
Abstract
Background
The modulation of perioperative inflammation seems crucial to improve postoperative morbidity and cancer-related outcomes in patients undergoing oncological surgery. Data from the literature suggest that perioperative corticosteroids decrease inflammatory markers and might be associated with fewer complications in esophageal, liver, pancreatic and colorectal surgery. Their benefit on cancer-related outcomes has not been assessed.
Methods
The CORTIFRENCH trial is a phase III multicenter randomized double-blind placebo-controlled trial to assess the impact of a flash dose of preoperative corticosteroids versus placebo on postoperative morbidity and cancer-related outcomes after elective curative-intent surgery for digestive cancer. The primary endpoint is the frequency of patients with postoperative major complications occurring within 30 days after surgery (defined as all complications with Clavien-Dindo grade > 2). The secondary endpoints are the overall survival at 3 years, the disease-free survival at 3 years, the frequency of patients with intraabdominal infections and postoperative infections within 30 days after surgery and the hospital length of stay. We hypothesize a reduced risk of major complications and a better disease-survival at 3 years in the experimental group. Allowing for 5% of drop-out, 1 200 patients (600 per arm) should be included.
Discussion
This will be the first trial focusing on the impact of perioperative corticosteroids on cancer related outcomes. If significant, it might be a strong improvement on oncological outcomes for patients undergoing surgery for digestive cancers.
Trial registration
ClinicalTrials.gov, NCT03875690, Registered on March 15, 2019, URL: https://clinicaltrials.gov/ct2/show/NCT03875690.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Inflammation is harmful in cancer patients, especially in those undergoing surgery. It increases the risk of postoperative complications, time to recovery, hospital length of stay and impairs cancer-related outcomes (recurrence and survival) [1,2,3,4,5,6,7]. High preoperative levels of C-reactive protein and pro inflammatory adipocytokines are associated with a higher risk of postoperative morbidity in colorectal cancer surgery [8,9,10]. Perioperative inflammation is also a predictor of poorer survival in patients operated for digestive cancer whether complications occur or not [11,12,13,14,15,16,17,18,19]. So, the modulation of surgery-induced inflammation seems crucial to improve cancer survival.
The effects of a preoperative high dose of corticosteroids (flash) over the inflammatory markers have been established in different surgical fields [20,21,22,23,24,25], as well as its safety, namely in digestive surgery regarding the onset of anastomotic leakage and surgical site infection [20, 22,23,24]. Two systemic reviews and meta-analyses showed that perioperative corticosteroids decreased inflammatory markers and were associated with a diminution until 50% of the risk of some postoperative complications after esophageal, liver, pancreatic and colorectal surgery [24, 25]. Regarding the dose used, a few studies have used dexamethasone or hydrocortisone at low doses [26, 27], but most of the trials have used methylprednisolone at high doses, ranging between 500 mg independently of the patient’s weight to 30 mg/kg [24, 25, 28,29,30,31,32,33,34].
In most studies, the main endpoint was the concentration of inflammatory markers [24, 25] with little attention paid to clinically pertinent criteria or the prognosis of cancer, although the literature suggests that reducing the incidence of severe complications will improve the oncological outcomes [7, 8, 29, 30].
Thus, a prospective randomized controlled trial is warranted in order to evaluate the safety and the benefit of a flash dose of corticosteroids on postoperative morbidity and cancer-related outcomes after surgery for digestive cancer.
Methods/design
Protocol overview
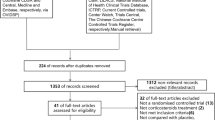
The CORTIFRENCH trial is a phase III, multi center, randomized, double-blind, placebo-controlled trial to assess the superiority of a flash dose of preoperative corticosteroids on the reduction of major complications after digestive surgical oncology. Patients likely to be included in this trial will be randomized in a 1:1 ratio between two groups: an experimental group receiving 20 mg/kg of methylprednisolone intravenous at the time of anesthesia induction and a control group receiving an intravenous placebo with an identical aspect. All members of the anesthesiology and surgical team will be unaware of the group assignments, as well as the investigator and the medical team managing the patient and recording the outcomes. Major complications (Clavien-Dindo grade > 2) [35] occurring within 30 days after surgery, postoperative and intra-abdominal infections at postoperative day 30 (D30) will be recorded and overall and disease-free survival at 3 years will be evaluated in order to assess if a flash dose of preoperative corticosteroids has a real impact on the onset of postoperative complications, recovery and cancer-related outcomes after digestive cancer surgery. The flowchart of the study has been reported in Fig. 1.

