarding the long-term or short-term impacts of different cancer treatment modalities. Lastly, the availability and consistency of data regarding specific complications and hospitalisations are limited. This inconsistency poses challenges for making direct comparisons and assessing the nature and severity of complications. Despite these acknowledged and essential limitations, one of the study's strengths was its strong study selection and screening protocols. Because of our rigorous search approach and inclusion criteria, this review conducted the systematic review of hospitalisation due to therapy-related complications among cancer patients to date. Most of the papers included in the review were of high quality. The comprehensive subgroup analyses demonstrate that our findings are applicable to a wide range of contexts. The review findings underscore the importance of delving deeper into the intricate relationships between systemic and radiotherapy-related complications and their causal links to hospitalisation. Future investigations can benefit from more robust research designs, utilising episode-driven data sources that enable a thorough exploration of these connections.
The results of this review have significant implications for clinical practice, healthcare policy, and future research aimed at reducing complications associated with cancer treatment and lowering hospitalisation rates. The findings offer valuable insights and potential strategies, including:
-
1)
Highlighting the need for healthcare reforms and improvements in several countries due to the high rates of hospitalisation resulting from treatment-related complications of cancer.
-
2)
Providing oncologists with a better understanding of the complications associated with therapy-related cancer treatments and their serious repercussions on hospitalisations, enabling them to provide early diagnosis, personalised care plans, and strategies to mitigate the effects.
-
3)
Educating patients and healthcare providers about the potential complications of cancer treatments, facilitating timely identification and intervention, ultimately improving patient outcomes and quality of life.
-
4)
Enabling policymakers to allocate resources more effectively by investing wisely and equitably in cancer preventive strategies, enhancing the quality of care provided to patients.
-
5)
Recommending that healthcare policies incorporate these findings and nations strengthen their preventive measures and care models.
-
6)
Suggesting the need for more research, particularly in low- and lower-middle-income countries, with long-term follow-up studies to assess the impact of treatments. Economically viable interventions and prolonged economic assessments are also recommended.
Conclusions
This review highlights the increasing burden of post-therapy complications due to systemic therapy and radiotherapy and the lack of data on cancer therapy-related complications in low-resource settings. Most studies were conducted in high-income countries, raising questions about research in low- and lower-middle-income countries. To reduce hospitalisation due to therapy-related complications, we need to invest in research, improve educational resources, increase screening and surveillance programs, and address misconceptions. Future research should be standardised, patient-centred, and investigate health economics.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- HICs:
-
High-income countries
- LIMCs:
-
Low- and middle-income countries
- LOS:
-
Length of stay
- SD:
-
Standard deviation
- RCTs:
-
Randomized controlled trials
References
DeVita VT, Rosenberg SA. Two hundred years of cancer research. N Engl J Med. 2012;366:2207–14.
Markham MJ, Wachter K, Agarwal N, Bertagnolli MM, Chang SM, Dale W, et al. Clinical cancer advances 2020: annual report on progress against cancer from the American society of clinical oncology. J Clin Oncol. 2020;38:1081–101.
Chen HHW, Kuo MT. Improving radiotherapy in cancer treatment: promises and challenges. Oncotarget. 2017;8:62742–58.
Debela DT, Muzazu SGY, Heraro KD, Ndalama MT, Mesele BW, Haile DC, et al. New approaches and procedures for cancer treatment: current perspectives. SAGE Open Med. 2021;9:20503121211034370.
Donovan JL, Hamdy FC, Lane JA, Mason M, Metcalfe C, Walsh E, et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2016;375:1425–37.
Nathan P, Hassel JC, Rutkowski P, Baurain J-F, Butler MO, Schlaak M, et al. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N Engl J Med. 2021;385:1196–206.
Ling DC, Kabolizadeh, Heron P, Ohr DE, Wang JPH, Johnson J, et al. Adult height and head and neck cancer: a pooled analysis within the INHANCE consortium. Head Neck. 2014;36:1391.
Goldstein D, Bennett BK, Webber K, Boyle F, De Souza PL, Wilcken NRC, et al. Cancer-related fatigue in women with breast cancer: outcomes of a 5-year prospective cohort study. J Clin Oncol. 2012;30:1805–12.
