
Abstract
Background
Both first and second-generation EGFR-TKIs are recommended in advanced NSCLC with common EGFR mutations. However, there are few data on the difference in efficacy of EGFR-TKIs based on the type of EGFR mutation and agents.
Methods
This retrospective real-world study evaluated the outcomes and clinicopathologic characteristics, including the type of EGFR mutations, of 237 advanced NSCLC patients treated with first- or second-generation (afatinib) EGFR-TKIs as first-line therapy.
Results
The median progression-free survival (PFS) and overall survival (OS) of all patients were 11 months (M) and 25M, respectively. In the univariate analysis, patients with exon 19 deletion (del) (n=130) had significantly longer median OS compared to those with other mutations (L858R: 84, others: 23) (30 vs. 22 M, p=0.047), without a difference in PFS (p=0.138). Patients treated with afatinib (n=60) showed significantly longer median OS compared to those treated with first-generation TKIs (gefitinib: 159, erlotinib: 18) (30 vs. 23 M, p=0.037), without a difference in PFS (p=0.179). In patients with exon 19 del, there was no significant difference in median PFS (p=0.868) or OS (p=0.361) between patients treated with afatinib and those treated with first-generation TKIs, while significantly better PFS (p=0.042) and trend in OS (p=0.069) were observed in patients receiving afatinib in other mutations. Exon 19 del was independently associated with favorable OS (p=0.028), while age >70 years (p=0.017), ECOG performance status ≥2 (p=0.001), primary metastatic disease (p=0.007), and synchronous brain metastasis (p=0.026) were independent prognostic factors of poor OS.
Conclusions
The EGFR exon 19 del was associated with favorable OS in advanced NSCLC patients receiving first-line EGFR-TKIs. Moreover, in patients with exon 19 del, first-generation TKIs seem to be a reasonable treatment option if osimertinib is unavailable.
Similar content being viewed by others

Background
Non-small cell lung cancer (NSCLC) is one of the most common neoplasms, and the leading cause of cancer-related mortality in several countries, including South Korea [1,2,3]. Approximately 65% of patients with NSCLC are diagnosed with advanced status [3], and the clinical outcome of advanced NSCLC with a median overall survival (OS) of 11–22 months remains unsatisfactory, despite advances of palliative chemotherapy [2, 4].
Since NSCLC patients with epidermal growth factor receptor (EGFR)-activating mutations (exon 19 deletion and exon 21 L858R mutation), which are observed in 20–40% of Asian patients, demonstrated high response to EGFR tyrosine kinase inhibitors (TKIs) [5, 6], EGFR-TKIs have been considered as the standard first-line therapy of EGFR mutation-positive advanced NSCLC [2, 7]. In the NCCN [8] and ESMO guidelines [9], osimertinib, third-generation TKI, is recommended as a first-line treatment based on the results of FLAURA trial, which reported a significant prolongation of progression-free survival (PFS) compared to first-generation EGFR-TKIs (gefitinib, erlotinib) [10]. However, the OS benefit of osimertinib was rather marginal (median OS: 38.6 vs. 31.8 months, P = 0.046), and there was no OS benefit for Asian patients and those with EGFR L858R mutation [11]. Therefore, first and second-generation EGFR-TKIs are still recommended equally, especially for Asian patients. Although there are some real-world data on the comparison of outcomes between first- and second-generation EGFR-TKIs [12,13,14,15,16], only two trials have compared the efficacy of first-line first- and second-generation EGFR-TKIs, reporting conflicting results [17,18,19,20].
The presence of differences in sensitivity to EGFR-TKIs among various types of EGFR mutation remains a subject of debate. Several studies demonstrated longer PFS and/or OS in patients with exon 19 deletion compared to those with L858R mutation [15, 21,22,23,24,25,26,27,28,29]. On the other hand, no significantly different effect of EGFR-TKIs based on the types of EGFR mutation was observed in other retrospective studies and phase III trials [30,31,32,33,34,35,36]. In addition, many studies included patients who received EGFR-TKIs as variable lines [22, 23, 25, 29, 30].
Therefore, in the present study, the clinical outcomes of EGFR mutation-positive advanced NSCLC patients treated with first- and second-generation EGFR-TKIs as their first-line treatment were investigated in terms of the EGFR mutation subtypes as well as the agents.
