
Abstract
Background
Concurrent chemoradiotherapy (CCRT) has become the cornerstone of treatment for patients with locally advanced non-small cell lung cancer (LA-NSCLC). The aim of this study was to compare the efficacies and toxicities of different CCRT regimens in the treatment of LA-NSCLC by adopting a network meta-analysis (NMA).
Methods
An exhaustive search of PubMed, EMBASE, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL) was conducted to identify relevant studies from inception to October 1, 2020. Direct and indirect evidence was combined to calculate the odds radios (ORs) and 95% confidence intervals (CIs), as well as to plot the surface under the cumulative ranking (SUCRA) curves. Cluster analyses were adopted to compare the efficacies and toxicities of different CCRT regimens according to the similarity of 2 variables. Publication bias was detected by comparison-adjusted funnel plots.
Results
Twenty-two studies were enrolled in this NMA, including 18 regimens: CCRT (cisplatin + etoposide), CCRT (carboplatin + paclitaxel), CCRT (pemetrexed + carboplatin), CCRT (pemetrexed + cisplatin), CCRT (docetaxel + cisplatin), CCRT (S-1 + cisplatin), CCRT (mitomycin + vindesine + cisplatin), CCRT (cisplatin + vinorelbine), CCRT (cisplatin), CCRT (etoposide + cisplatin + amifostine), RT, CCRT (5-FU), CCRT (paclitaxel + cisplatin), CCRT (irinotecan + carboplatin), CCRT (nedaplatin), CCRT (carboplatin + etoposide), CCRT (paclitaxel), and CCRT (carboplatin). The results indicated that the regimens with CCRT (cisplatin + etoposide), CCRT (carboplatin + paclitaxel), CCRT (pemetrexed + cisplatin), CCRT (S-1 + cisplatin), and CCRT (cisplatin + vinorelbine) had relatively better efficacies compared with other regimens. As for toxicities of different CCRT regimens, the CCRT (carboplatin + paclitaxel), CCRT (pemetrexed + cisplatin), and CCRT (docetaxel + cisplatin) were relatively lower.
Conclusions
Our study demonstrated that CCRT (pemetrexed + cisplatin) and CCRT (carboplatin + paclitaxel) might be the best options for the treatment of LA-NSCLC, and CCRT (pemetrexed + cisplatin) had the highest 3-year overall survival (OS) rate.
Similar content being viewed by others


Introduction
Lung cancer is the most common malignancy worldwide and the leading cause of cancer-related deaths [1, 2]. In many countries, lung cancer remains a major public health threat with a high overall incidence and high frequency of diagnosis [1, 2]. Every year, 2.2 million people are diagnosed with lung cancer and 1.6 million die from the disease around the world [3]. In China, lung cancer has the highest number of new cases and deaths of all cancers (820, 000 and 710, 000, respectively), accounting for 17.9 and 23.8% of all cancer incidence and mortality [3]. No-small cell lung cancer (NSCLC) approximately accounts for 85% of all lung cancer [2, 3], and approximately 30% of patients are diagnosed with locally advanced NSCLC (LA-NSCLC) [4]. Currently, greater effort in encouraging smoking cessation, screening in high-risk individuals, and prompt diagnostic procedures have significantly brought a rise of early-stage disease [5], but the most common presentation among non-metastatic patients remains LA-NSCLC.
Over the past decade, molecular oncology has rapidly elucidated so-called “driver mutations” in NSCLC, leading to the emergence of targeted therapies. While the initial clinical trials did not demonstrate a survival benefit with EGFR-TKIs for the overall population of advanced NSCLC patients [6], a specific subset of patients carrying mutations on the kinase domain of EGFR gene were found to be highly sensitive to the targeted drugs [7]. However, targeted therapy is ineffective in patients with negative driver genes. Therefore, for the unresectable patients with negative driver genes, combined-modality therapy using chemotherapy and thoracic radiation therapy is very crucial [8, 9]. The Radiation Therapy Oncology Group (RTOG) trial 0617 compared standard-dose (SD, 60 Gy) versus high-dose (HD, 74 Gy) radiation with concurrent chemotherapy for stage III NSCLC. Median overall survival (OS) was 28.7 and 20.3 months in the SD and HD arms, respectively, 5-year OS and progression-free survival (PFS) rates were 32.1% and 23% and 18.3% and 13%, respectively [10]. Consequently, the concurrent chemoradiotherapy (CCRT) regimen has been recommended as current standard therapeutic paradigms of care for patients with unresectable LA-NSCLC [11]. Meanwhile, radiation therapy has become more effective and safe, the RTOG 94–10 trial proved that CCRT arm with once-daily RT had a better median OS (17.0 months) [12]. Although the CCRT is considered the standard care [8] and a variety of CCRT combinations and schedules are currently used, and current guidelines list many regimens as recommended therapeutic options for LA-NSCLC. However, the adverse effects of certain agents, which lead to failure to complete the scheduled regimen, extension of chemotherapy intervals or reduction of the recommended dosage, have limited their clinical application, and the optimal chemotherapy regimen remains unclear. Therefore, it is extremely important to investigate and identify effective CCRT regimen with low toxicity.
Network meta-analysis (NMA), also known as multiple-treatments comparison (MTC), enables us to synthesize data from direct (within-trail) comparisons and can provide indirect (inter-trail) comparisons of multiple treatment regimens when direct comparisons are unavailable [13]. In addition, the cluster analysis enables us to estimate the rank probability that, witch of the treatments is the best, the second best, etc. Thus, we performed a NMA to compare the efficacies and toxicities of different CCRT regimens and to research which is the best regimen in the treatment of LA-NSCLC.
Materials and methods
Literature and database search strategy
We performed systematic literature search of PubMed, EMBASE (via Ovid interface), Web of Science (via campus network of Sichuan University), and the Cochrane Central Register of Controlled Trials (CENTRAL) (via Ovid interface) from their incipiency to October 1, 2020. We used the Medical Subject Headings/Emtree combined with free text words of locally advanced non-small lung cancer, LA-NSCLC, concurrent chemoradiotherapy, concurrent chemotherapy and radiotherapy, cisplatin, docetaxel, pemetrexed, carboplatin, S-1, etoposide, amifostine, vinorelbine, paclitaxel, nedaplatin, mitomycin, vindesine, irinotecan, 5-FU, and RT. Additionally, reference lists of eligible published clinical trials and meta-analyses were also tracked manually to identify other relevant studies. Only studies published in English were included. All the initially identified articles were scrutinized independently by two reviewers (Qiangqiang Zheng and Shihui Min).
Selection criteria
Eligible studies were selected according to the following inclusion criteria: (a) the study design was a randomized controlled trials (RCT), (b) different chemotherapeutic interventions were included, (c) research subjects were patients with LA-NSCLC, (d) literature containing the following outcome measures, including overall response rate (ORR), 1-year OS rate, 2-year OS rate, 3-year OS rate, and toxicities (anemia, leukopenia, neutropenia, thrombocytopenia, febrile neutropenia, pneumonitis, nausea, vomiting, and esophagitis). Studies were excluded if the following criteria were met: (a) the articles were meta-analyses, letters, reviews, editorial materials, meeting abstracts, case reports, and expert opinions, (b) not human studies, (c) not RCT, (d) not English literature, (e) patients who received surgery or adjuvant chemotherapy, (f) studies without adequate information about efficacy and toxicity. Two authors (Qiangqiang Zheng and Shihui Min) independently assessed the titles and abstracts of studies to identify whether these studies met the inclusion criteria. In the case of existing discrepancies, the two authors reached consensus via discussion.
Data extraction and quality assessment
Data were extracted from the selected studies by two independent investigators (Qiangqiang Zheng and Shihui Min). The following information were extracted: (a) publication data including first author, publication year, country, sample size, and therapeutic regimens, (b) the efficacy of different CCRT regimens in the treatment of LA-NSCLC, including ORR, 1-year OS rate, 2-year OS rate, and 3-year OS rate, (c) the toxicity of different CCRT regimens, including anemia, leukopenia, neutropenia, thrombocytopenia, febrile neutropenia, pneumonitis, nausea, vomiting, and esophagitis. Newcastle–Ottawa Quality Assessment Scale (NOS) was used to estimate the quality of every original study [14]. Three perspectives including selection, comparability, and ascertainment of exposure and outcomes were considered for a semi-quantitative estimation. A study with NOS ≥ 6 was regarded as a high-quality study [15].