Flowchart of the trial
Objectives
The primary objective is to assess the impact of a flash dose of preoperative corticosteroids versus placebo on the onset of major complications (Clavien-Dindo > 2) [35] within 30 days after elective curative-intent surgery for digestive cancer.
Secondary objectives are to assess the safety of a preoperative flash of corticosteroids versus placebo and its influence on postoperative and intra-abdominal infections at D30, hospital length of stay and 3-year overall and disease-free survival.
Inclusion criteria
Inclusion criteria are patients older than 18 years old, undergoing elective surgery for a digestive cancer (except purely hepatic surgery), operated in a curative intent, affiliated to the French National Health System and providing their written informed consent.
Exclusion criteria
Patients with any of the following criteria will not be included in the study: emergency surgery, palliative surgery, exclusive liver surgery, surgery with concomitant hyperthermic intraperitoneal chemotherapy, pregnant or breastfeeding women, ASA score > 3, long-term ongoing oral treatments with steroids, a contra-indication to steroids therapy (active infection, ongoing viral disease, uncontrolled psychotic state, hyper sensitivity to methylprednisolone or to one of his excipients), impossibility to adhere to the medical follow-up of the trial for geographical, social or psychological reasons, patients subject to a measure of legal protection (guardianship, tutorship) and persons subject to a court order. Patients with live vaccine or live attenuated vaccine administered within 1 month before surgery and cancelled surgery without deferral will be secondary excluded.
Endpoints
The primary endpoint is the frequency of patients with postoperative major complications occurring within 30 days after surgery (D30). Major complications are defined as all complications with Clavien-Dindo grade > 2 [35].
Secondary endpoints are:
-
the overall survival at 3 years (defined as the time from surgery to death from any cause),
-
the disease-free survival at 3 years (defined as the time from surgery to first documented progressive disease or death from any cause, whichever occurs first),
-
the frequency of patients with postoperative infections occurring within 30 days after surgery and defined according to the CDC (Centers for Disease Control and Prevention) definitions,
-
the frequency of patients with intra-abdominal infections (including anastomotic fistula and intraabdominal abscess) within 30 days after surgery and defined according to the CDC definitions,
-
the hospital length of stay (in the case of death, the patient will be considered as hospitalized until D30),
-
the frequency and the type of side effects, particularly hyperglycemia, electrolyte disorders and wound healing assessed respectively by glycemia and electrolyte panel within the first 24 postoperative hours and clinical inspection at D30 follow-up visit.
Randomization
Eligible patients will be identified at the preoperative consultation with the surgeon. If the patient meets the eligible criteria, the investigating doctor will present the study. The patient will have a reflection period after the consultation and will be informed of his/her right to withdraw consent at any time without prejudice and without having to justify this decision. After receiving the written informed consent and after verification of the inclusion criteria, the patient will be included.
Patients will be randomized in a 1:1 ratio between 2 groups receiving either 20 mg/kg of intravenous methylprednisolone (experimental group) or an identical-aspect intravenous placebo (control group) at the time of anesthesia induction.
Randomization will be performed online by the investigator using the secure CleanWeb platform at the time of inclusion and stratified on the center, the site of surgery (upper digestive/pancreatic or colorectal cancer) and the surgical approach (scheduled laparoscopic or open surgery).
Blinding process
To maintain a double-bind trial, all members of the anesthesiology and surgical team will be unaware of the group assignments. Only the pharmacy of each participating center will know the randomization group in order to prepare the bag to be infused and deliver it to the anesthesiology team. If the pharmacy is not able to prepare the allocated treatment for logistical reasons, a member of the nursing staff will be authorized to carry out the preparation. Then, this person will not be involved in the follow-up of the patient to maintain the double blind.
