
Abstract
Background
The purpose of this observational study was to evaluate feasibility, efficacy results and toxicity observations of capecitabine in routine first line treatment of patients with metastatic colorectal cancer, with particular regard of elderly patients (>75 years of age).
Methods
Patients with colorectal cancer receiving capecitabine as part of their first-line treatment were recorded until detection of disease progression or up to a maximum of 12 cycles on standardized evaluation forms. Additional information on long-term outcomes, progression-free survival, and overall survival were retrieved at two follow-up time points. Obtained data were analyzed with regard to age up to 75 and >75 years of age. There were no specific requirements for patient selection and conduct of therapy, corresponding to the non-interventional nature of the study.
Results
In total, 1249 evaluable patients were enrolled in Germany. The median age of the study population was 74 years (range: 21–99). Capecitabine-based combination was administered in 56 % of patients in the overall population. The median treatment duration was about 5 months. Severe toxicities occurred rarely without any difference regarding age groups. The most common hematological toxicity was anemia. Gastrointestinal side effects and hand-food-syndrome (HFS) were the most frequent non-hematologic toxicities. Overall response rate (ORR) was significantly higher in the patient group <=75 years compared to patients >75 years of age (38 vs. 32 %, p=0.019). Median progression free survival (PFS 9.7 vs. 8.2 months, p=0.00021) and overall survival (OS 31.0 vs. 22.6 months, p<0.0001) was decreased in elderly patients.
Conclusion
Efficacy and tolerability of capecitabine treatment either as single drug or in various combination regimens, as proven in randomized studies, could be confirmed in a clinical routine setting. Patients older than 75 years may derive a relevant benefit by first line capecitabine-based treatment with good tolerability.
Similar content being viewed by others


Background
While, for more than four decades, the treatment of colorectal cancer (CRC) consisted almost exclusively of the fluoropyrimidine 5-fluorouracil (5-FU) (eventually modulated by folinic acid or levamisole), the development of a plethora of new drugs since the 1990s has improved the therapeutic options in this indication. In addition to new agents with a classical cytotoxic mode of action, such as irinotecan and oxaliplatin, “targeted therapies”, such as monoclonal antibodies, tyrosine kinase inhibitors or fusion proteins directed against vascular endothelial growth factors (receptors) (VEGF(R)) or epidermal growth factor receptors (EGFR) have gained increasing importance [1, 2].
Administration of 5-FU, the main chemotherapy backbone in metastatic CRC (mCRC), is confined to either implanted venous access ports or in-patient treatment. Thus, the development of capecitabine, an oral fluoropyrimidine carbamate working as 5-FU prodrug, relevantly facilitated treatment for CRC patients. Capecitabine (Xeloda®) was licensed for the treatment of metastatic colorectal cancer mainly based on two large multicenter studies, both comparing the oral drug with a common 5-FU/leucovorin combination (Mayo regimen) [3, 4]. Following trials could establish the combination with oxaliplatin or irinotecan, and/or bevacizumab although particularly the combination of capecitabine and irinotecan has shown gastrointestinal side effects, which have to be closely monitored [5–10]. Currently, even chemotriplets with capecitabine, irinotecan and oxaliplatin with or without bevacizumab are being evaluated [11, 12]. Despite the long-standing application of capecitabine in the treatment of colorectal cancer, data in elderly patients are still limited.
The purpose of this non-interventional observation study was the acquisition of data on the routine usage of capecitabine, its efficacy and toxicity spectrum in routine clinical practice with particular focus on the benefit in patients >75 years of age.