Data synthesis and analysis
To assess the efficacy and toxicity of different CCRT regimens in the treatment of LA-NSCLC, we determined odds radios (ORs) and their 95% confidence intervals (CIs) under a fixed effect model or a random effect model as the appropriate summarized statistics, and the Z-test was performed to detect the significance of the pooled effect size [16].
Heterogeneity among the pooled studies was evaluated by Cochran Q-statistic and I2 test [17]. Random effect model was used when significant heterogeneity existed among studies (P < 0.1 or I2 > 50%). Otherwise, a fixed effect model was employed.
A network evidence plot was drawn with the nodes indicating interventions, the node size representing sample size, and the thickness of lines referring to the accuracy of the effect size of the comparison between 2 studies.
A surface under the cumulative ranking (SUCRA) curve was used to compare the SUCRA value of different CCRT regimens to ascertain the efficacy and toxicity ranks, the larger the SUCRA value, the better the efficacy or the lower the toxicity [18]. Cluster analyses were adopted to compare efficacy and toxicity of different CCRT regimens according to the similarity of 2 variables [18].
A comparison-adjusted funnel plot was used to evaluate the small-study effect, which considered the difference of the summary effect for each set of studies [19].
Finally, we declared that all of the above statistical analyses were accomplished by STATA (version 14.0) (Stata Corporation, College Station, TX, USA). All statistical tests were two-tailed with a P < 0.05 being considered statistically significant.
Results
Overview of the literature search
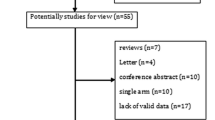
The study selection process was shown in Fig. 1. Computer-based database searches and complementary manual search retrieved a total of 1,032 relevant articles. After removing 564 duplicates, we read the titles and abstracts of the 468 studies left, 145 studies were excluded because they either did not English studies (n = 22), or did not human studies (n = 40), or were letters, reviews, meta-analyses, case reports, and meeting abstracts (n = 83). After meticulously reading, 301 studies were excluded because 231 studies were not RCT, 42 studies were not related to CCRT, and 28 studies were not related to LA-NSCLC. In total, 22 eligible studies [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] with 3,178 patients were enrolled in this NMA.

Flowchart of the study selection process. CCRT = concurrent chemoradiotherapy. CENTRAL = Cochrane central register of controlled trials. RCT = randomized controlled trial. LA-NSCLC = local advanced non-small cell lung cancer
Characteristics of the included studies
Twenty-two articles published between 1992 and 2017, consisting of a total number of 3,178 participants with LA-NSCLC were included in this NMA. There were 21 two-arm studies and 1 three-arm study with 20 comparisons. Briefly, study sample sizes ranged from 22 to 555. From the 22 studies, 10 studies were conducted in Caucasians, and the other 12 studies were Asians. Among all individuals, 507 were treated with CCRT (cisplatin + etoposide) regimen, 227 with CCRT (carboplatin + paclitaxel) regimen, 348 with CCRT (pemetrexed + cisplatin) regimen, 254 with CCRT (mitomycin + vindesine + cisplatin) regimen, 229 with CCRT (cisplatin) regimen, 584 with RT, and remaining 1029 were treated with other CCRT regimens. The detailed characteristics of the included studies were diaplayed in Table 1.
Quality assessment
Two researchers were assigned to evaluate all of the included studies. The results of the quality assessment involving 22 RCTs were presented in Table 2. The mean NOS score was 8.4 (range from 7 to 9), which suggested a good quality level.
Pairwise meta-analyses for efficacies of different CCRT regimens
Random effect models were used to perform direct pairwise matchings, and the results of efficacies were shown in Table 3. The results demonstrated that RT had a worse efficacy in ORR compared with CCRT (5-FU) and CCRT (nedaplatin) (OR = 0.45, 95% CI = 0.23–0.90; OR = 0.38, 95% CI = 0.17–0.85; respectively). For the 1-year OS rate, CCRT (docetaxel + cisplatin) had a worse efficacy compared with CCRT (mitomycin + vindesine + cisplatin) (OR = 0.45, 95% CI = 0.23–0.87), CCRT (cisplatin) had a better efficacy compared with the RT (OR = 4.08, 95% CI = 2.16–7.72), and RT had a worse efficacy compared with CCRT (nedaplatin) (OR = 0.39, 95% CI = 0.17–0.90). As for 2-year OS rate, CCRT (S-1 + cisplatin) had a better efficacy compared with CCRT (cisplatin) (OR = 3.15, 95% CI = 1.43–6.96), CCRT (etoposide + cisplatin) had a better efficacy compared with CCRT (docetaxel + cisplatin) (OR = 3.32, 95% CI = 1.47–7.51), CCRT (paclitaxel + carboplatin) had a better efficacy compared with CCRT (irinotecan + carboplatin) (OR = 1.32, 95% CI = 0.84–2.09), CCRT (cisplatin) had a better efficacy compared with the RT (OR = 5.78, 95% CI = 1.88–17.80), and RT had a worse efficacy compared with CCRT (carboplatin + etoposide) (OR = 0.46, 95% CI = 0.22–0.96). In terms of 3-year OS rate, CCRT (S-1 + cisplatin) had a better efficacy compared with CCRT (cisplatin) (OR = 3.08, 95% CI = 1.37–6.94), RT had a worse efficacy compared with CCRT (carboplatin) (OR = 0.42, 95% CI = 0.21–0.83), CCRT (etoposide + cisplatin) had a better efficacy compared with CCRT (docetaxel + cisplatin) and CCRT (paclitaxel + cisplatin) (OR = 3.09, 95% CI = 1.38–6.88; OR = 1.98, 95% CI = 1.07–3.65; respectively), CCRT (paclitaxel + carboplatin) had a better efficacy compared with CCRT (irinotecan + carboplatin) (OR = 1.70, 95% CI = 1.03–2.79), and CCRT (cisplatin) had a better efficacy compared with RT (OR = 4.90, 95% CI = 1.03–23.37).
Pairwise meta-analyses for hematological toxicities of different CCRT regimens
We conducted direct-paired comparisons of incidences of hematological toxicities, and the results were displayed in Table 4. Compared with CCRT (carboplatin), the incidence of leukopenia with RT was relatively lower (OR = 0.01, 95%CI = 0.00–0.05). Compared with CCRT (mitomycin + vindesine + cisplatin), the incidences of anemia, neutropenia, thrombocytopenia, and febrile neutropenia with CCRT (carboplatin + paclitaxel) were relatively lower (OR = 0.34, 95% CI = 0.15–0.76; OR = 0.02, 95% CI = 0.01–0.04; OR = 0.20, 95% CI = 0.09–0.44; OR = 0.08, 95% CI = 0.03–0.20; respectively). Compared with CCRT (carboplatin + paclitaxel), the incidence of neutropenia with CCRT (etoposide + cisplatin) was relatively higher (OR = 3.16, 95% CI = 1.57–6.34). Compared with CCRT (pemetrexed + cisplatin), the incidences of neutropenia and febrile neutropenia with CCRT (etoposide + cisplatin) were relatively higher (OR = 1.79, 95% CI = 1.20–2.66; OR = 2.42, 95% CI = 1.08–5.40; respectively). Compared with CCRT (irinotecan + carboplatin), the incidences of neutropenia and thrombocytopenia with CCRT (carboplatin + paclitaxel) were relatively lower (OR = 0.26, 95% CI = 0.16–0.42; OR = 0.42, 95% CI = 0.18–0.99; respectively). Compared with CCRT (mitomycin + vindesine + cisplatin), the incidences of neutropenia, thrombocytopenia, and febrile neutropenia with CCRT (docetaxel + cisplatin) were relatively lower (OR = 0.10, 95% CI = 0.04–0.26; OR = 0.06, 95% CI = 0.01–0.27; OR = 0.45, 95% CI = 0.24–0.84; respectively). Compared with CCRT (pemetrexed + cisplatin) and CCRT (S-1 + cisplatin), the incidences of leukopenia with CCRT (vinorelbine + cisplatin) were relatively lower (OR = 0.38, 95% CI = 0.16–0.90; OR = 0.19, 95% CI = 0.06–0.55; respectively). Compared with CCRT (irinotecan + carboplatin), the incidences of neutropenia and thrombocytopenia with CCRT (mitomycin + vindesine + cisplatin) were relatively higher (OR = 13.66, 95% CI = 6.48–28.77; OR = 2.13, 95% CI = 1.14–3.96; respectively). Compared with CCRT (pemetrexed + cisplatin), the incidences of febrile neutropenia with CCRT (mitomycin + vindesine + cisplatin) were relatively higher (OR = 7.05, 95% CI = 3.31–15.01).