Blind may be lifted in case of unexplained or possible toxic death, in case of a serious adverse event when the knowledge of the product administered is necessary for the care of the patient and if the medical care is different depending on the treatment receive, in the event of accidental or intentional taking by a person other than the participant tested and in the case of a suspected unexpected serious adverse reaction for the purpose of transmission to authorities.
Treatment methods
Patients randomized in the experimental group will receive 20 mg/kg intravenous methylprednisolone infused in a ready-to-use 50 mL bag of sodium chloride 0.9% during 30 min at the time of anesthetic induction.
Patients randomized in control/placebo group will receive 50 mL of intravenous sodium chloride 0.9% in a ready-to-use bag during 30 min at the time of anesthetic induction. As methylprednisolone is colorless, bags containing sodium chloride alone or sodium chloride plus methylprednisolone will identical aspect.
Live vaccines or live attenuated vaccines will be contra-indicated during the month preceding surgery and until 3 months later.
Surgical management
Pre-operative check-up
Each institution will prepare patients and scheduled surgery according to its own institutionally validated protocols. All patients included will undergo the preoperative evaluation currently performed at each institution. Preoperative immunonutrition will not be mandatory but its use will be recorded.
Intraoperative management
At the time of the anesthesia induction, methylprednisolone or placebo will be administrated according to the randomization group. Diabetics patients will be closely monitored in both groups during and immediately after surgery by capillary glycemia every 3 h in order to adjust insulin therapy as appropriate. Patients considered at risk for postoperative nausea and emesis will receive a single preoperative dose of 4–8 mg of dexamethasone intravenous (equivalent to 20–40 mg of methylprednisolone), following the guidelines of the French Society of Anesthesiology and Reanimation (SFAR). This information will be recorded.
Postoperative management
Clinical and biological follow-up (blood samples) will be performed according to the protocols of each institution. The only specific requirement of the study will be an electrolyte panel and fasting glycemia performed within the first 24 h after surgery in order to detect a possible effect of corticosteroids. The postoperative management, monitoring and follow-up will be as usual according to each institution’s current practices, but each participating center will be asked to record the following data: day of oral refeeding, mean daily pain visual analog scale, onset of fever or any complication (whether infectious or not), laboratory and imaging studies performed between surgery and postoperative day 30.
Follow-up
According to each center’s protocol, a D30 visit will be scheduled between postoperative days 28 and 45. Patients will undergo a clinical evaluation by the surgeon and will be asked about any events occurring since the initial hospital discharge. Any complications occurred since the initial discharge or detected during the examination will be recorded. In case of re-hospitalization between hospital discharge and the scheduled follow-up visit at postoperative D30, all data related to any complications will be collected. Dead patients will be considered to have been hospitalized between the date of death and postoperative D30.
The study will end at 3 years. At the end of the study, vital status (including date and cause of death if appropriate) and information about disease progression (including the date of discovery in case of recurrence) will be collected and recorded for all included patients.
Data collection
The data will be entered into an e-CRF (electronic Case Report Form) specifically developed for this study using a Clinical Data Management System (CMDS-CleanWeb). All required information for the study will be entered as and when it is obtained. Thanks to automatic checks, in case of missing or inconsistent data, request for correction will be sent to participating centers via the CMDS. If corrections are necessary, they will be made directly using the CMDS. At the end of the study, a blind review of data will be performed and in case of additional queries, it should be resolved before the final database lock.
Statistical analysis and sample size
This study is a phase III multi center randomized double blind placebo-controlled trial. According to the literature, the incidence of major complications at D30 after surgery is 26% [36]. We hypothesized this proportion will decrease to 18% in patients with corticosteroids administration. Based on these hypotheses with an alpha risk of 5% and a power of 90% and including an interim analysis at the half of the inclusions, 1184 analyzable patients (592 per arm) are required. Allowing for 5% of drop-out, 1200 patients (600 per arm) will be included. Statistical analyses will be performed at the coordinating center (INSERM CIC 1432 of Dijon).