Methods
The project fulfilled the criteria of a non-interventional study according to the European Community and German legislation, and therefore required neither an ethical committee vote nor informed consent of the patients when the registry was started in 2004 [13]. In order to achieve a representative picture of capecitabine use in Germany, participation was offered to a large variety of office or hospital-based medical oncologists or gastroenterologists. Recruitment was limited to a pre-specified number of cases per investigator. The per patient-documentation fee was independent of the number of cycles documented. To ensure enrolment of a typical advanced CRC population, eligibility criteria were minimized to age ≥18 years, histologically confirmed advanced (metastatic or inoperable, locally advanced or recurrent) colorectal cancer without prior palliative treatment and eligibility for capecitabine treatment based on the summary of product characteristics. Treatment regimen (combination), diagnostics or frequency of examinations were scheduled by the respective treating hospital and office based clinicians. The applied dosage, treatment duration, cycle delays and/or therapy interruptions and eventually concomitant antineoplastic therapy were investigated in addition to demographic and baseline characteristics. Efficacy endpoints were overall response rate (ORR), PFS and OS. Tumor regression and progressive disease was recorded as the best response achieved, based on standard clinical procedures at the discretion of the investigators, without formal requirement of objective remission confirmation. Toxicity data were recorded after every second cycle (6 weeks), based on NCI CTC (National Cancer Institute Common Terminology Criteria for Adverse events) criteria (version 2). The detailed documentation was performed to a maximum of 12 cycles or until progression. Thereafter, key long-term data on overall survival and progression-free survival were retrieved by fax forms at two time points in 2010 and 2012.
The statistical methods were mainly descriptive. Most of the analyses presented were performed separately for the patient subgroups aged ≤75 and >75 years, respectively. Patients beyond 75 years of age are henceforward defined as “older” within this report. Capecitabine dosages were calculated individually, based on the reported absolute dose and the body surface of the patient. To compare baseline characteristics, and the response or toxicity rates in different patient groups, a Mantel-Haenszel test for trend or Fisher’s exact test was applied. PFS was defined from the first day of therapy with capecitabine to disease progression or death from any reason without prior progression. The PFS and OS curves were calculated according to the Kaplan-Meier method [14] and between-group comparisons were performed using the logrank test [15].
Results
Baseline characteristics
Between 2004 and 2011 altogether 1305 German patients were recruited of whom 1249 patients with advanced colorectal cancer were eligible for the evaluation. The majority of patients (60 %) were recruited in the second half of the period (between 2008 and 2011). Table 1 provides a description of the study population and their baseline tumor characteristics. A considerable number of older patients participated in this non-interventional trial shown by a median age of the study population of 74 years. At the start of therapy the ECOG (Eastern Cooperative Oncology Group) performance status was not impaired (grade 0 in 28 %) or only slightly reduced (grade 1 in 52 %) in the majority of patients. Performance status in older patients was limited compared to patients up to the age of 75 years (p <0.0001). In 47 % of patients locoregional disease was present at study entry. Synchronous metastatic disease was reported in 646 patients. In the 541 patients with metachronous metastases the median relapse-free interval, defined as the time between first diagnosis of the disease and first detection of metastases was 1.6 years. Nearly two thirds (64 %) of the patients suffered from liver metastases and 29 % from lung involvement with the latter occurring significantly less frequently in older patients (p = 0.0057). Bone and central nervous system (CNS) lesions, pleural effusion and ascites occured rarely with an incidence of below 5 % each. Almost all patients (89 %) received initial surgery of their primary tumor, interestingly with no differences regarding age. Radiotherapy was applied in 15 % of the patients with a significantly decreasing proportion in older patients (p <0.0001). Overall 252 (30 %) patients received prior chemotherapy for non-metastatic disease (neo-/adjuvant). Chemotherapeutic pretreatment was more common in younger patients with a continuous and significantly decreasing percentage with age (37 % in patients younger than 76 years compared to 19 % in patients beyond 75 years; p <0.0001). Median time between the end of prior chemotherapy and initiation of systemic treatment for advanced disease and thus beginning of the observation period was 1 year. In 27 % of these patients the interval was longer than 2 years.
Treatment
580 patients (46 %) received single agent capecitabine, the other 668 patients (54 %) were treated with capecitabine in combination with one (39 %) or two (15 %) additional drugs (Table 2). The most frequently used concomitant drugs were oxaliplatin (43 %), bevacizumab (36 %) and irinotecan (17 %). Only 27 patients (4 %) received capecitabine in combination with EGFR antibodies. Single agent capecitabine was predominantly administered in the group of patients aged over 75 years (65 %) and in almost three out of four patients older than 85 years (74 %). Notably, the rates of oxaliplatin-based combinations were significantly lower in older patients (only 15 % of patients >75 years; p <0.0001).
