
Abstract
Background
Neighborhood stressors (e.g., crime and deprivation) have been associated with adverse pregnancy outcomes including preterm birth and low birth weight. A potential mechanism is disruption of maternal endocrine pathways. While stress hormones (e.g., cortisol) have received much attention, other relevant hormones, including sex steroids, have been overlooked.
Methods
Pregnant women in the Understanding Pregnancy Signals and Infant Development (UPSIDE) study contributed biospecimens, questionnaires, and medical record data (n = 262). In each trimester, maternal serum total testosterone [TT], estrone, estradiol, and estriol were measured using LC/MS-MS and serum free testosterone was measured by equilibrium dialysis. In the third trimester, participants reported on neighborhood stress over the last year through the validated City Stress Inventory. We examined two subscales: 11-item neighborhood disorder (e.g., vacant buildings, crime) and 7-item exposure to violence (personal experiences of violence). Composite scores were calculated and examined categorically (quartile (Q) for neighborhood disorder and any/none for exposure to violence). We fitted linear mixed models examining associations between neighborhood stressors and sex steroid hormones across pregnancy as well as trimester-specific linear regression models, all adjusting for confounders. Secondarily, we stratified by fetal sex. Results are presented as percentage change (∆%) and 95% confidence interval (CI) in hormones.
Results
Most participants (73%) reported one or more exposures to neighborhood disorder; 22% reported any exposure to violence. In adjusted models, neighborhood disorder was associated with higher TT across pregnancy (Q2: %∆= 37.3, 95%CI: 13.2, 66.5; Q3: %∆= 22.2, 95%CI: 1.2, 47.5; and Q4: %∆= 25.7, 95%CI: 1.6, 55.3), with the strongest associations observed in the third trimester (Q2: %∆= 38.0, 95%CI: 10.6, 72.1; Q3: %∆= 29.2, 95%CI: 4.4, 59.9; and Q4: %∆=33.4, 95%CI: 4.9, 69.6). In stratified models, neighborhood disorder was associated with higher TT among women carrying male fetuses (%∆ range: 48.2–84.8). Exposure to violence was not associated with any hormones.
Conclusion
Neighborhood disorder is associated with higher maternal testosterone levels, which may have implications for maternal and child health. Additional research is needed to understand the mechanisms by which neighborhood stress impacts endocrine physiology.
Similar content being viewed by others


Introduction
Extensive evidence demonstrates that the characteristics of the neighborhoods in which people reside can influence their health, including risks of cardiovascular disease, obesity, sleep disorders, anxiety and depression [1,2,3,4]. Studies of neighborhoods and health have additionally informed our understanding of spatial distributions of disease and health disparities. One area of increasing interest is how neighborhood social and physical characteristics may contribute to perinatal health including pregnancy outcomes [5,6,7,8]. For example, in a study of women in Chicago, participants living in neighborhoods with high levels of physical disorder (i.e., abandoned buildings, defaced property, building conditions), had a higher prevalence of hypertensive disorders of pregnancy compared to participants living in neighborhoods with low levels of physical disorder [9]. In a Swedish study, pregnant people living in a severely socially deprived area (defined as having low socioeconomic resources and high rates of unemployment, diverse ethnicities, overcrowding, segregation, criminality, and norm-breaking behaviors) had 90% higher odds of having an extremely preterm birth compared to pregnant people living in an area without deprivation [10]. These studies show similar results across different geographical areas and populations (Chicago vs. Sweden). To date, little research has examined the mechanisms by which neighborhood stressors may disrupt perinatal physiology, leading to adverse birth outcomes [11].
One possibility is that neighborhood features such as crime and disorder are sources of individual-level psychosocial stress, which has been associated with adverse pregnancy outcomes [12, 13]. For example, in pregnant women residing in Philadelphia, positive associations were observed between neighborhood level of crime and perceived stress [14]. Individual-level perceived stress can influence pregnancy physiology, leading to hormonal and neuroendocrine changes that may adversely impact maternal and/or fetal health [15, 16]. While the vast majority of research focuses on the hypothalamic-pituitary-adrenal (HPA) axis as the primary pathway underlying response to stressors [17,18,19], there are fewer studies examining other potentially relevant hormonal pathways, such as the hypothalamic-pituitary-gonadal (HPG) axis, which may also be sensitive to stressors and is known to engage in cross-talk with the HPA axis [20]. For instance, in animal models, prenatal stress disrupts the normal surge of testosterone in the developing male [21,22,23]. While human studies examining the relationship between prenatal stress and hormones produced by the HPG axis are limited, there is evidence linking prenatal stress to anogenital distance (AGD), a biomarker of the prenatal hormonal milieu that is thought to reflect prenatal androgen activity [24]. For example, one study found that couples who reported experiencing more stressful life events in pregnancy had female offspring with a longer, more androgenized AGD compared to couples who reported less stressful life events [25]. Similarly, in a study of Finnish adolescents who gestated during and after the Chernobyl nuclear disaster (considered a stressful life event), exposure to the stressor was associated with increased testosterone levels in female offspring [26]. The current study adds to prior research on environmental sources of stress and sex steroids of the HPG axis.
Given their critical role in pregnancy, including support of fetal growth and maturation, disruptions of maternal sex steroid hormones, such as those due to stressors, may be detrimental to the course of pregnancy. For example, many studies have linked maternal estrogen and testosterone in pregnancy to birth outcomes including birth weight and length [27,28,29,30,31]. Further, reproductive conditions characterized by altered hormone levels such as polycystic ovary syndrome have been associated with birth outcomes including preterm birth and small for gestational age [32,33,34]. Maternal sex steroid hormone levels may also impact a child’s long-term health and behavioral outcomes, as the prenatal hormonal milieu may “program” child development [35,36,37].
Although several prior studies have examined individual level factors impacting maternal sex steroid levels [38, 39], to our knowledge, no prior studies have assessed how neighborhood stressors may impact these important hormones during pregnancy. To that end, the aim of this study is to examine associations between neighborhood stress and maternal sex steroid hormone concentrations (testosterone and estrogens) across pregnancy using data from a longitudinal pregnancy cohort.