Pairwise meta-analyses for non-hematological toxicities of different CCRT regimens
Pairwise comparisons of non-hematological toxicites were accomplished for the different CCRT regimens, and the results were demonstrated in Table 5. Compared with CCRT (mitomycin + vindesine + cisplatin), the incidences of nausea/vomiting and pneumonitis with CCRT (carboplatin + paclitaxel) were relatively lower (OR = 0.09, 95% CI = 0.03–0.23; OR = 0.40, 95% CI = 0.21–0.76; respectively). Compared with CCRT (irinotecan + carboplatin) regimen, the incidences of nausea/vomiting and pneumonitis with CCRT (mitomycin + vindesine + cisplatin) were relatively higher (OR = 8.10, 95% CI = 3.51–18.69; OR = 2.08, 95% CI = 1.13–3.83; respectively). Compared with CCRT (paclitaxel + cisplatin), the incidence of esophagitis with CCRT (etoposide + cisplatin) was relatively higher (OR = 3.75, 95% CI = 1.43–9.87). Compared with CCRT (irinotecan + carboplatin), the incidence of esophagitis with CCRT (carboplatin + paclitaxel) was relatively higher (OR = 3.90, 95% CI = 1.07–14.28). Compared with CCRT (5-FU), the incidence of esophagitis with RT was relatively lower (OR = 0.24, 95% CI = 0.07–0.91). Compared with CCRT (paclitaxel + cisplatin), the incidence of pneumonitis with CCRT (etoposide + cisplatin) was relatively lower (OR = 0.47, 95% CI = 0.24–0.91).
Inconsistency tests for efficacies and toxicities of different CCRT regimens
Inconsistency tests showed that the results of direct and indirect evidences of different CCRT regimens were consistency, the consistency model was adopted (P > 0.05) (Tables 6, 7 and 8).
Network meta-analyses for efficacies of different CCRT regimens.
The results of network meta-analyses in efficacies and the network evidence plots were displayed in Table 9 and Fig. 2A. The results suggested that in terms of efficacies, CCRT (cisplatin + etoposide) had better efficacies in 1-year OS rate, 2-year OS rate, and 3-year OS rate than CCRT (5-FU) (OR = 9.49, 95%CI = 1.26–71.34; OR = 14.68, 95% CI = 1.94–110.81; OR = 21.37, 95% CI = 2.31–197.35; respectively). CCRT (cisplatin + pemtrexed) had better efficacies in 1-year OS rate, 2-year OS rate, and 3-year OS rate than RT (OR = 9.04, 95% CI = 1.25–65.44; OR = 14.74, 95% CI = 2.07–105.14; OR = 24.05, 95% CI = 2.67–216.31; respectively). CCRT (S-1 + cisplatin) had better efficacies in 1-year OS rate, 2-year OS rate, and 3-year OS rate than RT (OR = 6.51, 95% CI = 1.81–23.34; OR = 18.37, 95% CI = 4.35–77.48; OR = 15.11, 95% CI = 2.60–87.95; respectively). CCRT (cisplatin + vinorelbine) had better efficacies in 1-year OS rate, 2-year OS rate, and 3-year OS rate than RT (OR = 5.54, 95% CI = 1.01–30.39; OR = 16.25, 95% CI = 2.78–95.14; OR = 13.79, 95% CI = 1.80–105.85; respectively). CCRT (cisplatin) had better efficacies in 1-year OS rate, 2-year OS rate, and 3-year OS rate than RT (OR = 4.08, 95% CI = 2.16–7.72; OR = 5.78, 95% CI = 1.78–18.71; OR = 4.89, 95% CI = 1.03–23.34; respectively). CCRT (carboplatin + paclitaxel) had better efficacies in 1-year OS rate and 2-year OS rate than RT (OR = 10.83, 95% CI = 1.28–91.52; OR = 11.38, 95% CI = 1.29–100.34; respectively). CCRT (S-1 + cisplatin) had better efficacies in 1-year OS rate and 2-year OS rate than CCRT (5-FU) (OR = 6.33, 95% CI = 1.52–26.34; OR = 7.57, 95% CI = 1.12–51.28; respectively). CCRT (S-1 + cisplatin) had better efficacies in 1-year OS rate and 2-year OS rate than CCRT (carboplatin + etoposide) (OR = 4.94, 95% CI = 1.12–21.81; OR = 8.42, 95% CI = 1.61–44.00; respectively). CCRT (S-1 + cisplatin) had better efficacies in 1-year OS rate and 2-year OS rate than CCRT (carboplatin) (OR = 5.35, 95% CI = 1.38–20.68; OR = 12.62, 95% CI = 2.69–59.26; respectively). CCRT (cisplatin) had better efficacies in 1-year OS rate and 2-year OS rate than CCRT (carboplatin) (OR = 3.36, 95% CI = 1.54–7.29; OR = 3.97, 95% CI = 1.08–14.58; respectively). CCRT (carboplatin + paclitaxel) had better efficacies in 2-year OS rate and 3-year OS rate than CCRT (docetaxel + cisplatin) (OR = 3.32, 95% CI = 1.37–8.04; OR = 3.09, 95% CI = 1.38–6.88; respectively). CCRT (pemetrexed + cisplatin) had better efficacies in 2-year OS rate and 3-year OS rate than CCRT (docetaxel + cisplatin) (OR = 3.34, 95% CI = 1.22–9.11; OR = 3.47, 95% CI = 1.45–8.30; respectively). CCRT (pemetrexed + cisplatin) had better efficacies in 2-year OS rate and 3-year OS rate than CCRT (carboplatin) (OR = 10.13, 95% CI = 1.31–78.23; OR = 10.10, 95% CI = 1.01–101.01; respectively). CCRT (S-1 + cisplatin) had better efficacies in 2-year OS rate and 3-year OS rate than CCRT (cisplatin) (OR = 3.18, 95% CI = 1.38–7.31; OR = 3.09, 95% CI = 1.37–6.97; respectively). CCRT (paclitaxel + cisplatin) had better efficacies in 2-year OS rate and 3-year OS rate than RT (OR = 11.65, 95% CI = 1.39–97.88; OR = 10.80, 95% CI = 1.08–108.39; respectively). CCRT (etoposide + cisplatin) had a better efficacy in 1-year OS rate than CCRT (paclitaxel + cisplatin) (OR = 9.24, 95% CI = 1.12–76.48). CCRT (carboplatin + paclitaxel) had better efficacy in 1-year OS rate than CCRT (5-FU) and CCRT (carboplatin) (OR = 10.54, 95% CI = 1.14–97.62; OR = 8.91, 95% CI = 1.01–78.75; respectively). CCRT (pemetrexed + cisplatin) and CCRT (cisplatin) had better efficacies in 1-year OS rate than CCRT (5-FU) (OR = 8.80, 95% CI = 1.10–70.28; OR = 3.97, 95% CI = 1.62–9.75; respectively). CCRT (cisplatin) and CCRT (paclitaxel + cisplatin) had better efficacies in 1-year OS rate than CCRT (carboplatin + etoposide) (OR = 3.10, 95% CI = 1.15–8.34; OR = 9.87, 95% CI = 1.03–94.58; respectively). CCRT (paclitaxel + cisplatin) had a better efficacy in 1-year OS rate than CCRT (carboplatin) (OR = 10.69, 95% CI = 1.21–94.11). CCRT (S-1 + cisplatin) had a better efficacy in 2-year OS rate than CCRT (nedaplatin) (OR = 8.06, 95% CI = 1.32–49.10). CCRT (mitomycin + vindesine + cisplatin) had a better efficacy in 2-year OS rate than RT (OR = 11.70, 95% CI = 1.23–110.88). CCRT (cisplatin + vinorelbine) had better efficacies in 2-year OS rate than CCRT (carboplatin + etoposide) and CCRT (carboplatin) (OR = 7.45, 95% CI = 1.06–52.13; OR = 11.17, 95% CI = 1.75–71.40; respectively). CCRT (cisplatin + etoposide) had a better efficacy in 3-year OS rate than CCRT (irinotecan + carboplatin) (OR = 1.98, 95% CI = 1.07–3.65). CCRT (pemetrexed + cisplatin) had a better efficacy in 3-year OS rate than CCRT (carboplatin + paclitaxel) (OR = 3.94, 95% CI = 1.05–14.72). CCRT (carboplatin + paclitaxel) had better efficacies in 3-year OS rate than CCRT (cisplatin), CCRT (paclitaxel + cisplatin), CCRT (irinotecan + carboplatin), and CCRT (nedaplatin) (OR = 4.91, 95% CI = 1.05–23.03; OR = 2.23, 95% CI = 1.10–4.49; OR = 4.41, 95% CI = 1.07–18.18; OR = 12.68, 95% CI = 1.01–158.37; respectively). CCRT (carboplatin) had a better efficacy in 3-year OS rate than RT (OR = 2.38, 95% CI = 1.19–4.75). However, the ORRs of all CCRT regimens had no differences.

