
Abstract
Background
The optimal treatment for multiple brain metastases has been recently controversially discussed.This study was aimed to explore the feasibility of Hippocampus-Avoidance Whole-Brain Radiotherapy plus a simultaneous integrated boost (HA-WBRT + SIB) in patients with multiple brain metastases and assess tumor control in comparison with Hippocampus-Avoidance Whole-Brain Radiotherapy (HA-WBRT) alone for brain metastases.
Methods
In this study, 63 patients with multiple brain metastases (≥ 4 metastases) had undergone HA-WBRT + SIB between January 2016 and December 2020 in the observation group:HA-WBRT (30 Gy in 12 fractions, the maximum dose of the hippocampus ≤ 14 Gy) plus a simultaneous integrated boost (48 Gy in 12 fractions) for brain metastases.Overall Survival (OS), Median survival,intracranial control (IC = control within the entire brain), intracranial progression-free survival (iPFS) and adverse events were compared with the control group (a HA-WBRT retrospective cohort) by propensity score matching analysis.
Results
After 1:1 propensity score matching,there were 56 patients in each group (the observation group, the control group). OS, median survival and iPFS were significantly longer in the observation group (18.4 vs. 10.9 months, P<0.001), (13.0 vs. 8.0 months, P<0.001), (13.9 vs.7.8 months, P<0.001). In comparison of 1-year-IC rates, the observation group also demonstrated higher than the control group (51.8% vs. 21.4%, P = 0.002), respectively. Seven hippocampal metastases were found in the control group (4/56,7.1%) and the observation group (3/56,5.4%) after HA-WBRT. The death rate of intracranial progression were 23.2% in the observation group and 37.5% in the control group.All adverse events were not significant difference between the two groups (P>0.05).
Conclusions
HA-WBRT + SIB resulted in better OS,median survival, IC, iPFS, an acceptable risk of radiation response, and a potential way of declining neurocognitive adverse events, which may be a better treatment for patients with multiple brain metastases.
Similar content being viewed by others

Background
Brain metastases (BMs) are the most common intracranial tumors in adults. Brain metastases occur in 24–45% of all patients who are systemic tumors every year [1]. Among them, Brain metastases is common in lung, melanoma, breast, and renal cancer. Patients with one to three brain metastases usually were treated with Stereotactic Radiosurgery (SRS) or Stereotactic Body Radiation Therapy (SBRT) resulting in better local control (LC) and similar overall survival (OS). Although WBRT is a common treatment for multiple brain metastases, the best treatment is still controversial. Two retrospective studies demonstrated that WBRT plus SRS could improve local control but could not improve survival [2, 3]. In addition,132 patients did not achieve better survival through WBRT + SRS in a prospective trial [1]. In another retrospective study, patients without extracranial metastasis showed no better survival treated with WBRT + SRS compared to SRS alone [4]. However, the contradictory findings from the randomized clinical trials were that patients with one to three brain metastases were treated with stereotactic radiosurgery (SRS) [5]. Several studies have showed WBRT plus Simultaneous Integrated Boost (SIB) can improve overall survival of patients with brain metastases [6,7,8].
Neurocognitive decline was related to WBRT which led to hippocampal atrophy and long-term brain atrophy and leukoencephalopathy [9,10,11]. In addition, several studies showed that significant neurocognitive deterioration have also been related to poor IC and progressive brain metastases [12,13,14], and this demonstrated that IC is vital important to protect neurocognitive functions.
WBRT is associated with relatively low local tumor control (LTC),but better distant intracranial tumor control (DTC). On the contrary, SRS/SBRT displays higher LTC but relatively low DTC [15, 16]. Therefore, WBRT combined with SRS/SBRT can improve LTC of brain metastases [8]. Moreover, a phase 2 and a randomized phase 3 NRG Oncology CC001 trials demonstrated HA-WBRT preserved memory function [16, 17].
HA-WBRT plus SRS/SBRT could increase intracranial LTC,protect cognitive function,and also reduce neurologic death rates.
Prokic et al. [18] disclosed that The best way to protect the hippocampus can be attained if the dose escalation to brain metastases is planned as SIB instead of as sequential SRS in a planning study exploring the combination of HA-WBRT and SRS. Therefore, The purpose of this study was to explore the feasibility of HA-WBRT + SIB in the treatment of multiple brain metastases and assess OS, Median survival, IC, iPFS and adverse events in compared with HA-WBRT alone for brain metastases.
