
Abstract
Background
Per- and polyfluoroalkyl substances (PFAS) are persistent synthetic chemicals and are commonly found in everyday items. PFAS have been linked to disrupting glucose homeostasis, however, whether they are associated with gestational diabetes mellitus (GDM) risk remains inconclusive. We examined prospective associations of PFAS concentrations measured twice in pregnancy with GDM risk.
Methods
In the PETALS pregnancy cohort, a nested case–control study which included 41 GDM cases and 87 controls was conducted. PFAS analytes were measured in blood serum collected in both early and mid-pregnancy (mean [SD]: 13.9 [2.2] and 20.2 [2.2] gestational weeks, respectively), with cumulative exposure calculated by the area-under-the-curve (AUC) to integrate both the PFAS concentration and the timing of the exposure. Individual adjusted weighted unconditional logistic regression models examined seven PFAS in association with GDM risk. P-values were corrected using the false-discovery-rate (FDR). Mixture models were analyzed with Bayesian kernel machine regression (BKMR).
Results
PFDA, PFNA and PFOA were individually associated with higher GDM risk per interquartile range (IQR) in early pregnancy (OR [95% CI]: 1.23 [1.09, 1.38]), 1.40 [1.24, 1.58]), and 1.15 [1.04, 1.27], respectively), mid-pregnancy (1.28 [1.15, 1.43], 1.16 [1.05, 1.28], and 1.20 [1.09, 1.33], respectively), and with cumulative exposure (1.23 [1.09, 1.38], 1.21 [1.07, 1.37], and 1.19 [1.09, 1.31], respectively). PFOS in mid-pregnancy and with cumulative exposure was associated with increased GDM risk (1.41 [1.17, 1.71] and 1.33 [1.06, 1.58], respectively). PFUnDA in early pregnancy was associated with lower GDM risk (0.79 [0.64, 0.98]), whereas mid-pregnancy levels were associated with higher risk (1.49 [1.18, 1.89]). PFHxS was associated with decreased GDM risk in early and mid-pregnancy (0.48 [0.38, 0.60] and 0.48 [0.37, 0.63], respectively) and with cumulative exposure (0.49 [0.38,0.63]). PFPeA was not associated with GDM. Similar conclusions were observed in BKMR models; however, overall associations in these models were not statistically significant.
Conclusions
Higher risk of GDM was consistently observed in association with PFDA, PFNA, and PFOA exposure in both early and mid-pregnancy. Results should be corroborated in larger population-based cohorts and individuals of reproductive age should potentially avoid known sources of PFAS.
Similar content being viewed by others

Background
Gestational diabetes mellitus (GDM) is a common complication of pregnancy (7.8 per 100 US births in 2020), with sharp increases in incidence rates observed over recent years [1,2,3]. These rising rates are a public health concern given that GDM is associated with placental changes in pregnancy [4, 5], requires prompt and extensive management during pregnancy [6], and is associated with adverse perinatal outcomes and long-term health outcomes for both the mother and child [7]. Specifically, GDM is a predictor of maternal type 2 diabetes post-pregnancy [8, 9] and delivering an infant large for gestational age with possible adverse cardiometabolic phenotypes, including obesity, metabolic syndrome and type 2 diabetes [10,11,12]. Differences in prevalence rates have been documented across racial/ethnic groups with the highest rates in Asian, followed by Hispanic and Black, and lowest in non-Hispanic White [2, 3]. Established risk factors for GDM include advanced age at pregnancy, pre-pregnancy obesity, and excessive gestational weight gain [13,14,15,16]. In addition, recent literature has suggested that environmental factors, particularly exposure to endocrine-disrupting chemicals (EDCs) including per-and polyfluoroalkyl substances (PFAS) [17], may additionally play an important role in the risk of GDM [18].
PFAS are a large class of persistent synthetic chemicals used in numerous industrial and consumer products over recent decades due to their water and oil resistant properties which has resulted in widespread infiltration into the environment [19,20,21,22]. A common exposure route of PFAS to humans is through ingestion from the diet as compounds have been commonly found in drinking water and fish or being transferred into food from fast-food packaging and non-stick (i.e., Teflon) pans [23,24,25,26,27]. Pregnancy may be a susceptible exposure period with heightened sensitivity to these compounds due to biological alterations occurring during gestation that are regulated by the endocrine system with EDCs having the possibility to affect various physiological processes [28].
PFAS exposure during gestation has been associated with miscarriage, low birthweight, reduced fetal growth, preterm birth, and preeclampsia [29,30,31,32,33], and concentration levels have shown to differ based on race and ethnicity [34,35,36]. Most studies assessing the influence of prenatal PFAS exposure on GDM risk have been conducted in Chinese populations with varying results, although positive associations have been suggested [37,38,39,40,41,42,43]. Studies conducted in European and North American populations of predominantly non-Hispanic White participants have indicated PFAS exposure to be associated with higher blood glucose levels in pregnancy, but results remain largely inconsistent [44,45,46,47,48]. In addition, previous studies have primarily only measured PFAS concentrations at a single timepoint in pregnancy, limiting the ability to determine how exposure across pregnancy influences risk, as PFAS levels have shown to fluctuate across pregnancy [49].
This case–control study, nested within the diverse prospective Pregnancy Environment and Lifestyle Study (PETALS) cohort of pregnant individuals, assesses the associations of seven PFAS [perfluorooctanoic acid (PFOA), perfluorooctanesulfonic acid (PFOS), perfluorohexanesulfonic acid (PFHxS), perfluorodecanoic acid (PFDA), perfluorononanoic acid (PFNA), perfluoroundecanoic acid (PFUnDA), and perfluoro-n-pentanoic acid (PFPeA)] measured at two time points during pregnancy with the risk of GDM. We hypothesize that participants with higher levels of PFAS concentrations during gestation will have greater risk of GDM.