Network evidence plots of different CCRT regimens. A Network evidence plots of ORR and OS of different CCRT regimens. B Network evidence plots of toxicities of different CCRT regimens. The width of the lines is proportional to the number of trials comparing every pair of treatments, and the size of every circle is proportional to the number of randomly assigned participants (sample size). A = CCRT (cisplatin + etoposide). B = CCRT (carboplatin + paclitaxel). C = CCRT (pemetrexed + carboplatin). CCRT = concurrent chemoradiotherapy. D = CCRT (pemetrexed + cisplatin). E = CCRT (docetaxel + cisplatin). F = CCRT (S-1 + cisplatin). G = CCRT (mitomycin + vindesine + cisplatin). H = CCRT (cisplatin + vinorelbine). I = CCRT (cisplatin). J = CCRT (etoposide + cisplatin + amifostine). K = RT. L = CCRT (5-FU). M = CCRT (paclitaxel + cisplatin). N = CCRT (irinotecan + carboplatin). NMA = network meta-analysis. O = CCRT (nedaplatin). ORR = overall response rate. OS = overall survival. P = CCRT (carboplatin + etoposide). Q = CCRT (paclitaxel). R = CCRT (carboplatin)
Network meta-analyses for hematological toxicities of different CCRT regimens
The results of network meta-analyses in hematological toxicities and the network evidence plots were shown in Table 10 and Fig. 2B. The results demonstrated that in terms of hematological toxicities, the incidences of anemia, neutropenia, and thrombocytopenia with CCRT (mitomycin + vindesine + cisplatin) were higher than CCRT (carboplatin + paclitaxel) (OR = 2.94, 95% CI = 1.32–6.55; OR = 53.03, 95% CI = 24.50–114.78; OR = 5.11, 95% CI = 2.28–11.45; respectively). The incidences of neutropenia and febrile neutropenia with CCRT (cisplatin + etoposide) were higher than CCRT (pemetrexed + cisplatin) (OR = 1.79, 95% CI = 1.20–2.66; OR = 2.42, 95% CI = 1.08–5.40; respectively). The incidences of neutropenia and thrombocytopenia with CCRT (irinotecan + carboplatin) were higher than CCRT (carboplatin + paclitaxel) (OR = 3.88, 95% CI = 2.37–6.37; OR = 2.40, 95% CI = 1.01–5.71; respectively). The incidence of leukopenia with CCRT (cisplatin + vinorelbine) was higher than CCRT (S-1 + cisplatin) and CCRT (cisplatin) (OR = 5.34, 95% CI = 1.23–23.14; OR = 7.41, 95% CI = 1.14–48.39; respectively). The incidence of leukopenia with CCRT (carboplatin) was higher than CCRT (S-1 + cisplatin), CCRT (cisplatin), and RT (OR = 25.48, 95% CI = 2.70–240.60; OR = 35.35, 95% CI = 5.23–239.20, OR = 38.74, 95% CI = 8.50–176.58; respectively). The incidence of leukopenia with CCRT (nedaplatin) was higher than CCRT (cisplatin) and RT (OR = 22.60, 95% CI = 1.74–293.03; OR = 24.76, 95% CI = 2.53–242.76; respectively). The incidence of neutropenia with CCRT (etoposide + cisplatin) was higher than CCRT (paclitaxel + carboplatin) (OR = 3.28, 95% CI = 1.52–7.09). The incidence of neutropenia with CCRT (irinotecan + carboplatin) was higher than CCRT (etoposide + cisplatin) (OR = 16.15, 95% CI = 5.43–48.06). The incidence of neutropenia with CCRT (mitomycin + vindesine + cisplatin) was higher than CCRT (pemetrexed + cisplatin), CCRT (docetaxel + cisplatin), and CCRT (irinotecan + carboplatin) (OR = 28.85, 95% CI = 9.03–92.14; OR = 173.39, 95% CI = 7.49–4015.10; OR = 13.66, 95% CI = 5.46–34.17; respectively). The incidence of febrile neutropenia with CCRT (cisplatin + vinorelbine) was higher than CCRT (cisplatin + etoposide) (OR = 6.91, 95% CI = 1.39–34.42).
Network meta-analyses for non-hematological toxicities of different CCRT regimens
The results of network meta-analyses in non-hematological toxicities and the network evidence plots were shown in Table 10 and Fig. 2B. The results displayed that in terms of non-hematological toxicities, the incidences of pneumonia with CCRT (cisplatin + vinorelbine) and CCRT (irinotecan + carboplatin) were higher than CCRT (cisplatin + etoposide) (OR = 5.65, 95% CI = 1.82–17.56; OR = 2.14, 95% CI = 1.10–4.16; respectively). The incidences of pneumonia with CCRT (carboplatin + paclitaxel), CCRT (docetaxel + cisplatin), CCRT (mitomycin + vindesine + cisplatin), CCRT (paclitaxel + cisplatin), and CCRT (irinotecan + carboplatin) were higher than CCRT (etoposide + cisplatin + amifostine) (OR = 17.61, 95% CI = 1.62–191.58; OR = 46.79, 95% CI = 2.16–1013.71; OR = 44.08, 95% CI = 3.72–521.75; OR = 16.68, 95% CI = 1.68–165.50; OR = 21.23, 95% CI = 1.76–255.84; respectively). The incidence of pneumonia with CCRT (mitomycin + vindesine + cisplatin) was higher than CCRT (pemetrexed + cisplatin) (OR = 6.89, 95% CI = 1.42–33.51). The incidences of esophagitis with CCRT (cisplatin + etoposide) and CCRT (carboplatin + paclitaxel) were higher than CCRT (irinotecan + carboplatin) (OR = 3.75, 95% CI = 1.43–9.87; OR = 3.90, 95% CI = 1.07–14.28; respectively). The incidences of esophagitis with CCRT (carboplatin + paclitaxel) and CCRT (pemetrexed + cisplatin) were higher than CCRT (paclitaxel + cisplatin) (OR = 3.96, 95% CI = 1.20–13.03; OR = 3.78, 95% CI = 1.20–11.94; respectively). The incidence of esophagitis with CCRT (5-FU) was higher than RT (OR = 4.08, 95% CI = 1.10–15.11). The incidence of nausea/vomiting with CCRT (mitomycin + vindesine + cisplatin) was higher than CCRT (carboplatin + paclitaxel) and CCRT (irinotecan + carboplatin) (OR = 11.41, 95% CI = 4.38–29.77; OR = 8.10, 95% CI = 1.78–36.76; respectively). The incidence of the nausea/vomiting with CCRT (nedaplatin) was higher than CCRT (cisplatin), RT, and CCRT (carboplatin) (OR = 7.88, 95% CI = 1.51–41.20; OR = 10.43, 95% CI = 2.29–47.54; OR = 15.76, 95% CI = 1.45–170.99; respectively).