Methods
Study population
All EGFR mutation-positive advanced NSCLC patients who started first-line first- or second-generation EGFR-TKIs therapy between July 2011 and June 2018 at our institution were retrospectively identified. The eligibility criteria were cytologically or histologically confirmed NSCLC, and either stage IV based on the 7th edition of the American Joint Committee on Cancer (AJCC) [37] or stage IIIB/recurrent disease unsuitable for definitive local treatment. Some patients and methods of this study cohort were included in previous retrospective studies on EGFR-TKIs in NSCLC [21, 38]. Nonetheless the criteria for eligibility criteria of this study were slightly different from those of the previous studies, with longer follow-up duration of patients.
Clinical review
The clinical information of eligible patients was retrospectively reviewed. Data collected on the patients included patient characteristics (age, gender, smoking history), performance status (PS) based on the Eastern Cooperative Oncology Group (ECOG) performance scale, histology, disease status at the start of EGFR-TKIs, presence of synchronous brain metastasis, second- or further-line of therapy, and information of survival status.
EGFR mutation analysis
A direct sequencing method was applied for detecting EGFR mutation without routine tumor enrichment. Retrieved Formalin-fixed, paraffin embedded (FFPE) tumor samples were used for genomic DNA extraction by the QIAmp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany). Polymerase chain reaction (PCR) amplification of EGFR exons 18 to 21, using intron-based primers was followed. Sequencing was performed in both the forward and reverse directions. Since September 2014, the peptide nucleic acid-locked nucleic acid (PNA-LNA) PCR clamp method has been applied in almost all cases. Genomic DNA of EGFR mutation hot-spots were amplified by PCR with a PNA clamp primer synthesized from a PNA with a wild-type sequence and detected by a fluorescent primer that incorporates locked nucleic acids. This method for preferential amplification of the mutant sequence can detect EGFR mutation in specimens containing 100 to 1000 excess copies of wild-type EGFR sequence [39].
Statistical analysis
The Kaplan–Meier method was used for the calculation of OS and PFS. The time from the start day of the EGFR-TKI treatment to death and the time to disease progression or death by any cause were defined as OS and PFS, respectively. In case of surviving patients at the time of data cut-off with uncertain disease status, the data were censored on the last evaluation date at our institution for PFS. Data on the survivors were censored at the last follow-up for OS. The log-rank test was used for the analysis of the differences between the survival curves. Fisher’s exact test was applied to compare categorical variables among the different groups. The joint effects of several variables on survival were determined by the Cox proportional-hazards regression model, including factors with p-values < 0.1 in the univariate analysis. All statistical analyses were performed two-sided using SPSS for Windows 20.0 software.
Statement of ethics
This research protocol was approved by the Institutional Review Board (IRB) of Ajou University Hospital, Suwon, Republic of Korea (AJOUIRB-MDB-2019-394) and all methods were performed in accordance with the relevant guidelines and regulations. The study was designed retrospectively. Written informed consent from patients was not required in accordance with guidelines of the IRB of Ajou University Hospital.
Results
Patient characteristics
A total of 237 EGFR-mutation-positive, advanced NSCLC patients, who received first- (gefitinib, erlotinib) or second-generation (afatinib) EGFR-TKIs as first-line palliative chemotherapy, were analyzed. Table 1 describes the clinicopathological characteristics of patients. Almost all patients underwent EGFR-TKI treatment in the routine practice, except for four patients who received gefitinib in a clinical trial as a first-line TKI. The median age of all patients was 67 (23–91), and 138 (58.2%) patients were female. Primary metastatic and recurrent disease were diagnosed in 199 (84%) and 38 (16%) patients, respectively. The ECOG PS was 0 or 1 in 194 (81.9%) patients, 2 in 31 patients, 3 in 11 patients, and 4 in 1 patient. Synchronous brain metastasis was identified in 77 (32.5%) patients. Among the 220 patients with disease progression after first-line EGFR-TKI treatment, 37 (16.8%) patients received third-generation EGFR-TKIs (osimertinib: 28, olmutinib: 9 patients) as second- (27 patients) or further-lines (10 patients).