The median treatment duration with capecitabine was 5.3 months. Only 8 % of patients received capecitabine for more than 10 months. In general, treatment duration tended to be independent of patients’ age with medians of 5.3 months in both age cohorts. The overall median daily dose of capecitabine was 1727 mg/m2 with only very small difference between the two age groups (1744 mg/m2 for younger and 1702 mg/m2 for elderly patients). For the monotherapy the observed median dose of capecitabine was 1838 mg/m2. As to be expected, the dosage was lower when combination chemotherapy was given (1635 mg/m2), with medians between 1300 and 1777 mg/m2 depending on the type of combination regimen (Additional file 1: Table S1).
Treatment courses were delayed in only 13 % of all cycles, but nevertheless occurred at least once in 54 % of patients. Capecitabine dose reductions were reported in 22 % of all cycles and 45 % of all patients, respectively. In terms of treatment discontinuation, no distinct difference could be observed regarding age whereas dose reduction occurred more often in younger patients, likely related to the higher rate of combination regimen (p = 0.040).
In 663 patients (53 %) the observation was terminated according to the observation plan, either due to progressive disease (58 %) or due to reaching the maximum documentation period of 12 cycles (42 %). In the remaining 580 patients (47 %), reasons for a premature termination of the treatment were side effects (23 %), patient’s wish/non-compliance (15 %) and death due to the underlying disease (11 %). Other reasons (52 %) mainly were an a priori planned number of cycles of less than 12 or the achievement of a good response.
Toxicity
Table 3 shows the hematological and non-hematological adverse events according to age groups (split by median age) and combination vs. monotherapy. The NCI toxicity grade per patient was pre-specified in the observation forms. Regardless of age, severe hematological and non-hematological toxicities (grade 3 or 4) occurred only rarely, despite the high rate of combination regimens applied (54 % of patients). The most common toxicities were gastrointestinal disorders like nausea, diarrhea or vomiting, as well as hand-foot-syndrome (HFS) occurring in 42 % of the patients. Expectedly, oxaliplatin-based compared to irinotecan-based regimen showed different rates of all grade thrombocytopenia (33 % vs. 11 %), diarrhea (40 % vs. 49 %), alopecia (21 % vs. 41 %) and neurological disorders (21 % vs. 11 %), respectively. The proportion of patients affected by HFS increased with the duration of the treatment. In cycles 1 and 2, HFS occurred in only 15 % of the patients, increasing to 27 % in cycles 3 and 4, 32 % in cycles 5 and 6 and finally 39 % in cycles 7 and 8. Despite similar median daily dosage of capecitabine, all grade HFS was more frequent in younger patients (46 %) compared to only 37 % in patients older than 75 years (p = 0.0014). However, the rates of grade 3/4 HFS were similar in both age groups (Table 3).
Treatment efficacy
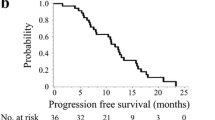
1237 patients were evaluable for objective tumor response (Table 4). 35 % of these achieved an objective remission (complete in 6 % and partial in 29 %), with rates decreasing from 38 % to 32 % in the respective age cohorts (p = 0.019). For the evaluation of the parameters PFS and OS 1245 patients could be included. The Kaplan-Meier estimate of PFS, based on 881 events in 1245 patients (71 %) showed a median of 9.2 months for the whole observation group (Additional file 2: Figure S1). Median PFS in elderly patients was significantly decreased with 8.2 months, compared to 9.7 months in patients up to 75 years of age (p = 0.00021, HR = 1.29, 95 % CI 1.13–1.47) (Fig. 1). In comparison to single drug capecitabine with a median PFS of 8.3 months, a non-significant difference towards an improved PFS with median 9.8 months could be observed for the combination regimen (p = 0.063, HR = 0.88, 95 % CI 0.77–1.01). For 497 (40 %) out of 1245 patients the date of death was documented, resulting in an overall median OS of 26.1 months. In elderly patients OS was significantly decreased (median 22.6 months), compared to 31.0 months in patients up to 75 years of age (p < 0.0001, HR = 1.61, 95 % CI 1.35–1.92) (Fig. 2). In contrast, the comparison of regimen types (single agent vs. combination) showed no differences in terms of OS (25.9 vs. 26.1 months, p = 0.71, HR = 0.97, 95 % CI 0.81–1.15).

