
Abstract
Background
AURA study reported 61% objective response rate and progression-free survival of 9.6 months with osimertinib in patients with EGFR/T790M+ non-small cell lung cancer. Due to lack of real-world data, we proposed this study to describe the experience with osimertinib in Spain.
Methods
Post-authorization, non-interventional Special Use Medication Program, multicenter, retrospective study in advanced EGFR/T790M+ non-small cell lung cancer. One hundred-fifty five patients were enrolled (August 2016–December 2018) from 30 sites. Primary objective: progression-free survival. Secondary objectives: toxicity profile, objective response rate, and use of health service resources.
Results
70% women, median age 66. 63.9% were non-smokers and 99% had adenocarcinoma. Most patients had received at least one prior treatment (97%), 91.7% had received previous EGFR-tyrosine kinase inhibitors and 2.8% osimertinib as first-line treatment. At data cutoff, median follow-up was 11.8 months. One hundred-fifty five patients were evaluable for response, 1.3% complete response, 40.6% partial response, 31% stable disease and 11.6% disease progression. Objective response rate was 42%. Median progression-free survival was 9.4 months. Of the 155 patients who received treatment, 76 (49%) did not reported any adverse event, 51% presented some adverse event, most of which were grade 1 or 2. The resource cost study indicates early use is warranted.
Conclusion
This study to assess the real-world clinical impact of osimertinib showed high drug activity in pretreated advanced EGFR/T790M+ non-small cell lung cancer, with manageable adverse events.
Trial registration
Clinical trial registration number: NCT03790397.
Similar content being viewed by others


Background
In Spain occur about 27,351 new lung cancer cases per year and the disease was responsible for 22,896 deaths in 2018 [1, 2]. Most non-small cell lung cancer (NSCLC) patients are diagnosed with unresectable disease and around 40% with advanced disease.
The identification of oncogenic driver alterations that can be targeted by EGFR tyrosine kinase inhibitors (EGFR-TKI: erlotinib, gefitinib, afatinib, dacotinib) for EGFR mutated tumors has improved median progression-free survival (PFS), overall response rates and quality of life in metastatic NSCLC patients, making EGFR TKIs the first-line treatment of choice in patients with EGFR mutation (EGFRm) advanced NSCLC [3]. Unfortunately, however, even these patients eventually develop resistance.
Multiple resistance mechanisms have been observed, including the EGFR Thr790Met (T790M) resistance mutation, MET amplification, HER2 amplification and small-cell histological transformation, among others. EGFR T790M mutations have been detected in 48–62% of patients that develop resistance to EGFR-TKIs [4, 5].
Until recently, treatment options in the post-EGFR-TKI second-line setting were limited, with low rates of response to platinum-based doublet chemotherapies [6,7,8].
Osimertinib (AZD9291) is a potent oral irreversible EGFR-TKI that is selective for both EGFR and T790M resistance mutations with activity in the central nervous system (CNS) [9, 10]. In the phase 1 component of the phase 1/2 AURA trial (ClinicalTrials.gov number, NCT01802632), objective response rate (ORR) for osimertinib in patients with T790M-positive NSCLC was 61% and median PFS was 9.6 months [11].
The publication of the FLAURA study, which obtained a significantly longer PFS and overall survival (OS) than with standard EGFR-TKI in first-line (18.9 months vs. 10.2 months), led to the approval of osimertinib for standard first-line treatment.
Osimertinib has been approved in Europe and commercialized in Spain for the treatment of patients with EGFR T790M-positive (EGFR/T790M+) advanced NSCLC and in first line regardless the T790M mutation status.
Then, just after the ASTRIS study had closed recruitment [12], the Foreign Medication Program was opened. This is a Special Use Medication Program (SUMP) from the Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) to access osimertinib in Spain for the patient population without other treatment options for pretreated patients with EGFR/T790M+ advanced NSCLC.
Based on the lack of real-world results in this setting, and the experience with osimertinib in Spain since 2015, we proposed a retrospective study to describe the experience in terms of efficacy and safety in EGFR/T790M+ NSCLC.
Methods
Study population
This was a post-authorization-other-designs, non-interventional, multicenter, retrospective study that in no way interfered with physicians’ normal clinical practice. The study is based on collection of data about those patients treated with osimertinib within the SUMP and therefore did not involve any diagnostic or therapeutic procedures beyond normal clinical practice. The results provide some insights into the clinical efficacy of osimertinib treatment and consumption of hospital primary care resources.
