
Abstract
Background
The benefit of adjuvant chemotherapy in invasive lobular carcinoma (ILC) is still unclear. The objective of the current study was to elucidate the effectiveness of adjuvant chemotherapy in hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative, pT1b-c/N0–1/M0 ILC.
Methods
Based on Surveillance, Epidemiology, and End-Results (SEER) database, we identified original 12,334 HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC patients, who were then divided into adjuvant chemotherapy group and control group. End-points were overall survival (OS) and breast cancer-specific mortality (BCSM). Aiming to minimize the selection bias of baseline characteristics, Propensity Score Matching (PSM) method was used.
Results
In a total of 12,334 patients with HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC, 1785 patients (14.5%) were allocated into adjuvant chemotherapy group and 10,549 (85.5%) into control group. Used PSM, the 1785 patients in adjuvant chemotherapy group matched to the 1785 patients in control group. By Kaplan-Meier survival analyses, we observed no beneficial effect of adjuvant chemotherapy on OS in both original samples (P = 0.639) and matched samples (P = 0.962), however, ineffective or even contrary results of adjuvant chemotherapy on BCSM both in original samples (P = 0.001) and in matched samples (P = 0.002). In both original and matched multivariate Cox models, we observed ineffectiveness of adjuvant chemotherapy on OS (hazard ratio (HR) for overall survival = 0.82, 95% confidence interval (CI) [0.62–1.09]; P = 0.172 and HR = 0.90, 95%CI [0.65–1.26]; P = 0.553, respectively), unexpectedly promoting effect of adjuvant chemotherapy on BCSM (HR = 2.33, 95%CI [1.47–3.67]; P = 0.001 and HR = 2.41, 95%CI [1.32–4.39]; P = 0.004, respectively). Standard surgery was beneficial to the survival of patients. Lymph node metastasis was detrimental to survival and radiotherapy brought survival benefit in original samples, but two issues had unobvious effect in matched samples.
Conclusion
In this study, adjuvant chemotherapy did not improve survival for patients with HR-positive, HER2-negative pT1b-c/N0–1/M0 ILC.
Similar content being viewed by others

Background
Invasive lobular carcinoma (ILC) is the most common ‘special’ morphological subtype of breast cancer and presents with a distinctive clinical behavior compared with invasive ductal carcinoma (IDC) (no special type) [1, 2]. Classical ILC is characterized by monotonous small, uniform, discohesive cells that infiltrate the stroma in a single-file pattern [2]. This distinctive feature of classical ILC results from the E-cadherin loss on tumor cell membranes [3, 4]. Importantly, loss of E-cadherin not only results in a dysfunctional E-cadherin-catenin complex with consequences on cell-cell adhesion but also the different inter-cellular and intracellular signaling pathways [5]. Therefore, ILC should be considered to a distinct entity different from IDC [6, 7].
Generally, ILC displays features associated with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative, being low grade and a good prognosis [8]. It is generally admitted that ILC, especially HR-positive, HER-2-negative ILC, is endocrine responsive, and responds poorly to chemotherapy [9, 10]. So for it is not yet settled in published clinical studies that whether adjuvant chemotherapy is effective for relatively early stage patients with HR-positive, HER2-negative ILC.
In 2011, based on a Dutch regional cohort of 498 ILC patients, Truin et al. [11] reported that overall survival (OS) was not statistically different in HR-positive ILC patients treated with adjuvant endocrine therapy and chemotherapy compared to adjuvant endocrine therapy alone (5-year OS 85.2% vs 82.8%, P = 0.68). In 2012, using the data from the Netherlands Cancer Registry (NCR) of 3685 ILC patients, Truin et al. [12] also reported that adjuvant chemotherapy seems to confer no additional beneficial effects in postmenopausal patients with pure or mixed type ILC (10-year OS 66% vs 68%, P = 0.45). In 2017, identifying 4638 ILC from California Cancer Registry (CCR), Marmor et al. [13] determined a similar result that patients with estrogen receptor (ER)-positive, HER2-negative, stage I/II ILC who received adjuvant endocrine therapy did not benefit from the addition of adjuvant chemotherapy. However, using 2318 ILC data source from 15 academic French cancer centers between 1990 and 2014, Nonneville et al. [14] recently reported that the significant disease-free survival (DFS) and OS benefits from adjuvant chemotherapy could be derived in high-risk ILC patients, but not in low-risk ILC patients.
In a dilemma, how should we make a treatment choice for HR-positive, HER2-negative, pT1–2/N0–1/M0 ILC, especially, the pT1b-c/N0–1/M0 ILC? The Surveillance, Epidemiology, and End-Results (SEER) database is publicly available for studies of cancer-based epidemiology and TNM staging of breast cancer and other cancers, which covers approximately 28% of the US population [7, 15]. Using SEER database, the aims of our study were to confirm whether the adjuvant chemotherapy could bring survival benefit to patients with HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC. To our knowledge, this is the first and the largest, population-based study presenting evidence of effect of adjuvant chemotherapy in patients with ILC used SEER database. Above all, our findings have a direct and meaningful translation to the clinic, allowing us to avoid excessive adjuvant chemotherapy for patients with HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC.