Progression-free survival by age group

Overall survival by age group
Patients suffering from HFS of any grade during therapy had a higher response rate (43 %) than patients without this symptom (31 %) (p < 0.0001). Moreover, PFS and OS were significantly prolonged in patients who experienced HFS. The median PFS was 10.6 months vs. 8.2 months (p <0.0001, HR: 0.86 [95 % CI: 0.81–0.93]) and the median OS to 28.8 months vs. 24.2 months (p = 0.00038, HR: 0.85 [95 % CI: 0.77–0.93]) in patients suffering from HFS CTC grade 1–3 compared to those without this symptom.
A similar favorable trend could also be observed in patients who received a capecitabine dose reduction during therapy, likely associated with the occurrence of HFS. The median PFS was 10 months vs. 8.3 months (p = 0.0009, HR: 0.89 [95 % CI: 0.83–0.95]) and the median OS was 28.6 months vs. 23.8 months (p = 0.0026, HR: 0.87 [95 % CI: 0.80–0.95]) in patients who received dose reduction compared to those who did not.
Discussion
The efficacy observed in this observational study is in the same range as previously reported from randomized trials. The reported ORR of 35 % mirrors the results obtained in previous single agent or combination trials, e.g., with oxaliplatin or bevacizumab [6, 9, 16]. The median PFS results observed compare favorably to prior trials, both for the overall as well as in the different subgroups regarding age and combination with other agents. However, these differences may be explained, at least in part, by the presence of an observation bias due to a less stringent re-staging schedule in our routine observation study compared to the randomized trials. With respect to median overall survival, our results compare quite favorably to those of the early single drug registration studies and capecitabine-based doublets [6, 16, 17]. The median OS of 26.1 months observed in our cohort is likely influenced by the observed shift in median OS during the last decades due to the availability of new agents and the increasing integration of locally ablative procedures. In comparison to former registries in first line mCRC e.g., BEAT or BRiTE recruited between 2004 and 2006 showing a median OS of up to 23 months the main recruitment period of this study (60 % of patients recruited between 2008 and 2011) was later and thus reflecting more the current developments of a median OS of about 30 months achieved in current first line trials [18–21]. Furthermore, the patient population seemed to have a favorable prognosis, in terms of a rather high rate of a good ECOG PS (0 or 1) despite the median age of 74 years and the resection of their primary tumor in the vast majority of patients [22]. Besides increased ORR (27 vs. 42 %) and median PFS (8.3 vs. 9.8 months, p = 0.06) comparing single agent and combination regimen, median OS was similar (25.9 vs. 26.1 months, p = 0.71). Combination regimen were more often applied in younger patients (77 % of patients ≤65 years compared to 26 % of patients >85 years) with likely more aggressive disease (e.g., higher rate of poorly differentiated tumors, multiple metastastic sites).
Regarding toxicity, capecitabine-based regimen can be administered without major complications in most patients. The rate of severe toxicities (grade 3 or 4) was below 5 % with respect to all NCI CTC categories in this observational study. Hand-foot-syndrome, which proved to be the dose-limiting toxicity of single drug capecitabine, was reported in somewhat less than half of our patients, but proved to be manageable, with only 3 % of the patients suffering from serious symptoms.
The treatment efficacy was decreased in the elderly subgroup (>75 years), but still remained on a high level with an ORR of 32 %, median PFS of 8.2 months and OS of 22.6 months. Therefore, the overall efficacy results of this large group of elderly patients is within the range as previously reported, considering the relevant number of elderly patients receiving combination treatment [16, 23, 24]. Moreover, tolerability did not seem to be limited in elderly patients with regard to grade 3/4 toxicities. During the last decade treatment approach in elderly patients has significantly changed, whereas early trials evaluated only single agent fluoropyrimidines, combination regimen are currently more frequently administered [25–27]. Elderly patients with a good performance status eligible for clinical phase 3 trials seem to derive a relevant benefit by the addition of further agents as shown in different subgroup analyses [28]. Randomized trials have furthermore established the relevant benefit and tolerability of combination regimen in elderly patients [16, 23, 29]. In order to stratify elderly patients to the different treatment intensities comprehensive geriatric assessment should be applied and is recommended by current guidelines [30].