Eligible patients had histologically or cytologically confirmed stage IIIb/IV EGFR/T790M+ NSCLC and had received osimertinib treatment within the osimertinib Spanish Special Use Medication Program (SUMP).
Living patients had to have signed and dated an Independent Ethics Committee/Institutional Review Board (IRB/EC)-approved written informed consent form following regulatory and institutional guidelines. This had to be obtained before the performance of any protocol-related procedures that were not part of normal care.
Assessment
The primary objective was to estimate PFS to osimertinib. Secondary objectives were to establish osimertinib toxicity profile, estimate duration of response (DOR), ORR by RECIST v1.1 and report on the consumption of hospital and primary care resources.
All clinical efficacy objectives were to be assessed depending on treatment line (first, second, third or further lines).
Date of progression, type of progression, DOR defined as time from documentation of tumor response until disease progression or death, and ORR by RECIST v1.1 were measured.
Adverse events (AEs) related to osimertinib treatment received within the SUMP in Spain were filed in a Remote Data Capture system (RDC)/Case Report Form (CRF). Type and severity of AEs were classified according to the NCI CTCAE Version 5.0. The causal relationship to the study drug was determined by the physician and should be used to assess all AEs. The casual relationship may be either “related” or “not related”.
Independent ethics committee (IEC) or institutional review board (IRB)
The study was evaluated by the Ethical Committee of Hospital Universitario Puerta de Hierro de Majadahonda, Madrid.
The study was also classified by the Spanish Health Authority as “EPA-OD” (post-authorization study, other designs). The ethical committees of other hospitals also reviewed the study as per local practice. The study was carried out following the Declaration of Helsinki on Good Clinical Practices and Organic Law 3/2018, 5th December on Protection of Personal Data and digital rights that were guaranteed during the study. The study was coordinated and monitored by the Spanish Lung Cancer Group (SLCG) and financed by AstraZeneca following the specifications in the protocol. This funding included the cost of submitting the study for approval to an accredited IEC; submission for classification to the AEMPS; database design, maintenance and management; monitoring activities; statistical analysis and corresponding statistical report.
Data quality assurance
The application used for data collection had safety margins and internal coherence rules to avoid input of incorrect data or anomalous or incoherent values. Data quality and queries were revised and dealt with by the SLCG Data Management Department. All patient information required was included in a Remote Data Capture system (RDC)/Case Report Form (CRF).
Statistical analysis
A total of approximately 156 patients were included from several Spanish sites. The observation period was from August 2016 and December 2018.
The following descriptive statistics were used. Frequency statistics for categorical variables: number and percentage. Mean, standard deviation, median (interquartile range) and categorical distribution for quantitative variables (e.g. number of exacerbations, hospital admissions, emergency unit visits, prescriptions, primary care visits). In addition, two-sided 95% confidence intervals (CI) were presented for the specified study outcomes.
PFS was defined from initiation of osimertinib treatment until radiological and/or clinical progression or death from any cause, whichever occurred first. OS was defined from initiation of osimertinib to death from any cause.
Progression was ideally measured by RECIST v 1.1; patients with unknown progression status at time of data collection were censored at the date they were last known to be free of radiological and/or clinical progression. DOR was defined as time from documentation of tumor response to disease progression or death.
PFS and DOR were estimated using Kaplan–Meier analysis.
ORR, defined as percentage of patients achieving complete or partial response, was evaluated based on RECIST v 1.1 response criteria.
Clinical efficacy variables were assessed for patients (squamous vs non-squamous) depending on whether they received first, second, third or subsequent lines of treatment. Safety of osimertinib administration was described by tabulation of the CTCAE version 5.0. No inferential analyses were foreseen. No interim analyses were predefined. All study results were considered exploratory and descriptive by design. All statistical analyses were performed using R software.
Protocol deviations
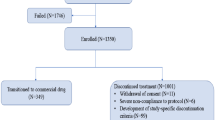
There were no major protocol deviations as this was not a clinical trial and data collection was carried out in a timely manner and according to protocol. One hundred and fifty-six patients were included but only 155 were valid since 1 patient was an inclusion error.
Results
Patient characteristics
One hundred and fifty-five patients who started osimertinib treatment between August 2016 and December 2018 were analyzed. Table 1 shows the main demographic data. One hundred and fifty-five were T790M positive: 70% (109/155) had EGFR deletion in exon 19, 25% (39/155) exon 21, and 5% (7/155) other previous mutation status. Four patients (2.6%) received osimertinib as first line, 83 (53.5%) as second line, 31 (20.0%) as third line and 37 (23.9%) as the fourth of further lines.
