
Abstract
Background
Sonic Hedgehog (SHH) pathway dysregulation is implicated in basal cell carcinoma (BCC) development. To evaluate the possible wider role of SHH gene variants in skin carcinogenesis, we assessed associations of genes in the SHH pathway with lifetime development of any keratinocyte cancer (KC), and with developing either BCCs or squamous cell carcinomas (SCCs) exclusively, in a 25-year prospective, population-based study of 1,621 Australians.
Methods
We genotyped 795 unrelated adults with available blood samples: 311 cases with any KC (186 developing BCCs-only, 55 SCCs-only, 70 BCCs and SCCs) and 484 controls. We compared allele frequencies of 158 independent SNPs across 43 SHH genes between cases and controls, and performed a gene-based analysis.
Results
We found associations between SNP rs4848627 (GLI2) (related to DNA synthesis in keratinocytes) and development of any KC (OR = 1.53; 95% CI = 1.06–2.13, P < 0.01) and SCCs exclusively (OR = 2.12; 95%CI = 1.39–3.23, P < 0.01). SNP rs3217882 located in CCND2 was associated with exclusive BCC development (OR = 1.43, CI = 1.12–1.82, P < 0.01). The gene-based analysis suggested an association of PRKACG (protein kinase cAMP-activated catalytic subunit gamma) with any KC (P = 0.013).
Conclusion
We conclude that variants located in genes in the SHH pathway may are involved in SCC as well as BCC development.
Similar content being viewed by others


Introduction
Keratinocyte cancers (KCs), comprising basal cell carcinomas (BCCs) and cutaneous squamous cell carcinomas (SCCs), are the most common cancers in fair-skinned people worldwide [1, 2]. The highest incidence rates of KCs are seen in white populations living in countries like New Zealand and Australia with high levels of solar ultraviolet (UV) radiation [3, 4]. Well-established risk factors associated with these skin cancers are light skin pigmentation, high sun exposure, and genetic factors [2, 5, 6]. Evidence from twin studies suggests the contribution from genetic inheritance is substantial [7].
In humans, the Sonic Hedgehog (SHH) signal transduction pathway is essential for embryonic development [8]. In skin, dysregulation of this signal transduction pathway is strongly implicated in the development of BCCs [9], and some laboratory evidence also suggests involvement with SCC development [10]. Specifically the SHH pathway is involved in cell cycle regulation, and an activated SHH pathway in adulthood results in stimulated cell growth and proliferation [11] associated consistently with sporadic BCCs [9]. Dysregulation of SHH-associated genes Patched 1 (PTCH1) and smoothened (SMO) has been observed in skin cancer and other malignant conditions [12]. Normally, the PTCH1 gene serves as a negative regulator that controls the SMO gene by inhibition, which in turn binds to the glioma-associated oncogene (GLI), a transcription factor regulating apoptosis and angiogenesis [13]. However, details of the mechanisms by which the SHH pathway affects keratinocyte tumorigenesis remain to be elucidated. We therefore evaluated whether genes involved in the SHH pathway are associated with the development of BCCs exclusively, SCCs exclusively, and overall KC, in a 25-year prospective population-based study of skin cancer in Australian adults, using well-characterized phenotypes [14, 15].
Materials and methods
Study design
The Nambour Skin Cancer Study was a prospective cohort study of 2095 randomly selected residents of the Nambour township in subtropical Australia. The study was initiated in 1986 with skin examinations of all participants by dermatologists [16]. Skin cancers occurring 1987–1992 were collected prospectively by postal surveys and confirmed against medical records [17]. From 1992 to 1996, 1621 of the original 2095 participants took part in a randomized trial of daily sunscreen application and beta-carotene supplementation for skin cancer prevention [16, 18, 19]. All participants underwent an interview at trial baseline in which detailed dietary, medical, and occupational histories were recorded, and blood was collected at the end of the trial in 1996.
Dermatologists carried out full-body skin examinations of Nambour Study participants in 1992, 1994, 1996, and 2007. Clinically diagnosed skin cancers were confirmed histologically and skin cancers between clinical surveys were ascertained by linkage with the databases of local pathology laboratories [16, 20]. Therefore we had complete records of all histologically confirmed BCCs and SCCs of Nambour Skin Cancer Study participants from 1986–2007, and were able to distinguish people who in their lifetime to 2007 had exclusively developed BCCs, exclusively developed SCCs, or who had developed both types of KC, and controls who had never developed skin cancer [21]. This study was approved by the Human Research Ethics Committee of the QIMR Berghofer Medical Research Institute and all participants gave written informed consent.