Methods
Study overview and population
From December 2015 to April 2019, n = 326 participants were enrolled in the Understanding Pregnancy Signals and Infant Development (UPSIDE) cohort study during their first trimester of pregnancy from outpatient obstetric clinics affiliated with Rochester University Medical Center [40]. Inclusion criteria included: <14 weeks gestation, age 18 or older, singleton pregnancy, no known substance abuse problems or a history of psychotic illness, and the ability to communicate in English. Women with major endocrine disorders (e.g., polycystic ovary syndrome), high-risk pregnancies, or significant obstetric problems at the time of enrollment were excluded. The current analysis was restricted to women with hormone data, at least one complete neighborhood stress subscale (disorder or violence), and complete covariate data. Participants engaged in face-to-face visits during each trimester of their pregnancy, during which biospecimens were collected and questionnaires were administered. The UPSIDE study was approved by the University of Rochester School of Medicine and Dentistry Institutional Review Board and the Rutgers University Institutional Review Board and all participants provided informed consent prior to engaging in study activities.
Measures
Neighborhood stress
Neighborhood stress was measured through a validated City Stress Inventory (CSI) questionnaire that was administered to participants during their third trimester visit [41]. The CSI contains 18 total questions and is divided into 2 subscales- neighborhood disorder (e.g., vacant buildings, crime) which consists of 11 questions and exposure to violence (personal experiences of violence) which contains 7 questions. Sixteen items queried how often different neighborhood-related stressors occurred in the last year, including time while pregnant, with response choices including never, once, a few times, or often. The remaining two items quantified neighborhood disorder/poverty and included answer choices for none, some, about half, or most. Responses were scored on a scale from 1 to 4, with 1 corresponding to never/none and 4 corresponding to often/most. The response values from each subscale were totaled to calculate composite scores for neighborhood disorder (range 11–44) and violence (range 7–28), with lower scores indicating less neighborhood disorder or violence. Given the skewed distribution of responses, we categorized neighborhood disorder scores in quartiles and neighborhood violence as any reported exposure versus none.
Maternal sex steroid hormones
Blood samples were collected in each trimester, then processed and frozen at -80°C. Serum aliquots from each trimester were shipped on dry ice to the Endocrine and Metabolic Research Laboratory at the Lundquist Institute at Harbor-UCLA Medical Center. We examined five hormones- estrone (E1), estradiol (E2), estriol (E3), total testosterone (TT), and free testosterone (FT). E1, E2, E3, and TT were assayed using gold standard liquid chromatography with tandem mass spectrometry (LC-MS/MS) protocol with slight modifications to the runtime and system parameters [36, 42,43,44]. A Shimadzu HPLC system (Columbia, MD) and an Applied Biosystems API5500 LC-MS/MS (Foster City, CA) with a Turbo-Ion-Spray source using positive mode was used for TT assessment. The Shimadzu HPLC system (Columbia, MD) was also used for estrogen assessment, with a triple quadrupole mass spectrometer (API5000 LC-MS/MS, Foster City, CA). FT, the unbound and biologically active fraction of testosterone, was measured through equilibrium dialysis using labeled testosterone [45]. In the first trimester, forty-nine participants had E3 values below the limit of detection (LOD). Observations below the LOD were imputed by assigning the value of LOD/(square root of 2) [46].
Demographic covariates
Demographic information was generally collected at baseline using questionnaires. Continuous variables included gestational age at hormone measurement, maternal age, and early pregnancy body mass index (body mass index [BMI] in kg/m2). BMI was calculated using height and weight from the earliest first trimester visit, because capturing participant’s actual pre-pregnancy BMI is challenging in a pregnancy cohort. However, research shows that this is a suitable substitute, as maternal weight in the first trimester is typically within 1-2 kg of pre-pregnancy weight [47]. Categorical variables included highest maternal education level (less than high school, high school; some college, bachelors; and post graduate degree), insurance status (Medicaid: yes or no), sex of fetus (male or female), and parity (0 or ≥ 1). We additionally included maternal race (Non-Hispanic White, Non-Hispanic Black, other) and maternal ethnicity (Non-Hispanic/Non-Latina or Hispanic/Latina) as proxies for systemic racism which may influence neighborhood of residence and contribute to physiologic dysregulation, including alterations in pregnancy physiology [48,49,50].
Statistical analysis
Summary statistics (mean, standard deviation, median, quartiles, range) were assessed for continuous variables; frequencies and percentages were calculated for categorical variables. Preliminary analysis showed the sex steroid hormones were not normally distributed, so they were natural log transformed for all subsequent analyses. The correlation among hormones was assessed by Pearson correlation analysis. We fitted two sets of models: one with neighborhood disorder as the main exposure and the other with exposure to violence as the main exposure. We first conducted unadjusted linear regression analyses examining associations between the two neighborhood stress exposure measures and the five individual hormone measures in each trimester. Potential confounders were selected a priori from existing literature and directed acyclic graphs (Supplemental Fig. 1). From the set of potential covariates described above, those that appreciably changed the beta estimates by 10% or more from the crude associations were included in final adjusted models. Final multivariable linear regression models were adjusted for maternal age, early pregnancy BMI, gestational age at visit, maternal race, maternal ethnicity, highest maternal education, Medicaid in pregnancy, parity, and infant sex. Our primary models capitalized on the repeat hormone measurements using linear mixed models (LMMs), with random intercepts. To adjust for variation in gestational age at sample collection, models included a fixed effect for neighborhood stressors, a smooth function for gestational age (using gestational age deviation), and a random effect for individual participants within an unstructured correlation matrix since we did not have a priori assumptions for correlation patterns. Secondarily, we fit models examining associations with hormone concentrations in each individual trimester, prioritizing third trimester hormone concentrations which were measured contemporaneously with the neighborhood stress data. Because stress may impact male and female fetuses differently [51], we repeated all analyses above stratifying by fetal sex. Lastly, we conducted sensitivity analyses excluding participants who moved during pregnancy. Results were back-transformed to obtain estimates representing percentage change (∆%) and 95% confidence interval (CI) in hormones. P-values < 0.05 were considered significant. Analyses were performed in SAS 9.4.
Results
Eight participants did not have hormone data, 42 did not have any neighborhood stress data (both the disorder and violence subscales were missing), and 14 did not have complete covariate data bringing the final sample to 262 participants. Participants were on average 29.2 ± 4.6 years old with an early pregnancy BMI of 28.0 ± 7.2 kg/m² (Table 1). The majority were Non-Hispanic White (63.7%), had a college/bachelor’s degree (38.9%), did not use Medicaid during pregnancy (55%), did not relocate during pregnancy (90.8%) and had a prior live birth (67.9%), with 9.9% reporting Hispanic ethnicity. Overall, 73.3% of participants reported any neighborhood disorder and 22.3% reported neighborhood violence.
