
Abstract
Background
The role of familial influence in chronic myeloid leukaemia (CML) occurrence is less defined. Previously, we conducted a study to determine the prevalence of harbouring BCR::ABL1 in our local adult normal population (designated as StudyN). We present our current study, which investigated the prevalence of harbouring BCR::ABL1 in the normal first-degree relatives of local CML patients (designated as StudyR). We compared and discussed the prevalence of StudyR and StudyN to assess the familial influence in CML occurrence.
Methods
StudyR was a cross-sectional study using convenience sampling, recruiting first-degree relatives of local CML patients aged ≥ 18 years old without a history of haematological tumour. Real-time quantitative polymerase chain reaction standardised at the International Scale (BCR::ABL1-qPCRIS) was performed according to standard laboratory practice and the manufacturer’s protocol.
Results
A total of 96 first-degree relatives from 41 families, with a mean age of 39 and a male-to-female ratio of 0.88, were enrolled and analysed. The median number of relatives per family was 2 (range 1 to 5). Among them, 18 (19%) were parents, 39 (41%) were siblings, and 39 (41%) were offspring of the CML patients. StudyR revealed that the prevalence of harbouring BCR::ABL1 in the first-degree relatives was 4% (4/96), which was higher than the prevalence in the local normal population from StudyN, 0.5% (1/190). All four positive relatives were Chinese, with three of them being female (p > 0.05). Their mean age was 39, compared to 45 in StudyN. The BCR::ABL1–qPCRIS levels ranged between 0.0017%IS and 0.0071%IS, similar to StudyN (0.0023%IS to 0.0032%IS) and another study (0.006%IS to 0.016%IS).
Conclusion
Our study showed that the prevalence of harbouring BCR::ABL1 in the first-degree relatives of known CML patients was higher than the prevalence observed in the normal population. This suggests that familial influence in CML occurrence might exist but could be surpassed by other more dominant influences, such as genetic dilutional effects and protective genetic factors. The gender and ethnic association were inconsistent with CML epidemiology, suggestive of a higher familial influence in female and Chinese. Further investigation into this topic is warranted, ideally through larger studies with longer follow-up periods.
Similar content being viewed by others


Background
Chronic myeloid leukaemia (CML) is a myeloproliferative neoplasm that originates from haematopoietic stem cells and is characterised by a chromosomal translocation t(9;22)(q34;q11.2), which forms the Philadelphia chromosome (Ph) containing the BCR::ABL1 fusion gene [1]. Evidence strongly indicates that BCR-ABL1 tyrosine kinase, the translated protein of BCR::ABL1, is the primary driver of CML. Diagnosis of CML requires detection of the Ph and/or BCR::ABL1, along with the clinical features, leucocytosis, and other laboratory findings. Untreated CML typically progresses through three phases: chronic phase (CP), marked by leucocytosis (total white blood cell count (TWC) ≥ 12 × 109/L); acceleration phase (AP); and blast crisis (BC) [1]. The introduction of tyrosine kinase inhibitor (TKI) targeting BCR-ABL1 has significantly improved prognosis. However, approximately 7% [2] to 18% [3] of CP patients progress to AP/BC despite treatment with imatinib, the first-generation TKI. In the latest World Health Organisation Classification (5th edition), AP is omitted in favour of an emphasis on high-risk features associated with CP progression and resistance to TKI [4].
For identifying CML-related laboratory features at low cancer load, the most sensitive test is polymerase chain reaction (PCR) detecting BCR::ABL1, followed by cytogenetic test detecting Ph, and then, full blood count (FBC) primarily identifying leucocytosis. Clinical features of CP e.g., constitutional symptoms and splenomegaly, typically appear thereafter. BCR::ABL1 transcript can be classified into major (M-BCR), minor (m-BCR), and micro (µ-BCR) depending on the breakpoint in BCR. M-BCR is the predominant transcript type in CML and the only one that has been standardised at International Scale (IS). IS-standardised real-time quantitative polymerase chain reaction (qPCR) for BCR::ABL1 (BCR::ABL1-qPCRIS) allows direct comparison of the BCR::ABL1 M-BCR level across different laboratories. When a CML patient achieves complete cytogenetic response (no detectable Ph) after starting TKI, the approximate equivalent BCR::ABL1 is around 1%IS [5].
There have been cases, of which Ph was detected incidentally in the absence of clinical features or leucocytosis, prompting a need of a new entity, designated as pre-clinical CML (pre-CP) [6] in this manuscript. In order to exclude those pre-CP cases without leucocytosis due to concurrent disease or medication usage that causes cytopaenia, we continue to use a criterion used by Kuan et al. [6] i.e., Ph was positive in < 75% metaphases. Pre-CP, at the median Ph of 35% (range 10-75%), often progresses to CP within a mean duration of 16 months (range 3 to 48) (Supplementary Table 1) [7,8,9,10,11,12,13,14,15,16,17]. The duration is supported by Hauser RG et al. [18] who investigated 1,623 patients underwent M-BCR testing for CML diagnosis and had at least six consecutive years of FBC with differentials prior to CML diagnosis. Among them, 6.2% were found to be M-BCR positive. This study revealed that the minimum basophil percentage over the previous year and the minimum TWC over the previous three years could predict a positive BCR::ABL1 M-BCR test result. Before the CML CP diagnosis, abnormalities in TWC and basophil percentage could persist for a year or more.