Methods
Data source and study design
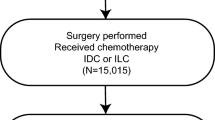
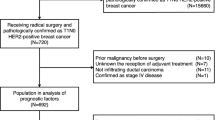
The SEER program is a national database and primary source of cancer statistics that is currently maintained by the National Cancer Institute. We have got permission to access the database and reproduce individual data in SEER*Stat Database: Incidence - SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975–2016 varying) - Linked To County Attributes - Total U.S., 1969–2017 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2019, based on the November 2018 submission. We obtained patients diagnosed with ILC of pT1b-c/N0–1/M0 according to Site Recode classification and AJCC 7th ed. stage system. The collected patients were diagnosed from 2010 to 2016, because breast cancer subtype was available in SEER database since 2010. We retrieved 14,844 record of HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC (Supplementary Table 1). After omitting censored data and excluding patients older than 80 years old, a total of 12,334 patients were enrolled in our study (Fig.1).

Flow diagram of patient selection and study development
Statistical analysis
The differences of demographic and clinic-pathological features between chemotherapy group and control group were analyzed by chi-square and Wilcoxon ranksum test. Propensity Score Matching (PSM) method (Match Ratio 1:1; Logit model; the nearest neighbor matching approach) was used to eliminate clinic-pathological mixed bias in two groups (Supplementary dofile). Overall survival (OS) was defined as the time from admission to the date of death from any cause. Breast cancer-specific mortality (BCSM) was defined as the period from the operative date to death of breast cancer. The OS curves and BCSM curves of each group were estimated by Kaplan-Meier survival analyses, and the curves were analyzed by the log-rank test. In the multivariate analysis, a COX’s Proportional Hazard Model was employed to estimate whether a factor was a significant independent prognostic factor of survival. All statistical tests were two-sided, P values less than 0.05 were considered as statistically significant. The statistical analyses were performed using STATA version 15.1 for windows (StataCorp LLC).
Results
Characteristics of the original patients
After omitting censored data and excluding patients older than 80 years old, an original of 12,334 patients with HR-positive, Her-2-negative, pT1b-c/N0–1/M0 ILC were enrolled in our study (Supplementary Table 2). In total patients, 1785 patients (14.5%) received the adjuvant chemotherapy (chemotherapy group) and 10,549 patients (85.5%) not (control group). Compared with patients of control group, patients of chemotherapy group presented significantly more adverse prognostic features, such as young age (58.49% vs. 32.83% age < 60, P < 0.05), larger tumor size (79.05% vs. 67.25% T1c, P = 0.001), high grade (75.91% vs. 65.7% grades II&III, P < 0.05), more lymph node involvement (49.86% vs. 11.76% pN1, P = 0.001). Patients of chemotherapy group underwent more mastectomy (50.81% vs. 34.08%, P < 0.05), but less radiotherapy (50.53% vs. 54.74%, P < 0.05). The comparisons of characteristics between two groups were shown in Table 1.
PSM method to minimize the selection bias of baseline characteristics
In order to study the effect of chemotherapy on survival by equilibrium, we employed PSM method (Match Ratio 1:1) to minimize the selection bias of demographic and clinic-pathological characteristics between the two groups. The kernel density functions of the chemotherapy group and the control group, based on pre-matching showed that the characteristics of the variables in the two groups had remarkable bias (Fig.2a). After matching, as shown in Fig.2b, the kernel density functions of the chemotherapy group and the control group (1785 patients from original control group) were a lot closer, indicating that the clinic-pathological characteristics in chemotherapy group and the control group are similar (Supplementary Table 3).

a Kernel Density of the chemotherapy and control groups before PS matching; b Kernel Density of the chemotherapy and control groups after PS matching
Characteristics of the matched patients
The matched results showed that the bias between chemotherapy group and the control group had unobvious statistically significant (bias< ± 10, P>0.05). In matched samples, apart from age (P = 0.001), almost all of the demographic and clinic-pathological characteristics were similarly distributed between chemotherapy group and control group (P>0.05) (Table 2).
OS and BCSM analysis before or after matching
In the original 12,334 patients with HR-positive, Her-2-negative, T1b-c/N0–1/M0 ILC were followed-up for a median of 42 months (range of 1 to 83 months). By the end of follow-up period, 74 of 1785 patients (chemotherapy group) had died, 41 patients died of breast cancer, with the corresponding, 361 of 10,549 patients (control group) had died, 76 patients due to recurrence and metastasis of breast cancer. Thus before matching, the OS of the chemotherapy group had no obviously difference than that of the control group (P = 0.639, log-rank test) (Fig.3a). However, the BCSM of the chemotherapy group was higher than that of the control group, which reach distinct levels of statistical significance (P = 0.001, log-rank test) (Fig.3b).