Median concentrations of maternal serum estrogens increased steadily across pregnancy while TT and FT concentrations were similar across trimesters (Table 2). Among the estrogens, E1 and E2 were strongly correlated (r: 0.81, 0.78, 0.77), E1 and E3 were weakly correlated (r: 0.19, 0.29, 0.18), and E2 and E3 were moderately correlated (r: 0.29, 0.45, 0.41) in trimesters one, two, and three, respectively. Among the androgens, TT and FT were weakly correlated in trimesters 1 (r: -0.13), 2 (r: -0.04), and 3 (r: 0.11). Androgens and estrogens were weakly correlated in all trimesters (Supplemental Fig. 2).
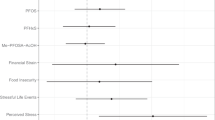
In our primary adjusted LMMs, compared to participants in the lowest quartile of neighborhood disorder, those who experienced greater neighborhood disorder had higher concentrations of TT across pregnancy (quartile 2: %∆= 37.3, 95%CI: 13.2, 66.5; quartile 3: %∆= 22.2, 95%CI: 1.2, 47.5; and quartile 4: %∆= 25.7, 95%CI: 1.6, 55.3) (Fig. 1, Supplemental Table 1). No statistically significant associations were found between neighborhood disorder and the 4 remaining hormones. In LMMs examining exposure to violence, we observed crude associations between exposure to violence and higher TT as well as E2, however associations were attenuated and non-significant after adjustment for covariates; no other hormones were associated with exposure to violence (Fig. 1, Supplemental Table 1).

Adjusted1 LMMs examining neighborhood stress and hormone concentrations in full cohort and by fetal sex. 1Adjusted for trimester, maternal age, early pregnancy BMI, gestational age deviation, fetal sex, parity, maternal race, maternal ethnicity, highest maternal education level, and Medicaid in pregnancy. *Stratified models not adjusted for fetal sex. 2Neighborhood disorder score = 12–13. 3Neighborhood disorder score = 14–17. 4Neighborhood disorder score = 18–42. Neighborhood disorder reference category is Q1 where score = 11. 5Any violence score > 7. Reference is no violence where score = 7. 6Neighborhood disorder (n = 258) and exposure to violence (n = 260). 7Neighborhood disorder (n = 130) and exposure to violence (n = 131). 8Neighborhood disorder (n = 128) and exposure to violence (n = 129)
In LMMs stratified by fetal sex, associations between neighborhood disorder and TT were positive in both groups, but were stronger among women carrying male fetuses (Fig. 1, Supplemental Table 2). For example, compared to participants in the lowest quartile of neighborhood disorder, women carrying male fetuses in the second quartile of neighborhood disorder had 84.8% higher TT (95%CI: 37.8, 148.0), while women carrying female fetuses in the second quartile of disorder had 15.2% higher TT across pregnancy (95%CI: -11.5, 49.9).
As a secondary approach to evaluate differences in associations across pregnancy, we fit linear regression models examining neighborhood stress and maternal sex steroid hormones in each individual trimester. Overall, the strongest associations were detected for neighborhood disorder and third trimester TT concentrations (Table 3). In adjusted models, compared to participants experiencing the lowest levels of neighborhood disorder, women reporting higher levels of neighborhood disorder had higher concentrations of third trimester TT (quartile 2: %∆= 38.0, 95%CI: 10.6, 72.1; quartile 3: %∆= 29.2, 95%CI: 4.4, 59.9; and quartile 4: %∆= 33.4, 95%CI: 4.9, 69.6).
In trimesters one and two, women in the second quartile of neighborhood disorder (score = 12–13) had higher concentrations of TT (trimester 1: %∆= 35.1, 95%CI: 9.6, 66.6; trimester 2: %∆= 40.4, 95%CI: 13.4, 73.9) compared to women with the lowest levels of neighborhood disorder (Supplemental Table 3). No trimester-specific associations between neighborhood disorder and estrogens were observed (Table 3, Supplemental Table 3). In unadjusted models, mothers reporting exposure to violence had significantly higher E2 concentrations in the first and third trimesters (not shown), however associations were attenuated after adjustment for covariates and no additional trimester-specific associations between neighborhood violence and sex steroid concentrations were observed (Table 3, Supplemental Table 3). Results of trimester-specific models stratified by fetal sex were similar to those of the LMMs, with stronger, significant associations between neighborhood disorder and TT observed in all trimesters in participants carrying males compared to females (not shown). For both the adjusted LMMs and trimester-specific linear regression models, associations were robust to the exclusion of the 24 participants (9.2%) who relocated during pregnancy, with the direction and magnitude of the estimates remaining similar (Supplemental Table 4, Supplemental Table 5).
Discussion
In this analysis of neighborhood stressors and sex steroid hormones measured across pregnancy, higher neighborhood disorder was associated with higher maternal testosterone concentrations across pregnancy, these associations were stronger among women carrying male fetuses and grew stronger in late pregnancy. No associations were observed in relation to estrogen concentrations, nor was neighborhood violence associated with any sex steroid hormone concentrations. To our knowledge, this is the first epidemiological study to report that neighborhood-level stressors may affect HPG axis activity during pregnancy.
The association between prenatal stress and sex steroid hormone activity has been demonstrated in numerous animal studies. Consistent with our results, these studies provide evidence that stress is associated with disrupted androgen levels, with notable differences by offspring sex [23, 52]. However these studies generally report that prenatal stress disrupts the male fetus’ testosterone surge [21,22,23], results that are further supported by evidence that compared to controls, the offspring of prenatally stressed dams have a reduced anogenital distance, indicative of less prenatal androgen exposure [53]. In contrast to those results, our study found maternal neighborhood stress was associated with higher testosterone levels, however a key distinction is that animal studies have generally examined testosterone levels in the offspring, while our study captures circulating maternal hormone levels, which reflect production by mother, placenta, and fetus. While a larger body of literature focuses on testosterone, associations between prenatal stress and estrogens have also been noted. Specifically, one study found that rats who were exposed to environmental prenatal stress had lower levels of estradiol compared to control rats [54]. To date, few human studies have examined maternal stress in pregnancy in relation to estrogens. Additional studies are required to provide greater insight into individual-level psychosocial measures and affective symptoms in relation to HPG axis activity during human pregnancy.