Simultaneously, some normal subjects were found harbouring BCR::ABL1 [19]. Most studies on normal subjects harbouring BCR::ABL1 used convenience sampling. Thus, the results could not be inferred to a normal population. About 8% of the normal subjects/population harboured BCR::ABL1 M-BCR (Supplementary Table 2) [20,21,22,23,24,25,26,27,28,29,30,31]. While pre-CP often progresses to CP, there was no reported progression to pre-CP or CP from normal subjects/population harbouring BCR::ABL1, probably because most studies did not report follow-up information on the positive subjects [19]. However, a lower BCR::ABL1 load might be a reason. Most studies did not use BCR::ABL1-qPCRIS making comparison across studies and further deduction difficult. Pre-CP is a subset of the normal subjects/population harbouring BCR::ABL1. We hypothesized that a considerable yet undetermined genetic abnormality load, maybe around 0.1%IS, is needed for CML occurrence.
Subsequently, it is interesting to investigate healthy relatives of CML patients who are a subset of normal population. CML is generally considered non-inheritable, but reported familial CML cases suggest genetic susceptibility associated with heritage (Supplementary Table 3) [32,33,34,35,36,37,38,39,40,41,42,43,44,45]. Familial CML is rare, partly attributed to the low incidence rate of CML. In 2017, global age-standardized incidence rate (ASIR) of CML typically ranged between 0.26 and 0.75 per 100,000 population [46]. Our local data also reported a low ASIR of 0.5 per 100,000 population from 1996 to 2015 [47]. However, the prevalence of CML is increasing due to the drastic improvement in survival with TKI. The aetiology of BCR::ABL1 and non-BCR::ABL1-related disease driver remain poorly understood. We hypothesize the occurrence of CML may be sporadic, related to genetic susceptibility, or combination of both, intertwining with environmental elements and protective genetic factors. Notable risk factor is ionized radiation [48]. Other suggested risk factors are benzene [49], obesity [50], and smoking [51]. Familial CML cases highlight genetic susceptibility in some CML patients that are worth further studying. Human leucocyte antigen [52,53,54,55,56,57] and single nucleotide polymorphisms [58] were suggested but a conclusive answer is not yet apparent. The reported familial CML cases were more common in first-degree relatives, noting that cases in more distance relative cases are likely more under-reported than first-degree relatives.
Only a few non-case report studies [33, 59,60,61,62] have examined risk of getting CML in relatives of CML patients. An earlier study by Gunz FW et al. [33] in Sydney, Australia, investigated 909 leukaemia patients, including 119 with CML, using interviews and tracing techniques. The study showed that the incidence of leukaemia was 2.8-3.0 times higher among first-degree relatives and about 2.3 times higher among more distant relatives compared to the expected rates. However, the study noted an unusually low proportion of CML cases among first-degree relatives, with only one instance of concordance (CML-CML). Another study by Hasle H and Olsen JH [62] investigated cancer in relatives of children with myelodysplastic syndrome, acute myeloid leukaemia and CML in Denmark. There were 37 first-degree relatives, as well as 7 second- and third-degree relatives of eight CML children in the study. They found no case of CML or increase risk of neoplasms in the relatives. Two consecutive Swedish studies investigated the prevalence of CML among first-degree relatives of CML patients utilizing registry data [59, 60]. The first study examined 9491 first-degree relatives of 4619 CML patients diagnosed between 1958 and 2004, and compared them with 42,474 first-degree relatives of matched controls. However, the diagnosis of CML did not incorporate Ph and/or BCR::ABL1 [59]. Using the same registries which later incorporated Ph and/or BCR::ABL1, the second study examined 4,287 first-degree relatives of 88 CML patients diagnosed between 2002 and 2013 and compared them with 20,930 first-degree relatives of matched controls [60]. Both studies showed no increase odds ratio of haematological or solid cancers in the first-degree relatives of CML patients. However, these studies do not report the demographic comparison between the two cohorts and are limited by the nature of the data source and natural history of CML that CML patients could be asymptomatic and undiagnosed for a long period of time. There was no confirmative conclusion could be made from the above non-case report studies in view of the study limitations.
If there is no increased risk of getting CML in relatives of CML patients, it does not eliminate the possibility of familial influence in CML occurrence. To our knowledge, there was only one study [61] explored the familial influence in CML occurrence by comparing the prevalence of harbouring BCR::ABL1 in first-degree relatives of CML patients and control group. The study performed qualitative PCR to detect BCR::ABL1 M-BCR in 46 normal first-degree relatives from nine CML families and 52 parents/siblings from 10 families without CML. The M-BCR positivity rate in the relative and control group was 33% and 25%, respectively, though not statistically significant. This study is limited by small sample size and demographic differences between the two groups. The male-to-female ratio was 0.53 versus 0.67 and mean age was 28.6 versus 36.5 in the relative and control group, respectively. CML is a relatively uncommon haematological cancer, primarily affecting male aged 60 years old and above [46].
Previously, we conducted a study to determine the prevalence of harbouring BCR::ABL1 M-BCR in our local adult normal population (designated as StudyN subsequently in this manuscript) [31]. In this manuscript, we present our current study to determine the prevalence of harbouring BCR::ABL1 M-BCR in first-degree relatives of local CML patients using BCR::ABL1-qPCRIS (designated as StudyR subsequently in this manuscript). We compared and discussed the prevalence of StudyR and StudyN [31] to assess the familial influence on CML occurrence.