DNA extraction
DNA was extracted from blood samples by the Perkin Elmer Chemagic 360 extraction robot which uses automated magnetic bead technology. Sample quality (A260/280 ratio) and concentration were checked with a BioTek Synergy HT plate reader. A number of 69 samples were extracted previously using the QiAMP blood kit (Qiagen, Inc., Chadstone Centre, VIC, Australia) [15].
Genotyping
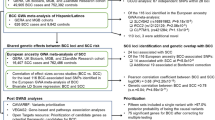
Genotyping was carried out on 863 available blood samples using Illumina Global Screening Array (GSA) chips (model GSAMD-24v1-0–20,011,747; manifest revision A4) by the Human Genomics Facility (HuGeF) at Erasmus Medical Centre, Rotterdam. Genotypes were called using the Genotyping Module in Illumina GenomeStudio by standard procedures, with the following marker (SNP) exclusions: (1) AB R mean (Mean of the normalized R-values for the AB genotypes) < 0.2 (N = 0); (2) AB T mean < 0.2 or > 0.8, and clusters not distinguishable on manual inspection (N = 0); (3) GenTrain score (a measurement of quality of SNP calling) below 0.6 (N = 13,698). Further SNP quality control (QC) resulted in exclusion of further SNPs due to, (4) missingness > 5% (634); (5) Hardy Weinberg equilibrium (HWE) in PLINK 1.90, p-value < 10–6 (N = 20,699); (6) minor allele frequency (MAF) < 1% (N = 152,735); (7) heterozygous for > 1% of males (chromosome X, N = 493); (8) called for > 1% of females (chromosome Y, N = 276). 560 SNPs were also dropped due to duplication or failure to align uniquely, or at all, to the hg19 reference genome in the BLAST searches (URL https://www.well.ox.ac.uk/~wrayner/strand/). This resulted in retention of 500,655 out of the original 692,338 SNPs. Six samples whose genotype call rate was < 97% were dropped, leaving 857 participants after the QC stage. Of the 857 participants, 33 were siblings, and 29 were parent/child pairs. Of the related pairs, we deleted one participant from each pair. If one of the people in the pair had been affected by skin cancer, we retained that person. After removing the participants who were related, 795 remained for further analysis.
SNPs associated with sonic hedgehog pathway
We used the KEGG pathways database [22, 23] to identify SNPs located in the Hedgehog signaling pathway. (Pathway identifier: hsa04340; Supplementary Table 5).
SNPs association analysis
From the 500,655 SNPs resulting from genotyping, we extracted information for all SNPs located in 43 known Hedgehog signaling pathway genes. We selected only independent SNPs by using linkage disequilibrium (LD) pruning (using a 5 SNPs shifting window every 100 SNPs and a 0.2 LD threshold; we further excluded SNPs with minor allele frequency (MAF) < 5%).
We analysed three different histologically-confirmed case groups: (1) participants who had only BCCs (had never developed SCC); (2) those with a history of SCCs only (no ss); and (3) a combination of groups 1 and 2 plus those who with a history of both BCCs and SCCs (group 3 is henceforth referred to as “any KC” phenotype). Each of the three case groups was compared to the controls who had never developed BCCs or SCCs. We tested associations between extracted SNPs in the SHH pathway with BCCs, SCCs and KCs using a χ2 test to compare allele frequencies between cases and controls using PLINK v1.90 [24]. Bonferroni correction (0.05/158) was applied to account for the multiple comparisons. However, since this method might impose an unnecessary high penalty in association studies in particular those with a relatively small sample size like ours [25], we also calculated empirical p-values using a label-swapping permutation test implemented in PLINK with the –perm command [24]. Using the empirical p-values we considered a SNP associated with an outcome when p < 0.05.
Gene-based analysis
Gene-based analysis was performed in MAGMA (Multi-marker analysis for genomic annotation) [26]. MAGMA uses SNP p-values to calculate a gene test-statistic as the mean of the χ2 statistics for all SNPs between the start and stop sites of a gene, correcting for gene size, number of SNPs in a gene, and LD [26]. We used the 1000 Genomes Build 37 reference data for gene annotation, and a 5 kb window to include neighbouring SNPs around each gene with potential regulatory roles in transcription.