Methods
Patients’ selection
In this study, 63 patients with multiple brain metastases had undergone HA-WBRT + SIB between January 2016 and December 2020 at the Department of Radiation Oncology of the Third Hospital of Zhangzhou and XiaMen ChangGung Hospital in the observation group: Patients received HA-WBRT (30 Gy in 12 fractions, the maximum dose of the hippocampus ≤ 14 Gy) and a SIB (48 Gy in 12 fractions). The control group (a HA-WBRT retrospective cohort): 189 patients being retrospectively selected had been treated with WBRT between January 2016 and December 2020. Among them, 98 patients had received HA-WBRT and 91 patients were treated with WBRT without Hippocampus-Avoidance, who were not fit for further analysis. There were 56 patients in each group (HA-WBRT + SIB, n = 56; HA-WBRT, n = 56) through 1:1 propensity score matching (Fig. 1). There was significant difference in the small cell lung cancer (SCLC)(HA-WBRT + SIB, n = 7; HA-WBRT, n = 42, χ2 = 210.00, P<0.0001) therefore,patients with SCLC were excluded. Primary focuses of all patients were confirmed by pathology and enhanced-brain-MRI-proven multiple brain metastases (range 4–15), without hippocampal metastasis or 7 mm away from hippocampus. Those patients with one to three brain metastases and maximum diameter of BM less than 5 mm were excluded. Those patients who had no clear records at diagnosis or incomplete treatment were also removed. Baseline characteristics of patients was listed Table 1. The average characteristics of the patients include age, gender, karnofsky performance status (KPS score), number and maximum size of brain metastasis, brain edema, symptoms of BM, primary tumor, type of radiotherapy, extracranial metastases and systemic treatment.

Eligible or ineligible for inclusion in the study. HA-WBRT + SIB indicates hippocampus-avoidance whole-brain radiation therapy plus a simultaneous integrated boost; HA-WBRT, hippocampus-avoidance whole-brain radiation therapy; WBRT,whole-brain radiation therapy
Treatment
All patients were diagnosed as multiple brain metastases by contrast-enhanced magnetic resonance imaging (MRI). Among them, 56 patients were treated with HA-WBRT + SIB and another 56 patients received HA-WBRT alone. 112 patients received radiotherapy-planning computed tomography (CT) with 1.5 mm slice thickness in thermoplastic mask, c-pillow and head frame immobilization as well as contrast-enhanced transversal T1-weighted magnetic resonance imaging (MRI). The scanned images were transmitted to Varian’s planning system (Varian Eclipse 8.0 and 15.0 version), and then the CT images were fused with the transversal T1-weighted MRI images and served for the target volume and organ-at-risk delineation.
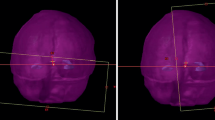
The whole brain excluding the hippocampus-avoidance region (HAR, a 7 mm 3-dimensional margin around the hippocampus) was defined as the clinical target volume (CTV), and an extension of 3 mm on CTV was defined as planning tumor volume (PCTV) in the observation group. PCTV was given 30 Gy in 12 fractions,per fraction one day,5 fractions per week, maximum dose of the hippocampus (Dmax) ≤ 14 Gy, mean dose (Dmean) ≤ 9 Gy. The gross tumor volume (GTVmetastases,i.e. GTVm) was contoured on the fused images (CT images and MRI images), GTVm with 2 mm extension formed PGTVm,with total dose of 48 Gy in 12 fractions, one fraction every day, 5 fractions one week in the observation group. The whole brain excluding HAR with 3 mm margin was defined as planning tumor volume of the brain (PTVwhole brain), with the same dose of PCTV of HA-WBRT + SIB in the control group. All plans were adopted volumetric intensity modulated arc therapy (VMAT) and the homogenous dose was prescribed to cover the 95% isodose (Fig. 2). SRT, SRS and SBRT have not been implemented in many places due to unbalanced development in various regions of China. Therefore, the dose escalation to PGTV was used to treat patients with multiple brain metastases (4–15) by linear accelerator (VARIAN CLINAC IX) in this study. Dose constraints of organs at risk are showed in Table 2.

Example of a dose distribution and dose-volume histogram of an HA-WBRT + SIB plan for one patient with 5 brain metastases. Colors indicate the following: green, hippocampi; light pink, PGTVm; orange, PCTV (whole brain + 3 mm); The maximum dose of hippocampus was 14.2 Gy, whereas the whole brain and the metastases received doses of 30 and 48 Gy, respectively. HA-WBRT + SIB, hippocampus-avoidance whole-brain radiation therapy with a simultaneous integrated boost; PGTVm, planning tumor volume of metastases; PCTV, planning tumor volume of the whole brain (clinical target volume)
On the basis of the situation of patients and clinical experience of physicians, 36 patients (HA-WBRT + SIB) and 34 patients (HA-WBRT) underwent more than 2 cycle of systemic therapy, 20 patients (HA-WBRT + SIB) and 22 patients (HA-WBRT) did not undergo systemic therapy.