Demographics and baseline characteristics
Patient’s characteristics at baseline will be described in terms of frequencies for categorical variables and in terms of means (+/- standard deviation) or medians (interquartile range) for continuous variables. These characteristics will be compared between groups using Chi squared (or Fisher’s exact test) or t-Test (or Mann-Whitney test) when appropriate.
Interim analysis
One interim analysis will be performed after the inclusion of 592 patients (296 per arm). The interim analysis will assess the superiority of the experimental arm versus the control group for the primary endpoint: early termination will be considered only if superiority is met. The interim analysis will have a two-sided alpha level of 0.0003. According to the O’Brien-Fleming spending rule [37], this will leave a two-sided alpha level of 0.049 for the final analysis. The data safety monitoring board will decide if the trial should be stopped according to the results of the interim analysis.
Main analysis
The main analysis will be conducted on intention-to-treat (ITT) analysis. The proportion of patients with postoperative major complications at D30 will be compared using Chi-square test. If there are any differences between the two groups concerning the baseline characteristics, a logistic regression analysis including confounding factors will allow us to check the robustness of the conclusion based on the main analysis. Patients with missing data on adjustment variables will be excluded from multivariate analysis. Results will be expressed using Odds ratios and their 95% confidence intervals. Patients lost to follow-up will be first analyzed successively under the maximal bias analysis (postoperative major complications in corticosteroids patients and no major complications in placebo patients) and then excluded. This ITT analysis will be completed with an m-ITT analysis (exclusion of all subjects in the ITT population who don’t meet inclusion and non-inclusion criteria) and with a per-protocol (PP) analysis (exclusion of all subjects in the ITT population who meet any of the following criteria: no study treatment administered or major protocol deviation).
Secondary analysis
The frequency of patients with postoperative infections and intra-abdominal infections will be compared between groups according to the same strategy as the main analysis (bivariate comparisons using Chi-square, multivariate analysis using logistic regression). The number of days without hospitalization at D30 will be expressed as means +/- SD or as medians (IQR) as appropriate. The Kaplan Meir methods will be used to estimate the overall and the disease-free survival curves. The corresponding survival rates will be calculated at 3 years. Median survival will also be calculated and differences between survival curves assessed using log rank test. A Cox regression analysis will be used to assess the impact of potential prognostic factors on overall survival and disease-free survival at 3 years. Subgroup analyses according to the stratification groups (site of surgery, surgical approach) will be performed for exploratory purposes. Descriptive statistics will be used to summarize adverse events and compared between the two groups. Safety analyses will be performed on the safety population which will comprise all randomized patients who consented to participate in the study and who have been given a treatment.
Participating centers
Twenty-three French centers will participate in this study: University Hospital of Amiens, University Hospital of Dijon, University Hospital of Besançon, Georges François Leclerc Cancer Center in Dijon, Hospital of Auxerre, Simone Veil Hospital in Beauvais, Bicêtre University Hospital in Le Kremlin-Bicêtre, Claude Huriez University Hospital in Lille, La Croix Saint Simon Hospital in Paris, University Hospital of Reims, Gustave Dron Hospital in Tourcoing, Pierre Benite University Hospital in Lyon, North University Hospital in Marseille, Cochin University Hospital in Paris, René-Dubos Hospital in Cergy-Pontoise, University Hospital of Nancy, Saint-Antoine University Hospital in Paris, Avicenne University Hospital in Paris, Rangueil University Hospital in Toulouse, University Hospital of Angers, University Hospital of Montpellier, Pitié Salpêtrière University Hospital in Paris, University Hospital of Rouen.
Ethical and safety approvals
This study protocol was approved on March 8th, 2019 by the Institutional Review Board of the Auvergne-Rhone-Alpes ethic committee. The institutional promoter is the University Hospital of Dijon. The Agence Nationale de Securité des Médicaments et des Produits de Santé gave its authorization for the study on March 12th, 2019. The study will be conducted in accordance with the ethical principles of the Declaration of Helsinki and the recommendations of the Good Clinical Practices guidelines.