a Kaplan–Meier analyses of the effect chemotherapy on OS in original samples (P = 0.639, log-rank test); b Kaplan–Meier analyses of the effect chemotherapy on BCSM in original samples (P = 0.001, log-rank test); c Kaplan–Meier analyses of the effect chemotherapy on OS in matched samples (P = 0.962, log-rank test); d Kaplan–Meier analyses of the effect chemotherapy on BCSM in matched samples (P = 0.002, log-rank test)
After matching, 66 of 1785 patients in the control group had dead, 15 of whom owing to the breast cancer. The OS curve of chemotherapy group and control group interwove with each other (P = 0.962, log-rank test) (Fig.3c). Unexpectedly, the BCSM of the chemotherapy group was still statistical significantly higher than that of the control group (P = 0.002, log-rank test) (Fig.3d). Accordingly, adjuvant chemotherapy was likely on the contrary to induced more breast cancer mortality.
The original and the matched multivariate Cox proportional hazards models for OS and BCSM
To adjust potential modifier effects to adjuvant chemotherapy, both the original and the propensity score matched multivariate Cox proportional hazards models were fitted for overall survival and BCSM. As shown in Fig.4a and Table 3, adjuvant chemotherapy did not bring overall survival benefit in both original and matched Cox models (HR = 0.82, 95%CI [0.62–1.09]; P = 0.172 and HR = 0.90, 95%CI [0.65–1.26]; P = 0.553, respectively). However, as shown in Fig.4b and Table 3, adjuvant chemotherapy unexpectedly increased the risk of BCSM in both original and matched Cox models (HR = 2.33, 95%CI [1.47–3.67]; P = 0.001 and HR = 2.41, 95%CI [1.32–4.39]; P = 0.004, respectively). Additionally, in both original and matched Cox models, standard surgery was negatively correlated with the risk of BCSM and improved overall survival (all coefficients < 0, P < 0.05) shown in Fig.4a, Fig.4b and Table 3. Advanced age was a pernicious factor for overall survival. Lymph node metastasis was positively related to both poor overall survival and risk of BCSM in original Cox models (all coefficients > 0, P < 0.05), however, they were no longer significant for overall survival and BCSM in matched Cox models shown in Fig.4a, Fig.4b and Table 3. The effect of radiotherapy was just opposite to lymph node metastasis. In original samples, the prognosis of white race patients is better than that of black race. This trend gets still more obvious in matched samples (HR for OS > 1 and HR for BCSM < 1, P < 0.05). High histological grade had no implicit relation with the risk of overall survival and BCSM in both original and matched samples (all coefficients > 0, but P > 0.05).

a Cox proportional hazards models for overall mortality before and after matching; b Cox proportional hazards models for BCSM before and after matching
Discussion
As well as HR and HER2 status, some studies have indicated that the histological subtype of the breast cancer also plays an important role in predicting the response to adjuvant chemotherapy and/or neoadjuvant chemotherapy (NAC) [16,17,18,19]. In 2005, Cristofanilli et al. [16, 17] reported that ILC is characterized by lower pathologic complete response (pCR) rates to NAC but better long-term outcomes compared to IDC. In 2007, Katz et al. [18] reviewed randomized trials of NAC and noted that the pCR rate was 1.7% in ILC and 11.6% in IDC (no special type). In 2010, in the era of tailored therapy for individual patients, Purushotham et al. [19] documented that we would no longer routinely recommend NAC in patients with ER-positive, HER2-negative, classical type ILC.
However, though it is generally admitted that ILC, especially HR-positive, HER2-negative ILC, responds poorly to chemotherapy, currently available data do not unanimously support these assumptions. In 2012, Lips et al. [9] reported a similar pCR rate in both ER-positive, HER2-negative IDC and ER-positive, HER2-negative ILC patients (4.2 and 4.3%, respectively). In 2014, Guiu et al. [20] reported that in multivariate analysis, histology of ILC was not an independent negative predictive factor of pCR in seven [21,22,23,24,25,26,27] of nine studies [21,22,23,24,25,26,27,28,29].
Thus, we could not draw a conclusion that ILC or even HR-positive, HER2-negativeis ILC is an independent predictor of poor response to adjuvant chemotherapy and/or NAC. In fact, minority of past and current studies take lobular histology into account in pretreatment stratification or subgroup analysis. Consequently, findings of these studies limit our ability to indicate whether patients with IDC or ILC should be managed with similar or different treatments. At present, the National Comprehensive Cancer Network (NCCN) and the St Gallen International Expert Consensus guidelines for systemic therapy decisions are almostly derived from studies based on IDC. Neither of these two guidelines consider histologic subtype as a factor for determining systemic therapy decisions. Making systemic therapy decisions for patients with ILC is thus challenging for the oncology community. It is unlikely that a future randomized clinical trial (RCT) concerning this subject will be accomplished. There is lack of stronger evidence support, this may be why our guidelines still do not distinguish ILC from IDC for treatment allocation or classification therapy.