Follow‑up and study endpoint
Follow-up was scheduled for examinations in the first month after radiotherapy, including contrast enhanced MRI, clinical examination, and adverse reaction evaluation on the basis of version 4.0 of the Common Terminology Criteria for Adverse Events (CTCAE), and repeated at 3 months interval for the first 2 years, then repeated at 6 months interval in years 3 to 5, and once a year thereafter. The last follow-up was November 2021. Overall survival (OS) ranged from the first day of brain radiotherapy to death or the day on which the patient was last known to be alive in the case of loss to follow-up. Median survival means that only 50% of the individuals can live through this time.Intracerebral control (IC) included complete response (CR), partial response (PR), or stable disease (SD) of brain metastases after radiotherapy. Furthermore, pseudoprogression and radionecrosis related to radiotherapy were excluded from local failures of IC. If the total maximum diameter of treated lesions increased by 20%, or increase the absolute value ≥ 5 mm, or new lesions appeared in the brain, which were considered progressive disease (PD). Intracranial progression-free survival (iPFS) was counted from the time to start radiotherapy until brain metastases progression or death for any reason or the day on which the patient was last known to be alive in the case of loss to follow-up.
Evaluation of treatment-related toxicity included alopecia, radiation dermatitis, encephaledema, headache, emesis, sicchasia, vertigo, fatigue, focal neurologic deficits, epilepsia, neurocognitive dysfunction, and radionecrosis.
Statistical analysis
Statistical analysis was adopted SPSS 20.0 (IBM Corporation, Chicago, IL, USA) statistical software. To manage the unbalance of potential interference factors, propensity score matching (PSM) was adopted to set up two treatment groups with an even distribution of original characteristics.The propensity score matching analysis was used between HA-WBRT + SIB (the observation group) and HA-WBRT (the control group) to control confounding factors of patients, and performed with a logistic regression that considered the following factors: age, gender, intracranial symptoms, karnofsky performance status, primary tumor, extracranial metastases, maximum size and number of brain metastases. OS, median survival and iPFS were calculated by Kaplan–Meier method. 1-year-IC rates and adverse events were calculated by χ2 test (fisher’s exact test). The baseline characteristics of the patients were counted by χ2 test after matching P<0.05 (two-tailed) of all analysis results were considered statistically significant.
Results
Patient characteristics
63 patients treated with HA-WBRT + SIB and 189 patients treated with HA-WBRT were confirmed. All patients were matched through 1:1 propensity score matching analysis, there were 56 patients in each group and were well balanced between them (Table 1). A total of 112 eligible patients with multiple brain metastases were enrolled in the analysis (Fig. 1). Among of them (median age, 58 years old), men were 65 (58%) and women were 47 (42%). Most patients of the two groups were non-small cell lung cancer (NSCLC,71% vs. 29%). The last follow-up date was November 30, 2021, the median follow-up time of the observation group and control group was 11.2 months and 9.8 months, respectively.
Outcome of overall survival and intracranial progression-free survival
At the end of this study, there were 102 patients of death (48 patients in the observation group, 54 patients in the control group) and 10 survival patients. Among of them, 13 patients of the observation group died in intracranial tumor progression and 30 patients died in extrabrain progression or other reasons (infection, massive hemorrhage, respiratory failure and circulatory failure) and 5 patients died of unknown causes. In the control group, the reason of 21 patients’ death was brain metastases progression, 23 patients died of extracranial progress or other reasons (infection, massive hemorrhage, respiratory failure and circulatory failure), 10 patients of death were unknown. OS improved in the observation group (18.4 vs. 10.9 months, P<0.0001; Fig. 3), with a median survival 13 months of the observation group and a median survival 8 months of the control group. Overall iPFS was also longer in the observation group (13.9 vs. 7.8 months, P<0.0001; Fig. 4).