Discussion
Current evidence suggests a strong impact of perioperative inflammation on postoperative outcomes, including morbidity and cancer-related survival [1,2,3,4,5,6,7, 28, 29]. According to previous studies showing that a lower inflammatory activity leads to improved postoperative morbidity, different approaches have been raised to modulate perioperative inflammation, namely the use of specific anesthetics [38], preoperative immunonutrition [39, 40], or perioperative corticosteroids [8, 10, 23, 24]. Preliminary results suggest lower postoperative morbidity and an improved recovery. A flash dose of corticosteroids administered at the time of surgery could improve lung function and decrease pain, fatigue, anorexia and ileus, leading to enhanced postoperative recovery and decreased hospital stay. Patients could also begin adjuvant treatment earlier after surgery and overall and disease-free survival might be improved.
Several highlights should be emphasized regarding this trial. First, its design (randomized, placebo-control, double-blind, multicentric) will provide high-quality evidence in this field. Moreover, all endpoints will be clinically significant rather than intermediate biomarkers; some of them will focus on postoperative complications and others on cancer prognosis. Twenty-three French medical institutions will include patients in a pragmatic way: each institution will manage his/her patient according to its own protocols, except for the administration of the methylprednisolone or the placebo and the necessary surveillance of glycemia and electrolytes within the first 24 postoperative hours. To avoid excessive heterogeneity within the surgical population, we focus only on digestive cancer surgery [41]. Registering preoperative inflammatory markers will also permit to detect a potential influence on postoperative outcomes.
We will voluntarily exclude purely hepatic surgery because in such a setting, the benefit of the preoperative flash dose of corticosteroids might be specifically related to the hepatic ischemia/reperfusion induced by clamping and measured in terms of liver function [42, 43]. The specific of hepatic tolerance to clamping is beyond the scope of this trial whose main aim is to assess the flash dose of corticosteroids as a new standard in perioperative medicine.
Regarding the dose of corticosteroids we chose, Mc Sorley et al. stated in their review safety and efficacy of methyldprenisolone with doses ranging between 10 and 30 mg/kg [23]. We fond 20 mg/kg of methylprednisolone is a good compromise.
Regarding the potentials adverse outcomes induced by a flash dose of corticosteroids, the benefit/risk ratio seems to be strongly in favor of a potential benefit [24, 44, 45]. Indeed, a single high dose of corticosteroids should have no impact on the healing process or the risk of infection because these side effects do exist only with long-course therapy. The most frequent expected adverse effects are hyperglycemia and hypokalemia. To prevent these complications glycemia and kaliemia will be monitored immediately after the operation and the following day.
To conclude, in the CORTIFRENCH randomized double-blind placebo-controlled trial, we aim to show that a flash dose of corticosteroids at the time of surgery is safe, improves the postoperative recovery and the cancer-related outcomes in patients operated for a digestive cancer.
Trial status
The trial is registered at ClinicalTrials.gov with the identifier NCT03875690. The trial is currently ongoing. The recruitment of subjects began in July 2019 and is expected to finish in September 2026.
Availability of data and materials
Indirect nominative data can’t be shared publicly under French laws. The study team is available to collaboration with other research teams on reasonable request to access study data. Expressions of interest to access study data, made out to the corresponding author, will be considered and then group-level or individual-level deidentified data may be shared as appropriate.
Abbreviations
- ASA:
-
American Society of Anesthesiologists
- CDC:
-
Center for Disease Control and Prevention
- eCRF:
-
Electronic Case Report Form
- CMDS:
-
Clinical Data Management System
- D30:
-
postoperative day 30
- IQR:
-
Interquartile Range
- SD:
-
Standard Deviation
References
Woo HD, Kim K, Kim J. Association between preoperative C-reactive protein level and colorectal cancer survival: a meta-analysis. Cancer Causes Control. 2015;26:1661–70.