Methods
Study population
This nested case–control study included participants in PETALS, a racially and ethnically diverse population-based prospective pregnancy cohort with participants recruited between 2014 and 2017. Details related to the study design have previously been described [50]. Participants are members of Kaiser Permanente Northern California (KPNC), an integrated health care delivery system with over 4.5 million patients served and is demographically representative of the geographical coverage area [51, 52].
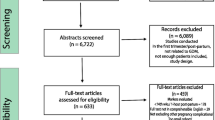
The flow chart of included participants from the PETALS cohort in this current study is shown in Fig. 1. There were 3,346 pregnant individuals who were enrolled in the PETALS cohort by completing the baseline assessment (Clinic Visit 1). Among these individuals, 4.8% (N = 161) were missing data on GDM screening due to either a pregnancy loss (1.0%), no longer a KPNC member (1.4%), or were not screened (2.4%). Of the remaining 3,185 who were screened for GDM, there were 310 GDM cases. For the original PETALS GDM case–control study, GDM cases were matched 1:2 with non-GDM controls on age (± 5 years), calendar time for enrollment (± 3 months), gestational week at the first clinic visit (± 3 weeks), and medical facility. For this current analysis, of the 310 GDM cases and 620 matched controls there were 43 GDM cases and 87 controls with serum collected at Clinic Visit 1 (CV1) available and who were also enrolled in the National Institute of Health’s Environmental influences on Child Health Outcomes (ECHO) program [53] at the time of the PFAS measurements sponsored by ECHO. For the analysis related to PFAS assessed at CV1, we further excluded 2 GDM cases because they were diagnosed with GDM prior to the serum collection. For the analysis related to PFAS at Clinic Visit 2 (CV2), 11 GDM cases were excluded because GDM was diagnosed prior to the serum collection at CV2. In addition, 1 GDM case and 3 controls were excluded because they did not have available serum at CV2. All participants with samples at CV2 also had samples at CV1. In the current study, participants completed CV1 on average at 13.8 weeks of gestation (SD: 2.2; Range: 10.1 –19.0 gestational weeks) and is referred to in this study as early pregnancy. Participants completed CV2 on average at 20.2 weeks of gestation (SD: 2.2; Range 15.6 – 26.0 gestational weeks) and is referred to in this study as mid-pregnancy. The average time between CV1 and CV2 for participants in this study was 6.5 (SD: 0.95) weeks.

Flow Chart of Included Participants from the PETALS Cohort
All participants in this analysis were enrolled into PETALS between 2014–2017 and provided written informed consent at time of enrollment. The human subjects committee of the Kaiser Foundation Research Institute approved all study design components. All participants included in the current analysis met the following criteria: 1) singleton gestation 2) no evidence based on medical record review of pre-existing cancer, diabetes mellitus, or liver disease (due to PFAS being associated with liver injury [54]); 3) data on GDM screening; and 4) data on PFAS concentrations measured in blood serum.
GDM ascertainment
GDM was ascertained using the following standardized criteria implemented across KPNC: a) ≥ 2 plasma glucose values during the 100-g, 3-h oral glucose tolerance test (OGTT) meeting or exceeding the Carpenter-Coustan thresholds (≥ 5.3 mmol/L for fasting, ≥ 10.0 mmol/L for 1-h, ≥ 8.6 mmol/L for 2 h and ≥ 7.8 mmol/L for 3 h) recommended by the American College of Obstetricians and Gynecologists [55]; or b) fasting glucose ≥ 5.1 mmol/L performed alone or during the OGTT as recommended by the International Association of Diabetes and Pregnancy Study Groups and American Diabetes Association [56].
PFAS concentrations during gestation
A fasting blood sample was collected at baseline from participants at CV1 and then again at CV2 which were conducted in early and mid-pregnancy. Serum samples were analyzed in 2020 at the Wadsworth Center's Human Health Exposure Assessment Resource (WC-HHEAR) laboratory at the NYU Langone Medical Center (Dr. Kannan's laboratory). Fourteen PFAS, specifically, PFHxS, PFOS, PFOA, PFNA, PFDA, PFUnDA, PFPeA, perfluorobutanesulfonic acid (PFBS), perfluoroheptanoic acid (PFHPA), perfluorododecanoic (PFDODA), perfluorooctanesulfonamide (PFOSA), n-ethyl perfluorooctane sulfonamido acetic acid (NETFOSAA), n-methyl perfluorooctane sulfonamido acetic acid (NMFOSAA), and perfluorohexanoic acid (PFHxA) were analyzed. The full method for the analysis of 14 PFAS in serum has previously been described [57] and further explained in the Supplemental methods. This study included analytes with at least 50% of samples above the limit of detection (LOD), as done previously [36, 58]. Values below the LOD were imputed with the LOD/\(\surd\) 2 [59].
Covariates
Covariates were identified a priori from existing literature and were visualized using a directed acyclic graph [60] (DAG) and is shown in Supplemental Fig. 1. Age, race/ethnicity, and parity information were self-reported using standardized questionnaires. Pre-pregnancy BMI was computed using weight (kg) at an average of 14 weeks prior to conception with 99% abstracted from the electronic health records and 1% being self-reported. Height (m) was measured at the first study clinic visit. Race and ethnicity was used as a covariate for a proxy of experiencing racism and discrimination and previous literature has indicated race and ethnicity is associated with both measured PFAS concentration levels [34,35,36], and GDM incidence rates [2, 3].
Statistical analysis
Differences in demographic characteristics by GDM status and PFAS concentrations were determined by Wilcoxon signed rank tests, student’s t tests, Kruskal Wallis tests and Pearson’s chi square tests. Spearman correlations examined relationships across PFAS compounds at each time point and across timepoints within the same individual.