The OS was significantly longer in HA-WBRT + SIB (18.4 vs. 10.9 months, P<0.0001). HA-WBRT + SIB,hippocampus-avoidance whole-brain radiation therapy with a simultaneous integrated boost; OS, overall survival; HA-WBRT, hippocampus-avoidance whole-brain radiation therapy

Obviously better iPFS with HA-WBRT + SIB versus HA-WBRT (13.9vs7.8 months, P<0.0001). HA-WBRT + SIB, hippocampus-avoidance whole-brain radiation therapy plus a simultaneous integrated boost; iPFS, intracranial progression-free survival; HA-WBRT, hippocampus-avoidance whole-brain radiation therapy
Intracerebral control
The 1-year IC rate was higher in the observation group (51.8% vs. 21.4%, P = 0.002). One month after radiotherapy, there were 442 brain metastases in the observation group, including 127 lesions (28.7%) of complete remission, 172 lesions (38.9%) of partial remission, 61 lesions (13.8%) of stable, and 82 lesions (18.6%) of progress.
There were 429 lesions in the control group, including 56 lesions (13.1%) of complete remission, 125 lesions (29.1%) of partial remission, 64 lesions (14.9%) of stable, and 184 lesions (42.9%) of progress.
Toxicity of two groups
At the end of follow-up, all adverse events of two groups were assessed according to National Cancer Institute’s CTCAE, version 4.0. Neurocognitive decline 12 months after radiotherapy 3 patients were observed in observation group (3/56,5.4%) and 2 patients were found in the control group (2/56,3.6%), adverse reactions more than grade 2 were 2 patients in the observation group (2/56,3.6%). No significant difference was found in the neurocognitive decline of the two groups (P = 0.843), Neurocognitive decline were evaluated according to Mini-mental State Examination (MMSE), including speech ability, orientation, calculation, memory, attention.The total score of MMSE is 30 points, and the evaluation time is about 5-10 min. According to the educational level of patients, the standard of cognitive impairment is divided into general illiteracy ≤ 17 points, primary school education ≤ 20 points, secondary school education ≤ 24 points. Below the standard score, cognitive impairment was considered to exist, which needed to be examined; Severity classification of cognitive impairment: mild MMSE ≥ 21 points; Moderate MMSE 10–20 points; Severe MMSE ≤ 9 points (Table 1 in the supplement). All of them underwent grade 1–2 alopecia (Table 3). The difference between pseudoprogression and radionecrosis related to radiotherapy is detailed in Table 4. Seven hippocampal metastases were found in the two groups (the control group: 4/56,7.1%) and the observation group:3/56,5.4%) after hippocampus-avoidance. The death rate of intracranial progression were 23.2% in HA-WBRT + SIB group and 37.5% in HA-WBRT alone group.
Discussion
WBRT was considered as the conventional treatment for multiple brain metastases for many years. Although,WBRT + SRS has been recognized the superior choose for the oligometastases in brain,no better OS has been demonstrated in recent years [19,20,21]. Nevertheless, the best treatment for multiple brain metastases was still controversial. This retrospective research was aimed at assessing the clinical effect and feasibility of HA-WBRT + SIB for multiple brain metastases,and comparing with OS,IC,iPFS for patients treated with HA-WBRT. Altogether HA-WBRT + SIB could improve OS, median survival,IC and iPFS in matched queue (n = 112), and higher IC was also associated with longer iPFS. Some studies showed that WBRT with radiation boost was more superior therapy for multiple brain metastases than WBRT alone. Two retrospective researches of Shanghavi et al. [22] and Wang et al. [23] demonstrated that WBRT plus SRS group for multiple brain metastases was better survival than WBRT alone. Shanghavi et al. displayed that the median survival were 16.1, 10.3, and 8.7 months for RPA categories I, II, and III, respectively, showing better survival in WBRT plus SRS group. The other study also showed that survival benefit was found in those patients with low KPS < 70. Wegner et al. suggested that the better survival was found in the cases with SCLC those who underwent WBRT plus SRS than did SRS alone (14 vs. 6 months, p = 0.040) [24]. Andrews et al. [8] demonstrated that WBRT plus SRS group had improved general condition and survival compare to the WBRT alone group for patients with one brain metastasis (6.5 vs. 4.9 months; P = 0.0393), also showed that 1-year control rate was better in the WBRT plus SRS group (82% vs. 71%, P = 0.01). It’s worth noting that merely 24 (7.2%) SCLC cases were contained in the research. These views are similar to this study, but SIB and hippocampus-avoidance were adopted in our study, which could has the biological advantage of dose fractionation and better protect the neurocognitive function.