In this study by using SEER database, we firstly compared the cohort characteristics between the included HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC patients with and without adjuvant chemotherapy, in both original and propensity score matched sample, respectively. Secondly, OS and BCSM analyses between chemotherapy and control groups were made, before or after PSM, respectively. Thirdly, to adjust the potential confounding factors to chemotherapy, the multivariate Cox regression analyses were performed for overall survival and BCSM, in both original and matched sample, respectively. Our data demonstrate that patients with HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC could not derive survival benefit from the adjuvant chemotherapy shown in Fig.2, Fig.3 and Table 3, neither for OS nor for BCSM. In both original and propensity score matched sample, ILC patients with adjuvant endocrine therapy and chemotherapy had a worse BCSM than ILC patients with adjuvant endocrine therapy alone. This finding is almost certainly secondary to selection bias and not cause and effect of adjuvant chemotherapy.
Histological grading is an important part of breast cancer classification, and is performed using the Nottingham histological grading system. However, it has been controversial as to the relevance of this system for ILC, since tubule formation is rare (except in the tubulo-lobular variant) [30]. With limited nuclear pleomorphism and sparse mitotic count, ILC (including variants) is often characterized by lower histologic grade compared to IDC [31]. In both our original and matched samples, almost or more than ninety percentages of ILC were histologic grade 1–2 (Table 1 and Table 2). Consequently, a therapeutic dilemma can occur in the event of the relative resistance of ILC to conventional chemotherapeutic agents [32, 33]. Moreover, lack of E-cadherin protein expression in ILC is distinctive from IDC [34]. It has been hypothesized that the lack of chemosensitivity of ILC is explained by the inactivation of E-cadherin in ILC. Loss of E-cadherin protein is thought to increase of epithelial to mesenchymal transition (EMT), which in turn become more resistant to chemotherapy [35]. Accordingly, lower histologic grade and deficiency of E-cadherin of ILC both supported our results.
It has been demonstrated that ILC and IDC have distinct genomic, transcriptomic and expression profiles [36]. Recent major advances in genome-wide transcription analyses, comparative genomic hybridization (CGH) and genomic tests further acknowledged the natural history and also the heterogeneity of ILC [37]. It has been suggested that the genomic signatures could be used to assist systemic therapy decisions for patients with ILC, and especially the decision of adding chemotherapy to hormonal therapy [38]. For instance, mutations in exon 9 of the PIK3CA gene have previously been reported more frequent in ILC than in IDC [39,40,41]. These mutations increase kinase activity, confer increased resistance to paclitaxel and are associated with metastatic capability [42, 43]. Intriguingly, loss of E-cadherin of ILC has been also associated with many genetic and molecular alterations including the inactivation of the CDH1 gene at 16q22 by mutation, loss of heterozygosity, or CDH1 promoter methylation, which finally lead to the poor response to cytotoxic chemotherapy [3, 4, 44].
Oncotype Dx Breast Cancer Assay is a 21-gene assay used in estrogen receptor (ER)-positive breast cancer to predict benefit from chemotherapy [45, 46]. In 2015, Conlon et al. [47] reported that Oncotype Dx recurrence score (RS) currently plays a clinically useful role in the management of ILC, which may prevent the over-treatment of adjuvant chemotherapy. In 2017, Kizy et al. [48] reported that patients with ER-positive ILC, 8% were in the high-risk and 72% were in the intermediate-risk groups as per the trial assigning individualized options for treatment (TAILORx) RS cutoffs. Adjuvant chemotherapy did not seem to confer a survival benefit for either the intermediate- or the high-risk cohorts [48].
Some limitations of our study have to be considered, thus we ought to be caution about our results. Our SEER database does not include information regarding the ILC and its variants, the loss of E-cadherin, the exact ER and PR and Ki67 expression, the 21-gene assay, the administration of chemotherapy and endocrine therapy, ect. Additionally, we should exclude all cases where breast cancer has only been reported by death certificate or autopsy. Thirdly, there is indeed an important deficiency is that the chemotherapy record in SEER database is classified as “No/Unknown” and “Yes”. Although we obtained data of 1785 patients with definite chemotherapy from SEER database, we don’t know whether the patients recorded as “No/Unknown” actually received chemotherapy. All these confounding factors may have affected our results. For example, the most recent 2012 WHO classification of breast cancer distinguishes the ILC and its variants: classic, solid, alveolar, pleomorphic, tubulo-lobular, and mixed variant [1]. Lack of E-cadherin is observed in all histological ILC variants, except for tubulo-lobular variant (tubulo-lobular carcinoma, TLC). Pleomorphic variant (pleomorphic invasive lobular carcinoma, PILC) shares many additional genomic changes with classic ILC such as TP53 stabilization, amplifications of MYC, MDM2, HER2/TOP2A and 20q13 [49].