Cumulative probability of efficacies and toxicities of different CCRT regimens
As shown in Table 11 and Fig. 3, the SUCRA values of different CCRT regimens demonstrated that in terms of efficacies, the ORR of CCRT (nedaplatin) ranked the highest (75.9%), followed by CCRT (paclitaxel) (73.2%). The 1-year OS rate of CCRT (paclitaxel + cisplatin) ranked the highest (85.9%), followed by CCRT (paclitaxel + carboplatin) (78.4%), CCRT (mitomycin + vindesine + cisplatin) (76.5%), CCRT (etoposide + cisplatin) (72.5%), and CCRT (pemetrexed + cisplatin) (70.4%). The 2-year OS rate of CCRT (S-1 + cisplatin) ranked the highest (83.8%), followed by CCRT (etoposide + cisplatin) (79.7%), CCRT (pemetrexed + cisplatin) (79.7%), and CCRT (carboplatin + paclitaxel) (68.6%). The 3-year OS rate of CCRT (pemetrexed + cisplatin) ranked the highest (95.1%), followed by CCRT (etoposide + cisplatin) (89.4%). As for toxicities, the incidences of anemia and febrile neutropenia with CCRT (pemetrexed + cisplatin) ranked the lowest (26.7%, 12.0%, respectively), followed by CCRT (paclitaxel + carboplatin) (39.3%, 16.7%, respectively). The incidences of neutropenia and thrombocytopenia with CCRT (docetaxel + cisplatin) ranked the lowest (10.3%, 27.4%, respectively), followed by CCRT (paclitaxel + carboplatin) (21.6%, 32.9%, respectively). The incidences of leukopenia with CCRT (cisplatin) and RT ranked the lowest (17.9%, 17.9%, respectively). The incidence of nausea/vomiting with CCRT (carboplatin) ranked the lowest (23.2%), followed by CCRT (cisplatin + vinorelbine) (26.1%). The incidence of esophagitis with CCRT (paclitaxel + cisplatin) ranked the lowest (16.9%), and the incidence of pneumonitis with CCRT (etoposide + cisplatin + amifostine) ranked the lowest (17.7%).

The SUCRA plots of efficacies and toxicities of different CCRT regimens. A The SUCRA plots of efficacies of different CCRT regimens. B The SUCRA plots of toxicities of different CCRT regimens. SUCRA curve was used to compare the SUCRA value of different CCRT regimens to ascertain the efficacies or the toxicities ranks, the larger the SUCRA value, the better the efficacy or the lower the toxicity. A = CCRT (cisplatin + etoposide). B = CCRT (carboplatin + paclitaxel). C = CCRT (pemetrexed + carboplatin). CCRT = concurrent chemoradiotherapy. D = CCRT (pemetrexed + cisplatin). E = CCRT (docetaxel + cisplatin). F = CCRT (S-1 + cisplatin). G = CCRT (mitomycin + vindesine + cisplatin). H = CCRT (cisplatin + vinorelbine). I = CCRT (cisplatin). K = RT. L = CCRT (5-FU). M = CCRT (paclitaxel + cisplatin). N = CCRT (irinotecan + carboplatin). O = CCRT (nedaplatin). ORR = overall response rate. OS = overall survival. P = CCRT (carboplatin + etoposide). Q = CCRT (paclitaxel). R = CCRT (carboplatin). SUCRA = surface under the cumulative ranking
Cluster analyses regarding efficacies and toxicities in the included studies
The cluster analyses based on SUCRA values indicated that the regimens with CCRT (cisplatin + etoposide), CCRT (carboplatin + paclitaxel), CCRT (pemetrexed + cisplatin), CCRT (S-1 + cisplatin), and CCRT (cisplatin + vinorelbine) had relatively better efficacies compared with other regimens (Fig. 4A). As for toxicities of different CCRT regimens, the hematological toxicities of CCRT (carboplatin + paclitaxel), CCRT (pemetrexed + cisplatin), and CCRT (docetaxel + cisplatin) were relatively lower (Fig. 4B). However, the differences of non-hematological toxicities with different CCRT regimens was not significant (Fig. 4B).

Clustered ranking plots based on SUCRA values of efficacies and efficacies with different CCRT regimens in the treatment of LA-NSCLC. A Clustered ranking plots based on SUCRA values of efficacies with different CCRT regimens in the treatment of LA-NSCLC. B Clustered ranking plots based on SUCRA values of toxicities with different CCRT regimens in the treatment of LA-NSCLC. Studies on the upper right corner have better efficacy or higher toxicity. A = CCRT (cisplatin + etoposide). B = CCRT (carboplatin + paclitaxel). C = CCRT (pemetrexed + carboplatin). CCRT = Concurrent Chemoradiotherapy. D = CCRT (pemetrexed + cisplatin). E = CCRT (docetaxel + cisplatin). F = CCRT (S-1 + cisplatin). G = CCRT (mitomycin + vindesine + cisplatin). H = CCRT (cisplatin + vinorelbine). I = CCRT (cisplatin). K = RT. L = CCRT (5-FU). LA-NSCLC = locally advanced non-small cell lung cancer. M = CCRT (paclitaxel + cisplatin). N = CCRT (irinotecan + carboplatin). O = CCRT (nedaplatin). ORR = overall response rate. OS = overall survival. P = CCRT (carboplatin + etoposide). Q = CCRT (paclitaxel). R = CCRT (carboplatin). SUCRA = surface under the cumulative ranking
Publication bias regarding efficacy and toxicity in the included studies
The comparison-adjusted funnel plots of efficacy and toxicity of CCRT regimens showed that there were no publication bias among the included studies (Fig. 5).

Comparison-adjusted funnel plots of efficacies and toxicities of different CCRT regimens. A Comparison-adjusted funnel plots of efficacies of different CCRT regimens. B Comparison-adjusted funnel plots of toxicities of different CCRT regimens. A = CCRT (cisplatin + etoposide). B = CCRT (carboplatin + paclitaxel). C = CCRT (pemetrexed + carboplatin). CCRT = concurrent chemoradiotherapy. D = CCRT (pemetrexed + cisplatin). E = CCRT (docetaxel + cisplatin). F = CCRT (S-1 + cisplatin). G = CCRT (mitomycin + vindesine + cisplatin). H = CCRT (cisplatin + vinorelbine). I = CCRT (cisplatin). K = RT. L = CCRT (5-FU). M = CCRT (paclitaxel + cisplatin). N = CCRT (irinotecan + carboplatin). O = CCRT (nedaplatin). ORR = overall response rate. OS = overall survival. P = CCRT (carboplatin + etoposide). Q = CCRT (paclitaxel). R = CCRT (carboplatin)
Discussion
LA-NSCLC keeps a high incidence and mortality around the world. Although many kinds of CCRT regimens have been utilized for treating it, the OS is still poor because of the high probability of lurks and recurrence. To give valuable suggestions for treatments through comparing the efficacy and safety, we conducted the NMAs among 18 CCRT regimens with 14 drugs commonly used for LA-NSCLC, including cisplatin, docetaxel, pemetrexed, paclitaxel, carboplatin, etoposide, and others. The main advantage of our study over published systematic reviews is that we could compare a variety of CCRT regimens simultaneously by applying the network method.
The results of efficacy conducted in the present study revealed that ORR of CCRT (nedaplatin) were higher than other regimens. Nedaplatin is a second generation platinum analog, and its mechanism of antitumor action is suggested as its interference on DNA adducts formation by affecting DNA damage repairing proteins, transcription factors and DNA polymerases [42]. It has been verified that nedaplatin concurrent radiotherapy for treating stage III/IV non-surgical patients with NSCLC showed a good curative effect of better ORR and well-tolerated [20], which is similar with the results of our NMA. However, it had a bad performance in known adverse events including leukopenia and nausea/vomiting, which suggested that the CCRT (nedaplatin) regimen may have a good efficacy and a high incidence of toxicity for the treatment in LA-NSCLC.