Direct sequencing (82 patients), the PNA-LNA PCR clamp method (152 patients), and next-generation sequencing (3 patients) were used for detection of EGFR mutation subtypes. The most common type of EGFR mutation was the exon 19 deletion (130 patients, 54.9%), followed by L858R mutation in exon 21 (84 patients, 35.4%). Moreover, 18 patients had uncommon mutations (exon 18 mutation: 8, exon 18 with exon 20 mutation: 3, exon 20 mutation: 3, exon 21 mutation: 4 [L861Q: 3, other mutation: 1]), and five patients dual mutations (exon 19 deletion with L858R mutation: 1, L858R mutation with exon 18 mutation: 1, exon 19 deletion with exon 20 mutation: 1, and L858R and L861Q mutations: 2). The baseline characteristics were not statistically different based on the EGFR mutation subtype. However, the proportion of patients who received third-generation TKIs after progression was significantly higher in patients with exon 19 deletion compared to those with other mutations (L858R and uncommon or dual mutations) (Table 1).
A total of 159 (67.1%), 18 (7.6%), and 60 (25.3%) patients were treated with gefitinib, erlotinib, and afatinib, respectively. The baseline characteristics of patients treated with afatinib in this cohort were significantly associated with younger age, male, smoker, better performance status, and exon 19 deletion (Table 1).
Progression-free and overall survival
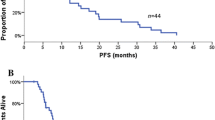
The median follow-up duration was 43 (35–103) months for the survivors (42 patients) at the time of analysis. Only one patient was lost to follow-up for survival status after receiving a 14-day prescription of gefitinib and was excluded from the analysis for PFS and OS. The median PFS and OS from the start of EGFR-TKI treatment for all patients were 11 and 25 months, respectively, while those for the 214 patients with EGFR-activating mutation were 12 and 26 months. Patients with exon 19 deletion had significantly longer median OS compared to those with other mutations (30 vs. 22 months, p=0.047, Fig. 1B), without a difference in PFS (12 vs. 9 months, p=0.138, Fig. 1A). Patients treated with afatinib showed significantly longer median OS (30 vs. 23 months, p=0.037, Fig. 2B) compared to those treated with first-generation TKIs, without a difference in PFS (14 vs. 10 months, p=0.179, Fig. 2A). In the multivariate analysis, EGFR exon 19 deletion showed independent association with favorable OS (p=0.028), while age >70 years (p=0.017), ECOG performance status ≥2 (p=0.001), primary metastatic disease (p=0.007), and synchronous brain metastasis (p=0.026) were independent prognostic factors for unfavorable OS (Table 2).

A Progression-free survival and (B) overall survival from the start of EGFR-TKI according to EGFR mutation subtypes. Exon 19 deletion: 130 patients, others: 106 patients (L858R: 83, uncommon mutations: 18, dual mutations: 5). Censoring was indicated by vertical lines

A Progression-free survival and (B) overall survival from the start of EGFR-TKI according to types of tyrosine kinase inhibitors. Exon 19 deletion: 130 patients, others: 106 patients (L858R: 83, uncommon mutations: 18, dual mutations: 5). Censoring was indicated by vertical lines
In patients with EGFR exon 19 deletion, significant differences were not observed in median PFS (12 vs. 12 months, p=0.868) and OS (31 vs. 28 months, p=0.361) between patients treated with afatinib and those treated with first-generation TKIs. However, afatinib resulted in significantly better PFS (15 vs. 9 months, p=0.042) and OS trend (27 vs. 19 months, p=0.069) compared to first-generation TKIs in patients with other EGFR mutations (Table 3). In patients receiving first-generation EGFR-TKIs, EGFR exon 19 deletion was significantly associated with better median PFS (12 vs. 9 months, p=0.031) and OS (28 vs. 19 months, p=0.045) compared to other mutations, while there was no difference in median PFS and OS based on EGFR mutation subtypes in those treated with afatinib (Table 3).
Of the patients who experienced disease progression after first-line EGFR-TKI treatment, those treated with third-generation TKIs demonstrated significantly longer median OS (44 months) from the start of first-line treatment compared to others (183 patients, 20 months, p<0.0001) as well as those who received cytotoxic agents with or without first- or second-generation TKIs (96 patients, 24 months, p=0.006) (Fig. 3).