Palliative radiotherapy use was also registered. Of the 155 patients included, 73 (47.1%) received radiotherapy treatment during follow up, of whom 60 (38.7%) started radiotherapy before beginning osimertinib treatment, and 13 (8.4%) started radiotherapy after beginning osimertinib treatment.
Regarding chemotherapy, 152 of the 155 patients included (98.1%) received chemotherapy during follow up.
Efficacy results
According to RECIST v 1.1, best response to osimertinib was distributed thus: 2 (1.3%) patients with complete response (CR), 63 (40.6%) with partial response (PR), 48 (31%) with stable disease (SD), 18 (11.6%) with progression and 24 (15.5%) without registered response. Of the 131 patients with registered response to osimertinib treatment, estimated objective response (PR or CR reached) was 42%. Regarding comparison of response rates between treatment lines when osimertinib was administered, no statistically significant differences were observed among the 75 patients who received osimertinib in first or second line with registered response (of the 35 that responded, 46.7%) and the 56 patients who received osimertinib in third or fourth line with registered response (of the 30 that responded, 53.6%) (p-value = 0.482). Table 2 shows the drugs administered as first, second and third lines prior to osimertinib.
Adverse events (AEs)
Table 3 shows a summary of AEs on osimertinib classified according to the CTCAEv5.0. One hundred and fifty-five patients received treatment and were included in the study. Of these, 76 (49.0%) did not show AEs; 29 (18.7%) showed AEs with a maximum grade of 1; 32 (20.6%) showed AEs with a maximum grade of 2; 14 (9%) showed AEs with a maximum grade of 3; 2 (1.3%) with a maximum grade of 4; and 2 (1.3%) with a maximum grade of 5.
Osimertinib dose was adjusted in 26 patients (16%) and was due to toxicity in 18 of these (11.6%). Treatment was discontinued in 4 patients (2.6% of the total treated) due to toxicity.
Follow up and survival
Patients were monitored from the beginning of osimertinib treatment until time of death, loss to follow up or study closure while they were still alive. Median follow up for all patients was 11.7 months (range 0.4–32.0 months), while the median for those patients that were alive was 14.9 months (range 1.8–32.0 months).
Of the 155 patients included, 80 (51.6%) died during follow up. Estimated median OS for these patients was 17.3 months (95% CI, 13.4–21.3 months). Figure 1.

Estimated median OS of patients treated with osimertinib
Overall survival can be compared depending on the line of treatment patients received. Of the 87 patients who received osimertinib as first (4 patients) or second line (83 patients), 46 died during follow up (52.9%). Of the 68 patients that received osimertinib as third (31 patients), forth (22 patients), fifth (11 patients), sixth (2 patients) or seventh line (2 patients), 34 died during follow up (50.0%). No statistically significant differences are observed between the overall survival curves of these two groups of patients (osimertinib as <2nd line versus >3rd line, p-value = 0.392).
Of the 155 patients included, 89 (57.4%) progressed during follow up, 16 (10.3%) died before progression and 50 (32.3%) were still alive without progression at the trial’s closure. Figure 2 shows the estimated median PFS curve for this type of patients, with a median PFS of 9.4 months (95% CI, 7.3–11.6 months).

Estimated median PFS of patients treated with osimertinib
PFS can be compared by treatment line. Of the 87 patients that received osimertinib as first or second line, 61 progressed or died during follow up (70.1%). Of the 68 patients who received osimertinib as third or further line, 44 progressed or died during follow up (64.7%). No statistically significant differences were observed between the PFS curves of both groups of patients (p-value = 0.113).
Follow up of patients with CNS metastases at osimertinib treatment initiation
Presence of CNS metastases was registered at the beginning of osimertinib treatment in 45 patients (29.9%).
Significant differences were observed according to the absence or presence of brain metastases prior osimertinib initiation [10.3 months (95% CI, 7.8–12.8 months) and 7.2 months (95% CI, 3.9–10.6 months), respectively (HR = 1.546 with 95% CI, 1.030–2.321); p-value = 0.034].
No significant differences were observed when comparing OS according to presence or absence of CNS metastases at the initiation of osimertinib treatment (p-value = 0.365). Median OS was 18.3 months (95% CI, 14.9–21.7 months) and 13.8 months (95% CI, 11.0–16.6 months) for those patients without and with brain involvement prior to osimertinib initiation, respectively.