Our study is subject to some methodologic limitations too, which will lead to inevitable bias. The present study is a retrospective cohort study, however, not a RCT. The patient demographics and tumor characteristics are not totally consistent between the included ILC patients with and without adjuvant chemotherapy, even though after PSM analysis. Furthermore, the PSM analysis is also limited by the lack of adjustment for the cointervention of surgery therapy or radiation therapy, which demotivates our study due to reduce the sample sizes or event rates.
Nevertheless, until now, it is not clear whether there is a difference ineffectiveness between chemotherapy regimens administered to patients with ILC. Therefore, we suggest that further research on the type of chemotherapy administered to patients with ILC should be carried out. Moreover, evaluation of the response of ILC patients to endocrine therapy is an emerging direction of clinical breast cancer research [50]. It was reported that the magnitude of benefit of adjuvant letrozole is greater for patients diagnosed with ILC compared to those with IDC [51]. In fact, it may be time for the oncologists to consider a prospective RCT to evaluate the role of NAC versus neoadjuvant endocrine therapy in ILC patients [18]. Additionally, whether CDK4/6 inhibitor is more effective for HR-positive, HER2-negative ILC than for HR-positive, HER2-negative IDC is worth to study. Finally, we advise to the oncologists that ILC and its variants should be studied, with further efforts made to develop more individualized treatment for them and to identify potential mechanisms of their biological inferiority and superiority, respectively [52, 53].
Conclusion
Adjuvant chemotherapy could not improve survival for patients with HR-positive, HER2-negative pT1b-c/N0–1/M0 ILC.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its sementary information files].
Abbreviations
- BCSM:
-
Breast cancer-specific mortality
- CGH:
-
Comparative genomic hybridization
- CI:
-
Confidence interval
- DFS:
-
Disease-free survival
- EMT:
-
Epithelial to mesenchymal transition
- ER:
-
Estrogen receptor
- HER2:
-
Human epidermal growth factor receptor 2
- HR:
-
Hazard ratio
- HR:
-
Hormone receptor
- IDC:
-
Invasive duct carcinoma of no special type
- ILC:
-
Invasive lobular carcinoma
- NAC:
-
neoadjuvant chemotherapy
- NCCN:
-
National Comprehensive Cancer Network
- OS:
-
Overall survival
- pCR:
-
Pathologic complete response
- PSM:
-
Propensity score matching
- RCT:
-
randomized clinical trial
- RS:
-
Recurrence score
- SEER:
-
Surveillance, Epidemiology, and End-Results database
References
Frank GA, Danilova NV, Andreeva I, Nefedova NA. WHO classification of tumors of the breast, 2012. Arkh Patol. 2013;75(2):53–63.
Pestalozzi BC, Zahrieh D, Mallon E, Gusterson BA, Price KN, Gelber RD, Holmberg SB, Lindtner J, Snyder R, Thurlimann B, et al. Distinct clinical and prognostic features of infiltrating lobular carcinoma of the breast: combined results of 15 international breast Cancer study group clinical trials. J Clin Oncol. 2008;26(18):3006–14.
Rakha EA, Ellis IO. Lobular breast carcinoma and its variants. Semin Diagn Pathol. 2010;27(1):49–61.
Rakha EA, Patel A, Powe DG, Benhasouna A, Green AR, Lambros MB, Reis-Filho JS, Ellis IO. Clinical and biological significance of E-cadherin protein expression in invasive lobular carcinoma of the breast. Am J Surg Pathol. 2010;34(10):1472–9.
Yeatman TJ, Cantor AB, Smith TJ, Smith SK, Reintgen DS, Miller MS, Ku NN, Baekey PA, Cox CE. Tumor biology of infiltrating lobular carcinoma. Implications for management. Ann Surg. 1995;222(4):549–59 discussion 559-561.
Ciriello G, Gatza ML, Beck AH, Wilkerson MD, Rhie SK, Pastore A, Zhang H, McLellan M, Yau C, Kandoth C, et al. Comprehensive molecular portraits of invasive lobular breast Cancer. Cell. 2015;163(2):506–19.
Chen Z, Yang J, Li S, Lv M, Shen Y, Wang B, Li P, Yi M, Zhao X, Zhang L, et al. Invasive lobular carcinoma of the breast: a special histological type compared with invasive ductal carcinoma. PLoS One. 2017;12(9):e0182397.
McCart Reed AE, Kutasovic JR, Lakhani SR, Simpson PT. Invasive lobular carcinoma of the breast: morphology, biomarkers and 'omics. Breast Cancer Res. 2015;17:12.