Neighborhood-level stressors may contribute to endocrine dysregulation through their impacts on individual-level experiences of stress and affective symptoms. The connection between neighborhood and individual stress has been well-studied both in pregnant and non-pregnant individuals. For example, in a study of 1,309 pregnant women in Philadelphia, those living in a neighborhood with high violent crime, assessed via public violent crime data, had 1.38 times higher odds of having high perceived stress compared to those living in a neighborhood with low violent crime [14]. Additional studies have identified maternal stress as a partial mediator in associations between neighborhood factors and outcomes such as maternal depression and birth weight, demonstrating how neighborhood characteristics may affect maternal and child outcomes through stress [55, 56]. Impacts of neighborhood characteristics on perceived stress and affective symptoms have also been shown in non-pregnant people. For example, in one study adolescents who perceived their neighborhood to be unsafe were 2.4 times more likely to report psychological distress compared to those who perceived their neighborhood to be safe [57]. Similar results have been demonstrated in older adults. In a population of mostly low-income, older African Americans, those who reported their neighborhoods to be safer and more socially cohesive had lower levels of perceived stress [58]. Thus, there is strong evidence to suggest that neighborhoods are important predictors of individual-level measures of mental health.
In pregnant people, androgens are produced by the mother (ovary and adrenal cortex), placenta, and the fetus (gonads and adrenal cortex) [59, 60]. One or more of these physiological sources of androgens may be responsive to stressors, but maternal circulating hormones alone are insufficient to determine the source. One biologically plausible explanation for our results suggesting higher testosterone associated with greater neighborhood disorder is upregulation of adrenal androgen activity. If neighborhood stress results in greater activation of the HPA axis, as suggested by some studies [61, 62], higher adrenocorticotropic hormone (ACTH) production may stimulate synthesis of adrenal androgens, including testosterone and dehydroepiandrosterone [63, 64]. In our study, associations between neighborhood disorder and testosterone strengthened across pregnancy, which may be the result of the changing nature of the HPA axis across gestation resulting from the exponential increase in placental corticotropin releasing hormone (CRH) production as pregnancy progresses [65, 66]. As placental CRH gets released into maternal circulation, it can stimulate ACTH, which in turn may lead to greater testosterone being released in later trimesters [66]. While one might expect higher stress to alter hormone activity in a dose-response manner, we observed that the lower quartiles of neighborhood disorder had stronger associations with testosterone than the higher quartiles. While we are unsure of what may be driving this interesting pattern, one potential explanation is that chronic stress may lead to habituation and blunting of the stress response, as is seen in the case of flattened diurnal cortisol levels following chronic stress or trauma [67]. Given known interactions between the HPA and HPG axes and that in women, 50% of androgens are of adrenal origin [68, 69], it is possible that high chronic stress may also blunt testosterone production in women, while lower levels of stress may result in greater activation.
We also noted that the relationship between neighborhood disorder and testosterone levels were stronger in mothers carrying male fetuses. During gestation, the fetal testes are a major source of testosterone production [70] and the fetal testosterone surge is largely responsible for sexual differentiation [71]. The extent to which fetal testicular testosterone production is reflected in maternal circulating concentrations is unclear; some studies have shown differences in maternal testosterone by fetal sex, while others have not [72, 73]. Some evidence from animal models suggests that maternal stress may dampen testosterone production in the fetal testes [21], while our results may be reflective of heightened testicular testosterone production given the observed differences by fetal sex in stratified models. Additionally, other human studies have shown evidence that male fetuses may be more sensitive to fetal insults. For example, a study in the Philippines found that maternal evening cortisol levels was a significant predictor of birth weight for male, but not female, offspring [74]. However, a study in Israel showed that female fetuses were more sensitive to prenatal stress in relation to birth outcomes [75]. Our results support previous research demonstrating increased sensitivity among male fetuses, as we show that women carrying male fetuses have stronger associations between neighborhood disorder and maternal testosterone than women carrying female fetuses. Lacking technologies to assess human fetal hormone activity in utero for research purposes, future research on maternal stressors and androgen-sensitive endpoints, such as anogenital distance, may shed light on this issue.
Better understanding the potential mechanisms by which maternal stressors (on both the individual and neighborhood levels) impact pregnancy physiology is critical as previous literature suggests that maternal stress may lead to adverse birth outcomes such as low birth weight and preterm birth [56, 76]. For example, a study by Gilles et al., used a composite measure of 6 different psychological questionnaires to measure prenatal stress during the third trimester and found that maternal prenatal stress was associated with a significant reduction in birth weight (− 217 g), birth length (− 1.2 cm), and head circumference (− 0.8 cm) [77]. Another study observed that compared to women who gave birth at term, women who had a preterm birth were 2.15 times more likely to have experienced maternal stress during pregnancy [78]. Additionally, neighborhood characteristics are associated with adverse pregnancy outcomes. Masi et al., used census tract level data to measure neighborhood economic disadvantage and violent crime rates and found they were each associated with increased odds of low birth weight for White, Black, and Hispanic children. The impact of neighborhood characteristics also varied by the racial composition of the census tract, as economic disadvantage and violent crime rates both increased as the proportion of Black and Hispanic residents increased [79]. Neighborhood economic disadvantage has also been associated with preterm birth. For example, Black women living in a wealthier census tract had a reduced risk of preterm birth compared to Black women living in a poorer census tract [80]. Similarly, research shows that residing in a neighborhood with favorable conditions (determined by social, environmental, and educational factors) is positively associated with birth length and weight [81]. An additional mechanism to consider is epigenetic modifications. Research shows that prenatal neighborhood conditions including poverty, public assistance, and healthy food deficiency are associated with epigenetic changes such as gestational epigenetic age deceleration [82]. Stress has also been associated with epigenetic alteration, as a meta-analysis found that maternal stress was correlated with DNA methylation [83]. Overall, maternal stress and neighborhood characteristics have an impact in population health and this impact may have long-term consequences particularly for in utero exposures. Some evidence from non-pregnant women suggests that interventions to lower stress may also lower testosterone levels [84] and in non-pregnant women, neighborhood characteristics such as increased walkability have also been associated with reduced testosterone levels [85]. Implications of altered prenatal testosterone activity on perinatal outcomes remain unknown and need further study.
