
Abstract
Background
Neuroblastoma, a neuroendocrine tumor originating from the sympathetic ganglia, is one of the most common malignancies in childhood. RTEL1 is critical in many fundamental cellular processes, such as DNA replication, DNA damage repair, genomic integrity, and telomere stability. Single nucleotide polymorphisms (SNPs) in the RTEL1 gene have been reported to confer susceptibility to multiple cancers, but their contributing roles in neuroblastoma remain unclear.
Methods
We conducted a study on 402 neuroblastoma cases and 473 controls to assess the association between four RTEL1 SNPs (rs3761124 T>C, rs3848672 T>C, rs3208008 A>C and rs2297441 G>A) and neuroblastoma susceptibility.
Results
Our results show that rs3848672 T>C is significantly associated with an increased risk of neuroblastoma [CC vs. TT/TC: adjusted odds ratio (OR)=1.39, 95% confidence interval (CI)=1.02-1.90, P=0.038]. The stratified analysis further indicated that boy carriers of the rs3848672 CC genotype had a higher risk of neuroblastoma, and all carriers had an increased risk of developing neuroblastoma of mediastinum origin. Moreover, the rs2297441 AA genotype increased neuroblastoma risk in girls and predisposed children to neuroblastoma arising from retroperitoneal.
Conclusion
Our study indicated that the rs3848672 CC and rs2297441 AA genotypes of the RTEL1 gene are significantly associated with an increased risk of neuroblastoma in Chinese children in a gender- and site-specific manner.
Similar content being viewed by others

Introduction
Neuroblastoma (NB) evolves from primitive neural crest cells, mostly stemming from the sympathetic nervous system chain and adrenal medulla [1]. NB occurs in ~150-200 children annually in Japan, and the incidence rate is 7.7 per million in China [2]. NB is not only highly heterogeneous but also has a variety of clinical symptoms [3, 4]. The International Neuroblastoma Risk Group (INRG) classifies NB into three risk groups (low-risk, intermediate-risk, or high-risk) based on age (month), tumor grade, histological category, 11q distortion, differentiation, MYCN and ploidy [5, 6]. Currently, the overall survival of NB is about 81% due to the great improvements in patient stratification and treatment regimens [7]. The five-year survival rates of low- and intermediate-risk neuroblastoma patients are as high as 80-90%, depending on the geographic area. Thanks to the emergence of stem cell transplantation, anti-GD2 based immunotherapy, and the differentiating agent isotretinoin, even in the high-risk group, the five-year survival rate of high-risk patients is enhanced by up to 50% [8, 9]. However, it is noteworthy that the majority of patients develop resistance to treatment, eventually experiencing recurrence, and NB survivors are often at risk of developing secondary neoplasms [10,11,12,13]. Therefore, there is an urgent need to understand the biological characteristics and pathogenesis of NB better and develop more efficacious therapies.
In recent decades, it has been reported that children exposed to some environmental factors are prone to the development of neuroblastoma, such as the mother's medication, living conditions, children's infection, pregnancy, and pregnancy exposure; however, the causal relationship between the two has not been confirmed [14, 15]. The etiology of neuroblastoma is still largely unknown. Many types of disease-causing genetic alterations are identified through whole genome sequencing and genome-wide association studies (GWASs), including single nucleotide polymorphisms (SNPs), mutations, deletions, amplification, and rearrangements [16, 17]. MYCN [18], ALK [14], and PHOX2B [19] gene mutations have been shown to increase the risk of neuroblastoma. Meanwhile, SNPs in a number of genes are associated with susceptibility to sporadic neuroblastoma, including TP53 [20], CASC15 [21, 22], LIN28B [23], TERT [24], ATRX [25], LMO1 [26], NBPF [27], BARD1 [28] genes and mitochondrial ND4 gene [29]. Although an increasing number of genetic variants have been identified, the more unknown causal genetic variants still needs to be explored for neuroblastoma.
Regulation of telomere elongation helicase 1 (RTEL1), containing Fe-S clusters, is an essential DNA helicase with 5’-3’ helicase activity. It could disassemble various DNA protein secondary structures to promote DNA repair, telomere maintenance and set telomere length in mice [30]. Rtel (-/-) mouse embryonic stem cells exhibit significant telomere deletion and chromosome breakage or fusion during differentiation [31]. Recently, GWAS showed that RTEL1 gene variations seem to be closely related to various diseases, such as glioma [32], lung cancer [33], astrocytomatal cancer [34], coronary heart [35], interstitial pneumonia [36], and ulcerative colitis [37]. However, no publication has reported a linkage between RTEL1 gene polymorphisms and the risk of neuroblastoma. To determine the association between neuroblastoma susceptibility and RTEL1 gene SNPs, we conducted this case-control study in Chinese children.