Besides, capecitabine has been shown to be well tolerated and efficacious in elderly patients in the adjuvant setting as single agent compared to bolus 5FU/LV [31]. In addition, capecitabine (or infusional 5-FU) seems to be the favorable combination partner if an oxaliplatin-based adjuvant treatment is chosen. In contrast to prior data including bolus 5FU based regimen (FLOX), Haller and colleagues recently demonstrated an attenuated but sustained DFS and OS benefit in elderly patients with a modern fluoropyrimidine schedule in combination with oxaliplatin (CAPOX or FOLFOX) [32–34].
Further oral fluoropyrimidines (S-1 or UFT) have been studied in localized or metastatic CRC, showing tolerability and efficacy as single agent or in different combinations (e.g., oxaliplatin – SOX/TEGAFOX regimen or irinotecan – IRIS/TEGAFIRI) without any apparent interaction with age [35–39]. Similar to capecitabine, these oral fluoropyrimidines can be safely combined with bevacizumab in elderly patients [24, 40]. Recently, TAS 102 has shown a significant survival benefit in heavily pretreated mCRC patients with good tolerability and similar OS benefit for patients ≤/>65 years [41].
Dose reductions of capecitabine during treatment does not lead to a poorer long-term outcome, as previously reported [42, 43]. However, due to the observational nature of our study, it is not possible to differentiate the effects of dose modifications from the association with HFS, the development of which seems to be a strong favorable prognostic factor by itself. The occurrence of toxicities like HFS and the consecutive dose reductions likely are clinical markers of the individual effective dosage of capecitabine.
The general characteristics of a non-interventional study focusing on a specific drug inevitably lead to major limitations, particularly in regard of bias in terms of patient selection. An intention-to-treat analysis, was performed with no documented, eligible patient excluded. However, as inclusion of patients into the observational study was not entirely under our control, we cannot completely rule out, that in individual patients with a very short treatment course (e.g., due to early death), the record file was not sent to the documentation centre (although this was clearly not intended or suggested). Moreover, we cannot control or adjust for any selection effect that is associated with the decision to use infusional 5-FU instead of the oral alternative. Possibly, high-risk patients with an immediate need for tumor shrinkage may be underrepresented. Moreover, decisions on treatment intensity will likewise be depending on patients’ age and, thus, subgroup analyses based on these characteristics are biased by this interdependence. Validity and completeness of tumor response and toxicity data is typically lower compared to randomized controlled trials.
Conclusions
Based on the shown efficacy and tolerability, capecitabine is a valid option for the treatment of colorectal cancer without any unequivocally apparent age limit.
Abbreviations
- 5-FU:
-
5-Fluorouracil
- BEAT:
-
Bevacizumab Expanded Access Trial
- BRiTE:
-
Bevacizumab Regimens: Investigation of Treatment Effects and Safety
- CNS:
-
central nervous system
- CRC:
-
colorectal cancer
- ECOG PS:
-
Eastern Cooperative Oncology Group Performance Status
- EGFR:
-
epidermal growth factor receptor
- HFS:
-
hand-foot-syndrome
- mCRC:
-
metastatic colorectal cancer
- NCI CTC:
-
National Cancer Institute Common Terminology Criteria for Adverse events
- ORR:
-
overall response rate
- OS:
-
overall survival
- PFS:
-
progression free survival
- VEGF(R):
-
vascular endothelial growth factor (receptor)
References
Schmoll HJ, Stein A. Colorectal cancer in 2013: Towards improved drugs, combinations and patient selection. Nat Rev Clin Oncol. 2014;11(2):79–80.
Van Cutsem E, Cervantes A, Nordlinger B, Arnold D, on behalf of the EGWG. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-updagger. Ann Oncol. 2014;25 Suppl 3:iii1–9.
Hoff PM, Ansari R, Batist G, Cox J, Kocha W, Kuperminc M, et al. Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol. 2001;19(8):2282–92.
Van Cutsem E, Twelves C, Cassidy J, Allman D, Bajetta E, Boyer M, et al. Oral capecitabine compared with intravenous fluorouracil plus leucovorin in patients with metastatic colorectal cancer: results of a large phase III study. J Clin Oncol. 2001;19(21):4097–106.