In this first study to examine the association between neighborhood stress and maternal sex steroid hormone levels, an important strength was the measurement of maternal hormone levels at each trimester, which enabled us to examine the associations across pregnancy as well as within each trimester. Additionally, hormone analysis was done using gold standard of LC/MS-MS and equilibrium dialysis for free testosterone. Most studies to date have used older, less sensitive immunoassay techniques, however LC/MS-MS is essential for measuring androgens in pregnancy given their low concentrations as well as the potential for cross-reactivity with other steroids in immunoassay platforms [86,87,88]. Another strength was our use of the validated CSI questionnaire to assess neighborhood stressors. Maternal perceptions of neighborhood stress (such as those measured by the CSI) may be informative when considering impacts on maternal physiology. Our study sample was relatively diverse in socioeconomic status (e.g., participant’s education ranged from high school to postgraduate) and reflected women living in a range of Upstate, NY neighborhoods including urban, suburban, and even rural areas. At the same time, we note some limitations. Neighborhood stress was measured at a single time point in the third trimester, while maternal hormones were measured in the first, second, and third trimester. However, questions on the City Stress Inventory referred to neighborhood environment in the prior year. Additionally, like other research indicating that most women do not move during pregnancy [89], only 24 (9.2%) of our sample reported relocating during pregnancy and sensitivity analyses excluding these participants showed similar results, demonstrating the robustness of our findings. Nevertheless, aside from the models examining neighborhood stress and third trimester hormones, we cannot establish causality due to the timing of the hormone measurements preceding the exposure measurement. Another limitation of our study is that a small number of participants reported exposure to violence, which may have affected our power to examine this association. It is possible that an association might have been detected if there was a larger sample with more exposure to violence. Similarly, due to smaller samples in some strata, we did not examine associations by race/ethnicity or socioeconomic strata and it is possible that the impact of neighborhoods on pregnancy physiology may differ by sociodemographic factors. Additional work in large, diverse samples is warranted. Finally, no objective measures of stress such as crime data were used, but would complement our self-reported neighborhood data.
Conclusion
Our findings suggest that greater exposure to neighborhood disorder is associated with higher levels of testosterone across pregnancy, particularly among mothers carrying male fetuses. Our findings are relevant to perinatal outcomes given evidence linking sex steroid dysregulation and pregnancy complications [90], adverse birth outcomes [28], and adverse long-term child health outcomes [91]. Additional work is needed to replicate these findings in large, diverse populations with higher exposure to neighborhood disorder and violence. Additionally, there is a need for more research on the impact of neighborhood stress on individual-level stress measures in pregnancy as well as on the interactions between HPA and HPG axis activity in the maternal-placental-fetal unit.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available because this is an ongoing active birth cohort, but are available from the corresponding author on reasonable request.
Abbreviations
- ACTH:
-
Adrenocorticotropin hormone
- AGD:
-
Anogenital distance
- BMI:
-
Body Mass Index
- CRH:
-
Corticotropin releasing hormone
- CSI:
-
City Stress Inventory
- E1:
-
Estrone
- E2:
-
Estradiol
- E3:
-
Estriol
- FT:
-
Free Testosterone
- HPA:
-
Hypothalamic-pituitary-adrenal axis
- HPG:
-
Hypothalamic–pituitary–gonadal axis
- LMM:
-
Linear mixed models
- LOD:
-
Limit of detection
- TT:
-
Total Testosterone
References
Letarte L, Samadoulougou S, McKay R, Quesnel-Vallée A, Waygood EOD, Lebel A. Neighborhood deprivation and obesity: sex-specific effects of cross-sectional, cumulative and residential trajectory indicators. Soc Sci Med. 2022;306:115049.
Pereira G, Foster S, Martin K, Christian H, Boruff BJ, Knuiman M, et al. The association between neighborhood greenness and cardiovascular disease: an observational study. BMC Public Health. 2012;12(1):466.
Nahmod NG, Master L, McClintock HF, Hale L, Buxton OM. Neighborhood disadvantage is Associated with Lower Quality Sleep and more variability in Sleep Duration among Urban Adolescents. J Urb Health. 2022;99(1):102–15.
Thompson S, Ohlsson H, Khoshnood A, Sundquist J, Sundquist K. Neighbourhood crime and major depression in Sweden: a national cohort study. Health Place. 2022;78:102922.
Ncube CN, Enquobahrie DA, Albert SM, Herrick AL, Burke JG. Association of neighborhood context with offspring risk of preterm birth and low birthweight: a systematic review and meta-analysis of population-based studies. Soc Sci Med. 2016;153:156–64.
Vos AA, Posthumus AG, Bonsel GJ, Steegers EA, Denktaş S. Deprived neighborhoods and adverse perinatal outcome: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2014;93(8):727–40.
Matoba N, Reina M, Prachand N, Davis MM, Collins JW. Neighborhood Gun Violence and Birth Outcomes in Chicago. Matern Child Health J. 2019;23(9):1251–9.
Martenies SE, Zhang M, Corrigan AE, Kvit A, Shields T, Wheaton W, et al. Associations between combined exposure to environmental hazards and social stressors at the neighborhood level and individual perinatal outcomes in the ECHO-wide cohort. Health Place. 2022;76:102858.
Mayne SL, Pellissier BF, Kershaw KN. Neighborhood Physical disorder and adverse pregnancy outcomes among women in Chicago: a cross-sectional analysis of Electronic Health Record Data. J Urban Health. 2019;96(6):823–34.
Hesselman S, Wikström AK, Skalkidou A, Sundström-Poromaa I, Wikman A. Neighborhood deprivation and adverse perinatal outcomes in Sweden: a population-based register study. Acta Obstet Gynecol Scand. 2019;98(8):1004–13.
Meng G, Thompson ME, Hall GB. Pathways of neighbourhood-level socio-economic determinants of adverse birth outcomes. Int J Health Geogr. 2013;12(1):32.
Giurgescu C, Zenk SN, Templin TN, Engeland CG, Kavanaugh K, Misra DP. The impact of Neighborhood Conditions and Psychological Distress on Preterm Birth in African-American Women. Public Health Nurs. 2017;34(3):256–66.
Cutrona CE, Russell DW, Hessling RM, Brown PA, Murry V. Direct and moderating effects of community context on the psychological well-being of african american women. J Pers Soc Psychol. 2000;79(6):1088–101.