Methods
Ethic and informed consent
StudyR received approval from the Ethic Committee of Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak (UNIMAS) (ref no: UNIMAS/TNC(PI)/09–65/01 [3]). It adhered to the Malaysian Good Clinical Practice Guideline, aligning with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participating relatives.
Study design
StudyR was a cross-sectional study using convenience sampling. Local CML patients followed-up under government hospitals in southern and middle zone of Sarawak were approached. After getting their verbal consent, their first-degree relatives (parents, siblings, including half-siblings, or offspring) were approached. Inclusion criteria were aged 18 years old or above, capable of providing consent, and able to attend scheduled blood taking session at stations in southern and middle zone of Sarawak. Exclusion criteria were refusal to participate and a history of haematological tumour. Demographic data e.g., age, gender, ethnic, weight, height, alcohol consumption, smoking habit, etc., was obtained. About 15 mL of peripheral blood was collected for FBC and BCR::ABL1–qPCRIS testing. Primary end point was to study the prevalence of positive BCR::ABL1–qPCRIS among first-degree relatives of CML patients.
Laboratory methodology
Laboratory methodology was similar to StudyN [31]: FBC was performed using an automated haematology analyser (XS800i, Sysmex). Total RNA was extracted using TRIzol® according to manufacturer’s protocol after red blood cell lysis. The RNA extracted underwent one-step RT-PCR and the BCR::ABL1–qPCRIS test using the SuperScript™ III Platinum™ One-Step qRT-PCR Kit (Invitrogen), the RNaseOUT™ Recombinant Ribonuclease Inhibitor (Invitrogen), and MolecularMD BCR–ABL1IS MR3 Assay™ according to the manufacturers’ protocols. The MolecularMD kit contains a BCR::ABL1 primer, ABL1 primer, three controls [negative, low (0.1%IS), and high (10%IS)], six calibrators [3e5 (300,000 copies/10 µL), 3e4 (30,000 copies/10 µL), 3e3 (3000 copies/10 µL), 3e2 (300 copies/10 µL), 3e1 (30 copies/10 µL), and 3e0 (3 copies/10 µL)] and nuclease-free water. Fusion gene (BCR::ABL1) and control gene (ABL1) transcripts were amplified in at least two replicates for each sample. The percentage of the BCR::ABL1:ABL1 copy number ratio was multiplied by a correction factor of 0.98, as specified in the MolecularMD kit, to obtain the percentage in IS [63].
The differences between StudyR and StudyN were the qPCR machine and testing site. StudyN used LightCycler 96 at Kumamoto University, while StudyR used Roche LightCycler 480II at UNIMAS. The software program used for quantification cycle (Cq) calling in StudyR was the Second Derivative Maximum Method.
Figure 1 illustrates the BCR::ABL1–qPCRIS workflow for both StudyR and StudyN. If one or both replicates in the first experiment (Experiment 1) were positive, a repeat experiment of the same sample (Experiment 2) was performed. If both replicates in Experiment 2 were positive, the relative was determined positive for harbouring BCR::ABL1. If one or both replicates tested positive in Experiment 1, the option of repeated blood sampling and testing (follow-up) was offered, contingent upon consent.

Flow chart of the study. Group C was defined as harbouring BCR::ABL1 by the study operational definition
The laboratory procedure was conducted cautiously to avoid contamination e.g., usage of biosafety/laminated flow cabinet and different workstation/laboratory for lysis, RNA extraction, and BCR::ABL1–qPCRIS. Each BCR::ABL1–qPCRIS included negative controls for BCR::ABL1 and nuclease-free water for BCR::ABL1 and ABL1. Besides that, there were other BCR::ABL1–qPCRIS evaluation criteria used to exclude possibility of contamination.
Statistical analysis
Data was entered into Microsoft® Excel® for Microsoft 365 MSO. Descriptive statistics was analysed using the same software. The data (relative cohort) was compared to the previous study on the normal population (population cohort) [31] using RStudio (version 2022.12.0 + 353 “Elsbeth Geranium” Release (7d165dcfc1b6d300eb247738db2c7076234f6ef0, 2022-12-03) for Windows Mozilla/5.0 (Windows NT 10.0; Win64; x64)). Chi-square (χ2) test for categorical data and analysis of variance (ANOVA) or Kruskal–Wallis test for normally and non-normally distributed continuous data, respectively, were used to compare the two cohorts. The significant level was set at 0.05, unless otherwise specified.
Results
A total of 103 first-degree relatives participated and had BCR::ABL1–qPCRIS done between February and May 2022. Seven relatives were removed from analysis because there was no written data form. Data of the 96 relatives are presented below.
The 96 relatives were from 41 families. Among them, 18 (19%) were parents, 39 (41%) were siblings, and 39 (41%) were offspring of CML patients. Two of the siblings were half-siblings who shared one biological parent, while the rest were full siblings with the same biological parents. The median number of first-degree relatives per family enrolled was 2 (range 1 to 5).