Focusing on the long-term efficacy, 1-year OS rate, 2-year OS rate, and 3-year OS rate of CCRT (etoposide + cisplatin), CCRT (paclitaxel + carboplatin), and CCRT (pemetrexed + cisplatin) were relatively higher. Moreover, the toxicities of CCRT (paclitaxel + carboplatin) and CCRT (pemetrexed + cisplatin) were relatively lower. Cisplatin, as an assistant drug for chemotherapy, was often combined with other drugs to treat cancer but was also combined by some side effects [43]. Pemetrexed is a potent inhibitor of thymidylate synthase [44] and other folate-dependent enzymes, including dihydrofolate reductase and glycinamide ribonucleotide formyl transferase [45]. Pemetrexed was formerly approved as a single agent for second-line treatment of advanced NSCLC [46]. Some studies have suggested that the combination of cisplatin and pemetrexed has promising activity and tolerability in locally advanced unresectable Stage III NSCLC when combined with RT [47,48,49]. Mornex F et al. [47] evaluated chemotherapy with cisplatin and pemetrexed and found that it is well tolerated and appears to be the only third-generation agent that can likely be recommended safely at full dose with concurrent RT, avoiding compromise on activity against distant disease while optimizing local control. The pemetrexed + cisplatin regimen are known to cause severe side effects, but our study indicated that the incidences of anemia and febrile neutropenia with CCRT (pemetrexed + cisplatin) were lower than other regimens, and other toxicities had not significant differences with other regimens. The doublet combinations of platinum compounds (cisplatin or carboplatin) with taxanes (paclitaxel or docetaxel) are also the reference regimens for NSCLC [50]. The carboplatin plus paclitaxel regimen is one of the most commonly used regimens, and there is considerable interest in the combination of carboplatin + paclitaxel and RT for the treatment of LA-NSCLC. Several studies had certified that CCRT (carboplatin + paclitaxel) had a better efficacy in the treatment of unresectable NSCLC [11, 51].
Subsequently, the cluster analysis of efficacies and toxicities of CCRT regimens demonstrated that CCRT (carboplatin + paclitaxel) and CCRT (pemetrexed + cisplatin) regimens had better efficacies and lower toxicities, may be the best regimens in treating LA-NSCLC. In addition, CCRT (cisplatin + etoposide), CCRT (S-1 + cisplatin), and CCRT (cisplatin + vinorelbine) also have relatively better efficacies, but the incidences of neutropenia with CCRT (cisplatin + etoposide), esophagitis with CCRT (S-1 + cisplatin), and leukopenia, febrile neutropenia, and esophagitis with CCRT (cisplatin + vinorelbine) were higher. Yamaguchi M et al. [52] reported that 74.2% of NSCLC patients treated with cisplatin plus etoposide regimen had incidence of neutropenia, which is similar to our study.
Despite the existence of dilemma in treatment of unresectable LA-NSCLC, the years since about 2010 have brought great progress in the understanding of the molecular mechanisms related to tumour immunology [53]. The discovery of these mechanisms has led to the development of several new drugs, including immune checkpoint inhibitors (ICIS) that specifically target PD-1, PD-L1, and CTLA-4 receptor, as well as drugs that target other regions of the immune system pathway. The use of ICIS as consolidation therapy within a curative-intent management plan for LA-NSCLC represents a promising strategy to improve the prognosis after CCRT. In NSCLC, the antitumour immunogenic effects of radiation might act as an adjuvant to checkpoint blockade. Theoretically, the combination of RT and ICIS could lead to enhanced responses by increasing the exposure or altering the presentation of tumour-related antigens to immune system cells. In a study of patients with advanced NSCLC treated with pembrolizumab, PFS and OS were longer in those who had previously received RT than in those who had not [54]. Moreover, compared with patients who received pembrolizumab alone, patients who were randomized to receive stereotactic body radiation therapy for a single metastasis before receiving pembrolizumab for advanced NSCLC experienced an improved response rate (41% vs. 19%) and PFS (6.4 months vs. 1.8 months; HR: 0.55; P = 0.04) [55]. The NICOLAS study is the first completed single-arm phase II trial in stage III NSCLC evaluating hierarchically first the safety and then the efficacy of adding nivolumab concurrently to standard definitive concurrent chemoradiotherapy, and it suggested that 44% of the cases being attributed to treatment toxicity [56]. Although there are many studies on the treatment measures after CCRT, the systematic analysis needs further research.
A few limitations should be mentioned. Firstly, due to the lack of available appropriate head-to-head RCTs, the quantity of studies included for one specific comparison was small, we could not compare all treatment interventions simultaneously for each complication in one network. Secondly, the sample size of some included RCTs were relatively small, which may affect the results. Thirdly, all of the data was extracted from published RCT studies, and individual patient data were not used. Therefore, the quality control of the data was difficult. Fourthly, the qualities of the included RCTs varied, however, our comparison-adjusted funnel plot did not exhibit any asymmetry, indicating that there were no significant publication bias. Finally, studies were conducted over a wide time period. With improvements in equipment and a greater understanding of quality metrics to augment the rate of detection of LA-NSCLC, it is possible that detection rates could have varied over time.
Conclusion
In conclusion, for the treatment of LA-NSCLC, CCRT (pemetrexed + cisplatin) and CCRT (paclitaxel + carboplatin) resulted in better efficacies and lower toxicities simultaneously. The 3-year OS rate of CCRT (pemetrexed + cisplatin) ranked the highest. These findings may help clinicians in their choice of proper CCRT regimens for LA-NSCLC patients.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CCRT:
-
Concurrent chemoradiotherapy
- CENTRAL:
-
Cochrane central register of controlled trials
- CI:
-
Confidence interval
- LA-NSCLC:
-
Locally advanced non-small cell lung cancer
- MTC:
-
Multiple-treatments comparison
- NMA:
-
Network meta-analysis
- OS:
-
Newcastle–Ottawa Quality Assessment Scale
- OR:
-
Odds radio
- ORR:
-
Overall response rate
- OS:
-
Overall survival
- RCT:
-
Randomized controlled trials
- RT:
-
Radiation Therapy
- RTOG:
-
Radiation Therapy Oncology Group
- SUCRA:
-
Surface under the cumulative ranking
References
Torre LA, Bray F, Siegel RL, Ferlay J, Joannie LT, Jemal A. Global cancer statistics, 2012. Ca A Cancer J Clin. 2015;65(1):33–64, 31.
Chen W, Zheng R, Baade PD, Zhang SW, Zeng HM, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30.
Yang P, Allen MS, Aubry MC, Wampfler JA, Claude D. Clinical features of 5,628 primary lung cancer patients: experience at Mayo Clinic from 1997 to 2003. Chest. 2005;128(1):452–62.
Verma V. Stereotactic radiotherapy versus surgery for early-stage operable lung cancer: more questions than answers. J Natl Compr Canc Netw. 2015;13(10):1293.
Thatcher N, Chang A, Parikh P, Pereira JR, Ciuleanu T, Pawel JV, Thongprasert S, Tan EH, Pemberton K, Archer V, Carroll K. Gefitinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet. 2005;366(9496):1527.
Tamura K, Okamoto I, Kashii T. Multicentre prospective phase II trial of gefitinib for advanced non-small cell lung cancer with epidermal growth factor receptor mutations: results of the West Japan Thoracic Oncology Group trial (WJTOG0403). Br J Cancer. 2008;98(5):907.
Auperin A, Pechoux CL, Rolland E, Curran WJ, Furuse K, Fournel P, Belderbos J, Clamon G, Ulutin HC, Paulus R, Yamanaka T, Bozonnat MC, Uitterhoeve A, Wang X, Stewart L, Arriagada R, Burdett S, Pignon JP. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non–small-cell lung cancer. J Am Soc Clin Oncol. 2010;28(13):2181.
Garrido P, Engel-Riedel W, Serke M, Giraud P, Ricardi U, Vallejo C, Visseren-Grul C, Ameryckx S, Soldatenkova V, Chouaki N, Novello S. Final results from a Phase II study of pemetrexed and cisplatin with concurrent thoracic radiation after Pem-Cis induction in patients with unresectable locally advanced non-squamous non-small cell lung cancer (NSCLC). Lung Cancer. 2015;88(2):160–6.