Some published papers showed that WBRT + SRS did not receive survival benefit in those patients with multiple brain metastases in contrast to SRS alone [25, 26]. So far, SRS has commonly been used to patients with one to three metastases [15, 27]. However, more and more radiotherapy physicians have used SRS for patients with multiple brain metastases instead of WBRT. Many academic researches have demonstrated that SRS has better survival advantage and less toxicity than WBRT In the past 30 years [28]. Jinyu Xue et al. had found that the mean dose of normal brain in SRS was related to the total target volume but not the number of brain metastases [29]. A prospective study (JLGK0901) showed that the survival of patients with 2–4 and 5–10 BMs who had undergone SRS alone were not significant difference, the median OS of these patients was 10.8 months [26, 30, 31].
This study was to compare the OS, iPFS and IC of HA-WBRT and HA-WBRT for patients with multiple brain metastases, to explore the clinical effect and practicability of HA-WBRT + SIB for patients with multiple brain metastases in the context of protecting neurological and neurocognitive function. There were three prospective clinical studies showed that intracranial tumor progression was associated with neurocognitive hypofunction, then decline the quality of life [12, 14, 32]. The 1-year IC rate was obviously higher in the HA-WBRT + SIB group,which increase iPFS. Several randomized researches compared the different dose-fractionation methods of WBRT with conventional dose-fractionation (30 Gy/10f,BED = 39 Gy,α/β = 10), which showed the higher BED for WBRT could not increase survival, but a lower BED could result in worse efficacy [16, 33, 34]. Nevertheless, a lower BED could decline the rate of neurocognitive dysfunction,particularly in case of prophylactic cranial irradiation [35].
Therefore, the lower BED of the whole brain (30 Gy/12f,BED = 37.5 Gy) in the HA-WBRT and HA-WBRT + SIB groups was to decline neurocognitive impairment as far as possible. HA-WBRT is a reliable radiotherapy concept, Because the higher rate of intracranial progression was not associated with the HA. In this study, four hippocampal metastases were found in HA-WBRT (4/56,7.1%), 3 patients were found single metastatic lesion in unilateral hippocampus, only one patient was found a lesion in bilateral hippocampus, respectively. Three hippocampal metastases were found in HA-WBRT + SIB (3/56,5.4%), 3 patients were found single metastatic lesion in unilateral hippocampus. The data analysed showed that all brain metastases been treated are far from the hippocampus, which led to the lower dose of hippocampus and may be related to hippocampal metastasis several researches showed the similar rates of new hippocampal metastases after HA-WBRT [36,37,38, 40].
In this study, the data in the HA-WBRT + SIB group demonstrated that the 4–15 brain metastases could improve 1-year rates, OS and iPFS, which were the same as the researches [39, 40]. Dose limit of hippocampus (Dmax ≤ 14 Gy) in the two groups were not found significant difference, we selected the maximum limit of hippocampus in the two groups owing to the dose of hippocampus being related to predict neurocognitive dysfunction [41, 42], which was slightly different from Phase III Trial NRG Oncology CC001 [17]. There are three limitations in our study, Firstly, There was no SRS control group in our study, therefore we could not compare with SRS group. Then, there were not univariate and multivariate analyses of overall survival.Finally, the material of retrospective study maybe bias the outcomes and did not take memantine during HA-WBRT.
Conclusions
In this study, HA-WBRT + SIB resulted in better OS, median survival, IC, iPFS, an acceptable toxicity, and a potential way of declining neurocognitive adverse events, which may be a better treatment for patients with multiple brain metastases.
Availability of data and materials
The original contributions presented in the study are included in the article/supplementary material.Further inquiries can be directed to the corresponding author.
Abbreviations
- WBRT:
-
Whole Brain Radiotherapy
- HA-WBRT:
-
Hippocampus-Avoidance Whole-Brain Radiotherapy
- HA-WBRT+SIB:
-
Hippocampus-Avoidance Whole-Brain Radiotherapy plus Simultaneous Integrated Boost
- OS:
-
Overall Survival
- IC:
-
Intracranial Sontrol
- iPFS:
-
Intracranial Progression-Free Survival
- BMs:
-
Brain Metastases
- LC:
-
Local Control
- CT:
-
Computed Tomography
- MRI:
-
Magnetic Resonance Imaging
- KPS:
-
Karnofsky Performance Status
- GTV:
-
The Gross Tumor Volume
- CTV:
-
Clinical Target Volume
- PGTV:
-
The planning gross tumor volume
- PCTV:
-
The Planning Clinical Target Volume
- CTCAE:
-
The Common Terminology Criteria for Adverse Events
- NSCLC:
-
Non Small Cell Lung Cancer
- PSM:
-
Propensity Score Matching
- CR:
-
Complete Response
- PR:
-
Partial Response
- SD:
-
Stable Disease
- PD:
-
Progressive Disease
References
Barnholtz-Sloan JS, Yu C, Sloan AE et al. A nomogram for individualized estimation of survival among patients with brain metastasis. Neuro Oncol(2012)14(7): 910–8doi: https://doi.org/10.1093/neuonc/nos087.