Fuchs CS, Marshall J, Mitchell E, Wierzbicki R, Ganju V, Jeffery M, et al. Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. J Clin Oncol. 2007;25(30):4779–86.
Arkenau HT, Arnold D, Cassidy J, Diaz-Rubio E, Douillard JY, Hochster H, et al. Efficacy of oxaliplatin plus capecitabine or infusional fluorouracil/leucovorin in patients with metastatic colorectal cancer: a pooled analysis of randomized trials. J Clin Oncol. 2008;26(36):5910–7.
Koopman M, Antonini NF, Douma J, Wals J, Honkoop AH, Erdkamp FL, et al. Sequential versus combination chemotherapy with capecitabine, irinotecan, and oxaliplatin in advanced colorectal cancer (CAIRO): a phase III randomised controlled trial. Lancet. 2007;370(9582):135–42.
Pectasides D, Papaxoinis G, Kalogeras K, Eleftheraki A, Xanthakis I, Makatsoris T, et al. XELIRI-bevacizumab versus FOLFIRI-bevacizumab as first-line treatment in patients with metastatic colorectal cancer: a Hellenic Cooperative Oncology Group phase III trial with collateral biomarker analysis. BMC Cancer. 2012;12(1):271.
Tebbutt NC, Wilson K, Gebski VJ, Cummins MM, Zannino D, van Hazel GA, et al. Capecitabine, bevacizumab, and mitomycin in first-line treatment of metastatic colorectal cancer: results of the Australasian Gastrointestinal Trials Group Randomized Phase III MAX Study. J Clin Oncol. 2010;28(19):3191–8.
Saltz LB, Clarke S, Diaz-Rubio E, Scheithauer W, Figer A, Wong R, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26(12):2013–9.
Vasile E, Masi G, Fornaro L, Cupini S, Loupakis F, Bursi S, et al. A multicenter phase II study of the combination of oxaliplatin, irinotecan and capecitabine in the first-line treatment of metastatic colorectal cancer. Br J Cancer. 2009;100(11):1720–4.
Di Bartolomeo M, Ciarlo A, Bertolini A, Barni S, Verusio C, Aitini E, et al. Capecitabine, oxaliplatin and irinotecan in combination, with bevacizumab (COI-B regimen) as first-line treatment of patients with advanced colorectal cancer. An Italian Trials of Medical Oncology phase II study. Eur J Cancer. 2015;51:473–81.
Directive 2001/20/EC of the European Parliament and of the Council of 4 April 2001 on the approximation of the laws, regulations and administrative provisions of the Member States relating to the implementation of good clinical practice in the conduct of clinical trials on medicinal products for human use. OJ. 2001;L121:34–44.
Kaplan E, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Ass. 1958;53:457–81.
Peto R, Peto J. Asymptotically efficient rank invariation test procedures (with discussion). J R Stat Soc A. 1972;135:185–206.
Cunningham D, Lang I, Marcuello E, Lorusso V, Ocvirk J, Shin DB, et al. Bevacizumab plus capecitabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX): an open-label, randomised phase 3 trial. Lancet Oncol. 2013;14(11):1077–85.
Van Cutsem E, Hoff PM, Harper P, Bukowski RM, Cunningham D, Dufour P, et al. Oral capecitabine vs intravenous 5-fluorouracil and leucovorin: integrated efficacy data and novel analyses from two large, randomised, phase III trials. Br J Cancer. 2004;90(6):1190–7.
Heinemann V, von Weikersthal LF, Decker T, Kiani A, Vehling-Kaiser U, Al-Batran SE, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(10):1065–75.
Loupakis F, Cremolini C, Masi G, Lonardi S, Zagonel V, Salvatore L, et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med. 2014;371(17):1609–18.
Van Cutsem E, Rivera F, Berry S, Kretzschmar A, Michael M, DiBartolomeo M, et al. Safety and efficacy of first-line bevacizumab with FOLFOX, XELOX, FOLFIRI and fluoropyrimidines in metastatic colorectal cancer: the BEAT study. Ann Oncol. 2009;20(11):1842–7.
Kozloff M, Yood MU, Berlin J, Flynn PJ, Kabbinavar FF, Purdie DM, et al. Clinical outcomes associated with bevacizumab-containing treatment of metastatic colorectal cancer: the BRiTE observational cohort study. Oncologist. 2009;14(9):862–70.