Bradley JD, Hu C, Komaki RR, Masters GA, Blumenschein GR, Schild SE, Bogart JA, Forster KM, Magliocco AM, Kavadi VS, Narayan S, Iyengar P, Robinson CG, Wynn RB, Koprowski CD, Olson MR, Meng J, Paulus R, Curran WJ Jr, Choy H. Long-term results of NRG oncology RTOG 0617: standard- versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage III non-small-cell lung cancer. J Clin Oncol. 2020;38(7):706–14.
Vansteenkiste J, De RD, Eberhardt WE, Lim E, Senan S, Felip P. Early and locally advanced non-small cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol Official J Eur Soci Med Oncol. 2013;24 Suppl 6(suppl_3):vi89.
Curran WJ, Paulus R, Langer CJ, Komaki R, Lee JS, Hauser S, Movsas B, Wasserman T, Rosenthal SA, Gore E, Machtay M, Sause W, Cox JD. Sequential vs Concurrent Chemoradiation for Stage III Non-Small Cell Lung Cancer: Randomized Phase III Trial RTOG 9410. J Natl Cancer Inst. 2011;103(19):1452.
Thijs V, Lemmens R, Fieuws S. Network meta-analysis: simultaneous meta-analysis of common antiplatelet regimens after transient ischaemic attack or stroke. Eur Heart J. 2008;29(9):1086.
Lo KL, Mertz D, Loeb M. Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. 2014;14(1):45.
Wong WC, Cheung CS, Hart GJ. Development of a quality assessment tool for systematic reviews of observational studies (QATSO) of HIV prevalence in men having sex with men and associated risk behaviours. Emerg Themes Epidemiol. 2008;5(1):23.
Chen H, Manning AK, Dupuis J. A Method of Moments Estimator for Random Effect Multivariate Meta-Analysis. Biometrics. 2012;68(4):1278.
Dan J, White IR, Riley RD. Quantifying the impact of between-study heterogeneity in multivariate meta-analyses. Stat Med. 2012;31(29):3805–20.
Anna C, Higgins JPT, Dimitris M, Panagiota S, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS One. 2013;8(10):e76654.
Peters JL, Sutton AJ, Jones DR, Abrams KR, Moreno SG. Assessing publication bias in meta-analyses in the presence of between-study heterogeneity. J Roy Stat Soc. 2010;173(3):575–91.
Chen F, Hu P, Liang N, Xie J, Yu S, Tian T, Zhang JX, Deng G, Zhang JD. Concurrent chemoradiotherapy with weekly nedaplatin versus radiotherapy alone in elderly patients with non-small-cell lung cancer. Clin Transl Oncol. 2017;20:294–301.
Liang J, Bi N, Wu S, Chen M, Lv C, Zhao L, Shi A, Jiang W, Xu Y, Zhou Z, Wang W, Chen D, Hui Z, Lv J, Zhang H, Feng Q, Xiao Z, Wang X, Liu L, Zhang T, Du L, Chen W, Shyr Y, Yin W, Li J, He J, Wang L. Etoposide and cisplatin versus paclitaxel and carboplatin with concurrent thoracic radiotherapy in unresectable stage III non-small cell lung cancer: a multicenter randomized phase III trial. Ann Oncol. 2017;28(4):777–83.
Feng J, Xu J, Wang X, Zhao DJ. S-1 plus cisplatin with concurrent radiotherapy versus cisplatin alone with concurrent radiotherapy in Chinese patients with nonsmall-cell lung cancer: a multicentre randomized controlled trial. Medicine. 2016;95(36):e4557.
Sen F, Tambas M, Ozkaya K, Guveli ME, Ciftci R, Ozkan B, Oral EN, Saip P, Toker A, Demir A, Firat P, Aydiner A, Eralp Y. Concomitant etoposide and cisplatin provided improved survival compared with docetaxel and cisplatin in patients with locally advanced non-small cell lung cancer treated with chemoradiotherapy. Medicine. 2016;95(30):e4280.
Senan S, Brade A, Wang LH, Vansteenkiste J, Dakhil S, Biesma B, Martinez Aguillo M, Aerts J, Govindan R, RubioViqueira B. PROCLAIM: randomized phase III trial of pemetrexed-cisplatin or etoposide-cisplatin plus thoracic radiation therapy followed by consolidation chemotherapy in locally advanced nonsquamous non-small-cell lung cancer. J AmSoc ClinOncol. 2016;34(9):953.
Zhao Q, Wang Z, Huang W, Wang Q, Yu SZ, Zhou T, Han D, Wu ZY, Gong HY, Sun HF, Zhang J, Wei YM, Li HS, Zhang ZC, Lin HQ, Li BS. Phase III study of cisplatin with pemtrexed or vinorelbine plus concurrent late course accelerated hyperfractionated radiotherapy in patients with unresectable stage III non-small cell lung cancer. Oncotarget. 2016;7(7):8422–31.
Yao L, Xu S, Xu J, Yang CY, Wang JF, Sun DW. S-1 plus cisplatin with concurrent radiotherapy versus cisplatin alone with concurrent radiotherapy for stage III non-small cell lung cancer: a pilot randomized controlled trial. Radiat Oncol. 2015;10:1–6.
Liew MS, Sia J, Starmans MH, Tafreshi A, Harris S, Feigen M, White S, Zimet A, Lambin P, Boutros PC, Mitchell P, John T. Comparison of toxicity and outcomes of concurrent radiotherapy with carboplatin/paclitaxel or cisplatin/etoposide in stage III non-small cell lung cancer. Cancer Med. 2013;2(6):916–24.
Sugawara S, Maemondo M, Tachihara M, Tafreshi A, Harris S, Feigen M, White S, Zimet A, Lambin P, Boutros PC, Mitchell P, John T. Randomized phase II trial of uracil/tegafur and cisplatin versus vinorelbine and cisplatin with concurrent thoracic radiotherapy for locally advanced unresectable stage III non-small-cell lung cancer: NJLCG 0601. Lung Cancer. 2013;81(1):91–6.
Atagi S, Kawahara M, Yokoyama A, Okamoto H, Yamamoto N, Ohe Y, Sawa T, Ishikura S, Shibata T, Fukuda H, Saijo N, Tamura T. Thoracic radiotherapy with or without daily low-dose carboplatin in elderly patients with non-small-cell lung cancer: a randomised, controlled, phase 3 trial by the Japan Clinical Oncology Group (JCOG0301). Lancet Oncology. 2012;13(7):671.
Wang LH, Wu SX, Ou GF, Bi N, Li WF, Ren H, Cao JZ, Liang J, Li JL, Zhou ZM, Lv JM, Zhang XR. Randomized phase II study of concurrent cisplatin/etoposide or paclitaxel/carboplatin and thoracic radiotherapy in patients with stage III non-small cell lung cancer. Lung Cancer. 2012;77(1):89–96.
Heinzerling Jh, Choy H, Hughes RS, Bradley JD, Schwartzberg LS, Peng GB, Treat TO. Toxicity and response of pemetrexed plus carboplatin or cisplatin with concurrent chest radiation therapy for patients with locally advanced non-small cell lung cancer: a phase I trial. J Thorac Oncol. 2010;5(9):1391–6.
Segawa Y, Kiura K, Takigawa N, Kamei H, Tanimoto M. Phase III Trial Comparing Docetaxel and Cisplatin Combination Chemotherapy With Mitomycin, Vindesine, and Cisplatin Combination Chemotherapy With Concurrent Thoracic Radiotherapy in Locally Advanced Non–Small-Cell Lung Cancer: OLCSG 0007. J Am Soc Clin Oncol. 2010;28(20):3299–306.
Yamamoto N, Nakagawa K, Nishimura Y, Tsujino K, Satouchi M, Kudo S, Hida T, Kawahara M, Takeda KJ, Katakami N. Phase III study comparing second- and third-generation regimens with concurrent thoracic radiotherapy in patients with unresectable stage III non-small-cell lung cancer: West Japan Thoracic Oncology Group WJTOG0105. J Am Soc Clin Oncol. 2010;28(23):3739.