Sensitivity analysis
In the control group there were 56 participants whose skin cancer history prior to 1986 was uncertain (11 did not answer a question in the 1986 survey about whether they had a past skin cancer treated by a doctor; two persons were unsure whether they had a prior skin cancer; and 43 answered that they had had a skin cancer in the past but that this was not histologically confirmed). To evaluate potential misclassification of controls, we performed a sensitivity analysis by repeating the analyses without these 56 participants.
Results
Characteristics of the study population
We included 186 persons who developed BCCs exclusively, 55 who developed SCCs exclusively, and 70 persons who developed both BCCs and SCCs during the study period, as well as 484 controls who had not developed keratinocyte cancers. A total of 427 BCC lesions were diagnosed in the 186 participants with BCCs exclusively during the 1986–2007 study period. Of these, 22% (n = 92) were classified as aggressive BCC subtypes (namely: morphoeic, infiltrative, micronodular, basosquamous), 57% (n = 244) as non-aggressive subtypes (nodular, superficial), while for 21% (n = 91), subtypes were not available. All SCCs in study participants were localized invasive SCCs. Among the cases, 126 (41%) were aged ≥ 60 years, 147 (47%) were male, 162 (52%) had fair skin, and the majority of all study participants claimed predominantly European ancestry (99.5%) (Supplementary Table 1). The age distribution was significantly different between cases and controls (p < 0.05), with most cases (64%) aged 50 to 70 years and most controls (63%) aged 20 to 49 years. Our case group also included a higher number of individuals with fair skin colour (52% vs 40%) that were more likely to report that they “always burn” after exposure to acute sun (30% vs 15%), and more likely to have clinical elastosis of the neck (41% vs 26%) compared to controls.
SNP association analysis
A total of 773 SNPs from the original extraction of the KEGG database were located across 43 genes in the SHH pathway. After excluding SNPs with MAF < 5% (n = 374), those in high LD (n = 234), and those in Hardy–Weinberg disequilibrium (n = 7), there were 158 remaining SNPs of interest distributed across the 43 genes (Supplementary Tables 2, 3 and 4).
Among the top 10 associated SNPs, rs4848627 in GLI2 was found to be associated with development of any KC (OR = 1.53; 95%CI = 1.06–2.13, P = 4.2 × 10–4) and with development of SCCs exclusively (OR = 2.12; 95%CI = 1.39–3.23, P = 3.0 × 10–4) (Table 1).The GLI2 SNP rs4848627 was also in the top SNPs associated with exclusive development of BCCs (OR = 1.38; 95%CI = 1.04–1.83, P = 0.021). Still other GLI2 variants, rs895485 in intron 2 and rs17050378 in intron 1 were present among the top 10 associated SNPs for SCCs-only (P = 0.014 and 0.021, respectively; Table 1).
In addition, we found an association with rs3217882, located in an intron of cyclin D2 (CCND2), which was associated with an increased risk of exclusive BCC development (OR 1.43; 95%CI 1.12–1.82, P = 0.004) and SNP rs970318 in PRKACB associated with exclusive BCC diagnosis (OR 0.72; 95% CI 0.56–0.92, P = 0.009).
SNP rs2849380 located in BCL2 was the second most strongly associated SNP among exclusive SCC cases (OR = 1.85; 95%CI 1.19–2.87, P = 0.0075). Sensitivity analysis in which we excluded the 56 participants who potentially could have been misclassified as controls, showed very similar results (data not shown).
Gene-based analysis
None of the top three genes associated with development of any KC, or exclusive development of either BCCs or SCCs respectively, reached statistical significance in our analysis (Table 2). PRKACG (protein kinase cAMP-activated catalytic subunit gamma) showed the strongest association among KC cases (P = 0.013; Z-score = 2.2) and was also the third strongest association in participants with exclusive BCC development (P = 0.012; Z-score = 1.7). The Sonic Hedgehog signaling molecule (SHH) was the top gene associated with BCCs-only cases (P = 0.005; Z-score 2.5). Kinesin family member 7 (KIF7) was the gene most strongly associated with SCCs-only cases (P = 0.008; Z-score 0.008).
Discussion
We have previously shown that people living in Queensland with high UV exposure who develop multiple skin cancers over time are more likely to develop the same type of KC exclusively (BCCs-only or SCCs-only), than a mix of BCCs and SCCs tumors [21], suggesting a genetic component in the aetiology of much KC development. While many skin cancer genes are associated with both BCCs and SCCs, there are genes which are involved with either BCC or SCC development exclusively [27], yet to our knowledge, there are no prior human studies which have evaluated if genes involved in the SHH pathway affect the risk of development of BCCs alone or SCCs alone. In our study, GLI2 was the gene that contained the most SNPs statistically significantly associated with any KC, as well as with exclusive development of BCCs or SCCs. The SNP with the strongest association with KC was rs4848627 in GLI2 (1.5 times increased risk for any KC), and it was the top SNP for people who developed SCCs exclusively with a doubling of risk. This SNP was also found in the top 10 list of SNPs associated with exclusive development of BCCs.