Overall survival from the start of 1st line treatment according to the 2nd or further line agents in patients with progressive disease after EGFR TKI. A Exon 19 deletion: 124 patients, others: 96 patients (L858R: 74, uncommon mutations: 17, dual mutations: 5) and (B) Exon 19 deletion: 81 patients, others: 52 patients (L858R: 39, uncommon mutations: 12, dual mutation: 1). Censoring was indicated by vertical lines
Discussion
In several retrospective/prospective studies and meta-analyses of those studies, first-generation EGFR-TKI therapy has revealed more favorable outcomes in patients with EGFR exon 19 deletion when compared to those with L858R mutation, especially in terms of PFS [21, 24, 26, 28]. Regarding second-generation EGFR-TKIs, an OS survival benefit of afatinib treatment was observed in patients with exon 19 deletion but not those with L858R mutation in a combined analysis of phase III studies (LUX-Lung 3, LUX-Lung 6) comparing cisplatin doublet chemotherapy with afatinib as a first-line setting [40]. A few molecular mechanisms were suggested, including higher drug-binding affinity [41, 42], different downstream signaling after drug treatment, and lesser baseline combined T790M mutation in exon 19 deletion [28], for the better efficacy of EGFR-TKIs in exon 19 deletion compared with L858R mutation [41,42,43]. However, subsequent retrospective studies and a metanalysis including afatinib and dacomitinib showed no significant differences in outcomes, especially OS, based on the type of EGFR mutation in first-line setting [27, 29, 36]. Similarly, in our cohort, patients with EGFR exon 19 deletion did not show significantly better outcomes compared with those with other mutations when treated with afatinib, while EGFR exon 19 deletion showed longer PFS and OS in patients treated with first-generation EGFR-TKIs, with an independently favorable prognostic significance of exon 19 deletion in terms of OS for all patients. Although the difference in PFS and OS between patients with EGFR exon 19 deletion and other mutations treated with first-generation TKIs is rather small compared with that reported in a previous study on patients with first-line gefitinib treatment, probably due to the longer follow-up duration, which resulted in progression in the majority of patients, the trend toward favorable clinical outcomes in patients with EGFR exon 19 deletion has been observed consistently [21]. The lack of improved PFS in patients with exon 19 deletion in the entire cohort may be explained by no significant difference in PFS based on mutation type in the afatinib group. Moreover, the significantly higher proportion of patients treated with third-generation TKIs after progression in exon 19 deletion compared with other mutations may be one of the possible explanations for favorable OS in patients with exon 19 deletion [44]. However, this result should be validated in further trials including larger numbers of patients.
Furthermore, in our study, patients with EGFR exon 19 deletion revealed almost similar median PFS and OS when they received either first-generation EGFR-TKIs or afatinib, while significantly longer median PFS and a better OS trend were observed in patients with other EGFR mutations receiving afatinib. It remains unclear whether the clinical efficacy of second-generation TKIs is superior to that of first-generation TKIs, as only dacomitinib has demonstrated an OS benefit compared to gefitinib [20]. Moreover, with second-generation TKIs, even with dose modification, the incidence of overall and grade ≥ 3 adverse events resulting in negative effects on patients’ quality of life (e.g., skin toxicity and diarrhea) is usually higher than that with first-generation TKIs [16,17,18, 45]. These concerns about the toxicity of afatinib may be reflected in the higher proportion of younger patients and the better performance status of patients treated with afatinib in the present study cohort. Because a proper agent must be selected based on the risk–benefit balance for each patient in clinical practice, the results of present study suggest that first-generation TKIs can be used more safely in poor performance status or elderly patients without compromising clinical efficacy compared to second-generation TKIs, especially those with exon 19 deletion.
In the FLAURA trial, osimertinib resulted in significant prolongation of PFS with a marginal OS benefit compared to first-generation EGFR-TKIs [10, 11]. However, in Asian patients and those with EGFR L858R mutation, OS benefit of osimertinib was not observed [11]. In the present study, patients treated with third-generation TKIs after first- or second-generation TKI failure showed a median OS of 44 months from the start of first-line therapy, comparable to that of osimertinib (38.6 months) in the FLAURA trial [11]. Considering that prospective data directly comparing second- and third-generation EGFR-TKIs are not currently available, the results of a few studies including ours suggest that first-line second-generation TKIs and sequential third-generation EGFR-TKI treatment may be an effective therapeutic strategy, especially in patients with EGFR L868R mutation [20, 46]. Overall, first-line first- or second-generation EGFR-TKIs may still be a reasonable choice in routine practice due to its cost-effectiveness [47] in countries where first-line osimertinib is not reimbursable, such as Korea.