Materials and methods
Study subject
In the present study, we applied structured questionnaires to collect epidemiological data. A total of 402 children with neuroblastoma and 473 healthy controls without cancer history were collected from the Children’s Hospital of Nanjing Medical University during the same period (Table S1) [38, 39]. Children with neuroblastoma who meet the eligibility criteria need to be diagnosed with the confirmation by pathological biopsy. Cases and healthy children were matched by age, gender, and ethnicity. All participants’ parents or guardians signed an informed consent form. The research scheme was approved by the Institutional Review Committee of Children’s Hospital of Nanjing Medical University. The authors are responsible for all aspects of this study.
Polymorphism selection and genotyping
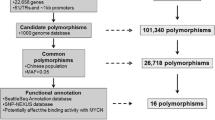
We identified four potential functions of SNPs (rs3761124 T>C, rs3848672 T>C, rs3208008 A>C, rs2297441 G>A) in the RTEL1 gene by combining the NCBI dbSNP database and SNPinfo software [40,41,42]. All selected SNPs were located in exons, introns, splice sites, 5’ untranslated regions (UTRs), or 3’ UTRs of the RTEL1 gene. They are in low linkage disequilibrium (LD) with each other (R2<0.8). LD is referred to as the non-random association of alleles at nearby loci. Variants in high LD (R2≥0.8) are highly correlated and can be a proxy of each other being associated with the same phenotypes, such as cancer susceptibility [43]. We chose SNPs in low LD to ensure the identification of maximal disease susceptibility loci with a limited number of SNPs. The minor allele frequencies of these SNPs in Chinese Han subjects are >5%. The rs3761124 T>C is located upstream of the RTEL1 gene, the rs3208008 A>C and rs3848672 T>C in exons, and the rs2297441 G>A is in the 3’ UTR of the RTEL1 gene. These polymorphisms may affect RTEL1 gene expression. Genomic DNA was isolated from the peripheral blood of participants using a TIANamp Blood DNA kit. Then, we genotyped the purified DNA samples of the neuroblastoma group and control group using standard TaqMan real-time PCR. Finally, to ensure reliability, accuracy, and repeatability, we randomly chose 10% of the completed research samples for repeated experiments. The repetition rate of all samples was 100%.
Statistical analysis
The chi-squared test of goodness of fit was used to determine the Hardy-Weinberg equilibrium (HWE) among the control groups. Bilateral χ2 tests were used to assess the differences in the distribution of genotype frequency and other characteristics between the patient and control groups. We applied multiple logistic regression to determine the association between the risk of neuroblastoma and the RTEL1 gene polymorphisms, with 95% confidence intervals (CIs) and odds ratios (ORs) adjusted by age and sex. The SNP genotype that increases the risk of neuroblastoma (OR>1) was defined as a risk genotype. In addition, we divided the patients into different subgroups based on age, sex, tumor origin, and clinical staging for further stratified analysis. We set 0.05 as the threshold of statistically significant difference for all tests, and all analyses were two-sided. All statistical analyses were calculated using SAS software version 9.4.
Results
RTEL1 gene polymorphisms and neuroblastoma susceptibility
The association between the genotype frequencies of the four RTEL1 gene polymorphisms (rs3761124 T>C, rs3848672 T>C, rs3208008 A>C, and rs2297441 G>A) and the susceptibility to neuroblastoma are shown in Table 1. We verified that the distribution of all four gene polymorphisms conformed to HWE (P>0.05) in controls. After adjusting for age and gender, we observed that rs3848672 T>C was significantly associated with an increased risk of neuroblastoma in the single-locus analysis (CC vs. TT/TC: adjusted OR=1.39, 95% CI=1.02-1.89, P=0.038). However, no significant associations were found for the rs3761124 T>C, rs3208008 A>C, and rs2297441 G>A polymorphisms.