Jairam V, Lee V, Park HS, Thomas CR, Melnick ER, Gross CP, et al. Treatment-related complications of systemic therapy and radiotherapy. JAMA Oncol. 2019;5:1028–35.
Schilling MB, Parks C, Deeter RG. Costs and outcomes associated with hospitalized cancer patients with neutropenic complications: a retrospective study. Exp Ther Med. 2011;2:859–66.
Chan RJ, Crichton M, Crawford-Williams F, Agbejule OA, Yu K, Hart NH, et al. The efficacy, challenges, and facilitators of telemedicine in post-treatment cancer survivorship care: an overview of systematic reviews. Ann Oncol. 2021;32:1552–70.
Jacobsen PB, Nipp RD, Ganz PA. Addressing the survivorship care needs of patients receiving extended cancer treatment. Am Soc Clin Oncol Educ Book. 2017;37:674–83.
Chan RJ, Crawford-Williams F, Crichton M, Joseph R, Hart NH, Milley K, et al. Effectiveness and implementation of models of cancer survivorship care: an overview of systematic reviews. J Cancer Surviv. 2023;17:197–221.
Moro-Valdezate D, Buch-Villa E, Peiró S, Morales-Monsalve MD, Caballero-Gárate A, Martínez-Agulló Á, et al. Factors associated with health-related quality of life in a cohort of Spanish breast cancer patients. Breast Cancer. 2014;21:442–52.
Du XL, Chan W, Giordano S, Geraci JM, Delclos GL, Burau K, et al. Variation in modes of chemotherapy administration for breast carcinoma and association with hospitalization for chemotherapy-related toxicity. Cancer. 2005;104:913–24.
Albano D, Benenati M, Bruno A, Bruno F, Calandri M, Caruso D, et al. Imaging side effects and complications of chemotherapy and radiation therapy: a pictorial review from head to toe. Insights Imaging. 2021;12:1–28.
Ohe Y. Treatment-related death from chemotherapy and thoracic radiotherapy for advanced cancer. Panminerva Med. 2002;44:205–12.
Waddle MR, Chen RC, Arastu NH, Green RL, Jackson M, Qaqish BF, et al. Unanticipated hospital admissions during or soon after radiation therapy: Incidence and predictive factors. Pract Radiat Oncol. 2015;5:e245–53.
Pan H, Gray R, Braybrooke J, Davies C, Taylor C, McGale P, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2018;377:1836–46.
Kasi A, Abbasi S, Handa S, Al-Rajabi R, Saeed A, Baranda J, et al. Total neoadjuvant therapy vs standard therapy in locally advanced rectal cancer: a systematic review and meta-analysis. JAMA Netw Open. 2020;3:1–11.
Ong WL, Nazareth L, Hindson B, Matheson B, Millar JL. Long-term outcomes following post-operative radiotherapy for Stage I/II testicular seminoma – An Australasian single-institution experience. J Med Radiat Sci. 2016;63:161–9.
Yang K, Murphy ES, Lo SS, Chao ST, Suh JH. Chapter 27-Neurological complications of radiation therapy. In: Newton HB, Malkin MG, editors. Neurological Complications of Systemic Cancer and Antineoplastic Therapy (Second Edition). Academic Press; 2022. p. 465–77.
Lim YJ, Lee SW, Choi N, Kwon J, Eom KY, Kang E, et al. Failure patterns according to molecular subtype in patients with invasive breast cancer following postoperative adjuvant radiotherapy: long-term outcomes in contemporary clinical practice. Breast Cancer Res Treat. 2017;163:555–63.
Schindler A, Denaro N, Russi EG, Pizzorni N, Bossi P, Merlotti A, et al. Dysphagia in head and neck cancer patients treated with radiotherapy and systemic therapies: literature review and consensus. Crit Rev Oncol Hematol. 2015;96:372–84.
Cardenal F, Nadal E, Jové M, Faivre-Finn C. Concurrent systemic therapy with radiotherapy for the treatment of poor-risk patients with unresectable stage III non-small-cell lung cancer: a review of the literature. Ann Oncol. 2015;26:278–88.