To approximate cumulative exposure across the two blood samples, the area under the curve (AUC) was calculated to integrate both the PFAS concentration and the timing of exposure assessment [61] (Equation Supplemental Fig. 2). To properly analyze the potentially broken matched trios from the original matched case–control study within PETALS, we fit adjusted weighted unconditional logistic regression models to determine the associations of individual PFAS concentrations during gestation with GDM risk separately using levels measured in early pregnancy, mid-pregnancy, and with the AUC across the two time points. Each participant was assigned an inverse of probability weight (IPW) to be used in models. IPW for cases were calculated as the inverse of the number of cases at each time point divided by the total number of cases in the PETALS cohort (n = 310). Controls were assigned a weight based on the inverse of the predicted probability in a logistic regression model using all PETALS controls that had GDM screening data (n = 2,875) with the original matching criteria. Due to the skewed PFAS distributions and for being a common approach in the literature, compounds were transformed with the natural log. PFAS analytes were then scaled by the relevant interquartile range (IQR) based on the log-transformed concentration levels for interpretations.
Since exposure to PFAS analytes occur concurrently, we assessed the effects of the seven PFAS as a mixture by fitting adjusted probit Bayesian kernel machine regression (BKMR) models on GDM risk [62]. BKMR models were fit for PFAS levels in early pregnancy, mid-pregnancy, and across both timepoints with the AUC. For the BKMR models to converge, we used a pre-adjustment method for covariates that first fit a frequentist probit regression model with no PFAS analytes but all covariates, and then incorporated the fitted values as a single adjustment covariate in the BKMR models. Each BKMR model fit used 50,000 Markov Chain Monte Carlo iterations, and the trace plots of model parameters were visually examined to confirm model convergence. Results of the mixture analysis were summarized with the posterior inclusion probabilities (PIPs) and cross-section plots of the exposure response function. The association of the PFAS mixture with risk of GDM was examined by re-estimating the BKMR model with the PFAS analyte of interest forced into the mixture and used posterior samples to estimate the odds ratio (OR) and 95% credible intervals (95% CI) for GDM by 10% increments of each single PFAS, with all other PFAS set to the median.
Analyses were conducted using SAS version 9.4 and R version 4.1.0 with the bkmr R package for mixture models [63]. To account for multiple comparisons, p-values (\(\alpha\)=0.05) were false discovery rate (FDR) adjusted for the weighted unconditional logistic regression models.
Results
Our sample included 128 participants at the baseline visit (CV1) in early pregnancy (41 cases, 87 controls) and 113 at CV2 in mid-pregnancy (29 cases, 84 controls). Participants were 32 ± 5 years of age and primarily Hispanic (39.1%) or Asian/Pacific Islander (25.0%), followed by White (21.9%), Black (7%), and 7% of individuals from other racial/ethnic groups. The majority were multiparous (55.9%). Participant characteristics of this sample were similar to the larger PETALS cohort [64] and characteristics for the GDM cases in PETALS (n = 310) and by timepoints of each clinic visit (n = 41 CV1, n = 29 CV2) are shown in Supplemental Table 1. Demographics for the sample and by GDM status are shown in Table 1.
Seven of the fourteen measured PFAS analytes met our LOD inclusion criteria: PFHxS, PFOS, PFOA, PFNA, PFDA, PFUnDA, and PFPeA. Median PFAS concentrations were similar between the two timepoints. Distributions at each time point and the AUC are shown in Table 2. The paired concentrations of participants with samples at both clinic visits (n = 113) showed each PFAS to be moderately to highly correlated with one another (rho 0.53–0.94) and are shown in Supplemental Fig. 3. Within each separate timepoint, most PFAS were positively correlated with one another (rho 0.18 to 0.78), except for PFPeA (rho 0.09 to -0.16) (Supplemental Fig. 3). Significant differences in median concentrations by race/ethnicity groups were observed for all analytes except PFPeA, with highest medians observed in Asian/Pacific Islander and Black participants. Differences in medians were also identified by parity and pre-pregnancy BMI groups (Supplemental Table 2).
In multivariable models shown in Table 3, early pregnancy concentrations, mid-pregnancy concentrations, and the AUC of PFDA, PFNA and PFOA were individually significantly associated with higher GDM risk. Specifically, for early pregnancy the following associations with GDM risk were found: PFDA (OR: 1.23 [95% CI 1.09, 1.38]), PFNA (OR:1.40 [95% CI 1.24, 1.58]), and PFOA (OR:1.15 [95% CI 1.04, 1.27]) per IQR. For mid-pregnancy, we observed the following associations: PFDA (OR:1.28 [95% CI 1.15, 1.43]), PFNA (OR:1.16 [95% CI 1.05, 1.28]), and PFOA (OR:1.20 [95% CI 1.09, 1.33]) per IQR. Finally, for the AUC the associations of each of these PFAS and GDM risk were as follows: PFDA (OR:1.23 [95% CI 1.09, 1.38]), PFNA (OR:1.21 [95% CI 1.07, 1.37]), and PFOA (OR:1.19 [95% CI 1.09, 1.31]) per IQR (Table 3). Early pregnancy concentrations of PFOS were not associated with GDM risk, however, mid-pregnancy concentrations and the AUC for PFOS were individually associated with higher GDM risk (OR:1.41 [95% CI 1.17, 1.71] and OR: 1.33 [95% CI 1.06, 1.58], per IQR, respectively). For PFUnDA, early pregnancy levels were associated with lower GDM risk (OR: 0.79 per IQR [95% CI 0.64, 0.98]), whereas mid-pregnancy levels were associated with higher GDM risk (OR:1.49 per IQR [95% CI 1.18, 1.89]). For PFHxS, concentrations were associated with decreased risk of GDM in early pregnancy (OR:0.48 [95% CI 0.38, 0.60]), mid-pregnancy (OR: 0.48 [95% CI 0.37, 0.63]) and with the AUC (OR: 0.49 [95% CI 0.38, 0.63]) per IQR. PFPeA was not associated with GDM risk at either timepoint or with the AUC (Table 3).