Atagi S, Kawahara M, Tamura T, Noda K, Watanabe K, Yokoyama A, Sugiura T, Senba H, Ishikura S, Ikeda H, Ishizuka N, Saijo N. Standard Thoracic Radiotherapy With or Without Concurrent Daily Low-dose Carboplatin in Elderly Patients with Locally Advanced Non-small Cell Lung Cancer: a Phase III Trial of the Japan Clinical Oncology Group (JCOG9812). Jpn J Clin Oncol. 2005;35(4):195.
Cakir S, Egehan I. A randomised clinical trial of radiotherapy plus cisplatin versus radiotherapy alone in stage III non-small cell lung cancer. Lung Cancer. 2004;43(3):309–16.
Sarihan S, Kayisogullari U, Ercan I, Engin K. Randomized phase 2 study of radiotherapy alone versus radiotherapy with paclitaxel in non-small cell lung cancer. J Int Med Res. 2004;32(4):375–83.
Komaki R, Lee JS, Kaplan B, Allen P, Kelly JF, Liao Z, Stevens CW, Fossella FV, Zinner R, Papadimitrakopoulou V, Khuri F, Glisson B, Pisters K, Kurie J, Herbst R, Milas L, Ro J, Thames HD, Hong WK, Cox JD. Randomized phase III study of chemoradiation with or without amifostine for patients with favorable performance status inoperable stage II-III non-small cell lung cancer: preliminary results. Semin Radiat Oncol. 2002;12(1):46–9.
Ball D, Bishop J, Smith J, Brien PO, Davis S, Ryan G, Olver I, Toner G, Walker Q, Joseph D. A randomised phase III study of accelerated or standard fraction radiotherapy with or without concurrent carboplatin in inoperable non-small cell lung cancer: final report of an Australian multi-centre trial. J Eur Soc Ther Radiol Oncol. 1999;52(2):129–36.
Ball D, Smith J, Bishop J, Olver I, Davis S, Brien P, Bernshaw D, Ryan G, Millward M. A phase III study of radiotherapy with or without continuous-infusion fluorouracil as palliation for non-small-cell lung cancer. Br J Cancer. 1997;75(5):690–7.
Jeremic B, Shibamoto Y, Acimovic L, Milisavljevic S. Hyperfractionated radiation therapy with or without concurrent low-dose daily carboplatin/etoposide for stage III non-small-cell lung cancer: a randomized study. J Am Soc Clin Oncol. 1996;14(4):1065–70.
Trovó MG, Minatel E, Franchin G, Boccieri MG, Gobitti C. Radiotherapy versus radiotherapy enhanced by cisplatin in stage III non-small cell lung cancer. Int J Radiat Oncol Biol Phys. 1992;24(3):573–4.
Perego P, Robert J. Oxaliplatin in the era of personalized medicine: from mechanistic studies to clinical efficacy. Cancer Chemother Pharmacol. 2015;77(1):5–18.
Dowdy SC, Boardman CH, Wilson TO, Podratz KC, Hartmann LC, Long HG. Multimodal therapy including neoadjuvant methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) for stage IIB to IV cervical cancer. Am J Obstet Gynecol. 2002;186(6):1167–73.
Schultz RM, Patel VF, Worzalla JF, Shih C. Role of thymidylate synthase in the antitumor activity of the multitargeted antifolate, LY231514. Anticancer Res. 1999;19(1A):437.
Shih C, Habeck LL, Mendelsohn LG, Chen VJ, Schultz RM. Multiple folate enzyme inhibition: mechanism of a novel pyrrolopyrimidine-based antifolate LY231514 (MTA). Adv Enzyme Regul. 1998;38(1):135–52.
Hanna N, Shepherd FA, Fossella FV, Pereira JR, De Marinis F, von Pawel J, Gatzemeier U, Tsao TC, Pless M, Muller T, Lim HL, Desch C, Szondy K, Gervais R. Shaharyar, Manegold C, Paul S, Paoletti P, Einhorn L, Bunn PA Jr: Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol. 2004;22(9):1589–97.
Mornex F, Peignaux K, Germain T, Pereira JR, Bunn PA. Phase I study of pemetrexed and cisplatin with concurrent high-dose thoracic radiation after induction chemotherapy in patients with unresectable locally advanced non-small cell lung cancer. Lung Cancer. 2013;80(1):68.
Gadgeel SM, Ruckdeschel JC, Patel BB, Wozniak A, Turrisi A. Phase II study of pemetrexed and cisplatin, with chest radiotherapy followed by docetaxel in patients with stage III non-small cell lung cancer. J Thorac Oncol. 2011;6(5):927.
Choy H, Schwartzberg LS, Dakhil SR, Garon EB, Gerber DE, Choksi JK, Govindan R, Peng GB, Koustenis A, Treat J, Obasaju C. Phase 2 study of pemetrexed plus carboplatin, or pemetrexed plus cisplatin with concurrent radiation therapy followed by pemetrexed consolidation in patients with favorable-prognosis inoperable stage IIIA/B non-small-cell lung cancer. J Thorac Oncol. 2013;8(10):1308.
Pfister DG, Johnson DH, Azzoli CG, Sause W, Smith TJ, Baker SJ, Olak J, Stover D, Strawn JR, Turrisi AT. American society of clinical oncology treatment of unresectable non-small-cell lung cancer guideline: update 2003. J Evid Base Med. 2004;22(2):330–53.
Belani CP, Choy H, Bonomi P, Scott C, Travis P, Haluschak J, Curran WJ. Combined chemoradiotherapy regimens of paclitaxel and carboplatin for locally advanced non-small-cell lung cancer: a randomized phase II locally advanced multi-modality protocol. J Am Soc Clin Oncol. 2005;23(25):5883–91.
Yamaguchi M, Seto T, Furuya A, Edagawa M, Shimamatsu S, Toyozawa R, Toyokawa G, Nosaki K, Hirai F, Takenoyama M, Ichinose Y. Feasibility of the administration of chemotherapy using cisplatin plus etoposide for non-small cell lung cancer patients with interstitial lung disease on chest computed tomography. Cancer Treat Res Commun. 2016;10:6–11.
Kumar R, Collins D, Dolly S, McDonald F, O’Brien MER, Yap TA. Targeting the PD-1/PD-L1 axis in non–small cell lung cancer. Curr Probl Cancer. 2017;41:111–24.
Shaverdian N, Lisberg AE, Bornazyan K, Veruttipong D, Goldman JW, Formenti SC, Garon EB, Lee P. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 phase 1 trial. Lancet Oncol. 2017;18(7):895–903.
Theelen W, Lalezari F, Michel V, Baas P, Peulen H. PUB013 randomized phase ii study of pembrolizumab after SBRT versus pembrolizumab alone in patients with advanced NSCLC, preliminary results. J Thorac Oncol. 2017;12(1):S1453.
Peters S, Felip E, Dafni U, Tufman A, Guckenberger M, Álvarez R, Nadal E, Becker A, Vees H, Pless M, Martinez-Marti A, Lambrecht M, Andratschke N, Tsourti Z, Piguet AC, Roschitzki-Voser H, Gasca-Ruchti A, Vansteenkiste J, Stahel RA, De Ruysscher D. Progression-free and overall survival for concurrent nivolumab with standard concurrent chemoradiotherapy in locally advanced stage IIIA-B NSCLC: results from the european thoracic oncology platform NICOLAS Phase II Trial (European Thoracic Oncology Platform 6–14). J Thorac Oncol. 2021;16(2):278–88.
Acknowledgements
Not applicable.
Funding
There is no funding in this study.
Author information
Authors and Affiliations
Contributions
Research design: ZQQ. Systematic search and study selection: ZQQ and MSH. Data analysis and interpretation: ZQQ. Initial manuscript writing: ZQQ. Manuscript revision: ZQQ, MSH and ZYF. Final approval of manuscript: ZQQ, MSH and ZYF. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable (systematic review and meta-analysis of existing data).
Consent for publication
Not applicable.
Competing interests
None of the authors have potential competing interests with this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, Q., Min, S. & Zhou, Y. A network meta-analysis for efficacies and toxicities of different concurrent chemoradiotherapy regimens in the treatment of locally advanced non-small cell lung cancer. BMC Cancer 22, 674 (2022). https://doi.org/10.1186/s12885-022-09717-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09717-8