Sneed PK, Lamborn KR, Forstner JM, et al. Radiosurgery for brain metastases: is whole brain radiotherapy necessary?Int. J Radiat Oncol Biol Phys. 1999;43(3):549.
Sneed PK, Suh JH, Goetsch SJ, et al. Int J Radiat Oncol Biol Phys. 2002;53(3):519–26. https://doi.org/10.1016/s0360-3016(02)02770-0.
O’Neill BP. Iturria NJ,Link MJ,a comparison of surgical resection and stereotactic radiosurgery in the treatment of solitary brain metastases. Int J Radiat Oncol Biol Phys(2003)55(5):1169–76. doi:https://doi.org/10.1016/s0360-3016(02)04379-1.
Brown PD, Jaeckle K, Ballman KV et al. Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial [published correction appears in JAMA. 2018;320(5):510]. JAMA (2016)316(4):401–409. doi:https://doi.org/10.1001/jama.2016.9839.
Sun HXuL, Wang Y, et al. Additional radiation boost to whole brain radiation therapy may improve the survival of patients with brain metastases in small cell lung cancer. Radiat Oncol. 2018;13(1):250. https://doi.org/10.1186/s13014-018-1198-4.
Khan M, Lin J, Liao G, et al. Whole Brain Radiation Therapy Plus Stereotactic Radiosurgery in the treatment of Brain Metastases leading to Improved Survival in patients with favorable prognostic factors. Front Oncol. 2019;9:205. 10.3389 /fonc.2019.00205.
Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. 2004;363(9422):1665. 1672. doi:10.1016/S0140-6736(04)16250-8.
Barani IJ, Benedict SH, Lin PS. Neural stem cells: implications for the conventional radiotherapy of central nervous system malignancies. Int J Radiat Oncol Biol Phys. 2007;68(2):324–33. https://doi.org/10.1016/j.ijrobp.2007.01.033.
Shibamoto Y, Baba F, Oda K et al. Incidence of brain atrophy and decline in mini-mental state examination score after whole-brain radiotherapy in patients with brain metastases: a prospective study. Int J Radiat Oncol Biol Phys(2008)72(4):1168–73. doi:https://doi.org/10.1016/j.ijrobp.2008.02.054.
Corn BW, Yousem DM, Scott CB, et al. White matter changes are correlated significantly with radiation dose. Observations from a randomized dose-escalation trial for malignant glioma (Radiation Therapy Oncology Group 83 – 02). Cancer. 1994;74(10):2828-2835.doi:10.1002/1097-0142(19941115)74:10<2828::aid-cncr2820741014>3.0.co;2-k.
Aoyama H, Tago M, Kato N, et al. Neurocognitive function of patients with brain metastasis who received either whole brain radiotherapy plus stereotactic radiosurgery or radiosurgery alone. Int J Radiat Oncol Biol Phys. 2007;68(5):1388–95. https://doi.org/10.1016/j.ijrobp.2007.03.048.
Regine WF, Scott C. Murray K,Curran W.Neurocognitive outcome in brain metastases patients treated with accelerated-fractionation vs. accelerated-hyperfrac tionated radiotherapy: an analysis from Radiation Therapy Oncology Group Study 91 – 04. Int J Radiat Oncol Biol Phys(2001)51(3):711–7. https://doi.org/10.1016/s0360-3016(01)01676-5.
Meyers CA, Smith JA, Bezjak A, et al. Neurocognitive function and progression in patients with brain metastases treated with whole-brain radiation and motexafin gadolinium: results of a randomized phase III trial. J Clin Oncol. 2004;22(1):157–65. https://doi.org/10.1200/JCO.2004.05.128.
Kocher M, Wittig A, Piroth MD, et al. Stereotactic radiosurgery for treatment of brain metastases. A report of the DEGRO Working Group on Stereotactic Radiotherapy. Strahlenther Onkol. 2014;190(6):521–32. https://doi.org/10.1007/s00066-014-06. 48 – 7.
Tsao MN, Xu W, Wong RK, et al. Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases. Cochrane Database Syst Rev. 2018;1(1):CD003869. https://doi.org/10.1002/14651858.CD003869.pub4.
