
Abstract
Background
Breast cancer is the most deadly malignancy in Mexican women. Although treatment has improved, it may significantly affect bone mineral status in those who receive it. The aim of this study was to assess the impact of cancer treatment on bone mineral density (BMD) and bone mineral content (BMC), in patients with breast cancer and explore the interaction of menopausal status and clinical stage with cancer treatment on such changes.
Methods
A quasi-experimental design was applied with measurements before and after a chemotherapy treatment in 40 patients with primary diagnosis of invasive breast cancer. BMD and body composition measurements were taken by dual X-ray absorptiometry (DXA) and changes in these variables due to therapy were analyzed using mixed regression for repeated measurements.
Results
Significant loss was found in femoral neck and L2-L4 BMD (p < 0.001). Patients diagnosed with osteopenia or osteoporosis received calcium + vitamin D supplementation (600 mg/200 IU day). It showed a protective effect in the decrease of femoral neck BMD and total BMC. BMD loss in both femoral neck and L2-L4 BMD was higher in premenopausal women: 0.023 g/cm2 in femoral neck and 0.063 g/cm2 in L2-L4 (p < 0.001), while in postmenopausal women BMD loss was 0.015 g/cm2 in femoral neck and 0.035 g/cm2 in L2-L4 (p = 0.021 and p = 0.001 respectively). Change in lumbar spine BMD was prominent in premenopausal women with advanced clinical stage (IIB, IIIA, IIIB): 0.066 g/cm2 (p = 0.003).
Conclusion
The antineoplastic breast cancer treatment with chemotherapy had a negative impact on BMD, in premenopausal women overall, although a differential effect was found according to clinical stage and calcium supplementation status.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Background
Breast cancer is considered the neoplasm with the highest incidence and mortality rate in women worldwide. One million seven hundred thousand new cases were recorded in 2012, whereby is the second most common cancer overall and ranks fifth cause of death (522000 deaths) [1].
Although the incidence of breast cancer in Latin America is lower than those in the United States and the European Union, the mortality proportion regarding in those with the disease is high (>30 %), while in Mexico is almost 40 %. Disparities in results are mainly explained by the high prevalence of women diagnosed in advanced stages. For example, 60 % of breast cancer diagnoses are in early stages in the United States and 10 % in Mexico. This explains the most adverse side-effects of the disease and anticancer treatment in those with more advanced stages [2, 3].
During breast cancer, bone tissue is one of the most affected, mainly by ovarian failure, secondary to chemotherapy. The role of estrogens in bone metabolism is important as they stimulate bone formation by promoting osteoprotegerin production (bone formation induction factor), regulating the synthesis of active cytokines in the skeleton (promoted in part by the neoplasm itself) and by apoptosis inhibition of osteoblasts and osteocytes. Thus, estrogen deficiency reduces osteoprotegerin production which causes uncontrolled activity of osteoclasts increasing bone resorption [4, 5].
Some studies have reported differential effects in treatment response and survival, due to different body weight and its distribution by ethnicity [6, 7]. Given the fact that the Mexican population is genetically diverse, along with the knowledge that environmental and demographic factors may also affect susceptibility to treatment, the objectives of this study was to evaluate the impact of initial anticancer therapy on bone mineral status in Mexican women, by estimating the change in BMD in the femoral neck, lumbar spine (L2-L4) and total BMC. An additional objective was to evaluate the differential effect due to the clinical stage and menopausal status on BMC and BMD.
Methods
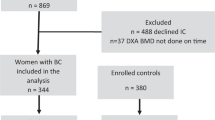
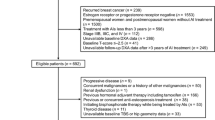
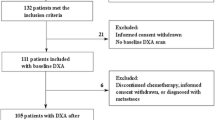
The design is based on a quasi-experimental prospective follow-up study of women with primary diagnosis of invasive breast cancer who attended at the State Center of Oncology (CEO from the acronym in Spanish) in Hermosillo, Sonora, to begin the anticancer treatment. The initial six-months of chemotherapy treatment was assay. Women were invited if they showed no metastasis or other diseases which affected their body composition such as hypo and hyperthyroidism, fractures and/or disabling injuries or those who had received chemotherapy in the past. Patients were also excluded from the analysis if they developed metastasis during the study course and/or discontinued their treatment.