Lips EH, Mulder L, de Ronde JJ, Mandjes IA, Vincent A, Vrancken Peeters MT, Nederlof PM, Wesseling J, Rodenhuis S. Neoadjuvant chemotherapy in ER+ HER2- breast cancer: response prediction based on immunohistochemical and molecular characteristics. Breast Cancer Res Treat. 2012;131(3):827–36.
Truin W, Vugts G, Roumen RM, Maaskant-Braat AJ, Nieuwenhuijzen GA, van der Heiden-van der Loo M, Tjan-Heijnen VC, Voogd AC. Differences in response and surgical management with Neoadjuvant chemotherapy in invasive lobular versus ductal breast Cancer. Ann Surg Oncol. 2016;23(1):51–7.
Truin W, Voogd AC, Vreugdenhil G, van der Sangen MJ, van Beek MW, Roumen RM. Influence of histology on the effectiveness of adjuvant chemotherapy in patients with hormone receptor positive invasive breast cancer. Breast. 2011;20(6):505–9.
Truin W, Voogd AC, Vreugdenhil G, van der Heiden-van der Loo M, Siesling S, Roumen RM. Effect of adjuvant chemotherapy in postmenopausal patients with invasive ductal versus lobular breast cancer. Ann Oncol. 2012;23(11):2859–65.
Marmor S, Hui JYC, Huang JL, Kizy S, Beckwith H, Blaes AH, Rueth NM, Tuttle TM. Relative effectiveness of adjuvant chemotherapy for invasive lobular compared with invasive ductal carcinoma of the breast. Cancer. 2017;123(16):3015–21.
de Nonneville A, Jauffret C, Goncalves A, Classe JM, Cohen M, Reyal F, Mazouni C, Chauvet MP, Chopin N, Colombo PE, et al. Adjuvant chemotherapy in lobular carcinoma of the breast: a clinicopathological score identifies high-risk patient with survival benefit. Breast Cancer Res Treat. 2019;175:379–87.
Yu TJ, Liu YY, Hu X, Di GH. Survival following breast-conserving therapy is equal to that following mastectomy in young women with early-stage invasive lobular carcinoma. Eur J Surg Oncol. 2018;44(11):1703–7.
Cristofanilli M, Gonzalez-Angulo A, Sneige N, Kau SW, Broglio K, Theriault RL, Valero V, Buzdar AU, Kuerer H, Buchholz TA, et al. Invasive lobular carcinoma classic type: response to primary chemotherapy and survival outcomes. J Clin Oncol. 2005;23(1):41–8.
Katz A. Does neoadjuvant/adjuvant chemotherapy change the natural history of classic invasive lobular carcinoma? J Clin Oncol. 2005;23(27):6796 author reply 6796-6797.
Katz A, Saad ED, Porter P, Pusztai L. Primary systemic chemotherapy of invasive lobular carcinoma of the breast. Lancet Oncol. 2007;8(1):55–62.
Purushotham A, Pinder S, Cariati M, Harries M, Goldhirsch A. Neoadjuvant chemotherapy: not the best option in estrogen receptor-positive, HER2-negative, invasive classical lobular carcinoma of the breast? J Clin Oncol. 2010;28(22):3552–4.
Guiu S, Wolfer A, Jacot W, Fumoleau P, Romieu G, Bonnetain F, Fiche M. Invasive lobular breast cancer and its variants: how special are they for systemic therapy decisions? Crit Rev Oncol Hematol. 2014;92(3):235–57.
Dieras V, Fumoleau P, Romieu G, Tubiana-Hulin M, Namer M, Mauriac L, Guastalla JP, Pujade-Lauraine E, Kerbrat P, Maillart P, et al. Randomized parallel study of doxorubicin plus paclitaxel and doxorubicin plus cyclophosphamide as neoadjuvant treatment of patients with breast cancer. J Clin Oncol. 2004;22(24):4958–65.
Reitsamer R, Peintinger F, Prokop E, Hitzl W. Pathological complete response rates comparing 3 versus 6 cycles of epidoxorubicin and docetaxel in the neoadjuvant setting of patients with stage II and III breast cancer. Anti-Cancer Drugs. 2005;16(8):867–70.