Faron M, Pignon JP, Malka D, Bourredjem A, Douillard JY, Adenis A, et al. Is primary tumour resection associated with survival improvement in patients with colorectal cancer and unresectable synchronous metastases? A pooled analysis of individual data from four randomised trials. Eur J Cancer. 2015;51(2):166–76.
Aparicio T. Bevacizumab + chemotherapy (BEV-CT) versus chemotherapy alone (CT) in elderly patients (pts) with untreated metastatic colorectal cancer (mCRC)—A randomized phase II trial. J Clin Oncol. 2015;33(15S):abstr. 3541.
Yoshida M, Muro K, Tsuji A, Hamamoto Y, Yoshino T, Yoshida K, et al. Combination chemotherapy with bevacizumab and S-1 for elderly patients with metastatic colorectal cancer (BASIC trial). Eur J Cancer. 2015;51(8):935–41.
Comella P, Natale D, Farris A, Gambardella A, Maiorino L, Massidda B, et al. Capecitabine plus oxaliplatin for the first-line treatment of elderly patients with metastatic colorectal carcinoma: final results of the Southern Italy Cooperative Oncology Group Trial 0108. Cancer. 2005;104(2):282–9.
Feliu J, Escudero P, Llosa F, Bolanos M, Vicent JM, Yubero A, et al. Capecitabine as first-line treatment for patients older than 70 years with metastatic colorectal cancer: an oncopaz cooperative group study. J Clin Oncol. 2005;23(13):3104–11.
Feliu J, Salud A, Safont MJ, Garcia-Giron C, Aparicio J, Vera R, et al. First-line bevacizumab and capecitabine-oxaliplatin in elderly patients with mCRC: GEMCAD phase II BECOX study. Br J Cancer. 2014;111(2):241–8.
McCleary NJ, Dotan E, Browner I. Refining the chemotherapy approach for older patients with colon cancer. J Clin Oncol. 2014;32(24):2570–80.
Seymour MT, Thompson LC, Wasan HS, Middleton G, Brewster AE, Shepherd SF, et al. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer (MRC FOCUS2): an open-label, randomised factorial trial. Lancet. 2011;377(9779):1749–59.
Papamichael D, Audisio RA, Glimelius B, de Gramont A, Glynne-Jones R, Haller D, Kohne CH, Rostoft S, Lemmens V, Mitry E et al: Treatment of colorectal cancer in older patients: International Society of Geriatric Oncology (SIOG) consensus recommendations 2013. Ann Oncol 2015, 26(3):463-476.
Twelves C, Scheithauer W, McKendrick J, Seitz JF, Van Hazel G, Wong A, et al. Capecitabine versus 5-fluorouracil/folinic acid as adjuvant therapy for stage III colon cancer: final results from the X-ACT trial with analysis by age and preliminary evidence of a pharmacodynamic marker of efficacy. Ann Oncol. 2012;23(5):1190–7.
Haller DG, O'Connell MJ, Cartwright TH, Twelves CJ, McKenna EF, Sun W, et al. Impact of age and medical comorbidity on adjuvant treatment outcomes for stage III colon cancer: a pooled analysis of individual patient data from four randomized, controlled trials. Ann Oncol. 2015;26:715–24.
McCleary NJ, Meyerhardt JA, Green E, Yothers G, de Gramont A, Van Cutsem E, et al. Impact of Age on the Efficacy of Newer Adjuvant Therapies in Patients With Stage II/III Colon Cancer: Findings From the ACCENT Database. J Clin Oncol. 2013;31(20):2600–6.
Haller D, O'Connell M. Impact of age and medical comorbidity (MC) on adjuvant treatment outcomes for stage III colon cancer (CC): A pooled analysis of individual patient data from four randomized controlled trials. J Clin Oncol. 2012;30:abstr. 3522.
Kim ST, Hong YS, Lim HY, Lee J, Kim TW, Kim KP, et al. S-1 plus oxaliplatin versus capecitabine plus oxaliplatin for the first-line treatment of patients with metastatic colorectal cancer: updated results from a phase 3 trial. BMC Cancer. 2014;14:883.