The demographic characteristics of the relatives are shown in Table 1. The mean age was 39 years old, but the age distribution was skewed to left and closely resembled the Sarawak population [47, 64] (Supplementary Fig. 1). There were more female (53%) and a higher proportion of individuals of Chinese ethnicity (46%). The majority of them were from southern zone (83%) and were overweight or obese (70%), but did not report presence of comorbidity (71%), past history of tumour (99%), family history of non-CML tumour (79%), history of smoking (70%), and did not consume alcohol or only consume it during festival/confinement (83%). As expected, the mean TWC, basophil count and eosinophil count were within normal range. The RNA quality was indicated by the sum of copy number (SCN) of the control gene, ABL1. 60% of the samples exhibited good quality, with SCNABL1 of 100,000 or more, meeting the criteria for evaluating a 5-log reduction in molecular response (MR5) or deeper when assessing CML patients on treatment.
Out of the 96 relatives, 16 tested positive for BCR::ABL1 in one or both replicates during Experiment 1. In Experiment 2, eight out of the 16 tested negative for BCR::ABL1 in both replicates (Group A), five tested positivity in one replicate (Group B), and four tested positive in both replicates (Group C) (Table 2).
According to the study operational definition, the four (4.2%) relatives in Group C (designated as R1, R2, R3, and R4) harboured BCR::ABL1 (Table 3). Notably, R2 and R3 were from the same family. There was no repeat blood sampling for R1 to R4 due to various logistical reasons. In September 2022, repeat blood sampling was conducted for three individuals in Group A and two individuals in Group B. All of them tested negative in both replicates of Experiment 1, with a mean SCNABL1 of 115,364.
Although there were more female than male relatives harbouring BCR::ABL1, and all positive relatives are Chinese, the differences were not statistically significant, as well as the other characteristics (Table 4). The characteristics that were significant were the residential zone being in the middle zone and a higher SCNABL1.
Discussion
Higher prevalence of harbouring BCR::ABL1 M-BCR in first-degree relatives of CML patients (current study, StudyR) compared to normal population (our previous study, StudyN)
Previously, we conducted a study, StudyN, to determine the prevalence of harbouring BCR::ABL1 M-BCR in our local adult normal population, using an unbiased sampling method [31]. The sampling method employed a two-stage sampling approach based on the Malaysia Department of Statistics population survey procedure. The first- and second-stage samplings were stratified sampling (selection of enumeration blocks (EB) based on the population density of Kuching Division and Samarahan Division) and cluster sampling (selection of 12 living quarters (LQ) out of all LQs in each EB), respectively. StudyN should be viewed and served as a baseline data.
In our current study, StudyR, we found that four (4.2%) (designated as R1 to R4) out of 96 first-degree relatives of CML patients harboured BCR::ABL1 M-BCR, whereas StudyN showed that one (0.5%) (designated as P1) out of 190 subjects in normal population harboured BCR::ABL1 M-BCR [31]. When considering samples with SCNABL1 ≥ 100,000, StudyR and StudyN revealed that four (7%) out of 57 and one (1%) out of 102 subjects were positive, respectively. These findings suggest a higher prevalence of harbouring BCR::ABL1 in first-degree relatives of CML patients compared to the normal population.
The demographic differences between these two studies (Table 1) initially seem to hinder further comparison. However, further interpretation heightens the significance of the higher prevalence in the relative cohort, as elaborated below.
The mean age in StudyR was 39, compared to 45 in StudyN. The mean age of R1 to R4 was 33.5, compared to 44 for P1. The age difference between StudyR and StudyN heightens the significance of the higher prevalence in relative cohort because CML is more common in older age group of 55 and above [65]. Several studies on normal subjects harbouring BCR::ABL1 also showed a higher prevalence in older age groups [20, 25, 27]. The younger age in StudyR corresponds to the younger mean age of diagnosis in the case reports of familial CML, which is 46 (median 49, range 0.8 to 73) (Supplementary Table 3).
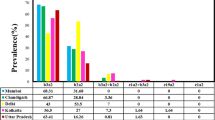
The prevalences of harbouring BCR::ABL1 M-BCR in StudyR were 5.5% and 2.1% for female and male relatives, respectively, while in StudyN it was 1.3% for male normal population. This finding is inconsistent with existing knowledge, as CML is known to be male predominant globally, with a male-to-female ASIR (ASIR-M:F) ratio of about 1.2 to 1.3 between 1990 and 2017 [46]. Interestingly, Meza-Espinoza JP et al. [61] also showed a female predominance in their study. The positive rate of female and male was 40% and 18.8%, respectively, in the relative group, and 31.3% and 15%, respectively, in the control group. Thus, there is a possibility that familial influence in CML occurrence is more pronounced in female than in male.
The positive relatives in StudyR were all Chinese, while the positive subject in StudyN was Malay. This finding is inconsistent with our local CML epidemiology. The ASIR of adult CML in Sarawak was higher in Malay, 0.7 per 100,000 population, compared to Chinese, 0.4, from 1996 to 2015 [47]. This might suggest a stronger familial influence in CML occurrence among Chinese individuals, while a stronger non-familial risk factor may be present and causing a higher occurrence of CML in Malay.
BCR::ABL1–qPCRIS level
Considering data from Experiment 1, the BCR::ABL1–qPCRIS level in StudyR and StudyN were similar, ranging from 0.0017%IS to 0.0071%IS in StudyR and 0.0023%IS to 0.0032%IS in StudyN [31]. The lowest detectable BCR::ABL1 level in standard clinical haematological practice is around MR4 (0.01%IS), MR4.5 (0.0032%IS), and MR5 (0.001%IS), indicating a good response in CML patients receiving treatment [66]. This finding supports the argument against employing more expensive BCR::ABL1–qPCRIS test detecting response deeper than MR4.5 in clinical practice.