Rocha P, Morgan CJ, Templeton AJ, Pond GR, Naik G, Sonpavde G. Prognostic impact of Creactive protein in metastatic prostate cancer: a systematic review and meta-analysis. Oncol Res Treat. 2014;37:772–6.
Liao C, Yu Z, Guo W, Liu Q, Wu Y, Li Y, Bai L. Prognostic value of circulating inflammatory factors in non-small cell lung cancer: a systematic review and meta-analysis. Cancer Biomark. 2014;14:469–81.
Dai J, Tang K, Xiao W, Yu G, Zeng J, Li W, et al. Prognostic significance of C-reactive protein in urological cancers: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15:3369–75.
Yu Q, Yu XF, Zhang SD, Wang HH, Wang HY, Teng LS. Prognostic role of C-reactive protein in gastric cancer: a meta-analysis. Asian Pac J Cancer Prev. 2013;14:5735–40.
Artinyan A, Orcutt ST, Anaya DA, Richardson P, Chen GJ, Berger DH. Infectious postoperative complications decrease long-term survival in patients undergoing curative surgery for colorectal cancer: a study of 12,075 patients. Ann Surg. 2015;261:497–505.
Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg. 2011;253:890–9.
De Magistris L, Paquette B, Orry D, Facy O, Di Giacomo G, Rat P, Binquet C, Ortega-Deballon P. Preoperative inflammation increases the risk of infection after elective colorectal surgery: results from a prospective cohort. Int J Colorectal Dis. 2016;31:1611–7.
Ortega-Deballon P, Ménégaut L, Fournel I, Orry D, Masson D, Binquet C, Facy O. Are adiponectin and leptin good predictors of surgical infection after colorectal surgery? A prospective study. Surg Infect (Larchmt). 2015;16:566–71.
Ortega-Deballon P, Duvillard L, Scherrer ML, Deguelte-Lardière S, Bourredjem A, Petit JM, Bonithon-Kopp C, AGARIC Study group. Preoperative adipocytokines as a predictor of surgical infection after colorectal surgery: a prospective survey. Int J Colorectal Dis. 2014;29:23–9.
Reeh M, Ghadban T, Uzunoglu FG, Nentwich MF, Bockhorn M, Pantel K, et al. Hamburg-Glasgow classification: preoperative staging by combination of disseminated tumour load and systemic inflammation in esophageal carcinoma. Br J Cancer. 2017;117:612–8.
Dolan RD, McSorley ST, Horgan PG, Laird B, McMillan DC. The role of the systemic inflammatory response in predicting outcomes in patients with advanced inoperable cancer: Systematic review and meta-analysis. Crit Rev Oncol Hematol. 2017;116:134–46.
Egenvall M, Mörner M, Martling A, Gunnarsson U. Prediction of Outcome after Curative Surgery for Colorectal Cancer: Preoperative Haemoglobin, CRP and Albumin. Colorectal Dis. 2018;20:26–34.
Jagadesham VP, Lagarde SM, Immanuel A, Griffin SM. Systemic inflammatory markers and outcome in patients with locally advanced adenocarcinoma of the oesophagus and gastrooesophageal junction. Br J Surg. 2017;104:401–7.
Li N, Tian GW, Wang Y, Zhang H, Wang ZH, Li G. Prognostic Role of the Pretreatment CReactive Protein/Albumin Ratio in Solid Cancers: A Meta-Analysis. Sci Rep. 2017;7:41298.
Li C, Xu Q, Chen L, Luo C, Ying J, Liu J. C-reactive protein (CRP) as a prognostic factor for colorectal cancer after surgical resection of pulmonary metastases. Bull Cancer. 2017;104:232–6.
Toiyama Y, Shimura T, Yasuda H, Fujikawa H, Okita Y, Kobayashi M, et al. Clinical burden of C-reactive protein/albumin ratio before curative surgery for patients with gastric cancer. Anticancer Res. 2016;36:6491–8.