The protocol was approved by the Research Ethics Committee of the CEO and Ethics Committee of the Research Center for Food and Development (CIAD from the acronym in Spanish). The recruited volunteers were requested to sign an informed consent form. Information on clinical stage, treatment schedule, menopausal status (menstruation absence for over a year before treatment), socioeconomic status (determined by the social work department of the hospital in terms of monthly income, housing characteristics and access to basic services, etc.) and demographic data were taken from the clinical records of the participants at CEO with their previous permission. Anthropometric, body composition and BMD measurements were analyzed at CIAD facilities.
Body composition and BMD were determined using a dual X-ray absorptiometry (DXA-MD + Lunar Co., Madison, WI). Precision of that measures was Coefficient Variation (CV) <2 %. Three measurements (scans) were obtained, one for the whole body to assess the body composition and two in the lumbar spine (L2-L4) and femoral neck to determine the BMD. The results of body composition were reported in kilograms and BMD in g/cm2. All measurements were performed by trained and certificated technical staff before and after 6 months of receiving antineoplastic therapy. Women with diagnosed osteopenia or osteoporosis at baseline (n = 10) received a prescription of calcium and vitamin D3 supplementation (600 mg/200 IU day).
A total of 57 women were recruited from August 2007 to January 2008 (24 women) and from February to August 2009 (33 women). Three women dropped out the treatment and 14 more were excluded from the study due to metastases development during the tracking period; therefore, 40 patients were included in analyses.
Statistical analysis
All analyzes were performed with NCSS software version 7.03 (2007). A paired t-test was applied to analyze the changes of the study parameters before and after treatment. Normal distribution of the quantitative variables was evaluated using histograms; all response variables exhibit Gaussian distribution. To evaluate the treatment related changes of total BMC, BMD on femoral neck and L2-L4, separate mixed regression models for repeated measures were used. Interaction terms of hypothesized variable (treatment) with menopausal status (pre or post), calcium supplementation (yes or no) and clinical stage phase were considered at p ≤ 0.05. When a significant interaction was found, stratified analyses were conducted. The clinical stage was analyzed as a dichotomous variable due to the small number of subjects in some stages. Stages I and IIA in one category and stages IIB, IIIA and IIIB in a second one. Statistical significance was considered at p ≤ 0.05.
Results
The patients age distribution was 32 to 61 years; 19 were premenopausal and 21 postmenopausal. The average age of menarche was 12 years. Five patients were nulliparous, 28 reported using oral contraceptives (>3 years), 6 recognized to be regular smokers (daily) at the diagnostic time and 7 accepted had consumed alcohol occasionally (>1 time/week). Regarding education status, 11 women were enrolled beyond the basic level (high school or technical degree). Regarding socioeconomic status, 62.5 % were in low and 37.5 % in medium or high.
Five women were found in the stage I, 12 in IIA, 8 in IIB, 9 in IIIA and 6 in IIIB (Classification TNM) [8]. All patients received chemotherapy. Prescribed schedules were FAC (5-Fluorouracil, Adriamycin, Cyclophosphamide), FEC (5-Fluorouracil, Epirubicin, Cyclophosphamide) or DAC (Docetaxel, Adriamycin, Cyclophosphamide). Of the premenopausal patients 68 % become amenorrheic. Radiotherapy was additionally administered to 25 patients and 7 were eligible for monoclonal antibodies treatment (Trastuzumab); one of them not receive it for cardiac issues. The clinical pathological characteristics and chemotherapy schemes distribution describes at Table 1.
Table 2 displays t-score of BMD distribution on premenopausal and postmenopausal patients before and after to receive antineoplastic treatment at femoral neck and lumbar spine (L2-L4).
Table 3 shows parameters from the unadjusted analysis. Significant loss was observed in femoral neck and L2-L4 BMD (p < 0.001). In BMC the change did not reach statistical significance (p = 0.066).
A protective effect in the reduction of BMD at femoral neck and total BMC due calcium supplementation was found. In women supplemented there was no significant decrease in femoral neck BMD or total BMC; but in L2-L4 BMD which was significant (p = 0.003) despite calcium + vitamin D supplementation. Conversely, women who did not receive calcium supplement, showed significantly loss in femoral neck BMD, L2-L4 BMD and total BMC (p < 0.001, p < 0.001 and p = 0.039) (Table 4).