Stratification analysis
First, we divided the study population into different subgroups by age, sex, tumor origin, and clinical stage. Second, we studied the effect of individual rs3761124 T>C, rs3848672 T>C, rs2297441 G>A polymorphisms and combined risk genotypes on the neuroblastoma susceptibility in different subgroups. As shown in Table 2, we detected that compared to the reference genotype, the rs3848672 CC genotype had enhanced effects on neuroblastoma risk in the following subgroups: male (adjusted OR=1.54, 95% CI=1.003-2.36, P=0.049) and tumors originating in the mediastinum (adjusted OR=1.94, 95% CI=1.25-3.01, P=0.003). Similarly, we found that the rs2297441 AA genotype had a more substantial risk effect in girls (adjusted OR=1.93, 95% CI=1.01-3.67, P=0.046) and increased children’s propensity to develop neuroblastoma originating from the retroperitoneal (adjusted OR=1.76, 95% CI=1.05-2.96, P=0.033).
Discussion
This research investigated the association between four RTEL1 gene SNPs and neuroblastoma risk by conducting a case–control study with 402 neuroblastoma patients and 473 healthy controls. Here, we found that rs3848672 T>C could increase the risk of neuroblastoma, especially among boys and subjects with mediastinum-origin tumors. Meanwhile, the rs2297441 G>A polymorphism conferred increased risk in girls and subjects with neuroblastoma of retroperitoneal origin. To the best of our knowledge, the association between RTEL1 gene polymorphisms and the risk of neuroblastoma in Chinese children has not been reported before.
The telomere structure comprises TTAGGG repeat sequences and their related factors or protective proteins, which are necessary for maintaining genomic stability and human linear chromosome integration [44]. In normal human somatic cells, telomeres are shortened due to cell replication or aging. In contrast, cancer cells proliferate infinitely without losing telomeres. RTEL1 plays an essential role in the process of DNA unwinding. Its encoding gene is located at 20q13.3 and contains 40 exons. RTEL1 can decompose different kinds of DNA secondary structures and promote DNA repair, replication, and recombination, thus helping to maintain the integrity of telomeres [45]. It has been reported that inactivation of the RTEL1 gene leads to chromosome breakage, fusion, and telomere loss in mice [46]. The human RTEL1 gene is a direct homolog of the mouse RTEL1 gene, and its protein products may have similar effects. When the RTEL1 gene is deleted in cells, sister chromatid exchange and gene replacement are more likely to occur [47]. RTEL1 gene-deficient stem cells are prone to local chromosome breaking, and their cell differentiation and proliferation abilities are significantly decreased [48]. In addition, RTEL1 gene-deficient cells are more sensitive to DNA damage during embryonic development. Therefore, any RTEL1 SNPs affecting telomere length after birth may be able to exacerbate or delay genetic susceptibility to relevant diseases.
Several GWAS and candidate gene studies have identified that RTEL1 variants are associated with cancer genetic susceptibility, including lung cancer, breast cancer, gastric cancer, colorectal cancer, and esophageal cancer [49]. A meta-analysis showed a correlation between the G allele of RTEL1 rs6010620 and an increased risk of glioma, including 1878 cases and 3670 controls [50]. In addition, a mouse model study showed that the RTEL1 gene could regulate the Wnt/β-Catenin signaling to support cell growth, suggesting that the RTEL1 may be considered a carcinogenic gene [48]. The above results collectively indicate that the RTEL1 gene is a cancer-promoting factor and may also be an anti-cancer target. Among the four investigated SNPs (rs3761124 T>C, rs3848672 T>C, rs3208008 A>C, and rs2297441 G>A) in the present study, Egan et al. reported that the rs3208008 was associated with an increased risk of glioma in a US study population [51]. The other three SNPs have not been reported to be related to disease. In this study, we concluded that rs3848672 T>C and rs2297441 G>A significantly increased the risk of neuroblastoma in Chinese children.
Consistent with the vital role of RTEL1 in malignancies, we report for the first time the association between RTEL1 polymorphisms and the risk of neuroblastoma. It is assumed that the RTEL1 polymorphism may change the binding affinity of transcription factors, leading to telomere elongation dysfunction, thus affecting the survival of glioma cells [52]. Therefore, there may be the same pathogenesis of neuroblastoma. Our results showed that rs3848672 T>C and rs2297441 G>A polymorphisms could contribute to an increased neuroblastoma risk. However, the other two SNPs, rs3761124 T>C, and rs3208008 A>C, were not associated with the risk of neuroblastoma. Several limitations should be mentioned in this study. First, the sample size of this study may not be large enough to generate a reliable association between genetic variants and disease risk. A larger sample size could improve the statistical power and the credibility of the conclusions. Second, we evaluated only four SNPs in this research. Many other potential functional RTEL1 polymorphisms should be investigated in the future. Third, the subjects involved in this study were all from the Chinese population, so the conclusions drawn in this study may not apply to other ethnic people. Fourth, this study only evaluated the effects of genetic alterations on the risk of neuroblastoma without considering the impact of environmental factors.