Besides StudyR and StudyN, to our knowledge, only Fenu E et al. have performed BCR::ABL1–qPCRIS. The levels ranged between 0.006%IS and 0.016% IS in four subjects [30], which is similar to StudyR and StudyN. Only two of them were re-tested after 10 days and three months, respectively, and the results were negative [30].
The higher mean SCNABL1 of the four positive relatives compared to the negative relatives in StudyR (p = 0.015) was within expectation. A good quality sample is required to detect a low level of BCR::ABL1 in normal population.
Study limitation
The main study limitation of StudyR is the small sample size. The lack of statistical significance in the association between female gender and Chinese ethnicity in the positive relatives may be attributed to this small sample size. Conducting a future study with similar demographics between a relative and normal cohort is ideal, but logistical challenges may arise. Using the results of StudyR and StudyN, along with OpenEpi software with a two-sided confidence level (1-alpha) of 95, 80% power, a 1:1 ratio of controls to cases, and hypothetical exposure proportions of 0.5 for controls and 4 for cases, the sample size needed for an unmatched case-control study was estimated to be about 280 in each case and control group.
Residential zone differed between StudyR and StudyN. R1 to R4 resided in the middle zone of Sarawak, as did three and all subjects in Group A and B, respectively. StudyN was conducted only in the southern zone [31], making it uncertain how residential location might influence our findings. We recommend a study investigating the prevalence of harbouring BCR::ABL1 in the normal population within the middle zone. Notably, the incidence rate of CML in southern and middle zone of Sarawak between 1996 and 2015 was 0.5 and 0.4 per 100,000 population, respectively (unpublished data in Kuan JW et al. [47]).
Repeat blood sampling is ideal for rectification and follow-up in positive cases, but unfortunately, it wasn’t possible for participants R1 to R4 due to logistical constraints. Repeat blood sampling was done for P1 in StudyN five months after detecting BCR::ABL1 and the result was negative with SCNABL1 of 232,077 [31].
The familial influence in CML occurrence might be diluted, for example in offspring, because of the presence of the other parent’s genetic features. In StudyR, three (7.7%) out of 39 siblings and one (5.5%) out of 18 parents were positive. None of 39 offspring was positive. Further research on the “dilutional genetic effect” in larger studies would be of interest. Notably, protective genetic factors are influential, as evidenced by immunotherapy like interferon in CML treatment. Another evidence comes from CML treatment-free remission studies, where NK-cell-based immune surveillance may contribute to CML control after TKI cessation.
Conclusion
Our study showed that the prevalence of harbouring BCR::ABL1 in the first-degree relatives of known CML patients was approximately 4%, higher than the 0.5% prevalence observed in the normal population. This suggests that familial influence in CML occurrence might exist but could be surpassed by other more dominant influences, such as genetic dilutional effects and protective genetic factors. Further investigation into this topic is warranted, ideally through larger studies with longer follow-up periods.
Data availability
The data that support the findings of this study are available from UNIMAS but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors (Prof Dr Kuan Jew Win) upon reasonable request and with permission of UNIMAS.
Abbreviations
- AP:
-
acceleration phase of CML
- ASIR:
-
Age-standardised Incidence Rate
- BC:
-
blast crisis of CML
- BMA:
-
bone marrow aspiration
- CML:
-
chronic myeloid leukaemia
- CP:
-
chronic phase of CML
- FBC:
-
full blood count
- IS:
-
International Scale
- M-BCR:
-
major transcripts of BCR::ABL1, namely e13a2 and e14a2
- MR:
-
molecular response in the quantity unit of log reduction
- M:F:
-
male-to-female
- PBF:
-
peripheral blood film
- PCR:
-
polymerase chain reaction
- Ph:
-
Philadelphia chromosome
- pre-CP:
-
pre-clinical CML or pre-clinical phase of CML
- qPCRIS :
-
IS-standardised real-time quantitative polymerase chain reaction
- SCN:
-
sum of copy number
- TKI:
-
tyrosine kinase inhibitor
- TWC:
-
total white cell count
- UNIMAS:
-
Universiti Malaysia Sarawak
References
Vardiman JW, Melo JV, Baccarani M, Thiele J et al. Chronic myeloid leukemia, BCR-ABL1-positive. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri AS, Stein H, editors. WHO classification of tumors of hematopoietic and lymphoid tissues. Revised 4th ed. Lyon: IARC Press; 2017. p. 32– 7.
Hochhaus A, Larson RA, Guilhot F, Radich JP, Branford S, Hughes TP, et al. Long-term outcomes of Imatinib Treatment for chronic myeloid leukemia. N Engl J Med. 2017;376(10):917–27.
Kuan JW, Melaine Michael S. The epidemiology of chronic myeloid leukaemia in southern Sarawak, Borneo Island. Med J Malaysia. 2018;73(2):78–85.
Khoury JD, Solary E, Abla O, Akkari Y, Alaggio R, Apperley JF, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: myeloid and Histiocytic/Dendritic neoplasms. Leukemia. 2022;36(7):1703–19.