There was also interaction between treatment effect vs. menopausal status and vs. clinical stage (p < 0.05). Consequently, all the analyses were completed in the stratus of the interaction variables (Table 5). BMD loss was significant in premenopausal and postmenopausal women: −0.023 g/cm2 in femoral neck and −0.063 g/cm2 in L2-L4 (p < 0.001) in premenopausal women and −0.015 g/cm2 in femoral neck (p = 0.021) and −0.035 g/cm2 in L2-L4 (p = 0.001) in postmenopausal. In premenopausal patients decrease in L2-L4 BMD was directly related with clinical stage: −0.059 g/cm2 on stage I, IIA (p = 0.006) and −0.066 g/cm2 on stage IIB, IIIA, IIIB (p = 0.003). However, in femoral neck, a reverse pattern was observed, where BMD was −0.030 g/cm2 on stage I, IIA (p = 0.004) and −0.017 g/cm2 on stage IIB, IIIA, IIIB (p = 0.007). Also this trend remained between postmenopausal women, with significant changes in stages I, IIA (p = 0.037 for femoral neck and p < 0.001 for L2-L4).
Discussion
Estrogen activity is linked to bone metabolism and some chemotherapeutic agents such as cyclophosphamide which is related with bone resorption because of ovarian failure in premenopausal women related with this agent [9, 10]. Although almost all volunteers showed a significant loss in BMD, the impact was greater in premenopausal women. Furthermore, the decrease in BMD is higher than that reported by other authors during the same post-diagnosis period (6 months): For example, Shapiro et al.[9] reported 4 % lumbar spine BMD loss, in the present study it was similar (almost 5 %). Other studies reported comparable decline over a period of two years [11, 12].
In postmenopausal patients, BMD change was −3.08 %. Powles et al. [13] in a similar group of women, found that the change in the lumbar spine BMD was only −0.37 %. Since there is lack of information in the literature about the magnitude of these changes in Mexican population under an internationally standardized chemotherapy regimen [14, 15], we believe that perhaps other causes such as genetic factors could be involved and can explain the differential effect found in this study with respect to others. Other studies have found that body composition differs significantly between Hispanic and Caucasian breast cancer female patients, however, neither group of countries have established guidelines for the administration of antineoplastic drugs based on body composition, in which case toxicity could be different for these groups [16]. Since the effective concentration of these antineoplastic drugs is affected by the amount of lean tissue [17, 18], it is believed that this can be a key element to elucidate the reason for the differences between the magnitude of the changes on BMD found by others researchers and the present study . The body antineoplastic concentration reached could also affect changes in body weight and body composition components such as BMD, fat mass, and fat free mass. However, other factors such as the diet may be involved.
Some patients started treatment with osteopenia, and calcium was part of their treatment. It appears that calcium showed a significant protective effect on the femur, but not on the lumbar spine. The explanation to the lower BMD loss on femoral neck than lumbar spine in both groups of women (calcium supplemented and no-supplemented) may be the same. The proportion of trabecular-cortical tissue and bone turnover rate are different in each skeletal region. The pathophysiology of osteoporosis [19, 20] indicates that about 25 % of trabecular bone (cancellous) is replaced every year, while cortical bone (laminar) is replaced at a level of 3 %. This is the reason why bone resorption degree is calculated using BMD as a reference at the proximal femur (neck, trochanter) and spine. Both sites contain high proportion of cancellous tissue. Although these points have a high content of trabecular bone compared to the rest of the skeletal system, there is an important difference in their composition. The fact that proximal femur has 30–50 % of trabecular tissue whereas the lumbar spine has 85 % explains why the lumbar spine is more susceptible to the effect due to decreased estrogen level, so that bone tissue resorption at L2-L4 resulted exacerbated. There is a greater release of calcium into the bloodstream, which can maintain parathyroid hormone (PTH) levels marginally low; preventing activation and mobilization of enough vitamin D on lumbar spine tissue to stimulate the calcium bond. On the other hand, the femoral neck bone turnover rate is lower and calcium supplied along with activation and mobilization of vitamin D with that level of PTH, is enough to raise the rate of mineralization at the newly remodeled tissue.
A recent finding indicates that the involvement of estrogens and its protective effect on trabecular tissue metabolism is much higher than that in cortical tissue, which could explain the higher susceptibility of cancellous tissue to ovarian ablation, regardless of differences in the rate of bone turnover between these tissues [21]. In addition to primary chemotherapeutic treatment scheme, which contributes to bone resorption, breast cancer patients received anti-estrogen therapy for a five-year period. These drugs also favored the decrease in BMD. Confavreux et al. [22] found that the patients who underwent treatment with anastrozole had a decrease of 3.3 % in lumbar spine BMD and 2.8 % in femoral neck in a one year period. Some investigations have published similar effects as those of Letrozole, Tamoxifen and Exemestane treatments [23–25].