Brown PD, Gondi V, Pugh S, Tome WA, Wefel JS, Armstrong TS, Bovi JA, Robinson C, Konski A, Khuntia D, Grosshans D, Benzinger TLS, Bruner D, Gilbert MR, Roberge D, Kundapur V, Devisetty K, Shah S, Usuki K, Anderson BM, Stea B, Yoon H, Li J, Laack NN, Kruser TJ, Chmura SJ, Shi W, Deshmukh S, Mehta MP, Kachnic LA. For NRG Oncology. Hippocampal avoidance during whole-brain Radiotherapy Plus Memantine for patients with brain metastases: Phase III Trial NRG oncology CC001. J Clin Oncol. 2020;38(10):1019–29. https://doi.org/10.1200/JCO.19.02767.
Prokic V, Wiedenmann N, Fels F, Schmucker M, Nieder C, Grosu AL. Whole brain irradiation with hippocampal sparing and dose escalation on multiple brain metastases: a planning study on treatment concepts. Int J Radiat Oncol Biol Phys. 2013;85:264–70.
Brown PD, Jaeckle K, Ballman KV, et al. Effect of Radiosurgery alone vs Radiosurgery with Whole Brain Radiation Therapy on cognitive function in patients with 1 to 3 brain metastases: a Randomized Clinical Trial. JAMA. 2016;316(4):401–doi. https://doi.org/10.1001/jama.2016.9839.
El Gantery MM,Abd, El Baky HM, El Hossieny HA, Mahmoud M, Youssef O. Management of brain metastases with stereotactic radiosurgery alone versus whole brain irradiation alone versus both. Radiat Oncol(2014)9:116. doi:https://doi.org/10.1186/1748-717X-9-116.
Chougule PB, Burton-Williams M, Saris S et al. Randomized treatment of brain metastasis with gamma knife radiosurgery, whole brain radiotherapy or both. Int J Radiat Oncol(2000)48(3): 114.doi:https://doi.org/10.1016/S0360-3016(00)80024-3.
Sanghavi SN, Miranpuri SS, Chappell R et al. Radiosurgery for patients with brain metastases: a multi-institutional analysis, stratified by the RTOG recursive partitioning analysis method. Int J Radiat Oncol Biol Phys(2001)51(2):426–34. doi:https://doi.org/10.1016/s0360-3016(01)01622-4.
Wang LG, Guo Y, Zhang X, et al. Brain metastasis: experience of the Xi-Jing hospital. Stereotact Funct Neurosurg. 2002;78(2):70–83. https://doi.org/10.1159/000068015.
Wegner RE, Olson AC, Kondziolka D, et al. Stereotactic radiosurgery for patients with brain metastases from small cell lung cancer. Int J Radiat Oncol Biol Phys. 2011;81(3):21–7. https://doi.org/10.1016/j.ijrobp.2011.01.001.
Bernhardt D, Hommertgen A, Schmitt D et al. Whole brain radiation therapy alone versus radiosurgery for patients with 1–10 brain metastases from small cell lung cancer (ENCEPHALON Trial): study protocol for a randomized controlled trial. Trials(2018)19(1):388. Published 2018 Jul 16. doi:https://doi.org/10.1186/s13063-018-2745-x.
Yamamoto M, Serizawa T, Higuchi Y, et al. A multi-institutional prospective observational study of stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901 study update): irradiation-related complications and long-term maintenance of Mini-Mental State Examination Scores. Int J Radiat Oncol Biol Phys. 2017;99(1):31–40. https://doi.org/10.1016/j.ijrobp.2017.04.037.
Soffietti R, Abacioglu U, Baumert B, et al. Diagnosis and treatment of brain metastases from solid tumors: guidelines from the European Association of Neuro-Oncology (EANO). Neuro Oncol. 2017;19(2):162–74. https://doi.org/10.1093/neuonc/now241.
Niranjan A, Monaco E, Flickinger J, Lunsford LD. Guidelines for multiple brain metastases Radiosurgery. Prog Neurol Surg. 2019;34:100–9. https://doi.org/10.1159/00049305.
Xue J, Kubicek GJ, Grimm J, et al. Biological implications of whole-brain radiotherapy versus stereotactic radiosurgery of multiple brain metastases. J Neurosurg. 2014;121(Suppl):60–8. https://doi.org/10.3171/2014.7.GKS141229.
Shuto T, Akabane A, Yamamoto M, et al. J Neurosurg. 2018;129(SuMultiinstitutional prospective observational study of stereotactic radiosurgery for patients with multiple brain metastases from non-small cell lung cancer (JLGK0901 study-NSCLC)ppl1):86–94. https://doi.org/10.3171/2018.7.GKS181378.