Shannon MM, Clougherty JE, McCarthy C, Elovitz MA, Nguemeni Tiako MJ, Melly SJ et al. Neighborhood violent crime and perceived stress in pregnancy. Int J Environ Res Public Health. 2020;17(15).
Hobel C, Culhane J. Role of psychosocial and nutritional stress on poor pregnancy outcome. J Nutr. 2003;133(5 Suppl 2):1709s–17s.
Dunkel Schetter C. Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Annu Rev Psychol. 2011;62:531–58.
Valsamakis G, Papatheodorou DC, Chalarakis N, Vrachnis N, Sidiropoulou EJ, Manolikaki M, et al. In pregnancy increased maternal STAI trait stress score shows decreased insulin sensitivity and increased stress hormones. Psychoneuroendocrinology. 2017;84:11–6.
Schreier HMC, Bosquet Enlow M, Ritz T, Coull BA, Gennings C, Wright RO, et al. Lifetime exposure to traumatic and other stressful life events and hair cortisol in a multi-racial/ethnic sample of pregnant women. Stress. 2016;19(1):45–52.
Murphy HR, Gu Y, Wu Q, Brunner J, Panisch LS, Best M, et al. Prenatal diurnal cortisol: normative patterns and associations with affective symptoms and stress. Psychoneuroendocrinology. 2022;143:105856.
Oyola MG, Handa RJ. Hypothalamic-pituitary-adrenal and hypothalamic-pituitary-gonadal axes: sex differences in regulation of stress responsivity. Stress. 2017;20(5):476–94.
Pallarés ME, Adrover E, Baier CJ, Bourguignon NS, Monteleone MC, Brocco MA, et al. Prenatal maternal restraint stress exposure alters the reproductive hormone profile and testis development of the rat male offspring. Stress. 2013;16(4):429–40.
Kemme K, Kaiser S, Sachser N. Prenatal maternal programming determines testosterone response during social challenge. Horm Behav. 2007;51(3):387–94.
Ward IL, Weisz J. Differential Effects of maternal stress on circulating levels of corticosterone, progesterone, and testosterone in male and female rat fetuses and their Mothers*. Endocrinology. 1984;114(5):1635–44.
Dean A, Sharpe RM. Clinical review: anogenital distance or digit length ratio as measures of fetal androgen exposure: relationship to male reproductive development and its disorders. J Clin Endocrinol Metab. 2013;98(6):2230–8.
Barrett ES, Parlett LE, Sathyanarayana S, Liu F, Redmon JB, Wang C, et al. Prenatal exposure to stressful life events is associated with masculinized anogenital distance (AGD) in female infants. Physiol Behav. 2013;114–115:14–20.
Huizink AC, Bartels M, Rose RJ, Pulkkinen L, Eriksson CJP, Kaprio J. Chernobyl exposure as stressor during pregnancy and hormone levels in adolescent offspring. J Epidemiol Commun Health. 2008;62(4):e5.
Noyola-Martínez N, Halhali A, Barrera D. Steroid hormones and pregnancy. Gynecol Endocrinol. 2019;35(5):376–84.
Carlsen SM, Jacobsen G, Romundstad P. Maternal testosterone levels during pregnancy are associated with offspring size at birth. Eur J Endocrinol. 2006;155(2):365–70.
Lagiou P, Samoli E, Hsieh CC, Lagiou A, Xu B, Yu GP, et al. Maternal and cord blood hormones in relation to birth size. Eur J Epidemiol. 2014;29(5):343–51.
Voegtline KM, Costigan KA, Kivlighan KT, Henderson JL, DiPietro JA. Sex-specific associations of maternal prenatal testosterone levels with birth weight and weight gain in infancy. J Dev Orig Health Dis. 2013;4(4):280–4.
Settiyanan T, Wanapirak C, Sirichotiyakul S, Tongprasert F, Srisupundit K, Luewan S, et al. Association between isolated abnormal levels of maternal serum unconjugated estriol in the second trimester and adverse pregnancy outcomes. J Matern Fetal Neonatal Med. 2016;29(13):2093–7.
Roos N, Kieler H, Sahlin L, Ekman-Ordeberg G, Falconer H, Stephansson O. Risk of adverse pregnancy outcomes in women with polycystic ovary syndrome: population based cohort study. BMJ. 2011;343:d6309.
Valgeirsdottir H, Sundström Poromaa I, Kunovac Kallak T, Vanky E, Akhter T, Roos N, et al. Polycystic ovary syndrome and extremely preterm birth: a nationwide register-based study. PLoS ONE. 2021;16(2):e0246743.
Sir-Petermann T, Hitchsfeld C, Maliqueo M, Codner E, Echiburú Br, Gazitúa R, et al. Birth weight in offspring of mothers with polycystic ovarian syndrome. Hum Reprod. 2005;20(8):2122–6.
Spencer D, Pasterski V, Neufeld SAS, Glover V, O’Connor TG, Hindmarsh PC, et al. Prenatal androgen exposure and children’s gender-typed behavior and toy and playmate preferences. Horm Behav. 2021;127:104889.
Day DB, Collett BR, Barrett ES, Bush NR, Swan SH, Wang C, et al. Prenatal sex hormones and behavioral outcomes in children. Psychoneuroendocrinology. 2020;113:104547.
Cherskov A, Pohl A, Allison C, Zhang H, Payne RA, Baron-Cohen S. Polycystic ovary syndrome and autism: a test of the prenatal sex steroid theory. Translational Psychiatry. 2018;8(1):136.
Toriola AT, Vääräsmäki M, Lehtinen M, Zeleniuch-Jacquotte A, Lundin E, Rodgers KG, et al. Determinants of maternal sex steroids during the first half of pregnancy. Obstet Gynecol. 2011;118(5):1029–36.
Barrett ES, Mbowe O, Thurston SW, Butts S, Wang C, Nguyen R, et al. Predictors of steroid hormone concentrations in early pregnancy: results from a Multi-Center Cohort. Matern Child Health J. 2019;23(3):397–407.
O’Connor T, Best M, Brunner J, Ciesla AA, Cunning A, Kapula N, et al. Cohort profile: understanding pregnancy signals and Infant Development (UPSIDE): a pregnancy cohort study on prenatal exposure mechanisms for child health. BMJ Open. 2021;11(4):e044798.
Ewart CK, Suchday S. Discovering how urban poverty and violence affect health: development and validation of a Neighborhood stress index. Health Psychol. 2002;21(3):254–62.