Conclusion
In conclusion, we provide the first evidence that polymorphisms rs3848672 T>C and rs2297441 G>A in the RTEL1 gene are associated with the risk of neuroblastoma in the Chinese population. In the future, studies should be conducted with large sample sizes, considering environmental factors, genetic-environmental interactions, and different races.
Availability of data and materials
All the data are available upon request from the correspondence authors (Jing He or Haiyan Wu).
Abbreviations
- NB:
-
neuroblastoma
- INRG:
-
International Neuroblastoma Risk Group
- GWAS:
-
genome-wide association study
- SNP:
-
single nucleotide polymorphism;
- RTEL1:
-
regulation of telomere elongation helicase 1
- UTR:
-
untranslated region
- LD:
-
linkage disequilibrium
- HWE:
-
Hardy-Weinberg equilibrium
- OR:
-
odds ratio
- CI:
-
confidence interval
Reference
Ivanova E, Sharma SD, Brichkina A, Pfefferle P, Keber U, Pagenstecher A, et al. DYRK3 contributes to differentiation and hypoxic control in neuroblastoma. Biochem Biophys Res Commun. 2021;567:215–21.
Bao PP, Li K, Wu CX, Huang ZZ, Wang CF, Xiang YM, et al. Recent incidences and trends of childhood malignant solid tumors in Shanghai, 2002-2010. Zhonghua Er Ke Za Zhi. 2013;51:288–94.
Meany HJ. Non-High-Risk Neuroblastoma: Classification and Achievements in Therapy. Children (Basel). 2019;6:5.
Morgenstern DA, Bagatell R, Cohn SL, Hogarty MD, Maris JM, Moreno L, et al. The challenge of defining “ultra-high-risk” neuroblastoma. Pediatr Blood Cancer. 2019;66:e27556.
Nakagawara A, Li Y, Izumi H, Muramori K, Inada H, Nishi M. Neuroblastoma. Jpn J Clin Oncol. 2018;48:214–41.
Cohn SL, Pearson AD, London WB, Monclair T, Ambros PF, Brodeur GM, et al. The International Neuroblastoma Risk Group (INRG) classification system: an INRG Task Force report. J Clin Oncol. 2009;27:289–97.
Han JZR, Hastings JF, Phimmachanh M, Fey D, Kolch W, Croucher DR. Personalized Medicine for Neuroblastoma: Moving from Static Genotypes to Dynamic Simulations of Drug Response. J Pers Med. 2021;11:395.
Matthay KK, Maris JM, Schleiermacher G, Nakagawara A, Mackall CL, Diller L, et al. Neuroblastoma. Nat Rev Dis Primers. 2016;2:16078.
Qiu B, Matthay KK. Advancing therapy for neuroblastoma. Nat Rev Clin Oncol. 2022;19:515–33.
Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999–2007: results of EUROCARE-5–a population-based study. Lancet Oncol. 2014;15:35–47.
Ward E, DeSantis C, Robbins A, Kohler B, Jemal A. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin. 2014;64:83–103.
Zheng R, Peng X, Zeng H, Zhang S, Chen T, Wang H, et al. Incidence, mortality and survival of childhood cancer in China during 2000–2010 period: A population-based study. Cancer Lett. 2015;363:176–80.
Westerveld ASR, van Dalen EC, Asogwa OA, Koopman MMW, Papadakis V, Laureys G, et al. Neuroblastoma survivors at risk for developing subsequent neoplasms: A systematic review. Cancer Treat Rev. 2022;104:102355.
Mosse YP, Laudenslager M, Longo L, Cole KA, Wood A, Attiyeh EF, et al. Identification of ALK as a major familial neuroblastoma predisposition gene. Nature. 2008;455:930–5.
Cook MN, Olshan AF, Guess HA, Savitz DA, Poole C, Blatt J, et al. Maternal medication use and neuroblastoma in offspring. Am J Epidemiol. 2004;159:721–31.
Consortium IHGS. Finishing the euchromatic sequence of the human genome. Science. 1984;224:1121–4.
Aygun N. Biological and Genetic Features of Neuroblastoma and Their Clinical Importance. Curr Pediatr Rev. 2018;14:73–90.