GLI2 plays an important role in regeneration and survival of keratinocytes, and the expression of GLI2 together with GLI1 are part of a positive feedback mechanism in BCC that leads to an increase in DNA-synthesis in confluent human keratinocytes [28]. Overexpression of GLI2 supports epidermal regeneration in organotypic cell cultures, which over time lead to manifestation of undifferentiated basal cell-associated keratinocytes [29]. It has also been shown that GLI transcription factors can facilitate keratinocyte survival and transformation upon exposure to genotoxic agents. Because GLI1 and GLI2 facilitate the propagation of cells with damaged DNA, their expression may be naturally higher in cells that form the earliest precursor tumor lesions [30]. Transgenic mice overexpressing GLI2 develop multiple BCCs and GLI2 is required to maintain tumor growth [31]. While most of this evidence suggests a role of GLI1 and GLI2 expression in maintenance of keratinocyte integrity and avoidance of BCC formation, our genetic analyses particularly suggested associations with SCCs-only development which has not been explored before, as well as their relevance to BCC.
We further found that SNP rs3217882 in cyclin D2 (CCND2) was associated with a 1.4 times increased risk of exclusive BCCs. CCND2 forms a complex which regulates the activity of cell cycle G1/S transition [32], which may partly explain why we found this SNP to be also associated with the overall KC group (1.3 times increased risk). There are no previous publications describing the association of KCs with this SNP.
Protein kinase cAMP-activated catalytic subunit gamma (PRKACG) was the gene with the second strongest association with KC overall, and it was also found in the top three gene list among people with exclusive. This gene has been linked to the bleeding disorder platelet-type 19 (BDPLT19) caused by platelet dysfunction [33]. Again there are no previous publications on skin cancer and PRKACG association, and repeated analyses in a larger cohort would be needed to confirm this possible association between the PRKACG gene and skin cancer.
The sonic hedgehog signaling molecule (SHH gene) was found to be associated with exclusive development of BCC. Defects in the SHH gene are otherwise known to cause a disorder characterised by facial deformities and problems with forebrain development in embryos [34]. Meanwhile, we found that kinesin family member 7 (KIF7) was the gene with the strongest association for exclusive development of SCCs. KIF7 is an important gene in the SHH pathway, and acts as a negative regulator by preventing activation of GLI2 in the absence of a ligand, and as a positive regulator by preventing the processing of GLI3 into its repressor form. It is also involved in the regulation of epidermal differentiation [35] which is altered in skin cancer development [36].
A main strength of these genetic analyses was that they were based within the Nambour Skin Cancer Study population who have excellent phenotypic characterisation through prospective long-term (1992–2007) follow-up and histological confirmation of all skin cancers, which is not the case for most previous such studies where skin cancer phenotypes have not been routinely confirmed by histopathology. Thus we are uniquely positioned to analyse genetic associations in relation to the characterisation of participants’ long-term propensity to develop either BCCs or SCCs exclusively, as well as any KC, and this is the first study to do this for genes in the SHH pathway. Our study cohort consisted of an ethnically homogenous population (mostly European ancestry), which minimises the chance of false positive associations due to population substructure. The major limitation of this study was the relatively small sample size resulting in a lack of statistical power, and hence we have focussed on the interpretation of top SNP and gene hits only, and have explored potential underlying mechanisms relevant to BCC and SCC development.
Conclusion and implications
Our study focussed on SNP and gene-associations of the SHH pathway in people who develop KC, including a novel long-term characterisation of propensity to develop BCCs or SCCs exclusively. We found GLI2 to be significantly associated with exclusive SCC development as well as development of KC overall. Further, we identified associations of other SNPs and genes in the SHH pathway, warranting larger longitudinal studies to replicate and build on these findings.
Availability of data and materials
All data generated or analysed during this study are available at the Queensland University of Technology (QUT) repository, https://doi.org/10.25912/RDF_1646199819849.