In mixture analyses, PFHxS had the largest contribution to the mixture (Supplemental Table 3), although PIPs for each PFAS were moderate (Early Pregnancy: 0.31–0.61; Mid-Pregnancy: 0.34–0.51). In the cross-section plots of the exposure response function for each PFAS, PFNA, PFOA and PFUnDA showed suggestive positive associations with GDM risk, while PFHxS suggested an inverse association with GDM risk (Fig. 2 (AUC) and Supplemental Figs. 4–5). No significant associations were found at any timepoint for the overall mixture effect via summary ORs (Fig. 3 (AUC) and Supplemental Figs. 6–7).

Exposure response function for each PFAS from Bayesian kernel machine regression models with the Area Under the Curve (AUC) between the two clinic visits

Overall PFAS Mixture Effect with Odds of GDM, Area Under the Curve
Discussion
This nested case–control study within the racially and ethnically diverse PETALS cohort found consistent evidence that prenatal exposure to PFAS, notably PFDA, PFNA, and PFOA, during early and mid-pregnancy was significantly associated with higher risk of GDM. For PFOS and PFUnDA, increased risk of GDM was observed only for exposure during mid-pregnancy. In contrast, PFHxS was associated with decreased risk of GDM during early and mid-pregnancy. Mixture results suggested similar findings, but overall mixture models were not statistically significant.
The current literature of PFAS exposure during gestation and risk of GDM has primarily been assessed using PFAS levels collected at only one timepoint in pregnancy. Although PFAS have long half-lives, analyte levels overall have been shown to vary across pregnancy in the same individual [49], and critical windows of exposure to PFAS may occur during gestation. It is also possible that maternal metabolic shifts occur including different rates of transplacental PFAS transfer to the fetus and blood volume expansion or mobilization of stored PFAS across pregnancy [65, 66] which may explain inverse associations or the possibility of reverse causation for samples collected late in pregnancy [67]. In our study, results using early pregnancy samples compared to mid-pregnancy samples were relatively consistent, although different conclusions were made for PFUnDA and PFOS across timepoints which may indicate less evidence for exposure to these analytes with risk of GDM. It is also possible that the physiological changes occurring during mid-pregnancy, such as increased insulin resistance and hormonal shifts in mid to late pregnancy may interact with PFOS and PFUnDA exposure differently compared to earlier in pregnancy [68]. An example includes Human Placental Lactogen (hPL) which is produced by the placenta and helps regulate maternal metabolism and fetal growth which steadily increases during the second trimester and works to decrease the mother's sensitivity to insulin, making more glucose available for the growing fetus [69].
Higher levels of PFAS have been associated with type 2 diabetes [70, 71], increased glucose and insulin levels in pregnancy [17] and may play an important role in GDM development [18]. During pregnancy, the body becomes more resistant to insulin due to hormonal changes and PFAS exposure may exacerbates this insulin resistance, thereby increasing the risk of GDM [68]. Proposed mechanisms of PFAS influences on glucose levels observed in pregnancy include inflammation and oxidative stress which can impair insulin signaling and glucose metabolism, alterations in fatty acid and adipose tissue disfunction including changes in adipokine secretion and adipocyte differentiation, which is associated with insulin resistance, and activation of peroxisome proliferator-activated receptors (PPARs) based on toxicological evidence [72, 73]. However, previous epidemiological studies on the association between PFAS exposure and GDM risk are inconclusive due to suggesting differential risks of certain analytes with GDM risk.
In studies conducted within the United States examining the association between PFAS exposure during gestation and GDM risk, PFAS were assessed either before pregnancy [74] or in the first trimester [46, 75] and included populations of primarily non-Hispanic White participants, except for Rahman et al. which included a diverse study population [75]. Our findings that PFOA and PFNA were associated with greater risk of GDM is consistent with results from two previous US cohorts [74, 75] though a third reported null associations with PFOA but observed PFOS to be a primary driver within BKMR models for increased continuous glucose levels [46]. PFOS and PFNA had significant positive associations with blood glucose levels among Asian participants with the largest effect estimates compared to other racial groups [46]. The inverse association found with PFHxS has not been replicated in other studies [41, 43,44,45, 47]. However, inverse associations have been reported with other cardiometabolic conditions in pregnancy from prenatal PFHxS exposure [76]. This inverse association with blood pressure in pregnancy was thought to be a chance finding from the authors due to not having a biological mechanism known that would explain this relationship [76]. It is possible that the inverse associations in this current study may also be due to chance even after FDR adjusting the p-values. Other hypotheses include random variation in PFHxS due to the small sample size creating potential noise in the data, a complex interaction with other PFAS compounds in that PFHxS may interact with other compounds in ways that are not yet fully understood which has potentially led to this unexpected association, as well as potential effect modification by a third variable (i.e., race/ethnicity, pre-pregnancy BMI, or maternal age), which we were interested in assessing but were unable to produce reliable estimates due to the small sample sizes within each strata.
Studies conducted in Chinese populations produced results that have been inconclusive. Wang et al. found that early pregnancy levels of PFOA and PFOS were not associated with GDM risk [40], however, PFOA was significantly associated with fasting insulin and homeostasis model assessment of insulin resistance [40]. Xu et al. found PFBS and PFDoA to be positively associated with GDM risk, but null for PFAS that overlapped in this study [42]. Liu et al. used summed values based on structural characteristics of PFAS and found total perfluoroalkyl carboxylates (including PFOA, PFNA, PFDA, PFUnDA among others) to be positively associated with GDM risk [38], which is consistent with analytes showing higher risk of GDM within our results. Yu et al. conducted a BKMR model and found that the PFAS mixture exposure was positively associated with GDM incidence and PFOS, PFNA and PFHpA were main contributors to the mixture [43]. This was inconsistent with our findings as PFHxS was a primary contributor although PFNA was the secondary contributor for both timepoints and the AUC. Our mixture analysis through BKMR was also not statistically significant and we hypothesize that the small sample size was a hinderance and that the complex inverse and positive associations across analytes may have made the mixture difficult to disentangle.