Yasui H, Muro K, Shimada Y, Tsuji A, Sameshima S, Baba H, et al. A phase 3 non-inferiority study of 5-FU/l-leucovorin/irinotecan (FOLFIRI) versus irinotecan/S-1 (IRIS) as second-line chemotherapy for metastatic colorectal cancer: updated results of the FIRIS study. J Cancer Res Clin Oncol. 2015;141(1):153–60.
Yoshida M, Ishiguro M, Ikejiri K, Mochizuki I, Nakamoto Y, Kinugasa Y, et al. S-1 as adjuvant chemotherapy for stage III colon cancer: a randomized phase III study (ACTS-CC trial). Ann Oncol. 2014;25(9):1743–9.
Bajetta E, Di Bartolomeo M, Buzzoni R, Mariani L, Zilembo N, Ferrario E, et al. Uracil/ftorafur/leucovorin combined with irinotecan (TEGAFIRI) or oxaliplatin (TEGAFOX) as first-line treatment for metastatic colorectal cancer patients: results of randomised phase II study. Br J Cancer. 2007;96(3):439–44.
Lembersky BC, Wieand HS, Petrelli NJ, O'Connell MJ, Colangelo LH, Smith RE, et al. Oral uracil and tegafur plus leucovorin compared with intravenous fluorouracil and leucovorin in stage II and III carcinoma of the colon: results from National Surgical Adjuvant Breast and Bowel Project Protocol C-06. J Clin Oncol. 2006;24(13):2059–64.
Mizushima T, Tamagawa H, Matsuda C, Murata K, Fukunaga M, Ota H, et al. Phase II Study of Oral Tegafur/Uracil and Leucovorin plus Bevacizumab as a First-Line Therapy for Elderly Patients with Advanced or Metastatic Colorectal Cancer. Oncology. 2015;89(3):152–8.
Mayer RJ, Van Cutsem E, Falcone A, Yoshino T, Garcia-Carbonero R, Mizunuma N, et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med. 2015;372(20):1909–19.
Cassidy J, Cox JV. Effective management of patients receiving XELOX: Evaluation of impact of dose modifications on outcome in patients from the NO16966, NO16967, and NO16968 trials. J Clin Oncol. 2011;29(supll 4):abstr. 497.
Stintzing S, Fischer von Weikersthal L, Vehling-Kaiser U, Stauch M, Hass HG, Dietzfelbinger H, et al. Correlation of capecitabine-induced skin toxicity with treatment efficacy in patients with metastatic colorectal cancer: results from the German AIO KRK-0104 trial. Br J Cancer. 2011;105(2):206–11.
Acknowledgments
This work was funded by Roche Pharma AG, Germany. We want to thank all patients who participated in this study, all participating clinicians who included patients, and all the staff engaged in this study.
Preliminary results of this study have been presented at ECCO 15 -- 34th ESMO Multidisciplinary Congress, Berlin, 2009 and the 11th World Conference on Gastrointestinal Cancer, Barcelona, 2011.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
Alexander Stein and Dirk Arnold report grants and personal fees from Roche. Tim Wohlfarth reports personal fees from Roche and stock ownership. All other authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Authors’ contributions
AS, JQ, JKS, TG, BT, ARV, HGH, SSM: recruited patients, collected patient data, interpreted results of analyses, prepared, reviewed and input into each stage of the manuscript; TW: coordinated the study, interpreted results of analyses, prepared, reviewed and input into each stage of the manuscript; AH, AE: performed statistical analyses, interpreted results of analyses, prepared, reviewed and input into each stage of the manuscript; DA: recruited patients, collected patient data, interpreted results of analyses, prepared, reviewed and input into each stage of the manuscript and was the coordinating investigator. All authors read and approved the final manuscript.
Additional files
Additional file 1: Table S1.
Mean daily Capecitabine doses (mg/m2) in terms of regimen types. (DOC 30 kb)
Additional file 2: Figure S1.
Progression-free survival; n = number of patients. (PPT 81 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Stein, A., Quidde, J., Schröder, J.K. et al. Capecitabine in the routine first-line treatment of elderly patients with advanced colorectal cancer - results from a non-interventional observation study. BMC Cancer 16, 82 (2016). https://doi.org/10.1186/s12885-016-2113-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-016-2113-8