Watt DG, McSorley ST, Park JH, Horgan PG, McMillan DC. A Postoperative Systemic Inflammation Score Predicts Short- and Long-Term Outcomes in Patients Undergoing Surgery for Colorectal Cancer. Ann Surg Oncol. 2017;24:1100–9.
Bert M, Devilliers H, Orry D, Rat P, Facy O, Ortega-Deballon P. Preoperative inflammation is an independent factor of worse prognosis after colorectal cancer surgery. J Visc Surg. 2021;158(4):305–11.
Toner AJ, Ganeshanathan V, Chan MT, Ho KM, Corcoran TB. Safety of perioperative glucocorticoids in elective noncardiac surgery: a systematic review and meta-analysis. Anesthesiology. 2017;126:234–48.
Da Silva EM, Hochman B, Ferreira LM. Perioperative corticosteroids for preventing complications following facial plastic surgery. Cochrane Database Syst Rev. 2014;6:CD009697.
Sauerland S, Nagelschmidt M, Mallmann P, Neugebauer EA. Risks and benefits of preoperative high dose methylprednisolone in surgical patients: a systematic review. Drug Saf. 2000;23:449–61.
Corcoran T, Kasza J, Short TG, O’Loughlin E, Chan MT, Leslie K, et al. ENIGMA-II investigators. Intraoperative dexamethasone does not increase the risk of postoperative wound infection: a propensity score-matched post hoc analysis of the ENIGMA-II trial (EnDEX). Br J Anaesth. 2017;118:190–9.
McSorley ST, Horgan PG, McMillan DC. The impact of preoperative corticosteroids on the systemic inflammatory response and postoperative complications following surgery for gastrointestinal cancer: A systematic review and meta-analysis. Crit Rev Oncol Hematol. 2016;101:139–50.
Srinivasa S, Kahokehr AA, Yu TC, Hill AG. Preoperative glucocorticoid use in major abdominal surgery: systematic review and meta-analysis of randomized trials. Ann Surg. 2011;254:183–91.
Zargar-Shoshtari K, Sammour T, Kahokehr A, et al. Randomized clinical trial of the effect of glucocorticoids on peritoneal inflammation and postoperative recovery after colectomy. Br J Surg. 2009;96:1253–61.
Laaninen M, Sand J, Nordback I, Vasama K, Laukkarinen J. Perioperative hydrocortisone reduces major complications after pancreaticoduodenectomy: a randomized controlled trial. Ann Surg. 2016;264:696–702.
Weijs TJ, Dieleman JM, Ruurda JP, Kroese AC, Knape HJ, van Hillegersberg R. The effect of perioperative administration of glucocorticoids on pulmonary complications after transthoracic oesophagectomy: a systematic review and meta-analysis. Eur J Anaesthesiol. 2014;31:685–94.
Lu ZR, Rajendran N, Lynch AC, Heriot AG, Warrier SK. Anastomotic leaks after restorative resections for rectal cancer compromise cancer outcomes and survival. Dis Colon Rectum. 2016;59:236–44.
Lin G, Han SY, Xu YP, Mao WM. Increasing the interval between neoadjuvant chemoradiotherapy and surgery in esophageal cancer: a meta-analysis of published studies. Dis Esophagus. 2016;29:1107–14.
Nagelschmidt M, Fu ZX, Saad S, et al. Preoperative high dose methylprednisolone improves patients outcome after abdominal surgery. Eur J Surg. 1999;165(10):971–8.
Vignali A, Di Palo S, Orsenigo E, et al. Effect of prednisolone on local and systemic response in laparoscopic vs. open colon surgery: a randomized, double-blind, placebo-controlled trial. Dis Col Rect. 2009;52:1080–8.
Schmidt SC, Hamann S, Langrehr JM, Hoflich C, Mittler J, Jacob D, et al. Preoperative highdose steroid administration attenuates the surgical stress response following liver resection: results of a prospective randomized study. J Hepatobiliary Pancreat Surg. 2007;14:484–92.
Schulze S, Andersen J, Overgaard H, et al. Effect of prednisolone on the systemic response and wound healing after colonic surgery. Arch Surg. 1997;132:129–35.