Yamamoto M, Serizawa T, Shuto T, et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. 2014;15(4):387–95. https://doi.org/10.1016/S1470-2045(14)70061-0.
Li J, Bentzen SM, Renschler M, Mehta MP. Regression after whole-brain radiation therapy for brain metastases correlates with survival and improved neurocognitive function. J Clin Oncol. 2007;25(10):1260–6. https://doi.org/10.1200/JCO.2006.09.2536.
Davey P, Hoegler D, Ennis M, Smith J. A phase III study of accelerated versus conventional hypofractionated whole brain irradiation in patients of good performance status with brain metastases not suitable for surgical excision. Radiother Oncol. 2008;88(2):173–6. https://doi.org/10.1016/j.radonc.2008.05.020.
Graham PH, Bucci J, Browne L. Randomized comparison of whole brain radiotherapy, 20Gy in four daily fractions versus 40Gy in 20 twice-daily fractions, for brain metastases. Int J Radiat Oncol Biol Phys. 2010;77(3):648–54. https://doi.org/10.1016/j.ijrobp.2009.05.032.
Wolfson AH, Bae K, Komaki R, et al. Primary analysis of a phase II randomized trial Radiation Therapy Oncology Group (RTOG) 0212: impact of different total doses and schedules of prophylactic cranial irradiation on chronic neurotoxicity and quality of life for patients with limited-disease small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2011;81(1):77–84. https://doi.org/10.1016/j.ijrobp.2010.05.013.
Oehlke O, Wucherpfennig D, Fels F, et al. Whole brain irradiation with hippocampal sparing and dose escalation on multiple brain metastases: Local tumour control and survival. Strahlenther Onkol. 2015;191(6):461–9. https://doi.org/10.1007/s00066-014-0808-9.
Gondi V, Tome WA, Marsh J, et al. Estimated risk of perihippocampal disease progression after hippocampal avoidance during whole-brain radiotherapy: safety profile for RTOG 0933. Radiother Oncol. 2010;95(3):327–31. https://doi.org/10.1016/j.radonc.2010.02.030.
Gondi V, Pugh SL, Tome WA, et al. Preservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): a phase II multi-institutional trial. J Clin Oncol. 2014;32(34):3810–6. https://doi.org/10.1200/JCO.2014.57.2909.
Popp I, Rau S, Hintz M, et al. Hippocampus-avoidance whole-brain radiation therapy with a simultaneous integrated boost for multiple brain metastases. Cancer. 2020;126(11):2694–703. https://doi.org/10.1002/cncr.32787.
Ni M, Jiang A, Liu W, et al. Whole brain radiation therapy plus focal boost may be a suitable strategy for brain metastases in SCLC patients: a multi-center study. Radiat Oncol. 2020;15(1):70. https://doi.org/10.1186/s13014-020-01509-3.
Gondi V, Hermann BP, Mehta MP, et al. Hippocampal dosimetry predicts neurocognitive function impairment after fractionated stereotactic radiotherapy for benign or low-grade adult brain tumors. Int J Radiat Oncol Biol Phys. 2012;83(4):348–54. https://doi.org/10.1016/j.ijrobp.2011.10.021.
Gondi V, Tolakanahalli R, Mehta MP, et al. Hippocampal-sparing whole-brain radiotherapy: A “how-to” technique using helical tomotherapy and linearaccelerator-based intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. 2010;78(4):1244–52. https://doi.org/10.1016/j.ijrobp.2010.01.039.
Acknowledgements
We thank the specific colleagues and institutions for the contributions of editing and reviewing the manuscript.
Funding
Research reported in the article received no funding.
Author information
Authors and Affiliations
Contributions
XW and JC make a lot of contributions to the conception and drafting of the study. HC,GL and SL collected the data. XW, JC and ZL performed the analyses and interpreted the data. XW, YZ and ZZ count the statistical results and drafted the manuscript. XW and JC carefully revised the manuscript. All authors commented on drafts of the paper and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Clinical Research Ethics Committee of The Third Hospital of Zhangzhou. Written informed consent was obtained from all participants. The acquisition of tissue specimens was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Written informed consent for publication was obtained from all participants.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, X., Chen, J., Lei, Z. et al. Propensity score-matched analysis comparing hippocampus-avoidance whole-brain radiotherapy plus simultaneous integrated boost with hippocampus‑avoidance whole-brain radiotherapy alone for multiple brain metastases-a retrospective study in multiple institutions. BMC Cancer 23, 796 (2023). https://doi.org/10.1186/s12885-023-11286-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11286-3