Lauseker M, Hanfstein B, Haferlach C, Schnittger S, Pfirrmann M, Fabarius A, et al. Equivalence of BCR-ABL transcript levels with complete cytogenetic remission in patients with chronic myeloid leukemia in chronic phase. J Cancer Res Clin Oncol. 2014;140(11):1965–9.
Kuan JW, Su AT, Leong CF, Osato M, Sashida G. Systematic review of pre-clinical chronic myeloid leukaemia. Int J Hematol. 2018;108(5):465–84.
Canellos GP, Whang-Peng J. Philadelphia-chromosome-positive preleukaemic state. Lancet. 1972;2(7789):1227–8.
Berman E, Strife A, Wisniewski D, Desai S, Gulati S, Jhanwar S, et al. Duration of the preclinical phase of chronic myelogenous leukemia: a case report. Blood. 1991;78(11):2969–72.
Hudnall SD, Northup J, Panova N, Suleman K, Velagaleti G. Prolonged preleukemic phase of chronic myelogenous leukemia. Exp Mol Pathol. 2007;83(3):484–9.
Shani D, Malik A. Incidental diagnosis of CML in a patient with anemia and IgG lamda monoclonal protein in blood. Ann Hematol Oncol. 2009;88(10):1041.
Bayraktar S, Goodman M. Detection of BCR-ABL positive cells in an asymptomatic patient: a Case Report and Literature Review. Case Rep Med. 2010;2010:939706.
Roper N, DeAngelo DJ, Kuo F, Dal Cin P, Ghobrial I, Aster JC. An asymptomatic 61-year-old man with BCR-ABL-positive bone marrow following autologous transplantation for multiple myeloma. Am J Hematol. 2010;85(12):944–6.
Aye LL, Loghavi S, Young KH, Siddiqi I, Yin CC, Routbort MJ, et al. Preleukemic phase of chronic myelogenous leukemia: morphologic and immunohistochemical characterization of 7 cases. Ann Diagn Pathol. 2016;21:53–8.
Morita K, Nakamura F, Taoka K, Satoh Y, Iizuka H, Masuda A, et al. Incidentally-detected t(9;22)(q34;q11)/BCR-ABL1- positive clone developing into chronic phase chronic myeloid leukaemia after four years of dormancy. Br J Haematol. 2016;174(5):815–7.
Alsidawi S, Ghose A, Qualtieri J, Radhakrishnan N. A Case of Multiple Myeloma with Metachronous Chronic Myeloid Leukemia Treated Successfully with Bortezomib, Dexamethasone, and Dasatinib. Case Reports in Oncological Medicine. 2014;2014.
Abecasis M, Cross NCP, Brito M, Ferreira I, Sakamoto KM, Hijiya N et al. Is cancer latency an outdated concept? Lessons from chronic myeloid leukemia. Leukemia. 2020.
Rivera D, Cui W, Gao J, Peker D, Zhang Q-Y, Dewar R et al. Aleukemic chronic myeloid leukemia without Neutrophilia and Thrombocytosis: a Report from the < em > BCR::ABL1 Pathology Group. Mod Pathol. 2024;37(2).
Hauser RG, Esserman D, Beste LA, Ong SY, Colomb DG Jr, Bhargava A, et al. A machine learning model to successfully predict future diagnosis of Chronic Myelogenous Leukemia with Retrospective Electronic Health Records Data. American Journal of Clinical Pathology; 2021.
Kuan JW, Su AT, Leong CF, Osato M, Sashida G. Systematic review of normal subjects harbouring BCR-ABL1 Fusion Gene. Acta Haematol. 2020;143(2):96–111.
Biernaux C, Loos M, Sels A, Huez G, Stryckmans P. Detection of major bcr-abl gene expression at a very low level in blood cells of some healthy individuals. Blood. 1995;86(8):3118–22.
Bose S, Deininger M, Gora-Tybor J, Goldman JM, Melo JV. The presence of typical and atypical BCR-ABL fusion genes in leukocytes of normal individuals: biologic significance and implications for the assessment of minimal residual disease. Blood. 1998;92(9):3362–7.
Ravetto PF, Agarwal R, Chiswick ML, D’Souza SW, Eden OB, Taylor GM. Absence of leukaemic fusion gene transcripts in preterm infants exposed to diagnostic x rays. Archives Disease Child Fetal Neonatal Ed. 2003;88(3):F237–44.
Hsu H, Tan L, Au L, Lee Y, Lieu C, Tsai W, et al. Detection of bcr-abl gene expression at a low level in blood cells of some patients with essential thrombocythemia. J Lab Clin Med. 2004;143(2):125–9.
le Coutre P, Reinke P, Neuhaus R, Trappe R, Ringel F, Lalancette M, et al. BCR-ABL positive cells and chronic myeloid leukemia in immune suppressed organ transplant recipients. Eur J Haematol. 2010;84(1):26–33.
Song J, Mercer D, Hu X, Liu H, Li MM. Common leukemia- and lymphoma-associated genetic aberrations in healthy individuals. J Mol Diagnostics: JMD. 2011;13(2):213–9.
Boquett JA, Alves JRP, de Oliveira CEC. Analysis of BCR/ABL transcripts in healthy individuals. Genet Mol Research: GMR. 2013;12(4):4967–71.