The current study demonstrated that EGFR exon 19 deletion was associated independently with favorable OS in advanced NSCLC patients treated with first-line EGFR-TKIs. To the best of our knowledge, current study is the first one showing a significantly favorable OS in patients with EGFR exon 19 deletion, when compared with other mutations in advanced NSCLC patients treated with either first- or second-generation EGFR-TKIs as first-line therapy. Moreover, as this study analyzed every EGFR mutation-positive patient who received first-line first- or second-generation EGFR-TKIs therapy during the defined period with a fairly long follow-up duration (minimum follow-up duration of survivors: 35 months), it reflected the patient outcomes of everyday clinical practice.
However, several limitations were included in this study. First, it was retrospective and performed at a single institution. Second, the number of patients who received third-generation TKIs as second- or further-line therapy was small, as second- or further-line osimertinib treatment has been reimbursable by the Korean national health insurance system since late 2017. Finally, the collection of treatment-related adverse events was not planned considering the retrospective nature of this study.
Nonetheless, several clinical implications can be suggested by the results of our study. First, first-generation EGFR-TKIs could still be recommended as a first-line palliative treatment for NSCLC with EGFR exon 19 deletion, especially in elderly and fragile patients. Second, patients and their families could receive more precise explanations regarding the outcomes and further treatment options after EGFR-TKI therapy based on the types of EGFR mutation. Finally, this study recommends that further clinical trials with EGFR-TKIs should still consider the types of EGFR mutation as a stratification factor.
Conclusions
The EGFR exon 19 deletion was correlated with favorable OS in advanced NSCLC treated with first-line EGFR-TKIs. Moreover, in patients with exon 19 deletion, first-generation TKIs seem to be a reasonable treatment option if osimertinib is unavailable.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to the confidentiality of the data of patient but are available from the corresponding author on reasonable request.
Abbreviations
- NSCLC:
-
Non-small cell lung cancer
- OS:
-
Overall survival
- EGFR:
-
Epidermal growth factor receptor
- TKIs:
-
Tyrosine kinase inhibitors
- PFS:
-
Progression-free survival
- AJCC:
-
American Joint Committee on Cancer
- PS:
-
Performance status
- ECOG:
-
Eastern Cooperative Oncology Group
- FFPE:
-
Formalin-fixed, paraffin embedded
- PCR:
-
Polymerase chain reaction
- PNA-LNA:
-
Peptide nucleic acid-locked nucleic acid
- IRB:
-
Institutional review board
References
Jung KW, Won YJ, Kang MJ, Kong HJ, Im JS, Seo HG. Prediction of cancer incidence and mortality in Korea, 2022. Cancer Res Treat. 2022;54(2):345–51.
Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–54.
Reck M, Heigener DF, Mok T, Soria JC, Rabe KF. Management of non-small-cell lung cancer: recent developments. Lancet. 2013;382(9893):709–19.
Rodriguez-Abreu D, Powell SF, Hochmair MJ, Gadgeel S, Esteban E, Felip E, Speranza G, De Angelis F, Domine M, Cheng SY, et al. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: protocol-specified final analysis from KEYNOTE-189. Ann Oncol. 2021;32(7):881–95.
Jang TW, Oak CH, Chang HK, Suo SJ, Jung MH. EGFR and KRAS mutations in patients with adenocarcinoma of the lung. Korean J Intern Med. 2009;24(1):48–54.
Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(21):2129–39.
Reck M, Popat S, Reinmuth N, De Ruysscher D, Kerr KM, Peters S, Group EGW: Metastatic non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014, 25 Suppl 3:iii27-39.
Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman JR, Bharat A, Bruno DS, Chang JY, Chirieac LR, D’Amico TA, et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(5):497–530.
Hendriks LE, Kerr KM, Menis J, Mok TS, Nestle U, Passaro A, Peters S, Planchard D, Smit EF, Solomon BJ et al: Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(4):358–76.
Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, Dechaphunkul A, Imamura F, Nogami N, Kurata T, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–25.
Ramalingam SS, Vansteenkiste J, Planchard D, Cho BC, Gray JE, Ohe Y, Zhou C, Reungwetwattana T, Cheng Y, Chewaskulyong B, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41–50.