Sathyanarayana S, Butts S, Wang C, Barrett E, Nguyen R, Schwartz SM, et al. Early prenatal Phthalate exposure, sex steroid hormones, and birth outcomes. J Clin Endocrinol Metab. 2017;102(6):1870–8.
Shiraishi S, Lee PW, Leung A, Goh VH, Swerdloff RS, Wang C. Simultaneous measurement of serum testosterone and dihydrotestosterone by liquid chromatography-tandem mass spectrometry. Clin Chem. 2008;54(11):1855–63.
Rivera-Núñez Z, Kinkade CW, Khoury L, Brunner J, Murphy H, Wang C, et al. Prenatal perfluoroalkyl substances exposure and maternal sex steroid hormones across pregnancy. Environ Res. 2023;220:115233.
Qoubaitary A, Meriggiola C, Ng CM, Lumbreras L, Cerpolini S, Pelusi G, et al. Pharmacokinetics of testosterone undecanoate injected alone or in combination with norethisterone enanthate in healthy men. J Androl. 2006;27(6):853–67.
Hornung RW, Reed LD. Estimation of average concentration in the Presence of nondetectable values. Appl Occup Environ Hyg. 1990;5(1):46–51.
Institute of Medicine, Guidelines NRCCtRIPW. The National Academies Collection: Reports funded by National Institutes of Health. In: Rasmussen KM, Yaktine AL, editors. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington (DC): National Academies Press (US) Copyright © 2009, National Academy of Sciences.; 2009.
Geronimus AT. The weathering hypothesis and the health of african-american women and infants: evidence and speculations. Ethn Dis. 1992;2(3):207–21.
Ioannidis JPA, Powe NR, Yancy C. Recalibrating the Use of Race in Medical Research. JAMA. 2021;325(7):623–4.
Chambers BD, Arabia SE, Arega HA, Altman MR, Berkowitz R, Feuer SK, et al. Exposures to structural racism and racial discrimination among pregnant and early post-partum black women living in Oakland, California. Stress Health. 2020;36(2):213–9.
Sutherland S, Brunwasser SM. Sex differences in vulnerability to prenatal stress: a review of the recent literature. Curr Psychiatry Rep. 2018;20(11):102.
Ward IL, Weisz J. Maternal stress alters plasma testosterone in fetal males. Science. 1980;207(4428):328–9.
Desaulniers AT, Lamberson WR, Safranski TJ. Prenatal heat stress reduces male anogenital distance at birth and adult testis size, which are rescued by concurrent maternal Artemisia absinthium consumption. J Therm Biol. 2016;57:84–91.
Del Cerro MC, Ortega E, Gómez F, Segovia S, Pérez-Laso C. Environmental prenatal stress eliminates brain and maternal behavioral sex differences and alters hormone levels in female rats. Horm Behav. 2015;73:142–7.
Giurgescu C, Misra DP, Sealy-Jefferson S, Caldwell CH, Templin TN, Slaughter- Acey JC, et al. The impact of neighborhood quality, perceived stress, and social support on depressive symptoms during pregnancy in african american women. Soc Sci Med. 2015;130:172–80.
Nkansah-Amankra S, Luchok KJ, Hussey JR, Watkins K, Liu X. Effects of maternal stress on low Birth Weight and Preterm Birth Outcomes across neighborhoods of South Carolina, 2000–2003. Matern Child Health J. 2010;14(2):215–26.
Goldman-Mellor S, Margerison-Zilko C, Allen K, Cerda M. Perceived and objectively-measured Neighborhood Violence and adolescent psychological distress. J Urban Health. 2016;93(5):758–69.
Henderson H, Child S, Moore S, Moore JB, Kaczynski AT. The influence of Neighborhood Aesthetics, Safety, and Social Cohesion on Perceived stress in Disadvantaged Communities. Am J Community Psychol. 2016;58(1–2):80–8.
Makieva S, Saunders PT, Norman JE. Androgens in pregnancy: roles in parturition. Hum Reprod Update. 2014;20(4):542–59.
Parsons AM, Bouma GJ. A Potential Role and Contribution of Androgens in Placental Development and Pregnancy. Life (Basel). 2021;11(7).
Karb RA, Elliott MR, Dowd JB, Morenoff JD. Neighborhood-level stressors, social support, and diurnal patterns of cortisol: The Chicago Community Adult Health Study. Social Science & Medicine. 2012;75(6):1038-47.
Do DP, Diez Roux AV, Hajat A, Auchincloss AH, Merkin SS, Ranjit N, et al. Circadian rhythm of cortisol and neighborhood characteristics in a population-based sample: the multi-ethnic study of atherosclerosis. Health Place. 2011;17(2):625–32.
Sheng JA, Bales NJ, Myers SA, Bautista AI, Roueinfar M, Hale TM et al. The hypothalamic-pituitary-adrenal Axis: development, programming actions of hormones, and maternal-fetal interactions. Front Behav Neurosci. 2021;14.
White BA, Harrison JR, Mehlmann LM. Endocrine and Reproductive Physiology. 5 ed2019.
Lindsay JR, Nieman LK. The hypothalamic-pituitary-adrenal Axis in pregnancy: Challenges in Disease Detection and Treatment. Endocr Rev. 2005;26(6):775–99.
Gangestad SW, Caldwell Hooper AE, Eaton MA. On the function of placental corticotropin-releasing hormone: a role in maternal-fetal conflicts over blood glucose concentrations. Biol Rev Camb Philos Soc. 2012;87(4):856–73.
Herman JP, McKlveen JM, Ghosal S, Kopp B, Wulsin A, Makinson R, et al. Regulation of the hypothalamic-pituitary-adrenocortical stress response. Compr Physiol. 2016;6(2):603–21.
Toufexis D, Rivarola MA, Lara H, Viau V. Stress and the reproductive axis. J Neuroendocrinol. 2014;26(9):573–86.
Burger HG. Androgen production in women. Fertil Steril. 2002;77:3–5.
Beharie N, Jessell L, Osuji H, McKay MM. The Association between Shelter Rules and Psychosocial Outcomes among Homeless Youth Residing in Family Shelters. Fam Soc. 2017;98(2):113–20.
Nassar GN, Leslie SW, Physiology. Testosterone. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2022. StatPearls Publishing LLC.; 2022.