Brodeur GM, Seeger RC, Schwab M, et al. Amplification of N-myc in untreated human neuroblastomas correlates with advanced disease stage. Science. 1984;224:1121–4.
van Limpt V, Schramm A, van Lakeman A, Sluis P, Chan A, van Noesel M, et al. The Phox2B homeobox gene is mutated in sporadic neuroblastomas. Oncogene. 2004;23:9280–8.
Diskin SJ, Capasso M, Diamond M, Oldridge DA, Conkrite K, Bosse KR, et al. Rare variants in TP53 and susceptibility to neuroblastoma. J Natl Cancer Inst. 2014;106:dju047.
Russell MR, Penikis A, Oldridge DA, Alvarez-Dominguez JR, McDaniel L, Diamond M, et al. CASC15-S Is a Tumor Suppressor lncRNA at the 6p22 Neuroblastoma Susceptibility Locus. Cancer Res. 2015;75:3155–66.
He J, Zou Y, Wang T, Zhang R, Yang T, Zhu J, et al. Genetic Variations of GWAS-Identified Genes and Neuroblastoma Susceptibility: a Replication Study in Southern Chinese Children. Transl Oncol. 2017;10:936–41.
Molenaar JJ, Domingo-Fernandez R, Ebus ME, Lindner S, Koster J, Drabek K, et al. LIN28B induces neuroblastoma and enhances MYCN levels via let-7 suppression. Nat Genet. 2012;44:1199–206.
Peifer M, Hertwig F, Roels F, Dreidax D, Gartlgruber M, Menon R, et al. Telomerase activation by genomic rearrangements in high-risk neuroblastoma. Nature. 2015;526:700–4.
Cheung NK, Zhang J, Lu C, Parker M, Bahrami A, Tickoo SK, et al. Association of age at diagnosis and genetic mutations in patients with neuroblastoma. JAMA. 2012;307:1062–71.
Wang K, Diskin SJ, Zhang H, Attiyeh EF, Winter C, Hou C, et al. Integrative genomics identifies LMO1 as a neuroblastoma oncogene. Nature. 2011;469:216–20.
Diskin SJ, Hou C, Glessner JT, Attiyeh EF, Laudenslager M, Bosse K, et al. Copy number variation at 1q21.1 associated with neuroblastoma. Nature. 2009;459:987–91.
Capasso M, Devoto M, Hou C, Asgharzadeh S, Glessner JT, Attiyeh EF, et al. Common variations in BARD1 influence susceptibility to high-risk neuroblastoma. Nat Genet. 2009;41:718–23.
Chang X, Liu Y, Glessner J, Hou C, Qu H, Nguyen K, et al. Identification of Mitochondrial DNA Variants Associated With Risk of Neuroblastoma. J Natl Cancer Inst. 2022;114:910–3.
Barber LJ, Youds JL, Ward JD, McIlwraith MJ, O’Neil NJ, Petalcorin MIR, et al. RTEL1 Maintains Genomic Stability by Suppressing Homologous Recombination. Cell. 2008;135:261–71.
Ding H, Schertzer M, Wu X, Gertsenstein M, Selig S, Kammori M, et al. Regulation of murine telomere length by Rtel: an essential gene encoding a helicase-like protein. Cell. 2004;117:873–86.
Namgoong S, Cheong HS, Kim JH, Kim LH, Seo JY, Kang SG, et al. Association analysis of RTEL1 variants with risk of adult gliomas in a Korean population. PLoS One. 2018;13:e0207660.
Yan S, Xia R, Jin T, Ren H, Yang H, Li J, et al. RTEL1 polymorphisms are associated with lung cancer risk in the Chinese Han population. Oncotarget. 2016;7:70475–80.
Jin T, Wang Y, Li G, Du S, Yang H, Geng T, et al. Analysis of difference of association between polymorphisms in the XRCC5, RPA3 and RTEL1 genes and glioma, astrocytoma and glioblastoma. Am J Cancer Res. 2015;5:2294–300.
Lu S, Zhong J, Wu M, Huang K, Zhou Y, Zhong Z, et al. Genetic analysis of the relation of telomere length-related gene (RTEL1) and coronary heart disease risk. Mol Genet Genomic Med. 2019;7:e550.
Yuan ZZ, Fan LL, Wang CY, Luo H, Liu L. Novel heterozygous mutation of RTEL1 in interstitial pneumonia with autoimmune feature. QJM. 2022;115:253–5.