Follow up of patients that received osimertinib as last treatment
Overall survival for the 134 patients that received osimertinib as last treatment (no posterior treatment registered) was compared with that of the 21 patients that received subsequent chemotherapy and no significant differences were observed (p-value = 0.411).
Of the 134 patients, whose last treatment was osimertinib, the end date was not registered for 52 of them, so they continued on treatment at the date of treatment data collection closure (31/12/2018).
Follow up of T790M+ “de novo” patients
Overall survival and PFS of the 10 (8.3%) “T790M+ de novo” patients were analyzed.
The small number of these subgroup of patients does not lend itself to precise estimates, making it difficult to detect potential differences. Estimated median OS for these patients was 14.8 months (95% CI, 3.1–26.5 months), while estimated median PFS was 8.6 months (95% CI, 0.0–18.1 months).
Of the 6 patients included in this group that had received previous treatment, 3 (50%) died during follow up. Estimated median OS for these patients was 15.6 months, while estimated median PFS was 9.4 months.
Health service resources
Data on use of health service resources during treatment with osimertinib (from first dose to last) was collected. It was assumed that all 155 patients had finished treatment with osimertinib, so none were censored.
The use of health service resources is described according to previous characteristics before osimertinib treatment. Table 4 shows the main number of resources used according to different characteristics. A comparison between the values observed using the Mann-Whitney U test is also shown. The results show that stage T3-T4 patients consumed more resources, with a significant difference in R13 (other imaging tests). Similarly, non-smokers and those who had more previous chemotherapy lines also required more resources.
Discussion
Obtaining real-life data is a very important factor in understanding drug efficacy. Typically, clinical trials include a highly selected population that is not always representative of real-world clinical practice. Our study consolidates information about the efficacy of osimertinib in any line of treatment, thus over 40% of our patients received the drug beyond third line, and in 78% of cases patients had some type of comorbidity.
In fact, PFS was 9.4 months (95% CI, 7.5–11.6), which does not show significant differences even in fourth line, according to the literature [13].
It should be remembered that standard treatment with chemotherapy in these patients does not reach more than 5–6 months PFS, at best [14]. Other real-world studies with osimertinib [15] have reached PFS of 10.1 months (95% CI, 9.2–11.0 months), including a recently published pooled analysis [16] with median PFS of 9.9 months (95% CI, 9.5–12.3), very similar to our own.
Similarly, for the other objective measure of efficacy, ORR, significant differences were not observed by treatment line. Our study obtained ORR of 50%, very similar to other retrospective studies [17] and to pivotal studies with osimertinib in these patients, bearing in mind they are mostly Caucasian, and Asian populations have higher response rates and, usually, longer PFS [18].
As well as efficacy, one of the most important factors is the excellent tolerance and minimal side effects with osimertinib. Of 155 patients that received treatment and were included in the study, 76 (49.0%) did not experience AEs. Only 2 (1.3%) had AEs with a maximum grade of 4, 2 patients (1.3%) had AEs with a maximum grade of 5, and discontinuation due to toxicity was just 2.6%, in line with the pivotal clinical trials published.
CNS involvement, both at time of initial diagnosis and at disease progression, is common in these patients [19] and is an indicator of poor prognosis. It should be noted that among patients with brain metastases at the start of osimertinib treatment, the majority had been previously treated (58%) and, despite this, response rate with osimertinib was 40%—rising to almost 70% if we include stabilizations—confirming the drug’s activity in this setting [8]. Notably, all this was achieved outside the framework of a clinical trial in which only asymptomatic patients with stable disease and not requiring steroids were included in the previous 4 weeks [20].
Since the publication of the results of the FLAURA study, which demonstrated clearly improved median PFS in patients treated with osimertinib (18.9 months) versus first-generation TKIs (10.2 months) [21], it seems that the debate about the role of osimertinib now no longer focuses on its activity in second lines, when the patient develops the resistance mutation, but on the treatment sequence.
It is important to note that the greatest use of resources occurs when more lines of treatment have been given prior to osimertinib. Therefore, in addition to the clear benefit of early-line osimertinib, toxicity is reduced and the economic benefit is increased.