Ismail SI, Naffa RG, Yousef A-MF, Ghanim MT. Incidence of bcr–abl fusion transcripts in healthy individuals. Mol Med Rep. 2014;9(4):1271–6.
van Rhee F, Hochhaus A, Lin F, Melo JV, Goldman JM, Cross NC. p190 BCR-ABL mRNA is expressed at low levels in p210-positive chronic myeloid and acute lymphoblastic leukemias. Blood. 1996;87(12):5213–7.
Winn-Deen ES, Helton B, Van Atta R, Wong W, Peralta J, Wang J, et al. Development of an integrated assay for detection of BCR-ABL RNA. Clin Chem. 2007;53(9):1593–600.
Fenu E, O’Neill SS, Insuasti-Beltran G. BCR-ABL1 p210 screening for chronic myeloid leukemia in patients with peripheral blood cytoses. Int J Lab Hematol. 2021;43(6):1458–64.
Kuan JW, Su AT, Tay SP, Fong IL, Kubota S, Su’ut L, et al. Low prevalence of the BCR-ABL1 fusion gene in a normal population in southern Sarawak. Int J Hematol. 2020;111(2):217–24.
Tokuhata GK, Neely CL, Williams DL. Chronic myelocytic leukemia in identical twins and a sibling. Blood. 1968;31(2):216–25.
Gunz FW, Gunz JP, Veale AM, Chapman CJ, Houston IB. Familial leukaemia: a study of 909 families. Scand J Haematol. 1975;15(2):117–31.
Avilés A, Sinco A, Zapata N, Ambriz R, Pizzuto J. [Familial chronic myelogenous leukemia. Report of 3 cases in a family]. Sangre (Barc). 1982;27(5):953–8.
Lillicrap DA, Sterndale H. Familial chronic myeloid leukaemia. Lancet. 1984;2(8404):699.
Spremolla G, Simi P, Bilancia D, Papineschi F. [Familial chronic myeloid leukemia. Description of 2 cases in brothers]. Recenti Prog Med. 1987;78(2):69–72.
Horwitz M, Goode EL, Jarvik GP. Anticipation in familial leukemia. Am J Hum Genet. 1996;59(5):990–8.
Kapsali E, Tsiara S, Christou L, Panteli A, Bourantas KL. Two siblings with chronic myelogenous leukemia. J Exp Clin Cancer Res. 2000;19(4):541–3.
Lessen DS, Novoselac AV, Hellman G, Tapia A, Ratner LH, Najfeld V. Chronic myelogenous leukemia occurring in two brothers diagnosed 26 years apart. Cancer Genet Cytogenet. 2005;160(1):73–5.
Caocci G, Atzeni S, Vacca A, Orrù N, Ledda A, La Nasa G. Familial occurrence of chronic myeloid leukemia. Leuk Lymphoma. 2009;50(5):854–6.
Malak S, Labopin M, Saint-Martin C, Bellanne-Chantelot C, Najman A. Long term follow up of 93 families with myeloproliferative neoplasms: life expectancy and implications of JAK2V617F in the occurrence of complications. Blood Cells Mol Dis. 2012;49(3–4):170–6.
Prasad S, Bala S, Chennamaneni R, Lakshmi KM, Sadashivudu G. Chronic myeloid leukemia in mother and son: what are the odds? Pediatr Blood Cancer. 2019;66(8):e27772.
Aitken MJL, Benton CB, Issa GC, Sasaki K, Yilmaz M, Short NJ. Two cases of possible familial chronic myeloid leukemia in a family with extensive history of Cancer. Acta Haematol. 2021;144(5):585–90.
Tsumura AM, Druker BJ, Brewer D, Press R, Braun TP. BCR-ABL + chronic myeloid leukemia arising in a family with inherited ANKRD26-Related Thrombocytopenia. JCO Precis Oncol. 2021;5.
Verrou E, Tsirou K, Karampatzakis N, Triantafyllou T, Sevastoudi A, Grigoriadou GI, et al. Chronic myelogenous leukemia occurring in two brothers: the opposite sides of the same coin? Leuk Res Rep. 2021;16:100261.
Dong Y, Shi O, Zeng Q, Lu X, Wang W, Li Y, et al. Leukemia incidence trends at the global, regional, and national level between 1990 and 2017. Exp Hematol Oncol. 2020;9:14.
Kuan JW, Su AT, Wahab M, Hamdan A, Hashim J, Kiyu A, et al. The epidemiology of haematological cancers in Sarawak, Malaysia (1996 to 2015). BMC Cancer. 2023;23(1):563.
Tomonaga M. Leukaemia in Nagasaki atomic bomb survivors from 1945 through 1959. Bull World Health Organ. 1962;26:619–31.
Lamm SH, Engel A, Joshi KP, Byrd DM 3rd, Chen R. Chronic myelogenous leukemia and benzene exposure: a systematic review and meta-analysis of the case-control literature. Chem Biol Interact. 2009;182(2–3):93–7.
Strom SS, Yamamura Y, Kantarijian HM, Cortes-Franco JE. Obesity, weight gain, and risk of chronic myeloid leukemia. Cancer Epidemiol Biomarkers Prev. 2009;18(5):1501–6.
Musselman JR, Blair CK, Cerhan JR, Nguyen P, Hirsch B, Ross JA. Risk of adult acute and chronic myeloid leukemia with cigarette smoking and cessation. Cancer Epidemiol. 2013;37(4):410–6.