Glass AR, Klein T. Changes in maternal serum total and free androgen levels in early pregnancy: lack of correlation with fetal sex. Am J Obstet Gynecol. 1981;140(6):656–60.
Meulenberg PM, Hofman JA. Maternal testosterone and fetal sex. J Steroid Biochem Mol Biol. 1991;39(1):51–4.
Thayer ZM, Feranil AB, Kuzawa CW. Maternal cortisol disproportionately impacts fetal growth in male offspring: evidence from the Philippines. Am J Hum Biol. 2012;24(1):1–4.
Wainstock T, Shoham-Vardi I, Glasser S, Anteby E, Lerner-Geva L. Fetal sex modifies effects of prenatal stress exposure and adverse birth outcomes. Stress. 2015;18(1):49–56.
Hobel CJ, Goldstein A, Barrett ES. Psychosocial stress and pregnancy outcome. Clin Obstet Gynecol. 2008;51(2):333–48.
Gilles M, Otto H, Wolf IAC, Scharnholz B, Peus V, Schredl M, et al. Maternal hypothalamus-pituitary-adrenal (HPA) system activity and stress during pregnancy: Effects on gestational age and infant’s anthropometric measures at birth. Psychoneuroendocrinology. 2018;94:152–61.
Lilliecreutz C, Larén J, Sydsjö G, Josefsson A. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth. 2016;16:5.
Masi CM, Hawkley LC, Piotrowski ZH, Pickett KE. Neighborhood economic disadvantage, violent crime, group density, and pregnancy outcomes in a diverse, urban population. Soc Sci Med. 2007;65(12):2440–57.
Kaufman JS, Dole N, Savitz DA, Herring AH. Modeling community-level effects on preterm birth. Ann Epidemiol. 2003;13(5):377–84.
Appleton AA, Lin B, Holdsworth EA, Feingold BJ, Schell LM. Prenatal exposure to favorable Social and Environmental Neighborhood Conditions is Associated with healthy pregnancy and infant outcomes. Int J Environ Res Public Health. 2021;18(11).
Appleton AA, Lin B, Kennedy EM, Holdsworth EA. Maternal depression and adverse neighbourhood conditions during pregnancy are associated with gestational epigenetic age deceleration. Epigenetics. 2022;17(13):1905–19.
Palma-Gudiel H, Córdova-Palomera A, Eixarch E, Deuschle M, Fañanás L. Maternal psychosocial stress during pregnancy alters the epigenetic signature of the glucocorticoid receptor gene promoter in their offspring: a meta-analysis. Epigenetics. 2015;10(10):893–902.
Cruess DG, Antoni MH, Kumar M, McGregor B, Alferi S, Boyers AE, et al. Effects of stress management on testosterone levels in women with early-stage breast cancer. Int J Behav Med. 2001;8:194–207.
India-Aldana S, Rundle AG, Clendenen TV, Quinn JW, Arslan AA, Afanasyeva Y, et al. Neighborhood walkability and sex steroid hormone levels in women. Environ Res. 2022;215:114285.
Middle JG. Dehydroepiandrostenedione sulphate interferes in many direct immunoassays for testosterone. Ann Clin Biochem. 2007;44(Pt 2):173–7.
Krasowski MD, Drees D, Morris CS, Maakestad J, Blau JL, Ekins S. Cross-reactivity of steroid hormone immunoassays: clinical significance and two-dimensional molecular similarity prediction. BMC Clin Pathol. 2014;14:33.
Tejada F, Cremades A, Monserrat F, Peñafiel R. Interference of the antihormone RU486 in the determination of testosterone and estradiol by enzyme-immunoassay. Clin Chim Acta. 1998;275(1):63–9.
Bell ML, Belanger K. Review of research on residential mobility during pregnancy: consequences for assessment of prenatal environmental exposures. J Expo Sci Environ Epidemiol. 2012;22(5):429–38.
Troisi R, Potischman N, Roberts JM, Ness R, Crombleholme W, Lykins D, et al. Maternal serum oestrogen and androgen concentrations in preeclamptic and uncomplicated pregnancies. Int J Epidemiol. 2003;32(3):455–60.
Kosidou K, Dalman C, Widman L, Arver S, Lee BK, Magnusson C, et al. Maternal polycystic ovary syndrome and the risk of autism spectrum disorders in the offspring: a population-based nationwide study in Sweden. Mol Psychiatry. 2016;21(10):1441–8.
Acknowledgements
We are very grateful to all UPSIDE study participants and their families. The authors also thank the nurses and research staff who participated in cohort recruitment and follow up.
Funding
This work was supported by the National Institutes of Health (NHI; grant number R01HD083369. Additional support was provided from NIEHS (grant number P30ES005022) and the Environmental influences on Child Health Outcomes (ECHO) program (grant numbers UH3OD0223349 and UG3OD0223349), the Wynne Family Center, and National Institutes of Health/National Center for Advancing Translational Sciences (UL1TR001881). ECHO is a nationwide research program supported by the NIH, Office of the Director to enhance child health. The first author received support from the 21PHirst Century Pre-Doctoral Fellowship, Rutgers School of Public Health.
Author information
Authors and Affiliations
Contributions
Megan Hansel: Methodology, Formal analysis, Data visualization, Writing- original draft; Hannah R. Murphy: Writing- review and editing; Jessica Brunner: Data curation, Project administration, Writing – review & editing; Christina Wang: Hormone analytical protocol – development, preparation and quantification, Writing – review & editing; Richard K. Miller: Funding acquisition, Investigation, Writing – review & editing; Thomas G. O’Connor: Funding acquisition, Investigation, Writing – review & editing; Emily S. Barrett: Conceptualization, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft; Zorimar Rivera-Núñez: Methodology, Supervision, Writing – original draft. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This research was performed in accordance with the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations. The UPSIDE study was approved by the University of Rochester School of Medicine and Dentistry Institutional Review Board and the Rutgers University Institutional Review Board and all participants provided informed consent prior to engaging in study activities (Protocol # 20160001514).
Minor participation
Although the UPSIDE study followed the infants born from the cohort, the current analysis does not include data from these children.
Consent for publication
Not appliable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hansel, M.C., Murphy, H.R., Brunner, J. et al. Associations between neighborhood stress and maternal sex steroid hormones in pregnancy. BMC Pregnancy Childbirth 23, 730 (2023). https://doi.org/10.1186/s12884-023-06043-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-06043-0