
Abstract
Background
Perinatal maternal depression and anxiety are associated with adverse maternal outcomes, and nutrition may play an important role in their emergence. Previous research shows that certain micro and macronutrients found in different dietary patterns may associate with perinatal mood disorders. This study aims to explore relationships between nutrition during pregnancy and perinatal maternal depression and anxiety symptoms using network analyses.
Methods
Using data from the French EDEN mother-child cohort, the sample consisted of 1438 women with available mental health outcomes (CES-D, STAI and EPDS) and nutritional markers collected from food frequency questionnaires. Four networks were constructed to explore the relationships between prenatal nutrient status, dietary patterns, and perinatal mental health, while accounting for important confounders.
Results
The Healthy dietary pattern was associated with the presence of vital micronutrients, while the Western dietary pattern was consistently associated with poorer intake of specific micronutrients and contained an excess of certain macronutrients. Western dietary pattern and symptoms of postnatal depression were connected by a positive edge in both the macronutrient and micronutrient networks. Lower education levels were associated with higher Western dietary pattern scores, from which a positive edge linked to postnatal depression symptoms in both models.
Conclusions
A Western dietary pattern was associated with increased symptoms of postnatal depression in our adjusted network models; The Healthy dietary pattern was associated with essential micronutrients but not with symptoms of depression or anxiety. Perinatal mental health might be impacted by specific dietary patterns in the context of psychosocial and physical stress associated with pregnancy.
Similar content being viewed by others

Background
Perinatal depression and anxiety affect mothers worldwide and are associated with an increased likelihood of mental health problems in their offspring [1]. Prevalence rates during the perinatal period are estimated to be 11.9% for symptoms of depression and 22.9% for symptoms of anxiety [2, 3]. The need to identify factors that contribute to maternal mental illness, specifically during the vulnerable gestational and post-natal periods, remains a challenge. Historically, the literature has focused on common psychosocial risk factors including a personal or family history of mental health problems, adverse childhood events (ACE), or increased life stress [4, 5]. Nutrition has recently emerged as a factor that potentially contributes to perinatal anxiety and depression, possibly due to the increasing evidence of this association with mental health in the general population [6, 7]. Concomitantly, evidence links lower socioeconomic status (SES) and nutritional status, specifically a lack of micronutrients in the diets of lower SES individuals, creating a complex matrix of influential variables related to perinatal mental health [8].
The perinatal period is considered a time of intense nutritional demands for expectant mothers, mainly due to an increase in their resting metabolic rate [9]. Demanding pathophysiological changes require an additional intake of an extra 450 kcal/day on average throughout the course of pregnancy to account for total daily energy expenditure [9]. Throughout the life span, availability of vital nutrients is conditional upon patterns of dietary intake. Although no standardized definition of specific dietary patterns exists, previous studies have identified patterns such as ‘Healthy’ or ‘Western’ that generally consist of distinct food groups and their nutrients’ quality and quantity [10]. Research investigating dietary patterns and maternal mental health suggests that a ‘Healthy’ dietary pattern may have a protective effect against pre- and post-natal depression and potentially anxiety; however, the specific mechanisms surrounding these associations are not yet clear [11]. For example, a systemic review found a positive association between poor quality and unhealthy diets and prenatal depressive symptoms and that healthy diets were inversely associated with prenatal depressive and anxiety symptoms [12]. However, associations between perinatal diet and postnatal depressive remain inconsistent. Other previously studied factors increase the complexity of these mechanisms of action. This complexity is partly attributable to how nutrients are absorbed, processed, and utilized in the body during pregnancy and the ability to account for and accurately measure other factors that affect mental health. For example, Wang et al., found that in economically vulnerable women, a pro-inflammatory diet was associated with more prenatal depressive symptoms while the same association was not significant in women with a less-vulnerable economic status [13]. Research thus far has mainly focused on singular micronutrients or food groups with analyses restricted to dyadic correlations. This might fail to capture the complex interdependency between nutrients, the wider environment, and mental health. Additionally, many studies fail to adequately adjust for important confounders, including social determinants or history of mental health problems [14].