Dindo D, Demartines N, Clavien PA, et al. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Tevis SE, Kennedy GD. Postoperative complications and implications on patient-centered outcomes. J Surg Res. 2013;181:106–13.
O’Brien PC, Fleming TR. A multiple testing procedure for clinical trials. Biometrics. 1979;35:549–56.
Perry NJS, Buggy D, Ma D. Can Anesthesia Influence Cancer Outcomes After Surgery? JAMA Surg. 2019;154(4):279–280.
Niu JW, Zhou L, Liu ZZ, Pei DP, Fan WQ, Ning W. A Systematic Review and Meta-Analysis of the Effects of Perioperative Immunonutrition in Gastrointestinal Cancer Patients. Nutr Cancer. 2021;73(2):252–61.
Buzquurz F, Bojesen RD, Grube C, Madsen MT, Gögenur I. Impact of oral preoperative and perioperative immunonutrition on postoperative infection and mortality in patients undergoing cancer surgery: systematic review and meta-analysis with trial sequential analysis. BJS Open. 2020;4(5):764–75.
Abdelmalak BB, Bonilla A, Mascha EJ, Maheshwari A, Tang WH, You J, et al. Dexamethasone, light anaesthesia, and tight glucose control (DeLiT) randomized controlled trial. Br J Anaesth. 2013;111:209–21.
Hayashi Y, Takayama T, Yamazaki S, et al. Validation of Perioperative Steroids Administration in Liver Resection: A Randomized Controlled Trial. Ann Surg. 2011;253:50–5.
Aldrighetti L, Pulitano C, Arru M, et al. Impact of preoperative steroids administration on ischemia-reperfusion injury and systemic responses in liver surgery: a prospective randomized study. Liver Transpl. 2006;12:941–9.
Corcoran TB, Myles PS, Forbes AB, Cheng AC, Bach LA, O’Loughlin E, et al. Dexamethasone and Surgical-Site Infection. N Engl J Med. 2021;384(18):1731 41.
Corcoran T, Kasza J, Short TG, O’Loughlin E, Chan MTV, Leslie K, et al. Intraoperative dexamethasone does not increase the risk of postoperative wound infection: a propensity score-matched post hoc analysis of the ENIGMA-II trial (EnDEX). Br J Anaesth. 2017;118(2):190 9.
Acknowledgements
The authors thank the funding source (the Programme Hospitalier de Recherche Clinique from the French Ministry of Health), all the investigators of the study and Aurélie Bouvier, Emilie Galizzi, Marion Cortier, Camille Fleck and Pierre Landreau for their help.
Funding
This project is funded by the French Ministry of Health through the Programme Hospitalier de Recherche Clinique (PHRC) 2017. The PHRC underwent a full per-review of this study protocol prior to submission. The funding body has no role in collecting, analyzing, or interpreting data.
Author information
Authors and Affiliations
Contributions
JM, IF and POD wrote the manuscript. AD assisted in writing the manuscript. JM, IF, AB and AC were involved in the study design. POD, AD, JMR, PZ, GP, LBB, SD, ZL, LS, DO, AA, FM, FM, GP, NT, AV, SB, MM, DF, BB, CT, AV, FRS, AH, SG, and JL were involved in the study design and the inclusion of patients in the trial. POD is the coordinating principal investigator. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study protocol was approved by the Institutional Review Board of the Auvergne-Rhone-Alpes ethic committee on March 8th, 2019 (ref 2019/AU1499) The study complies with the Declaration of Helsinki and the principles of good clinical practice guidelines. Informed consent is obtained from each patient in written form prior to randomization.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
CORTIFRENCH Trial: List of investigators.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Magnin, J., Fournel, I., Doussot, A. et al. Benefit of a flash dose of corticosteroids in digestive surgical oncology: a multicenter, randomized, double blind, placebo-controlled trial (CORTIFRENCH). BMC Cancer 22, 913 (2022). https://doi.org/10.1186/s12885-022-09998-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09998-z