Prominent strengths of this study include the longitudinal design, diverse study population from an integrated health care system with universal screening for GDM, the availability of pregnancy levels of glycemia for rigorous and standardized assessment of GDM and multiple time points for PFAS concentration assessment within pregnancy which held temporality due to being collected prior to GDM ascertainment. This study also incorporated mixture methods using BKMR which has been underutilized and identified as a gap within the current literature [71]. Mixture approaches are important when assessing these associations due to the concurrent and correlated nature of the exposures.
Limitations are also present. The sample size is relatively small, but the original 2–1 matching design increased statistical power for the individual models and all results were FDR-adjusted to reduce the risk of chance findings. The mixture models suggested similar conclusions to the individual models but did not reach statistical significance, likely due to not being well powered for BKMR models. Additionally, low detection frequencies (< 50% of samples) for seven of the fourteen PFAS inhibited inclusion. Lastly, true overall exposure to PFAS across early to mid-pregnancy was not obtained and instead used the AUC as a proxy measurement. However, AUC results were consistent to early and mid-pregnancy results.
Conclusions
This prospective nested case–control study observed that higher serum levels of PFDA, PFNA, and PFOA during early and mid-pregnancy were consistently associated with higher GDM risk in an ethnically diverse population. It is important to corroborate results in larger sample sizes and to potentially advise individuals of reproductive age to avoid known sources of PFAS.
Availability of data and materials
Extracted data are available within the publication and its supplementary files. A de-identified analytic dataset with code used in this study can be shared with qualified researchers subject to approval by the Kaiser Foundation Research Institute Human Subjects Committee and by the Human Subjects Committee at the institutions requesting the data and a signed data sharing agreement. Please send all requests to the corresponding author of this article. Data will be available to requesters from 1 year after the date of publication of this article.
Abbreviations
- BKMR:
-
Bayesian kernel machine regression
- CV1:
-
Clinic Visit 1
- CV2:
-
Clinic Visit 2
- EDCs:
-
Endocrine-disrupting chemicals
- FDR:
-
False discovery rate
- GDM:
-
Gestational diabetes mellitus
- IQR:
-
Interquartile range
- KPNC:
-
Kaiser Permanente Northern California
- LOD:
-
Limit of detection
- OR:
-
Odds ratio
- OGTT:
-
Oral glucose tolerance test
- NETFOSAA:
-
N-ethyl perfluorooctane sulfonamido acetic acid
- NMFOSAA:
-
N-methyl perfluorooctane sulfonamido acetic acid
- PFAS:
-
Per- and polyfluoroalkyl substances
- PFOA:
-
Perfluorooctanoic acid
- PFOS:
-
Perfluorooctanesulfonic acid
- PFHxS:
-
Perfluorohexanesulfonic acid
- PFDA:
-
Perfluorodecanoic acid
- PFNA:
-
Perfluorononanoic acid
- PFUnDA:
-
Perfluoroundecanoic acid
- PFPeA:
-
Perfluoro-n-pentanoic acid
- PFBS:
-
Perfluorobutanesulfonic acid
- PFHPA:
-
Perfluoroheptanoic acid
- PFDODA:
-
Perfluorododecanoic
- PFOSA:
-
Perfluorooctanesulfonamide
- PFHxA:
-
Perfluorohexanoic acid
- PIPs:
-
Posterior inclusion probabilities
- CI:
-
95% Confidence Interval
References
Ferrara A, Kahn HS, Quesenberry CP, Riley C, Hedderson MM. An increase in the incidence of gestational diabetes mellitus: Northern California, 1991–2000. Obstet Gynecol. 2004;103(3):526–33.
Gregory EC, Ely DM. Trends and characteristics in gestational diabetes: United States, 2016–2020. Natl Vital Stat Rep. 2022;71(3):1–15.
Shah NS, Wang MC, Freaney PM, Perak AM, Carnethon MR, Kandula NR, et al. Trends in gestational diabetes at first live birth by race and ethnicity in the US, 2011–2019. JAMA. 2021;326(7):660–9.
Guadix P, Corrales I, Vilariño-García T, Rodríguez-Chacón C, Sánchez-Jiménez F, Jiménez-Cortegana C, et al. Expression of nutrient transporters in placentas affected by gestational diabetes: role of leptin. Front Endocrinol (Lausanne). 2023;14:1172831.
Sirico A, Rossi ED, Degennaro VA, Arena V, Rizzi A, Tartaglione L, et al. Placental diabesity: placental VEGF and CD31 expression according to pregestational BMI and gestational weight gain in women with gestational diabetes. Arch Gynecol Obstet. 2023;307(6):1823–31.
Luo R, Wen W, Corsi DJ, Fell DB, Taljaard M, Wen SW, et al. Comparison of adverse maternal and perinatal outcomes between induction and expectant management among women with gestational diabetes mellitus at term pregnancy: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2023;23(1):509.
Murray SR, Reynolds RM. Short- and long-term outcomes of gestational diabetes and its treatment on fetal development. Prenat Diagn. 2020;40(9):1085–91.
Bellamy L, Casas J-P, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373(9677):1773–9.
Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care. 2002;25(10):1862–8.
Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational diabetes mellitus: mechanisms, treatment, and complications. Trends Endocrinol Metab. 2018;29(11):743–54.
Nicholas L, Morrison J, Rattanatray L, Zhang S, Ozanne S, McMillen I. The early origins of obesity and insulin resistance: timing, programming and mechanisms. Int J Obes. 2016;40(2):229–38.
Page KA, Luo S, Wang X, Chow T, Alves J, Buchanan TA, et al. Children exposed to maternal obesity or gestational diabetes mellitus during early fetal development have hypothalamic alterations that predict future weight gain. Diabetes Care. 2019;42(8):1473–80.
Chu SY, Callaghan WM, Kim SY, Schmid CH, Lau J, England LJ, et al. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care. 2007;30(8):2070–6.
Hedderson MM, Gunderson EP, Ferrara A. Gestational weight gain and risk of gestational diabetes mellitus. Obstet Gynecol. 2010;115(3):597.