Huang MY, Hsieh KP, Huang RY, Hung JY, Chen LT, Tsai MJ, Yang YH. Comparing survival and subsequent treatment of first-line tyrosine kinase inhibitors in patients of advanced lung adenocarcinoma with epidermal growth factor receptor mutation. J Formos Med Assoc. 2022;121(1 Pt 1):170–80.
Kwok WC, Ho JCM, Tam TCC, Ip MSM, Lam DCL. Survival benefits from afatinib compared with gefitinib and erlotinib among patients with common EGFR mutation in first-line setting. Thorac Cancer. 2022;13(14):2057–63.
Bilgin B, Sendur MAN, Yucel S, Celik E, Ozyukseler DT, Ayhan M, Basoglu T, Ilhan A, Akdeniz N, Gulmez A, et al. Real-life comparison of the afatinib and first-generation tyrosine kinase inhibitors in nonsmall cell lung cancer harboring EGFR exon 19 deletion: a Turk Oncology Group (TOG) study. J Cancer Res Clin Oncol. 2021;147(7):2145–52.
Gijtenbeek RGP, Damhuis RAM, van der Wekken AJ, Hendriks LEL, Groen HJM, van Geffen WH. Overall survival in advanced epidermal growth factor receptor mutated non-small cell lung cancer using different tyrosine kinase inhibitors in The Netherlands: a retrospective, nationwide registry study. Lancet Reg Health Eur. 2023;27:100592.
Kim Y, Lee SH, Ahn JS, Ahn MJ, Park K, Sun JM. Efficacy and safety of Afatinib for EGFR-mutant non-small cell lung cancer, compared with Gefitinib or Erlotinib. Cancer Res Treat. 2019;51(2):502–9.
Park K, Tan EH, O’Byrne K, Zhang L, Boyer M, Mok T, Hirsh V, Yang JC, Lee KH, Lu S, et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016;17(5):577–89.
Wu YL, Cheng Y, Zhou X, Lee KH, Nakagawa K, Niho S, Tsuji F, Linke R, Rosell R, Corral J, et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18(11):1454–66.
Paz-Ares L, Tan EH, O’Byrne K, Zhang L, Hirsh V, Boyer M, Yang JC, Mok T, Lee KH, Lu S, et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: overall survival data from the phase IIb LUX-Lung 7 trial. Ann Oncol. 2017;28(2):270–7.
Mok TS, Cheng Y, Zhou X, Lee KH, Nakagawa K, Niho S, Chawla A, Rosell R, Corral J, Migliorino MR, et al. Updated overall survival in a randomized study comparing dacomitinib with gefitinib as first-line treatment in patients with advanced non-small-cell lung cancer and EGFR-activating mutations. Drugs. 2021;81(2):257–66.
Choi YW, Jeon SY, Jeong GS, Lee HW, Jeong SH, Kang SY, Park JS, Choi JH, Koh YW, Han JH, et al. EGFR Exon 19 deletion is associated with favorable overall survival after first-line gefitinib therapy in advanced non-small cell lung cancer patients. Am J Clin Oncol. 2018;41(4):385–90.
Jackman DM, Yeap BY, Sequist LV, Lindeman N, Holmes AJ, Joshi VA, Bell DW, Huberman MS, Halmos B, Rabin MS, et al. Exon 19 deletion mutations of epidermal growth factor receptor are associated with prolonged survival in non-small cell lung cancer patients treated with gefitinib or erlotinib. Clin Cancer Res. 2006;12(13):3908–14.
Sun JM, Won YW, Kim ST, Kim JH, Choi YL, Lee J, Park YH, Ahn JS, Park K, Ahn MJ. The different efficacy of gefitinib or erlotinib according to epidermal growth factor receptor exon 19 and exon 21 mutations in Korean non-small cell lung cancer patients. J Cancer Res Clin Oncol. 2011;137(4):687–94.
Lee VH, Tin VP, Choy TS, Lam KO, Choi CW, Chung LP, Tsang JW, Ho PP, Leung DK, Ma ES, et al. Association of exon 19 and 21 EGFR mutation patterns with treatment outcome after first-line tyrosine kinase inhibitor in metastatic non-small-cell lung cancer. J Thorac Oncol. 2013;8(9):1148–55.
Rosell R, Moran T, Queralt C, Porta R, Cardenal F, Camps C, Majem M, Lopez-Vivanco G, Isla D, Provencio M, et al. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med. 2009;361(10):958–67.