Conclusion
Given all of the above, we believe that it is important to report real-world data from patients treated with osimertinib in any line. Our results with 155 patients are similar to those of real-world studies in China with 77 patients [22], Germany with 51 [15], or France with 205 patients [23] and demonstrate that real-world data closely agrees with that obtained in pivotal clinical trials, even without patient selection.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- AEs:
-
Adverse events
- CNS:
-
Central nervous system
- CRF:
-
Case report form
- DOR:
-
Duration of response
- EPA-OD:
-
Post-authorization study, other designs
- IEC:
-
Independent ethics committee
- NSCLC:
-
Non-small cell lung cancer
- ORR:
-
Objective response rate
- OS:
-
Overall survival
- PFS:
-
Progression-free survival
- PR:
-
Partial response
- RDC:
-
Remote data capture system
- SD:
-
Stable disease
- SLCG:
-
Spanish lung cancer group
- SUMP:
-
Special use medication program
- TKI:
-
Tyrosine kinase inhibitors
References
López-Abente G, Pollán M, Aragonés N, Pérez Gómez B, Hernández Barrera V, Lope V, Suárez B. Situación del cáncer en España: incidencia. An Sist Sanit Navar. 2004;27:165–73.
Provencio M, Carcereny E, Rodríguez-Abreu D, López-Castro R, Guirado M, Camps C, et al. Lung cancer in Spain: information from the thoracic tumors registry (TTR study). Transl Lung Cancer Res. 2019;8(4):461–75.
Lee CK, Davies L, Wu YL, Mitsudomi T, Inoue A, Rosell R, et al. Gefitinib or erlotinib vs chemotherapy for EGFR mutation-positive lung cancer: individual patient data meta-analysis of overall survival. J Natl Cancer Inst. 2017:109.
Lee CK, Brown C, Gralla RJ, Hirsh V, Thongprasert S, Tsai CM, et al. Impact of EGFR inhibitor in non-small cell lung cancer on progression-free and overall survival: a meta-analysis. J Natl Cancer Inst. 2013;105(9):595–605.
Oxnard GR, Arcila ME, Sima CS, Riely GJ, Chmielecki J, Kris MG, et al. Acquired resistance to EGFR tyrosine kinase inhibitors in EGFR-mutant lung cancer: distinct natural history of patients with tumors harboring the T790M mutation. Clin Cancer Res. 2011;17(6):1616–22.
Schiller JH, Harrington D, Belani CP, Langer C, Sandler A, Krook J, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346(2):92–8.
Gridelli C, Ciardiello F, Gallo C, Feld R, Butts C, Gebbia V, et al. First-line erlotinib followed by second-line cisplatin-gemcitabine chemotherapy in advanced non-small-cell lung cancer: the TORCH randomized trial. J Clin Oncol. 2012;30(24):3002–11.
Schuler M, Yang JC-H, Park K, Kim J-H, Bennouna J, Chen Y-M, et al. Afatinib beyond progression in patients with non-small-cell lung cancer following chemotherapy, erlotinib/gefitinib and afatinib: phase III randomized LUX-lung 5 trial. Ann Oncol. 2016;27(3):417–23.
Ballard P, Yates JWT, Yang Z, Kim D-W, Yang JC-H, Cantarini M, et al. Preclinical comparison of osimertinib with other EGFR-TKIs in EGFR-mutant NSCLC brain metastases models, and early evidence of clinical brain metastases activity. Clin Cancer Res. 2016;22(29):5130–40.
Cross DAE, Ashton SE, Ghiorghiu S, Eberlein C, Nebhan CA, Spitzler PJ, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4(9):1046–61.
Khozin S, Weinstock C, Blumenthal GM, Cheng J, He K, Zhuang L, et al. Osimertinib for the treatment of metastatic EGFR T790M mutation-positive non-small cell lung Cancer. Clin Cancer Res. 2017;23(9):2131–5.
Marinis F, Wu YL, de Castro G Jr, Chan G-C, Chen Y-M, Cho BC, et al. ASTRIS: a global real-world study of osimertinib in >3000 patients with EGFR T790M positive non-small-cell lung cancer. Future Oncol. 2019;15(26):3003–14.
Yang JCH, Ahn MJ, Kim DW, Ramalingam SS, Sequist LV, Su W-C, et al. Osimertinib in pretreated T790M-positive advanced non-small-cell lung cancer: AURA study phase II extension component. J Clin Oncol. 2017;35(12):1288–96.