Shah C, Kundu N, Arthur D, Vicini F. Radiation therapy following postmastectomy reconstruction: a systematic review. Ann Surg Oncol. 2013;20:1313–22.
Rim CH, Kim Y, Kim CY, Yoon WS, Yang DS. Is stereotactic body radiotherapy for ultra-central lung tumor a feasible option? A systemic review and meta-analysis. Int J Radiat Biol. 2018;95:329–37.
Zackrisson B, Mercke C, Strander H, Wennerberg J, Cavallin-Ståhl E. A systematic overview of radiation therapy effects in head and neck cancer. Acta Oncol (Madr). 2003;42:443–61.
Hölscher T, Bentzen SM, Baumann M. Influence of connective tissue diseases on the expression of radiation side effects: a systematic review. Radiother Oncol. 2006;78:123–30.
Robinson KA, Saldanha IJ, Mckoy NA. Development of a framework to identify research gaps from systematic reviews. J Clin Epidemiol. 2011;64(12):1325–30.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions. 2nd Edition. Chichester (UK): Wiley; 2019.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic. ESRC methods programme. 2006;15:47–71.
Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R et al. Systematic reviews of etiology and risk (2020). Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis. JBI; 2024.
Xiao J, Ding J, Huang C. Notion of a good death for patients with cancer: a qualitative systematic review protocol. BMJ Open. 2022;12:e056104.
Mahumud RA, Kamara JK, Renzaho AMN. The epidemiological burden and overall distribution of chronic comorbidities in coronavirus disease-2019 among 202,005 infected patients: evidence from a systematic review and meta-analysis. Infection. 2020;48:813–33.
Vangelov B, Smee RI. Clinical predictors for reactive tube feeding in patients with advanced oropharynx cancer receiving radiotherapy ± chemotherapy. Eur Arch Otorhinolaryngol. 2017;274:3741–9.
Hassett MJ, O’Malley AJ, Pakes JR, Newhouse JP, Earle CC. Frequency and cost of chemotherapy-related serious adverse effects in a population sample of women with breast cancer. J Natl Cancer Inst. 2006;98:1108–17.
O’Neill CB, Atoria CL, O’Reilly EM, Henman MC, Bach PB, Elkin EB. Hospitalizations in older adults with advanced cancer: the role of chemotherapy. J Oncol Pract. 2016;12:e138–48.
Wijetunga AR, Chua TC, Nahm CB, Pavlakis N, Clarke S, Chan DL, et al. Survival in borderline resectable and locally advanced pancreatic cancer is determined by the duration and response of neoadjuvant therapy: survival in advanced pancreatic cancer. Eur J Surg Oncol. 2021;47:2543–50.
Rivera DR, Gallicchio L, Brown J, Liu B, Kyriacou DN, Shelburne N. Trends in adult cancer–related emergency department utilization: an analysis of data from the nationwide emergency department sample. JAMA Oncol. 2017;3:1–8.
Alamgeer M, Coleman A, McDowell L, Giddings C, Safdar A, Sigston E, et al. Treatment outcomes of standard (high dose) cisplatin and non-standard chemotherapy for locally advanced head and neck cancer. Cancer Rep. 2023;6:1–9.
David R, Hiwase M, Kahokehr AA, Lee J, Watson DI, Leung J, et al. Predicting post-radiation genitourinary hospital admissions in patients with localised prostate cancer. World J Urol. 2022;40:2911–8.
Bassal M, Silva M, Patel S, Gibson PJ, Breakey VR, Athale U, et al. Phase-specific risks of outpatient visits, emergency visits, and hospitalizations during children’s oncology group-based treatment for childhood acute lymphoblastic leukemia: a population-based study. Pediatr Blood Cancer. 2021;68:1–8.
te Marvelde L, Whitfield A, Shepheard J, Read C, Milne RL, Whitfield K. Epidemiology of sepsis in cancer patients in Victoria, Australia: a population-based study using linked data. Aust N Z J Public Health. 2020;44:53–8.
Saxena A, Rubens M, Ramamoorthy V, Tonse R, Veledar E, McGranaghan P, et al. Hospitalization rates for complications due to systemic therapy in the United States. Sci Rep. 2021;11:1–7.