Kim DW, Lee SH, Lee JS, Lee MA, Kang JH, Kim SY, Shin SW, Kim HK, Heo DS. A multicenter phase II study to evaluate the efficacy and safety of gefitinib as first-line treatment for Korean patients with advanced pulmonary adenocarcinoma harboring EGFR mutations. Lung Cancer. 2011;71(1):65–9.
Winfree KB, Molife C, Peterson PM, Chen Y, Visseren-Grul CM, Leusch MS, Beyrer J, Dimou A. Real-world characteristics and outcomes of advanced non-small-cell lung cancer patients with EGFR exon 19 deletions or exon 21 mutations. Future Oncol. 2021;17(22):2867–81.
Zhang Y, Sheng J, Kang S, Fang W, Yan Y, Hu Z, Hong S, Wu X, Qin T, Liang W, et al. Patients with exon 19 deletion were associated with longer progression-free survival compared to those with L858R mutation after first-line EGFR-TKIs for advanced non-small cell lung cancer: a meta-analysis. PLoS One. 2014;9(9):e107161.
Sheng M, Wang F, Zhao Y, Li S, Wang X, Shou T, Luo Y, Tang W. Comparison of clinical outcomes of patients with non-small-cell lung cancer harbouring epidermal growth factor receptor exon 19 or exon 21 mutations after tyrosine kinase inhibitors treatment: a meta-analysis. Eur J Clin Pharmacol. 2016;72(1):1–11.
Igawa S, Kasajima M, Ishihara M, Kimura M, Hiyoshi Y, Asakuma M, Otani S, Katono K, Sasaki J, Masuda N. Comparison of the efficacy of gefitinib in patients with non-small cell lung cancer according to the type of epidermal growth factor receptor mutation. Oncology. 2014;87(4):215–23.
Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362(25):2380–8.
Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–8.
Asahina H, Yamazaki K, Kinoshita I, Sukoh N, Harada M, Yokouchi H, Ishida T, Ogura S, Kojima T, Okamoto Y, et al. A phase II trial of gefitinib as first-line therapy for advanced non-small cell lung cancer with epidermal growth factor receptor mutations. Br J Cancer. 2006;95(8):998–1004.
Sequist LV, Martins RG, Spigel D, Grunberg SM, Spira A, Janne PA, Joshi VA, McCollum D, Evans TL, Muzikansky A, et al. First-line gefitinib in patients with advanced non-small-cell lung cancer harboring somatic EGFR mutations. J Clin Oncol. 2008;26(15):2442–9.
Sugio K, Uramoto H, Onitsuka T, Mizukami M, Ichiki Y, Sugaya M, Yasuda M, Takenoyama M, Oyama T, Hanagiri T, et al. Prospective phase II study of gefitinib in non-small cell lung cancer with epidermal growth factor receptor gene mutations. Lung Cancer. 2009;64(3):314–8.
Huang CH, Ju JS, Chiu TH, Huang AC, Tung PH, Wang CC, Liu CY, Chung FT, Fang YF, Guo YK, et al. Afatinib treatment in a large real-world cohort of nonsmall cell lung cancer patients with common and uncommon epidermal growth factor receptor mutation. Int J Cancer. 2022;150(4):626–35.
Edge SB, American Joint Committee on Cancer.: AJCC cancer staging manual, 7th edn. New York: Springer; 2010.
Choi JH, Choi YW, Lee HW, Kang SY, Jeong GS, Ahn MS, Oh YT, Noh OK, Kim SH, Roh TH, et al. The efficacy of EGFR-tyrosine kinase inhibitor in non-small cell lung cancer patients with synchronous brain metastasis: a real-world study. Korean J Intern Med. 2022;37(2):434–43.
Nagai Y, Miyazawa H, Huqun, Tanaka T, Udagawa K, Kato M, Fukuyama S, Yokote A, Kobayashi K, Kanazawa M et al: Genetic heterogeneity of the epidermal growth factor receptor in non-small cell lung cancer cell lines revealed by a rapid and sensitive detection system, the peptide nucleic acid-locked nucleic acid PCR clamp. Cancer Res. 2005, 65(16):7276-7282.
Yang JC, Wu YL, Schuler M, Sebastian M, Popat S, Yamamoto N, Zhou C, Hu CP, O’Byrne K, Feng J, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015;16(2):141–51.