Soria J-C, Wu Y-L, Nakagawa K, Kim S-W, Yang J-J, Ahn M-J, et al. Gefitinib plus chemotherapy versus placebo plus chemotherapy in EGFR-mutation-positive non-small-cell lung cancer after progression on first-line gefitinib (IMPRESS): a phase 3 randomised trial. Lancet Oncol. 2015;16(8):990–8.
Stratmann JA, Michels S, Hornetz S, Christoph DC, Sackmann S, Spengler W, et al. Efficacy and safety of the German expanded access program of osimertinib in patients with advanced, T790M-positive non-small cell lung cancer. J Cancer Res Clin Oncol. 2018;144(12):2457–63.
Ahn MJ, Tsai CM, Shepherd FA, Bazhenova L, Sequist LV, Hida T, et al. Osimertinib in patients with T790M mutation-positive, advanced non-small cell lung cancer: long-term follow-up from a pooled analysis of 2 phase 2 studies. Cancer. 2019;125(6):892–901.
Mehlman C, Cadranel J, Rousseau-Bussac G, Lacave R, Pujals A, Girard N, et al. Resistance mechanism to Osimertinib in EGFR-mutated advanced non-small-cell lung cancer: a multicentric retrospective French study. Lung Cancer. 2019;137:149–56.
Douillard J-Y, Ostoros G, Cobo M, Ciuleanu T, McCormack R, Webster A, Milenkova T. First-line gefitinib in caucasian EGFR mutation-positive NSCLC patients: a phase-IV, open-label, single-arm study. Br J Cancer. 2014;110(1):55–62.
Rangachari D, Yamaguchi N, VanderLaan PA, Folch E, Mahadevan A, Floyd SR, et al. Brain metastases in patients with EGFR-mutated or ALK-rearranged non-small-cell lung cancers. Lung Cancer. 2015;88(1):108–11.
Mok TS, Wu Y-L, Ahn M-J, Garassino MC, Kim HR, Ramalingam SS, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. 2017;376(7):629–40.
Ramalingam SS, Vansteenkiste J, Planchard D, Cho BC, Gray JE, Ohe Y, et al. Overall survival with Osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41–50.
Mu Y, Xing P, Hao X, Wang Y, Li J. Real-world data of osimertinib in patients with pretreated non-small cell lung cancer: a retrospective study. Cancer Manag Res. 2019;11:9243–51.
Auliac JB, Pérol M, Planchard D, Monnet I, Wislez M, Doubre H, et al. Real-life efficacy of osimertinib in pretreated patients with advanced non-small cell lung cancer harboring EGFR T790M mutation. Lung Cancer. 2019;127:96–102.
Acknowledgements
We thank the investigators and staffs at all 30 sites that participated.
Authors´ contributions
All authors read and approved the manuscript. MP, JT, PG, RG, FA, PD, DA, CG-G, JH, CA, JG, EE, LG-A, TM, OJ, LEC, JLM, RL, ALO, EM, JC, AMS, JB-B, AS, NF, EB, MC, DI, MM, FN, VC have contributed to all the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted. The authors read and approved the final manuscript.
Funding
The study was coordinated and monitored by the Spanish Lung Cancer Group (SLCG) and financed by AstraZeneca following the specifications in the protocol. This funding included the cost of submitting the study for approval to an accredited Independent Ethics Committee (IEC); submission for classification to the Agencia Española de Medicamentos y Productos Sanitarios (AEMPS); database design, maintenance and management; monitoring activities; statistical analysis and corresponding statistical report.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was evaluated by the Ethical Committee of Hospital Universitario Puerta de Hierro de Majadahonda, Madrid. The study was also classified by the Spanish Health Authority as “EPA-OD” (post-authorization study, other designs). The study was carried out following the Declaration of Helsinki on Good Clinical Practices and Organic Law 3/2018, 5th December on Protection of Personal Data and digital rights that were guaranteed during the study. Alive patients have signed and dated an Institutional Review Board/Independent Ethics Committee (IRB/IEC)-approved written informed consent form in accordance with regulatory and institutional guidelines.
Consent for publication
Not applicable.
Competing interests
A summary conflict of interest statement in a separate document.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Provencio, M., Terrasa, J., Garrido, P. et al. Osimertinib in advanced EGFR-T790M mutation-positive non-small cell lung cancer patients treated within the Special Use Medication Program in Spain: OSIREX-Spanish Lung Cancer Group. BMC Cancer 21, 230 (2021). https://doi.org/10.1186/s12885-021-07922-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-021-07922-5