Another consideration in decreasing BMD is the increase in body weight in patients. As previously reported [26], this patients group decreased lean mass, while premenopausal women increased body weight and adipose tissue. Since one of the mechanisms that stimulates the bone remodeling is the body calcium demand, it appears that the higher increase of body mass the greater the rate of calcium mobilization from bone matrix, combined with poor bone remodeling by estrogen loss which can help control osteoclastic activity [20]. However, the fact that fat tissue showed higher increase than lean tissue, could result in increased toxicity due to antineoplastic drugs, because they can have a greater effect since the dosage thereof is calculated according to total body weight but its real concentration in the body is affected for the lean tissue proportion. This could be a reason to suggest the evaluation of sarcopenia status in patients with cancer as well as chemotherapy dose adjustments [17, 18].
An additional finding is the clinical stage effect on BMD. In the initial chemotherapy scheme there are no important differences in the antineoplastic doses and their combinations between clinical stages that could result in a different effect on estrogen concentration in the 6-month-follow-up period. Variations in treatment are prescribed depending on factors such as the type of carcinoma (ductal, lobular, etc.), molecular subtype and the age of the patients [15]. Patients in medium (IIB) or advanced clinical stages (IIIA, IIIB) are the most affected in regards to BMD, which could be explained by the tumor’s increased production of catabolic cytokines as well as by the body’s induced response [27, 28]. There is also the effect mediated by IL-1, IL-6, IFNγ and TNFα, that increases the invasiveness of the tumor on bone tissue. These cytokines also contribute to the loss of lean tissue in cancer patients with cachexia [29]. The loss of lean tissue can be masked by increased body fat in breast cancer patients [30].
The evaluation of BMD is not a routinely part of the treatment in cancer patients, even considering the harmful effects of anticancer and anti-estrogen on bone matrix. Breast cancer women may benefit from a proper diagnosis, plus the fact that they could also be given antirresorptive drugs with no additional cost to the patient that is already covered by the public government health programs. One might speculate that loss in BMD is not so relevant when considering the cost-benefit ratio of cancer treatment, in short term. In our study we found 4.97 % of BMD loss at the lumbar spine in six months. Saarto et al. [12] evaluated a group of patients and after two years found a similar decrease of BMD; after ten years, 23 % of them developed osteoporosis [31].
Health institutions worldwide should implement the evaluation of BMD in patients with breast cancer as part of the treatment regimen as suggested by the American Society of Clinical Oncology (ASCO) [32]. In addition, antiresorptive therapies could prevent bone metastasis [33]. Due to the alert issued in 2011 by the Food and Drug Administration (FDA) regarding the kidney damage in some cases, the ASCO recommended the limited use of bisphosphonates to the patients with bone metastases, restricting their prescription in patients with osteopenia or osteoporosis with no evidence of bone destruction diagnosed by X-ray Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) [34]. However, since the high loss in BMD found in this study, it is suggested that the treatment could be implemented in patients with osteopenia and osteoporosis at baseline; while monitoring renal function, as routinely done for patients receiving cisplatin in chemotherapy scheme [35]. This strategy may reduce long-term costs, would impact positively on the quality of life and survival of these women.
A few limitations should be mentioned. Due to the nature of the study design and the fact that the chemotherapy treatment scheme was standardized, it is not possible isolate completely the effect thereof on the measured parameters considered. For this reason, it is unknown the influence of the tumor on BMD changes and its induced catabolic body response. Furthermore, the protective effect of calcium supplementation on demineralization in the femoral neck must be interpreted with caution since supplemented patients who initiated treatment had osteopenia. It is considered that women who begin the chemotherapy scheme with normal BMD calcium supplementation could not have the same effect. One more limitation was the small sample size in this study which confines its generalizability. Therefore, results need to be replicated in larger studies.
Conclusions
This study showed evidence of a significant reduction of BMD in both femoral neck and L2-L4. Due to treatment and menopausal status interaction, bone resorption was higher in premenopausal patients. Also, calcium supplementation exerted a protective effect by reducing the loss of total BMC and femoral neck BMD. The treatment and clinical stage interaction on L2-L4 BMD loss suggested that the bone resorption could be due not only to the antineoplastic drugs, but also to the disease itself, which could have had an effect even before clinical signs such as the bone metastasis and cachexia appeared. However, further studies focused on tumor response at the initial phase of treatment are required to elucidate the extent of malignancy per se.