Posthuma EF, Falkenburg JH, Apperley JF, Gratwohl A, Roosnek E, Hertenstein B, et al. HLA-B8 and HLA-A3 coexpressed with HLA-B8 are associated with a reduced risk of the development of chronic myeloid leukemia. The Chronic Leukemia Working Party of the EBMT. Blood. 1999;93(11):3863–5.
Posthuma EF, Falkenburg JH, Apperley JF, Gratwohl A, Hertenstein B, Schipper RF, et al. HLA-DR4 is associated with a diminished risk of the development of chronic myeloid leukemia (CML). Chronic Leukemia Working Party of the European blood and Marrow Transplant Registry. Leukemia. 2000;14(5):859–62.
Yasukawa M, Ohminami H, Kojima K, Inokuchi K, Nishimura Y, Fujita S. Analysis of HLA-DRB1 alleles in Japanese patients with chronic myelogenous leukemia. Am J Hematol. 2000;63(2):99–101.
Rosas-Cabral A, Irigoyen L, Alvarado L, Vela-Ojeda J, Ayala-Sánchez M, Tripp-Villanueva F, et al. HLA CW3 and HLA CW4 have a protective effect on acquisition of chronic myeloid leukemia on Mexican patients. Rev Invest Clin. 2003;55(4):423–8.
Chhaya SU. Human leukocyte antigens in Indian patients with chronic myeloid leukemia. Leuk Lymphoma. 2006;47(2):291–5.
Zhang MY, Chen FY, Zhong H. Meta-analysis of human leukocyte antigen genetic polymorphisms and susceptibility to chronic myelogenous leukemia in Chinese population. Leuk Res. 2011;35(12):1564–70.
Bruzzoni-Giovanelli H, González JR, Sigaux F, Villoutreix BO, Cayuela JM, Guilhot J, et al. Genetic polymorphisms associated with increased risk of developing chronic myelogenous leukemia. Oncotarget. 2015;6(34):36269–77.
Björkholm M, Kristinsson SY, Landgren O, Goldin LR. No familial aggregation in chronic myeloid leukemia. Blood. 2013;122(3):460–1.
Gunnarsson N, Höglund M, Stenke L, Sandin F, Björkholm M, Dreimane A, et al. No increased prevalence of malignancies among first-degree relatives of 800 patients with chronic myeloid leukemia: a population-based study in Sweden. Leukemia. 2017;31(8):1825–7.
Meza-Espinoza JP, Vasquez-Jimenez EA, Barajas-Torres RL, Magana-Torres MT, Gonzalez-Garcia JR. BCR/ABL1 transcripts in healthy individuals: a comparative analysis between First-Degree relatives of patients with chronic myelogenous leukemia and subjects without antecedents of the Disease. Ann Clin Lab Sci. 2019;49(6):703–9.
Hasle H, Olsen JH. Cancer in relatives of children with myelodysplastic syndrome, acute and chronic myeloid leukaemia. Br J Haematol. 1997;97(1):127–31.
Cross NC, White HE, Colomer D, Ehrencrona H, Foroni L, Gottardi E, et al. Laboratory recommendations for scoring deep molecular responses following treatment for chronic myeloid leukemia. Leukemia. 2015;29(5):999–1003.
Population by state. administrative district and sex, 2016–2018 [Internet]. [cited 6th September 2022]. Available from: https://www.dosm.gov.my/v1/index.php?r=column3/accordion&menu_id=amZNeW9vTXRydTFwTXAxSmdDL1J4dz09.
Miranda-Filho A, Piñeros M, Ferlay J, Soerjomataram I, Monnereau A, Bray F. Epidemiological patterns of leukaemia in 184 countries: a population-based study. Lancet Haematol. 2018;5(1):e14–24.
Hochhaus A, Baccarani M, Silver RT, Schiffer C, Apperley JF, Cervantes F et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020.
Acknowledgements
We would like to thank Dr. Isabel Fong Lim for advice during the conduct of the study and Dr. Paul Cliff Simon Divis for allowing the usage of laminated flow hood in Malaria Research Centre, UNIMAS. We also would like to thank UNIMAS for all the support including publication support.
Funding
Open Access funding provided by Universiti Malaysia Sarawak. This study was funded by UNIMAS under Research ID: F05/IMPACT/2114/2021.
Open Access funding provided by Universiti Malaysia Sarawak.
Author information
Authors and Affiliations
Contributions
J.W. Kuan: conceived, designed, planned and conducted the whole research, collected, analysed and interpreted the data and wrote the manuscript; A.T. Su: designed, planned and conducted the samplings, provided statistical consultation; S.P. Sim: provided technical consultation and support for the study; S.P. Tay: performed full blood count and smear of peripheral blood film.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study received approval from the Ethic Committee of Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak (UNIMAS) (ref no: UNIMAS/TNC(PI)/09–65/01 [3]). It adhered to the Malaysian Good Clinical Practice Guideline, aligning with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participating relatives.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kuan, J.W., Su, A.T., Sim, SP. et al. Higher prevalence of harbouring BCR::ABL1 in first-degree relatives of chronic myeloid leukaemia (CML) patients compared to normal population. BMC Cancer 24, 734 (2024). https://doi.org/10.1186/s12885-024-12102-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12102-2