Li Y, Ren X, He L, Li J, Zhang S, Chen W. Maternal age and the risk of gestational diabetes mellitus: a systematic review and meta-analysis of over 120 million participants. Diabetes Res Clin Pract. 2020;162: 108044.
Solomon CG, Willett WC, Carey VJ, Rich-Edwards J, Hunter DJ, Colditz GA, et al. A prospective study of pregravid determinants of gestational diabetes mellitus. JAMA. 1997;278(13):1078–83.
Birru RL, Liang H-W, Farooq F, Bedi M, Feghali M, Haggerty CL, et al. A pathway level analysis of PFAS exposure and risk of gestational diabetes mellitus. Environ Health. 2021;20(1):1–16.
Yan D, Jiao Y, Yan H, Liu T, Yan H, Yuan J. Endocrine-disrupting chemicals and the risk of gestational diabetes mellitus: a systematic review and meta-analysis. Environ Health. 2022;21(1):53.
Dauchy X, Boiteux V, Bach C, Rosin C, Munoz J-F. Per-and polyfluoroalkyl substances in firefighting foam concentrates and water samples collected near sites impacted by the use of these foams. Chemosphere. 2017;183:53–61.
Houde M, De Silva AO, Muir DC, Letcher RJ. Monitoring of perfluorinated compounds in aquatic biota: an updated review: PFCs in aquatic biota. Environ Sci Technol. 2011;45(19):7962–73.
Schaider LA, Balan SA, Blum A, Andrews DQ, Strynar MJ, Dickinson ME, et al. Fluorinated compounds in US fast food packaging. Environ Sci Technol Lett. 2017;4(3):105–11.
Sinclair GM, Long SM, Jones OA. What are the effects of PFAS exposure at environmentally relevant concentrations? Chemosphere. 2020;258:127340.
Barbo N, Stoiber T, Naidenko OV, Andrews DQ. Locally caught freshwater fish across the United States are likely a significant source of exposure to PFOS and other perfluorinated compounds. Environ Res. 2023;220:115165. https://doi.org/10.1016/j.envres.2022.115165. Epub 2022 Dec 28.
Christensen KY, Raymond M, Blackowicz M, Liu Y, Thompson BA, Anderson HA, et al. Perfluoroalkyl substances and fish consumption. Environ Res. 2017;154:145–51.
Domingo JL, Nadal M. Human exposure to per-and polyfluoroalkyl substances (PFAS) through drinking water: a review of the recent scientific literature. Environ Res. 2019;177: 108648.
Lestido-Cardama A, Barbosa-Pereira L, Sendón R. Presence of Perfluoroalkyl and Polyfluoroalkyl Substances (PFAS) in Food Contact Materials (FCM) and its migration to food. Foods. 2021;10(7):1443.
Susmann HP, Schaider LA, Rodgers KM, Rudel RA. Dietary habits related to food packaging and population exposure to PFASs. Environ Health Perspect. 2019;127(10):107003.
Varshavsky J, Smith A, Wang A, Hom E, Izano M, Huang H, et al. Heightened susceptibility: a review of how pregnancy and chemical exposures influence maternal health. Reprod Toxicol. 2020;92:14–56.
Cao T, Qu A, Li Z, Wang W, Liu R, Wang X, et al. The relationship between maternal perfluoroalkylated substances exposure and low birth weight of offspring: a systematic review and meta-analysis. Environ Sci Pollut Res Int. 2021;28(47):67053–65.
Gao X, Ni W, Zhu S, Wu Y, Cui Y, Ma J, et al. Per- and polyfluoroalkyl substances exposure during pregnancy and adverse pregnancy and birth outcomes: a systematic review and meta-analysis. Environ Res. 2021;201: 111632.
Gui SY, Chen YN, Wu KJ, Liu W, Wang WJ, Liang HR, et al. Association between exposure to Per- and polyfluoroalkyl substances and birth outcomes: a systematic review and meta-analysis. Front Public Health. 2022;10: 855348.
Sevelsted A, Gürdeniz G, Rago D, Pedersen CET, Lasky-Su JA, Checa A, et al. Effect of perfluoroalkyl exposure in pregnancy and infancy on intrauterine and childhood growth and anthropometry. Sub study from COPSAC2010 birth cohort. EBioMedicine. 2022;83:104236.
Szilagyi JT, Avula V, Fry RC. Perfluoroalkyl substances (PFAS) and their effects on the placenta, pregnancy, and child development: a potential mechanistic role for placental peroxisome proliferator–activated receptors (PPARs). Curr Environ Health Rep. 2020;7(3):222–30.
Boronow KE, Brody JG, Schaider LA, Peaslee GF, Havas L, Cohn BA. Serum concentrations of PFASs and exposure-related behaviors in African American and non-Hispanic white women. J Expo Sci Environ Epidemiol. 2019;29(2):206–17.
Calafat AM, Kuklenyik Z, Reidy JA, Caudill SP, Tully JS, Needham LL. Serum concentrations of 11 polyfluoroalkyl compounds in the US population: data from the National Health and Nutrition Examination Survey (NHANES) 1999 – 2000. Environ Sci Technol. 2007;41(7):2237–42.
Peterson AK, Eckel SP, Habre R, Yang T, Faham D, Farzan SF, et al. Prenatal perfluorooctanoic acid (PFOA) exposure is associated with lower infant birthweight within the MADRES pregnancy cohort. Front Epidemiol. 2022;2:21.
Li J, Yao J, Xia W, Dai J, Liu H, Pan Y, et al. Association between exposure to per-and polyfluoroalkyl substances and blood glucose in pregnant women. Int J Hyg Environ Health. 2020;230: 113596.
Liu X, Zhang L, Chen L, Li J, Wang Y, Wang J, et al. Structure-based investigation on the association between perfluoroalkyl acids exposure and both gestational diabetes mellitus and glucose homeostasis in pregnant women. Environ Int. 2019;127:85–93.
Ren Y, Jin L, Yang F, Liang H, Zhang Z, Du J, et al. Concentrations of perfluoroalkyl and polyfluoroalkyl substances and blood glucose in pregnant women. Environ Health. 2020;19(1):1–10.