Abbreviations
- BMC:
-
Bone mineral content
- BMD:
-
Bone mineral density
- CEO:
-
State Oncology Center
- CIAD:
-
Food and Development Research Center
- DXA:
-
Dual X Absorptiometry
References
Ferlay J, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86.
Goss PE, et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol. 2013;14(5):391–436.
Mohar A, et al. Available resources for the treatment of breast cancer in Mexico. Salud Publica Mex. 2009;51:s263–9.
Pacifici R. Estrogen, cytokines, and pathogenesis of postmenopausal osteoporosis. J Bone Miner Res. 1996;11(8):1043–51.
Greenspan SL, et al. Instant vertebral assessment: a noninvasive dual X-ray absorptiometry technique to avoid misclassification and clinical mismanagement of osteoporosis. J Clin Densitom. 2002;4(4):373–80.
Abdel-Maksoud MF, et al. Behavioral risk factors and their relationship to tumor characteristics in Hispanic and non-Hispanic white long-term breast cancer survivors. Breast Cancer Res Treat. 2012;131(1):169–76.
Slattery ML, et al. Body size, weight change, fat distribution and breast cancer risk in Hispanic and non-Hispanic white women. Breast Cancer Res Treat. 2007;102(1):85–101.
Greene FL, Page DL, Fleming ID, et al. AJCC Cancer Staging Manual. 6th ed. New York: Springer-Verlag; 2002.
Shapiro CL, Manola J, Leboff M. Ovarian failure after adjuvant chemotherapy is associated with rapid bone loss in women with early-stage breast cancer. J Clin Oncol. 2001;19(14):3306–11.
Van Poznak C, et al. Prevention of aromatase inhibitor–induced bone loss using risedronate: the SABRE trial. J Clin Oncol. 2010;28(6):967–75.
Delmas P, et al. Bisphosphonate risedronate prevents bone loss in women with artificial menopause due to chemotherapy of breast cancer: a double-blind, placebo-controlled study. J Clin Oncol. 1997;15(3):955–62.
Saarto T, et al. Chemical castration induced by adjuvant cyclophosphamide, methotrexate, and fluorouracil chemotherapy causes rapid bone loss that is reduced by clodronate: a randomized study in premenopausal breast cancer patients. J Clin Oncol. 1997;15(4):1341–7.
Powles T, et al. Randomized, placebo-controlled trial of clodronate in patients with primary operable breast cancer. J Clin Oncol. 2002;20(15):3219–24.
Burstein HJ, et al. American Society of Clinical Oncology clinical practice guideline: Update on adjuvant endocrine therapy for women with hormone receptor–positive breast cancer. J Clin Oncol. 2010;28(23):3784–96. doi:10.1200/JCO.2009.26.3756.
Theriault RL, et al. Breast cancer, version 3.2013. J Natl Compr Cancer Netw. 2013;11(7):753–61.
Baumgartner K, et al. Association of body composition and weight history with breast cancer prognostic markers: divergent pattern for Hispanic and non-Hispanic White women. Am J Epidemiol. 2004;160(11):1087–97.
Prado CM, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008;9(7):629–35.
Roubenoff R. Excess baggage: sarcopenia, obesity, and cancer outcomes. Lancet Oncol. 2008;9(7):605–7.
Manolagas SC, Jilka RL. Bone marrow, cytokines, and bone remodeling. Emerging insights into the pathophysiology of osteoporosis. N Engl J Med. 1995;332(5):305–11.
Marcus R, Feldman D, Kelsey J (eds). Osteoporosis. St. Louis: Elsevier Science & Technology; 2001.
Martin-Millan M, et al. The estrogen receptor-α in osteoclasts mediates the protective effects of estrogens on cancellous but not cortical bone. Mol Endocrinol. 2010;24(2):323–34.
Confavreux C, et al. Estrogen-dependent increase in bone turnover and bone loss in postmenopausal women with breast cancer treated with anastrozole. Prevention with bisphosphonates. Bone. 2007;41(3):346–52.
Coleman RE, et al. Skeletal effects of exemestane on bone-mineral density, bone biomarkers, and fracture incidence in postmenopausal women with early breast cancer participating in the Intergroup Exemestane Study (IES): a randomised controlled study. Lancet Oncol. 2007;8(2):119–27.