Hassett MJ, Rao SR, Brozovic S, Stahl JE, Schwartz JH, Maloney B, et al. Chemotherapy-related hospitalization among community cancer center patients. Oncologist. 2011;16:378–87.
Gridelli C, De Marinis F, Pujol JL, Reck M, Ramlau R, Parente B, et al. Safety, resource use, and quality of life in paramount: a phase III study of maintenance pemetrexed versus placebo after induction pemetrexed plus cisplatin for advanced nonsquamous non-small-cell lung cancer. J Thorac Oncol. 2012;7:1713–21.
Enright K, Grunfeld E, Yun L, Moineddin R, Ghannam M, Dent S, et al. Population-based assessment of emergency room visits and hospitalizations among women receiving adjuvant chemotherapy for early breast cancer. J Oncol Pract. 2015;11:126–32.
Hanna N, Shepherd FA, Fossella FV, Pereira JR, Demarinis F, Von Pawel J, et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Oncol Pract. 2004;22:1589–97.
Früh M, Besrour H, Gillessen S, Joerger M, Hitz F, Savidan A, et al. Management of elderly patients with advanced non-small cell lung cancer: a single-center experience. Chemotherapy. 2013;59:42–50.
Lang K, Marciniak MD, Faries D, Stokes M, Buesching D, Earle C, et al. Costs of first-line doublet chemotherapy and lifetime medical care in advanced non-small-cell lung cancer in the United States. Value Health. 2009;12:481–8.
Sederholm C, Hillerdal G, Lamberg K, Kölbeck K, Dufmats M, Westberg R, et al. Phase III trial of gemcitabine plus carboplatin versus single-agent gemcitabine in the treatment of locally advanced or metastatic non-small-cell lung cancer: the Swedish lung cancer study group. J Clin Oncol. 2005;23:8380–8.
Du XL, Osborne C, Goodwin JS. Population-based assessment of hospitalizations for toxicity from chemotherapy in older women with breast cancer. J Clin Oncol. 2002;20:4636–42.
Novello S, Pimentel FL, Douillard JY, O’Brien M, Von Pawel J, Eckardt J, et al. Safety and resource utilization by non-small cell lung cancer histology: results from the randomized phase III study of pemetrexed plus cisplatin versus gemcitabine plus cisplatin in chemonaïve patients with advanced non-small cell lung cancer. J Thorac Oncol. 2010;5:1602–8.
Carey MS, Gawlik C, Fung-Kee-Fung M, Chambers A, Oliver T. Systematic review of systemic therapy for advanced or recurrent endometrial cancer. Gynecol Oncol. 2006;101:158–67.
Rogers L, Siu SSN, Luesley D, Bryant A, Heather O. Radiotherapy and chemoradiation after surgery for early cervical cancer. Cochrane Database Syst Rev. 2014;5:1–43.
Chin V, Nagrial A, Sjoquist K, O’Connor CA, Chantrill L, Biankin AV, et al. Chemotherapy and radiotherapy for advanced pancreatic cancer. Cochrane Database Syst Rev. 2018;3(3):CD011044.
Ooi BS, Tjandra J, Green MD. Morbidities of adjuvant chemotherapy and radiotherapy for resectable rectal cancer. Dis Colon Rectum. 1999;42:403–18.
Akinosoglou K, Karkoulias K, Marangos M. Infectious complications in patients with lung cancer. Eur Rev Med Pharmacol Sci. 2013;17:8–18.
Acknowledgements
Not applicable.
Funding
There was no funding available for this study.
Author information
Authors and Affiliations
Contributions
R.A.M. conceived and designed the experiments. R.A.M., M.S., P.D., M.P.M. contributed to the literature search, and the data acquisition. R.A.M. and M.S. prepared the draft manuscript. R.A.M. and M.S. contributed to the data interpretation. R.A.M., M.S., M.E.H., and O.W. edited and reviewed the manuscript and contributed to the acquisition, or interpretation of data for the work. All authors contributed to the critical revision of the manuscript and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mahumud, R.A., Shahjalal, M., Dahal, P.K. et al. Systemic therapy and radiotherapy related complications and subsequent hospitalisation rates: a systematic review. BMC Cancer 24, 826 (2024). https://doi.org/10.1186/s12885-024-12560-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12560-8