Wang H, Yang J, Du H, Xu L, Liu S, Yi J, et al. Perfluoroalkyl substances, glucose homeostasis, and gestational diabetes mellitus in Chinese pregnant women: a repeat measurement-based prospective study. Environ Int. 2018;114:12–20.
Wang Y, Zhang L, Teng Y, Zhang J, Yang L, Li J, et al. Association of serum levels of perfluoroalkyl substances with gestational diabetes mellitus and postpartum blood glucose. J Environ Sci. 2018;69:5–11.
Xu H, Zhou Q, Zhang J, Chen X, Zhao H, Lu H, et al. Exposure to elevated per-and polyfluoroalkyl substances in early pregnancy is related to increased risk of gestational diabetes mellitus: a nested case-control study in Shanghai, China. Environ Int. 2020;143: 105952.
Yu G, Jin M, Huang Y, Aimuzi R, Zheng T, Nian M, et al. Environmental exposure to perfluoroalkyl substances in early pregnancy, maternal glucose homeostasis and the risk of gestational diabetes: a prospective cohort study. Environ Int. 2021;156: 106621.
Jensen RC, Glintborg D, Timmermann CAG, Nielsen F, Kyhl HB, Andersen HR, et al. Perfluoroalkyl substances and glycemic status in pregnant Danish women: the Odense Child Cohort. Environ Int. 2018;116:101–7.
Matilla-Santander N, Valvi D, Lopez-Espinosa M-J, Manzano-Salgado CB, Ballester F, Ibarluzea J, et al. Exposure to perfluoroalkyl substances and metabolic outcomes in pregnant women: evidence from the Spanish INMA birth cohorts. Environ Health Perspect. 2017;125(11):117004.
Preston EV, Rifas-Shiman SL, Hivert M-F, Zota AR, Sagiv SK, Calafat AM, et al. Associations of per-and polyfluoroalkyl substances (PFAS) with glucose tolerance during pregnancy in project viva. J Clin Endocrinol Metab. 2020;105(8):e2864–76.
Shapiro GD, Dodds L, Arbuckle TE, Ashley-Martin J, Ettinger AS, Fisher M, et al. Exposure to organophosphorus and organochlorine pesticides, perfluoroalkyl substances, and polychlorinated biphenyls in pregnancy and the association with impaired glucose tolerance and gestational diabetes mellitus: the MIREC Study. Environ Res. 2016;147:71–81.
Valvi D, Oulhote Y, Weihe P, Dalgård C, Bjerve KS, Steuerwald U, et al. Gestational diabetes and offspring birth size at elevated environmental pollutant exposures. Environ Int. 2017;107:205–15.
Chen L, Tong C, Huo X, Zhang J, Tian Y. Prenatal exposure to perfluoroalkyl and polyfluoroalkyl substances and birth outcomes: a longitudinal cohort with repeated measurements. Chemosphere. 2021;267: 128899.
Zhu Y, Hedderson MM, Feng J, Mevi AA, Ferrara A. The Pregnancy Environment and Lifestyle Study (PETALS): a population-based longitudinal multi-racial birth cohort. BMC Pregnancy Childbirth. 2017;17(1):1–10.
Davis AC, Voelkel JL, Remmers CL, Adams JL, McGlynn EA. Comparing kaiser permanente members to the general population: implications for generalizability of research. Perm J. 2023;27(2):87.
Gordon NP. Similarity of the adult Kaiser Permanente membership in Northern California to the insured and general population in Northern California: statistics from the 2011 California health interview survey. Oakland: Kaiser Permanente Division of Research; 2015.
Blaisdell CJ, Park C, Hanspal M, Roary M, Arteaga SS, Laessig S, et al. The NIH ECHO Program: investigating how early environmental influences affect child health. Pediatr Res. 2022;92(5):1215–6.
Midya V, Colicino E, Conti DV, Berhane K, Garcia E, Stratakis N, et al. Association of prenatal exposure to endocrine-disrupting chemicals with liver injury in children. JAMA Netw Open. 2022;5(7):e2220176-e.
Obstetricians ACo, Gynecologists. ACOG practice bulletin no. 201: pregestational diabetes mellitus. Obstet Gynecol. 2018;132(6):e228–48.
Diabetes IAo, Panel PSGC. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–82.
Honda M, Robinson M, Kannan K. A rapid method for the analysis of perfluorinated alkyl substances in serum by hybrid solid-phase extraction. Environ Chem. 2018;15(2):92–9.
Ames JL, Burjak M, Avalos LA, Braun JM, Bulka CM, Croen LA, et al. Prenatal exposure to per- and polyfluoroalkyl substances and childhood autism-related outcomes. Epidemiology. 2023;34(3):450.
Hornung RW, Reed LD. Estimation of average concentration in the presence of nondetectable values. Appl Occup Environ Hyg. 1990;5(1):46–51.
Textor J, van der Zander B, Gilthorpe MS, Liskiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package ‘dagitty.’ Int J Epidemiol. 2016;45(6):1887–94.
Smith TJ, Kriebel D. A biologic approach to environmental assessment and epidemiology. Oxford University Press; 2010.
Bobb JF, Claus Henn B, Valeri L, Coull BA. Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ Health. 2018;17(1):1–10.
Bobb JF, Valeri L, Claus Henn B, Christiani DC, Wright RO, Mazumdar M, Godleski JJ, Coull BA. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics. 2015;16(3):493–508. https://doi.org/10.1093/biostatistics/kxu058. Epub 2014 Dec 22.
Ehrlich SF, Ferrara A, Hedderson MM, Feng J, Neugebauer R. Exercise during the first trimester of pregnancy and the risks of abnormal screening and gestational diabetes mellitus. Diabetes Care. 2021;44(2):425–32.