Ziv A, Werner L, Konnikova L, Awad A, Jeske T, Hastreiter M, et al. An RTEL1 Mutation Links to Infantile-Onset Ulcerative Colitis and Severe Immunodeficiency. J Clin Immunol. 2020;40:1010–9.
Lin L, Deng C, Zhou C, Zhang X, Zhu J, Liu J, et al. NSUN2 gene rs13181449 C>T polymorphism reduces neuroblastoma risk. Gene. 2023;854:147120.
Chang J, Lin L, Zhou C, Zhang X, Yang T, Wu H, et al. Functional polymorphisms of the TET1 gene increase the risk of neuroblastoma in Chinese children. J Cell Mol Med. 2023;27:2239–48.
He J, Yuan L, Lin H, Lin A, Chen H, Luo A, et al. Genetic variants in m(6)A modification core genes are associated with glioma risk in Chinese children. Mol Ther Oncolytics. 2021;20:199–208.
Chen YP, Liao YX, Zhuo ZJ, Yuan L, Lin HR, Miao L, et al. Association between genetic polymorphisms of base excision repair pathway and glioma susceptibility in Chinese children. World J Pediatr. 2022;18:632–5.
Guan Q, Lin H, Hua W, Lin L, Liu J, Deng L, et al. Variant rs8400 enhances ALKBH5 expression through disrupting miR-186 binding and promotes neuroblastoma progression. Chin J Cancer Res. 2023;35:140–62.
Machiela MJ, Chanock SJ. LDlink: a web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics. 2015;31:3555–7.
Telomeres SG. Telomerase and Ageing. Subcell Biochem. 2018;90:221–308.
Vannier JB, Sarek G, Boulton SJ. RTEL1: functions of a disease-associated helicase. Trends Cell Biol. 2014;24:416–25.
Youds J L, Mets D G, McIlwraith M J, Martin J S, Ward J D, Oneil N J, et al. RTEL-1 Enforces Meiotic Crossover Interference and Homeostasis. Science. 2010;327:1254–8.
Wang RC, Smogorzewska A, de Lange T. Homologous recombination generates T-loop-sized deletions at human telomeres. Cell. 2004;119:355–68.
Wu X, Sandhu S, Nabi Z, Ding H. Generation of a mouse model for studying the role of upregulated RTEL1 activity in tumorigenesis. Transgenic Res. 2012;21:1109–15.
Muleris M, Almeida A, Gerbault-Seureau M, Malfoy B, Dutrillaux B. Identification of amplified DNA sequences in breast cancer and their organization within homogeneously staining regions. Genes Chromosomes Cancer. 1995;14:155–63.
Shete S, Hosking FJ, Robertson LB, Dobbins SE, Sanson M, Malmer B, et al. Genome-wide association study identifies five susceptibility loci for glioma. Nat Genet. 2009;41:899–904.
Egan KM, Thompson RC, Nabors LB, Olson JJ, Brat DJ, Larocca RV, et al. Cancer susceptibility variants and the risk of adult glioma in a US case-control study. J Neurooncol. 2011;104:535–42.
Viana-Pereira M, Moreno DA, Linhares P, Amorim J, Nabico R, Costa S, et al. Replication of GWAS identifies RTEL1, CDKN2A/B, and PHLDB1 SNPs as risk factors in Portuguese gliomas patients. Mol Biol Rep. 2020;47:877–86.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from Taizhou Science and Technology Project (No: 20ywb135, No: 21ywb123), Wenling Science and Technology Project (No: 2021S00148, No: 2020S0180128, No: 2021S00158), and The Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (No: 2021KY1228).
Author information
Authors and Affiliations
Contributions
T.Z., J.G., and J.C. analyzed the data and prepared all the tables; T.Z. and C.Z. wrote the paper. C.Z. and H.W. performed the study and collected the samples and clinical data; J.H. conceptualized and designed the research study and performed data management, review and editing.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The research has obtained approval from the institutional review board of the Children’s Hospital of Nanjing Medical University (Approval No: 202112141-1). According to the Declaration of Helsinki, written informed consent was obtained from each participant. All participants’ parents or guardians signed an informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Demographic characteristics of neuroblastoma patients and cancer-free controls from Jiangsu province.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, T., Zhou, C., Guo, J. et al. RTEL1 gene polymorphisms and neuroblastoma risk in Chinese children. BMC Cancer 23, 1145 (2023). https://doi.org/10.1186/s12885-023-11642-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11642-3