Untch M, Fasching PA, Konecny GE, von Koch F, Conrad U, Fett W, Kurzeder C, Luck HJ, Stickeler E, Urbaczyk H, et al. PREPARE trial: a randomized phase III trial comparing preoperative, dose-dense, dose-intensified chemotherapy with epirubicin, paclitaxel and CMF versus a standard-dosed epirubicin/cyclophosphamide followed by paclitaxel +/− darbepoetin alfa in primary breast cancer--results at the time of surgery. Ann Oncol. 2011;22(9):1988–98.
von Minckwitz G, Blohmer JU, Raab G, Lohr A, Gerber B, Heinrich G, Eidtmann H, Kaufmann M, Hilfrich J, Jackisch C, et al. In vivo chemosensitivity-adapted preoperative chemotherapy in patients with early-stage breast cancer: the GEPARTRIO pilot study. Ann Oncol. 2005;16(1):56–63.
von Minckwitz G, Kummel S, Vogel P, Hanusch C, Eidtmann H, Hilfrich J, Gerber B, Huober J, Costa SD, Jackisch C, et al. Neoadjuvant vinorelbine-capecitabine versus docetaxel-doxorubicin-cyclophosphamide in early nonresponsive breast cancer: phase III randomized GeparTrio trial. J Natl Cancer Inst. 2008;100(8):542–51.
von Minckwitz G, Eidtmann H, Rezai M, Fasching PA, Tesch H, Eggemann H, Schrader I, Kittel K, Hanusch C, Kreienberg R, et al. Neoadjuvant chemotherapy and bevacizumab for HER2-negative breast cancer. N Engl J Med. 2012;366(4):299–309.
Untch M, Loibl S, Bischoff J, Eidtmann H, Kaufmann M, Blohmer JU, Hilfrich J, Strumberg D, Fasching PA, Kreienberg R, et al. Lapatinib versus trastuzumab in combination with neoadjuvant anthracycline-taxane-based chemotherapy (GeparQuinto, GBG 44): a randomised phase 3 trial. Lancet Oncol. 2012;13(2):135–44.
von Minckwitz G, Kummel S, Vogel P, Hanusch C, Eidtmann H, Hilfrich J, Gerber B, Huober J, Costa SD, Jackisch C, et al. Intensified neoadjuvant chemotherapy in early-responding breast cancer: phase III randomized GeparTrio study. J Natl Cancer Inst. 2008;100(8):552–62.
Chang HR, Glaspy J, Allison MA, Kass FC, Elashoff R, Chung DU, Gornbein J. Differential response of triple-negative breast cancer to a docetaxel and carboplatin-based neoadjuvant treatment. Cancer. 2010;116(18):4227–37.
Sinha PS, Bendall S, Bates T. Does routine grading of invasive lobular cancer of the breast have the same prognostic significance as for ductal cancers? Eur J Surg Oncol. 2000;26(8):733–7.
Mokbel K. Grading of infiltrating lobular carcinoma. Eur J Surg Oncol. 2001;27(6):609–10.
Rakha EA, El-Sayed ME, Menon S, Green AR, Lee AH, Ellis IO. Histologic grading is an independent prognostic factor in invasive lobular carcinoma of the breast. Breast Cancer Res Treat. 2008;111(1):121–7.
Christgen M, Steinemann D, Kuhnle E, Langer F, Gluz O, Harbeck N, Kreipe H. Lobular breast cancer: clinical, molecular and morphological characteristics. Pathol Res Pract. 2016;212(7):583–97.
Rakha EA, Abd El Rehim D, Pinder SE, Lewis SA, Ellis IO. E-cadherin expression in invasive non-lobular carcinoma of the breast and its prognostic significance. Histopathology. 2005;46(6):685–93.
Altundag K, Altundag O, Akyurek S, Karakaya E, Turen S. Inactivation of E-cadherin and less sensitivity of lobular breast carcinoma cells to chemotherapy. Breast. 2006;15(3):300.
Bertucci F, Orsetti B, Negre V, Finetti P, Rouge C, Ahomadegbe JC, Bibeau F, Mathieu MC, Treilleux I, Jacquemier J, et al. Lobular and ductal carcinomas of the breast have distinct genomic and expression profiles. Oncogene. 2008;27(40):5359–72.
Desmedt C, Zoppoli G, Gundem G, Pruneri G, Larsimont D, Fornili M, Fumagalli D, Brown D, Rothe F, Vincent D, et al. Genomic characterization of primary invasive lobular breast Cancer. J Clin Oncol. 2016;34(16):1872–81.
Prat A, Ellis MJ, Perou CM. Practical implications of gene-expression-based assays for breast oncologists. Nat Rev Clin Oncol. 2011;9(1):48–57.
Buttitta F, Felicioni L, Barassi F, Martella C, Paolizzi D, Fresu G, Salvatore S, Cuccurullo F, Mezzetti A, Campani D, et al. PIK3CA mutation and histological type in breast carcinoma: high frequency of mutations in lobular carcinoma. J Pathol. 2006;208(3):350–5.
Kalinsky K, Jacks LM, Heguy A, Patil S, Drobnjak M, Bhanot UK, Hedvat CV, Traina TA, Solit D, Gerald W, et al. PIK3CA mutation associates with improved outcome in breast cancer. Clin Cancer Res. 2009;15(16):5049–59.
Christgen M, Noskowicz M, Schipper E, Christgen H, Heil C, Krech T, Langer F, Kreipe H, Lehmann U. Oncogenic PIK3CA mutations in lobular breast cancer progression. Genes Chromosomes Cancer. 2013;52(1):69–80.