Appel M, Forsthuber M, Ramos R, Widhalm R, Granitzer S, Uhl M, et al. The transplacental transfer efficiency of per- and polyfluoroalkyl substances (PFAS): a first meta-analysis. J Toxicol Environ Health B Crit Rev. 2022;25(1):23–42.
Nielsen C, Andersson Hall U, Lindh C, Ekström U, Xu Y, Li Y, et al. Pregnancy-induced changes in serum concentrations of perfluoroalkyl substances and the influence of kidney function. Environ Health. 2020;19(1):1–9.
Verner M-A, Loccisano AE, Morken N-H, Yoon M, Wu H, McDougall R, et al. Associations of perfluoroalkyl substances (PFAS) with lower birth weight: an evaluation of potential confounding by glomerular filtration rate using a physiologically based pharmacokinetic model (PBPK). Environ Health Perspect. 2015;123(12):1317–24.
Catalano PM, Drago NM, Amini SB. Longitudinal changes in pancreatic beta-cell function and metabolic clearance rate of insulin in pregnant women with normal and abnormal glucose tolerance. Diabetes Care. 1998;21(3):403–8.
Bhagavan NV, Ha C-E. Chapter 32 - Endocrine metabolism V: reproductive system. In: Bhagavan NV, Ha C-E, editors. Essentials of medical biochemistry. 2nd ed. San Diego: Academic Press; 2015. p. 589–606.
Gui SY, Qiao JC, Xu KX, Li ZL, Chen YN, Wu KJ, Jiang ZX, Hu CY. Association between per-and polyfluoroalkyl substances exposure and risk of diabetes: a systematic review and meta-analysis. J Expo Sci Environ Epidemiol. 2023;33(1):40–55. https://doi.org/10.1038/s41370-022-00464-3. Epub 2022 Aug 15.
Roth K, Petriello MC. Exposure to per- and polyfluoroalkyl substances (PFAS) and type 2 diabetes risk. Front Endocrinol (Lausanne). 2022;13:965384.
Lau C, Anitole K, Hodes C, Lai D, Pfahles-Hutchens A, Seed J. Perfluoroalkyl acids: a review of monitoring and toxicological findings. Toxicol Sci. 2007;99(2):366–94.
Wolf CJ, Takacs ML, Schmid JE, Lau C, Abbott BD. Activation of mouse and human peroxisome proliferator – activated receptor alpha by perfluoroalkyl acids of different functional groups and chain lengths. Toxicol Sci. 2008;106(1):162–71.
Zhang C, Sundaram R, Maisog J, Calafat AM, Barr DB, Louis GMB. A prospective study of prepregnancy serum concentrations of perfluorochemicals and the risk of gestational diabetes. Fertil Steril. 2015;103(1):184–9.
Rahman ML, Zhang C, Smarr MM, Lee S, Honda M, Kannan K, et al. Persistent organic pollutants and gestational diabetes: a multi-center prospective cohort study of healthy US women. Environ Int. 2019;124:249–58.
Birukov A, Andersen LB, Andersen MS, Nielsen JH, Nielsen F, Kyhl HB, et al. Exposure to perfluoroalkyl substances and blood pressure in pregnancy among 1436 women from the Odense Child Cohort. Environ Int. 2021;151: 106442.
Acknowledgements
We thank our families participating in the PETALS cohort and the medical, nursing, and program staff.
Funding
The research was supported by the National Institute of Environmental Health Sciences (R01ES019196 to AF and U2CES026542 to KK), National Institutes of Health Office of Directors (UG3/UH3OD023289 to AF and UH3OD023272 to AP), National Institute of Diabetes and Digestive and Kidney Diseases (K01DK120807 to YZ and T32DK116684 to AKP), and National Heart, Lung, and Blood Institute (R01HL157666 to YZ). The funding sources had no role in the design of the study, analysis or interpretation of findings, writing the manuscript, or the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Conceptualization AF, AKP, YZ; Data curation JF, SF; Formal analysis SF; Funding acquisition AF, AP, KK, AKP, YZ; Investigation AF, AKP, YZ; Methodology AF, AKP, AP, KK, MR, SA, SDM, ; Project administration AF, YZ; Resources AF, AP, KK, YZ; Software JF, SF; Supervision AF; Validation AKP, JF, MR SF; Visualization AKP, JF, SF; Roles/Writing - original draft AKP; Writing - review & editing all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants in this analysis provided written informed consent at time of enrollment. The human subjects committee of the Kaiser Foundation Research Institute approved all study design components. All the methods and procedures carried out in this study were in accordance with relevant guidelines and regulation (for e.g., Declaration of Helsinki).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplemental Figure 1. Directed acyclic graph (DAG) Reflecting the Total Effect of Gestational PFAS Exposure on GDM. Supplemental Figure 2. Area Under the Curve (AUC) Equation. Supplemental Figure 3. Spearman Correlations of PFAS Analytes by Timepoint. Supplemental Table 1. Demographics of GDM Cases in the PETALS Cohort and those Included in Current Study. Supplemental Table 2. Median PFAS Analyte Concentrations (ng/mL) by Participant Characteristics. Supplemental Table 3. Posterior Inclusion Probabilities of each PFAS analyte in Bayesian kernel machine regression models. Supplemental Figure 4. Exposure response function for each PFAS from Bayesian kernel machine regression model in early pregnancy (Clinic Visit 1). Supplemental Figure 5. Exposure response function for each PFAS from Bayesian kernel machine regression model among in mid-pregnancy (Clinic Visit 2). Supplemental Figure 6. Overall PFAS Mixture Effect with Odds of GDM, Clinic Visit 1. Supplemental Figure 7. Overall PFAS Mixture Effect with Odds of GDM, Clinic Visit 2.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peterson, A.K., Zhu, Y., Fuller, S. et al. PFAS concentrations in early and mid-pregnancy and risk of gestational diabetes mellitus in a nested case-control study within the ethnically and racially diverse PETALS cohort. BMC Pregnancy Childbirth 23, 657 (2023). https://doi.org/10.1186/s12884-023-05953-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05953-3