Mulloy R, Ferrand A, Kim Y, Sordella R, Bell DW, Haber DA, Anderson KS, Settleman J. Epidermal growth factor receptor mutants from human lung cancers exhibit enhanced catalytic activity and increased sensitivity to gefitinib. Cancer Res. 2007;67(5):2325–30.
Carey KD, Garton AJ, Romero MS, Kahler J, Thomson S, Ross S, Park F, Haley JD, Gibson N, Sliwkowski MX. Kinetic analysis of epidermal growth factor receptor somatic mutant proteins shows increased sensitivity to the epidermal growth factor receptor tyrosine kinase inhibitor, erlotinib. Cancer Res. 2006;66(16):8163–71.
Choi YW, Choi JH. Does the efficacy of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor differ according to the type of EGFR mutation in non-small cell lung cancer? Korean J Intern Med. 2017;32(3):422–8.
Liang H, Pan Z, Wang W, Guo C, Chen D, Zhang J, Zhang Y, Tang S, He J, Liang W, et al. The alteration of T790M between 19 del and L858R in NSCLC in the course of EGFR-TKIs therapy: a literature-based pooled analysis. J Thorac Dis. 2018;10(4):2311–20.
Schuler M, Tan EH, O’Byrne K, Zhang L, Boyer M, Mok T, Hirsh V, Yang JC, Lee KH, Lu S, et al. First-line afatinib vs gefitinib for patients with EGFR mutation-positive NSCLC (LUX-Lung 7): impact of afatinib dose adjustment and analysis of mode of initial progression for patients who continued treatment beyond progression. J Cancer Res Clin Oncol. 2019;145(6):1569–79.
Jung HA, Hong MH, Lee HW, Lee KH, Kim IH, Min YJ, Ahn HK, Shim BY, Choi YH, Lee YG, et al. Totality outcome of afatinib sequential treatment in patients with EGFR mutation-positive non-small cell lung cancer in South Korea (TOAST): Korean Cancer Study Group (KCSG) LU-19-22. Transl Lung Cancer Res. 2022;11(7):1369–79.
Shu Y, Ding Y, He X, Liu Y, Wu P, Zhang Q. Cost-effectiveness of osimertinib versus standard EGFR-TKI as first-line treatment for EGFR-mutated advanced non-small-cell lung cancer in China. Front Pharmacol. 2022;13: 920479.
Acknowledgments
The authors are grateful to Geum Sook Jeong for administrative assistance in preparing and submitting the manuscript.
This study was presented in part at the 2023 American Society of Clinical Oncology annual meeting (online publication), and 15th Annual Meeting of the Korean Society of Medical Oncology and 2022 International Conference (KSMO 2022, poster).
Funding
This work was supported in part by Samyang Biopharmaceuticals Corporation, Korea to J.-H.C., and by National Research Foundation of Korea and by the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health & Welfare, Republic of Korea to Y.W.C. (NRF-2021R1C1C1012266, HR22C1734).
Author information
Authors and Affiliations
Contributions
T.-H.K., J.-H.C. and Y.W.C. designed and planned the study. T.-H.K., J.-H.C., M.S.A., H.W.L., S.Y.K., and Y.W.C. collected and analyzed clinical data, and Y.W.K. analyzed and confirmed pathologic data. T.-H.K. and J.-H.C. wrote the main manuscript and J.-H.C. and Y.W.C. edited the manuscript. T.-H.K., J.-H.C., and Y.W.C. performed statistical analysis and S.-S.S. reviewed the statistical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research protocol was approved by the Institutional Review Board (IRB) of Ajou University Hospital, Suwon, Republic of Korea (AJOUIRB-MDB-2019-394) and all methods were performed in accordance with the relevant guidelines and regulations. The study was designed retrospectively. Written informed consent from patients was not required in accordance with guidelines of the IRB of Ajou University hospital.
Consent for publication
Not applicable.
Competing interests
J.-H.C. received research grants from AstraZeneca, Roche, and Yuhan Corporation, Korea.
T.-H.K., M.S.A., H.W.L., S.Y.K., Y.W.C., Y.W.K., and S.-S.S. declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kim, TH., Choi, JH., Ahn, M.S. et al. Differential efficacy of tyrosine kinase inhibitors according to the types of EGFR mutations and agents in non-small cell lung cancer: a real-world study. BMC Cancer 24, 70 (2024). https://doi.org/10.1186/s12885-023-11782-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11782-6