Abbreviations
- BCC:
-
Basal cell carcinoma
- HWE:
-
Hardy Weinberg Equilibrium
- KC:
-
Keratinocyte cancer
- MAF:
-
Minor allele frequency
- LD:
-
Linkage disequilibrium
- QC:
-
Quality control
- SCC:
-
Cutaneous squamous cell carcinoma
- SHH:
-
Sonic Hedgehog
- SNP:
-
Single nucleotide polymorphism
- UV:
-
Ultraviolet radiation
References
Pandeya N, Olsen CM, Whiteman DC. The incidence and multiplicity rates of keratinocyte cancers in Australia. Med J Aust. 2017;207(8):339–43.
Leiter U, Keim U, Garbe C. Epidemiology of skin cancer: update 2019. Adv Exp Med Biol. 2020;1268:123–39.
Scherer D, Kumar R. Genetics of pigmentation in skin cancer–a review. Mutat Res. 2010;705(2):141–53.
Apalla Z, et al. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7(2):1–6.
Fransen M, et al. Non-melanoma skin cancer in Australia. Med J Aust. 2012;197(10):565–8.
Madan V, et al. Genetics and risk factors for basal cell carcinoma. Br J Dermatol. 2006;154(Suppl 1):5–7.
Mucci LA, et al. Familial risk and heritability of cancer among twins in Nordic countries. JAMA. 2016;315(1):68–76.
Araújo GLL, et al. Sonic hedgehog signaling regulates mode of cell division of early cerebral cortex progenitors and increases astrogliogenesis. Front Cell Neurosci. 2014;8:77–77.
Pellegrini C, Maturo MG, Di Nardo L, Ciciarelli V, Gutiérrez García-Rodrigo C, Fargnoli MC. Understanding the Molecular Genetics of Basal Cell Carcinoma. Int J Mol Sci. 2017;18(11):2485. https://doi.org/10.3390/ijms18112485.
Sun Q, Bai J, Lv R. Hedgehog/Gli1 signal pathway facilitates proliferation, invasion, and migration of cutaneous SCC through regulating VEGF. Tumour Biol. 2016.
Iwasaki JK, et al. The molecular genetics underlying basal cell carcinoma pathogenesis and links to targeted therapeutics. J Am Acad Dermatol. 2012;66(5):e167–78.
Li C, Chi S, Xie J. Hedgehog signaling in skin cancers. Cellular signaling. 2011;23(8):1235–43.
Rohatgi R, Milenkovic L, Scott MP. Patched1 regulates hedgehog signaling at the primary cilium. Science. 2007;317(5836):372–6.
Hughes MCB et al. Dietary antioxidant capacity and skin photoaging: A 15-year longitudinal study. J Invest Dermatol. 2020;(37):16215–25.
Von Schuckmann LA, et al. Vitamin D pathway gene polymorphisms and keratinocyte cancers: a nested case-control study and meta-analysis. Anticancer Res. 2016;36(5):2145–52.
Green A, et al. Daily sunscreen application and betacarotene supplementation in prevention of basal-cell and squamous-cell carcinomas of the skin: a randomised controlled trial. Lancet. 1999;354(9180):723–9.
Green A, Battistutta D. Incidence and determinants of skin cancer in a high-risk Australian population. Int J Cancer. 1990;46(3):356–61.
Green AC, et al. Reduced melanoma after regular sunscreen use: randomized trial follow-up. J Clin Oncol. 2011;29(3):257–63.
Darlington S, et al. A randomized controlled trial to assess sunscreen application and beta carotene supplementation in the prevention of solar keratoses. Arch Dermatol. 2003;139(4):451–5.
Hughes MC, et al. Comparison of histological measures of skin photoaging. Dermatology. 2011;223(2):140–51.
Keim U, et al. Exclusive development of a single type of keratinocyte skin cancer: evidence from an Australian population-based cohort study. J Invest Dermatol. 2015;135(3):728–33.
Kanehisa M, et al. New approach for understanding genome variations in KEGG. Nucleic Acids Res. 2019;47(D1):D590–5.
Kanehisa M, Goto S. KEGG: kyoto encyclopedia of genes and genomes. Nucleic Acids Res. 2000;28(1):27–30.
Purcell S, et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. 2007;81(3):559–75.
Perneger TV. What’s wrong with bonferroni adjustments. BMJ. 1998;316(7139):1236–8.
de Leeuw CA, et al. MAGMA: generalized gene-set analysis of GWAS data. PLoS Comput Biol. 2015;11(4):e1004219.
Liyanage UE, et al. Combined analysis of keratinocyte cancers identifies novel genome-wide loci. Hum Mol Genet. 2019;28(18):3148–60.