Eastell R, et al. Effect of an Aromatase Inhibitor on BMD and Bone Turnover Markers: 2‐Year Results of the Anastrozole, Tamoxifen, Alone or in Combination (ATAC) Trial (18233230). J Bone Miner Res. 2006;21(8):1215–23.
Gonnelli S, et al. Changes in bone turnover and in bone mass in women with breast cancer switched from tamoxifen to exemestane. Bone. 2007;40(1):205–10.
Monroy Cisneros K, et al. Impacto del tratamiento antineoplásico en el estado nutricional en pacientes con cáncer de mama. Nutr Hosp. 2014;30(4):876–82.
Berger NA. Cancer and energy balance, epidemiology and overview. New York: Springer; 2010.
Tisdale MJ. Mechanisms of Cancer Cachexia. Physiological reviews. 2009;89(2):381-410.
Argilés JM, et al. Fisiología de la sarcopenia: Similitudes y diferencias con la caquexia neoplásica. Nutr Hosp. 2006;21:38–45.
Demark-Wahnefried W, et al. Changes in weight, body composition, and factors influencing energy balance among premenopausal breast cancer patients receiving adjuvant chemotherapy. J Clin Oncol. 2001;19(9):2381–9.
Saarto T, et al. Ten-year follow-up of 3 years of oral adjuvant clodronate therapy shows significant prevention of osteoporosis in early-stage breast cancer. J Clin Oncol. 2008;26(26):4289–95.
Hillner BE, et al. American Society of Clinical Oncology 2003 update on the role of bisphosphonates and bone health issues in women with breast cancer. J Clin Oncol. 2003;21(21):4042–57.
Fournier PG, et al. How do bisphosphonates inhibit bone metastasis in vivo. Neoplasia. 2010;12(7):571–8.
Van Poznak CH, et al. American Society of Clinical Oncology executive summary of the clinical practice guideline update on the role of bone-modifying agents in metastatic breast cancer. J Clin Oncol. 2011;29(9):1221–7.
Perry MC, Anderson CM, Doll DC, (eds). Companion handbook to the chemotherapy sourcebook. Lippincott Williams & Wilkins; 2004.
Acknowledgements
The authors acknowledge all breast cancer patients, for participating in this study. The State Centre of Oncology (CEO) and Center for Food Research and Development (CIAD) granted by the facilities. The National Council of Science and Technology (CONACyT) for the scholarship that made the project possible. To QFB Diana Mendoza Bermudez, QB Bertha Pacheco Moreno, M. in C. Orlando Tortoledo Ortiz and M. in C. Ana Cristina Gallegos Aguilar by providing technical support. To Dr. Benjamin Arroyo Acosta and Dr. Ernesto Rivera Claisse for the hospitality and facilities granted.
Funding
The National Council of Science and Technology (CONACyT) through to scholarship that made the project possible.
Availability of data and materials
The informed consent form signed for the patients did not include the availability of data to third party.
Authors’ contributions
MCK participated in study design, collated data, analysis and drafted the manuscript. ERJ interpreted data and statistics, contributed to discussion and drafted the manuscript. VME participated in nutritional and body composition advice; contributed to discussion and drafting the manuscript. GTAG provided medical oncology advice and manuscript edition. MERO made BMD and BMC assay, bone metabolism advice and edited the manuscript. ACI edited the manuscript. AGH participated in study design, acquisition of funding, general supervision, discussion and drafted the manuscript. All authors have read and approved the final version of this manuscript.
Authors’ information
MCK was a Doctoral student in Center for Food Research and Development (CIAD); ERJ is Epidemiologist researcher at CIAD; VME is Nutritional researcher at Sonora University and Emeritus professor at CIAD; GTAG is Medical oncologist at The State Centre of Oncology (CEO); MERO is Researcher on micronutrients metabolism at CIAD; ACI is Associate-Researcher at CIAD and AGH is Researcher and Director of Nutrition Department at CIAD.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
The informed consent form signed for the patients already include the approval to publish their overall data avoiding individual information.
Ethics approval and consent to participate
The protocol was approved by the Research Ethics Committee of the CEO and Ethics Committee of the Research Center for Food and Development (CIAD from the acronym in Spanish). The recruited volunteers were requested to sign an informed consent form.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Monroy-Cisneros, K., Esparza-Romero, J., Valencia, M.E. et al. Antineoplastic treatment effect on bone mineral density in Mexican breast cancer patients. BMC Cancer 16, 860 (2016). https://doi.org/10.1186/s12885-016-2905-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-016-2905-x