Isakoff SJ, Engelman JA, Irie HY, Luo J, Brachmann SM, Pearline RV, Cantley LC, Brugge JS. Breast cancer-associated PIK3CA mutations are oncogenic in mammary epithelial cells. Cancer Res. 2005;65(23):10992–1000.
Barbareschi M, Buttitta F, Felicioni L, Cotrupi S, Barassi F, Del Grammastro M, Ferro A, Dalla Palma P, Galligioni E, Marchetti A. Different prognostic roles of mutations in the helical and kinase domains of the PIK3CA gene in breast carcinomas. Clin Cancer Res. 2007;13(20):6064–9.
Cancer Genome Atlas N. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70.
Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, Geyer CE Jr, Dees EC, Perez EA, Olson JA Jr, et al. Prospective validation of a 21-gene expression assay in breast Cancer. N Engl J Med. 2015;373(21):2005–14.
Kwa M, Makris A, Esteva FJ. Clinical utility of gene-expression signatures in early stage breast cancer. Nat Rev Clin Oncol. 2017;14(10):595–610.
Conlon N, Ross DS, Howard J, Catalano JP, Dickler MN, Tan LK. Is there a role for Oncotype dx testing in invasive lobular carcinoma? Breast J. 2015;21(5):514–9.
Kizy S, Huang JL, Marmor S, Tuttle TM, Hui JYC. Impact of the 21-gene recurrence score on outcome in patients with invasive lobular carcinoma of the breast. Breast Cancer Res Treat. 2017;165(3):757–63.
Vargas AC, Lakhani SR, Simpson PT. Pleomorphic lobular carcinoma of the breast: molecular pathology and clinical impact. Future Oncol. 2009;5(2):233–43.
Arthur LM, Turnbull AK, Webber VL, Larionov AA, Renshaw L, Kay C, Thomas JS, Dixon JM, Sims AH. Molecular changes in lobular breast cancers in response to endocrine therapy. Cancer Res. 2014;74(19):5371–6.
Metzger Filho O, Giobbie-Hurder A, Mallon E, Gusterson B, Viale G, Winer EP, Thurlimann B, Gelber RD, Colleoni M, Ejlertsen B, et al. Relative effectiveness of Letrozole compared with Tamoxifen for patients with lobular carcinoma in the BIG 1-98 trial. J Clin Oncol. 2015;33(25):2772–9.
Coates AS, Winer EP, Goldhirsch A, Gelber RD, Gnant M, Piccart-Gebhart M, Thurlimann B, Senn HJ, Panel M. Tailoring therapies--improving the management of early breast cancer: St Gallen international expert consensus on the primary therapy of early breast Cancer 2015. Ann Oncol. 2015;26(8):1533–46.
Ribnikar D, Cardoso F. Tailoring chemotherapy in early-stage breast Cancer: based on tumor biology or tumor burden? Am Soc Clin Oncol Educ Book. 2016;35:e31–8.
Acknowledgments
The authors acknowledge the efforts of the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER database.
Funding
This work was supported by those Funds: Key Medical Specialty Fund Projects of Shanghai (grants number ZK2015A07) for design of the study; Shanghai Huangpu district science projects (grants number HKQ201804) for data collection and analysis; Shanghai Yangpu district science projects (grants number YP18M03) for interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
Literature search GFH, GXH, ZCJ and NRJ. Study design GFH, HY, XYL, MS, YMY, YWL, CW and CX. Methodology GFH and CX. Writing GFH, GXH, CW, and CX. Review and editing CX, XYL and CW. All authors have critically reviewed the final version of the manuscript and approved its content. The corresponding author had final responsibility for the decision to submit for publication. The authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by medical ethics committee of the Central Hospital of Huangpu District and conforming to the principles outlined in the Declaration of Helsinki for the use of human data. The need for consent was waived by our medical ethics committee of the Central Hospital of Huangpu District. It was deemed unnecessary according to our medical ethics committee and national regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Table 1.
14,844 initial samples - 14,844 initial record of HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC retrieved from SEER database.
Supplementary Table 2.
12,334 original samples - 12,334 record of HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC enrolled in the study.
Supplementary Table 3.
3570 matched samples - 3570 record of HR-positive, HER2-negative, pT1b-c/N0–1/M0 ILC (including 1785 matched non-chemotherapy patients and 1785 chemotherapy patients).
Additional file 4.
Supplementary dofile: dofile for Stata
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hu, G., Hu, G., Zhang, C. et al. Adjuvant chemotherapy could not bring survival benefit to HR-positive, HER2-negative, pT1b-c/N0–1/M0 invasive lobular carcinoma of the breast: a propensity score matching study based on SEER database. BMC Cancer 20, 136 (2020). https://doi.org/10.1186/s12885-020-6614-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-020-6614-0