Regl G, et al. Human GLI2 and GLI1 are part of a positive feedback mechanism in basal cell carcinoma. Oncogene. 2002;21(36):5529–39.
Pantazi E, et al. GLI2 is a regulator of beta-Catenin and is associated with loss of E-Cadherin, cell invasiveness, and long-term epidermal regeneration. J Invest Dermatol. 2017;137(8):1719–30.
Harrison W, et al. The oncogenic GLI transcription factors facilitate keratinocyte survival and transformation upon exposure to genotoxic agents. Oncogene. 2014;33(19):2432–40.
Grachtchouk M, et al. Basal cell carcinomas in mice overexpressing Gli2 in skin. Nat Genet. 2000;24(3):216–7.
Neganova I, et al. Expression and functional analysis of G1 to S regulatory components reveals an important role for CDK2 in cell cycle regulation in human embryonic stem cells. Oncogene. 2009;28(1):20–30.
Manchev VT, et al. A new form of macrothrombocytopenia induced by a germ-line mutation in the PRKACG gene. Blood. 2014;124(16):2554–63.
Dubourg C, et al. Holoprosencephaly. Orphanet J Rare Dis. 2007;2:8.
Li ZJ, et al. Kif7 regulates Gli2 through Sufu-dependent and -independent functions during skin development and tumorigenesis. Development. 2012;139(22):4152–61.
Panelos J, Massi D. Emerging role of Notch signaling in epidermal differentiation and skin cancer. Cancer Biol Ther. 2009;8(21):1986–93.
Acknowledgements
We would like to thank all participants of the Nambour Skin Cancer Study. We thank Prof Lyn Griffiths, Ms Rebecca Grealy, and Griffith University for their invaluable contributions to the Nambour Skin Cancer Study DNA resource, including sharing sample processing and storage.
Funding
This work was supported by a Program Grant (1073898) from the National Health and Medical Research Council of Australia (NHMRC). The funding body played no role in the design or conduct of the study. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the funding body.
Author information
Authors and Affiliations
Contributions
AR contributed to the conception, design, analysis, data interpretation and drafting of the manuscript. AA contributed to the conception, design and drafting of the manuscript. UL drafted and revised the manuscript. SG performed the quality control of the genetic data used in this study. JV contributed to the study design and revision and AG supervised and contributed to the conception, design, and revision of the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with the Declaration of Helsinki. This study was approved by the Human Research Ethics Committee of the QIMR Berghofer Medical Research Institute (P327). All participants gave written informed consent.
Consent for publication
Not Applicable.
Competing interests
Nothing to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary Table 1. General characteristics of controls and cases (total, BCC only, SCC only, and BCC and SCC). Supplementary Table 2. Association of gene variants in the SHH pathway with KC. We tested the association of 158 SNPs distributed across 43 genes involved in the SHH pathway with KC (BCC, SCC, BCC, and SCC). SNPs are presented in ascending order by p-value. Information on the chromosome location (CHR), SNP name (SNP), base pair position along the chromosome (BP), the allele with the minor allele frequency (A1), allele 2 (A2), A1 frequency in cases (F_cases), and controls (F_controls), Chi-square value (CHISQ), p-value (P) and odds ratio (OR) are presented. Supplementary Table 3. Association of gene variants in the SHH pathway with BCC. We tested the association of 158 SNPs distributed across 43 genes involved in the SHH pathway with BCC. SNPs are presented in ascending order by p-value. Information on the chromosome location (CHR), SNP name (SNP), base pair position along the chromosome (BP), the allele with the minor allele frequency (A1), allele 2 (A2), A1 frequency in cases (F_cases) and controls (F_controls), Chi-square value (CHISQ), p-value (P) and odds ratio (OR) are presented. Supplementary Table 4. Association of gene variants in the SHH pathway with SCC. We tested the association of 158 SNPs distributed across 43 genes involved in the SHH pathway with SCC. SNPs are presented in ascending order by p-value. Information on the chromosome location (CHR), SNP name (SNP), base pair position along the chromosome (BP), the allele with the minor allele frequency (A1), allele 2 (A2), A1 frequency in cases (F_cases) and controls (F_controls), Chi-square value (CHISQ), p-value (P) and odds ratio (OR) are presented. Supplementary Table 5. Sonic Hedgehog pathway genes.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rodriguez-Acevedo, A.J., Antonsson, A., Liyanage, U.E. et al. Associations of keratinocyte cancers with snp variants in the sonic hedgehog pathway. BMC Cancer 22, 490 (2022). https://doi.org/10.1186/s12885-022-09565-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09565-6