To address these issues, we propose the analytic framework of network analysis, which allows researchers to study dynamic systems of several mutually interacting components and their inter-relationships [15]. Often used in psychological research, this useful method enables the study of the complex interplay of variables whose nuance cannot be captured by traditional analytic procedures. Recently, network analysis has been proposed as a way to address “systems epidemiology” in which multiple risk factors can be simultaneously identified at a systems-level (e.g., clinical, biological, socio-economic) in place of the classic ‘one exposure’, ‘one outcome’ approach [16, 17]. Thus, our aim is not to produce an overall effect estimate but rather, visualize the inter-relationships between nutrition during pregnancy and maternal mental health, specifically the association between prenatal dietary patterns, nutrient intake, and the occurrence of symptoms of perinatal depression and anxiety in women in the French general population.
Methods and materials
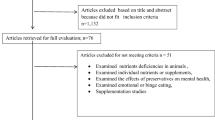
Analysis was based on data from the French EDEN (Etude sur les déterminants pré et post natals précoces du Développement psychomoteur et de la santé de l’Enfant) mother-child cohort [18]. This cohort was set up to assess the pre- and postnatal nutritional, social, and environmental determinants of infant and child development and health. Participants were pregnant women recruited between 2003 and 2006 at two university maternity clinics in Nancy and Poitiers, France. Exclusion criteria were multiple pregnancies, a history of diabetes, intention to deliver outside the university hospital or move out of the study region within the next 3 years, and the inability to speak or read French. Informed consent was obtained from the mother at inclusion. Birth data were obtained from 1899 mother-infant pairs. During pregnancy and after birth, sociodemographic and biomedical data on the mother were gathered from obstetrical records, in face-to- face interviews with the mother, and by the mother’s self-completed questionnaires. Ethical approval for the collection and use of this data was approved by the ethics committee of Kremlin Bicêtre and by the Commission Nationale Informatique et Liberté. The current study sample consists of 1438 women with available data from food frequency questionnaires collected at birth, and mental health outcomes (see Fig. 1, flowchart).

Study flowchart for EDEN cohort
Perinatal maternal Mental Health
To assess the intensity of symptoms of prenatal depression, the Center for Epidemiological Studies-Depression Scale (CES-D) [19] was self-completed by the mother at inclusion between the 24th and 28th week of pregnancy. This 20-item questionnaire measures the intensity of depressive symptoms over the past week (score ranging 0–60) [20, 21] with higher scores indicative of increased intensity of symptoms.
The ‘state’ portion of the State-Trait Anxiety Inventory (STAI) [22] was used to assess symptoms of prenatal anxiety in mothers at the same data collection wave. This 20-question self-assessment (range 20–80) rates items on a 4-point scale with higher scores indicating greater anxiety.
Depressive symptoms at four months post-partum were assessed using the Edinburgh Postnatal Depression Scale (EDPS) a 10-item questionnaire (score ranging 0–30) designed to screen women at risk of postnatal depression [23]. All questionnaires have been translated and validated in French [20, 24, 25] with all scores being treated as continuous variables in the analysis.
Prenatal maternal Nutrition
Maternal diet during the last trimester of pregnancy was assessed retrospectively during the mother’s stay at the maternity ward. Each participant completed a French validated Food Frequency Questionnaire (FFQ) that comprised 137 items with frequency ranges on a scale between ‘never’ and ‘more than once a day’ across seven categories. Portion sizes were determined using pictures for 12 food types (meat, French fries, pasta, vegetables, cakes, cheese etc.) on a three-level scale or were standard portions for the French adult population for other food types [26]. Each food item was assigned to one of the 44 food groups [27]. The nutrient composition database from the SU.VI.MAX study [26] was used to determine the nutrient content of foods and beverages. Nutrient values were only calculated for those women in the study who had two or fewer missing responses on the survey (n = 1599). The networks included the following macronutrients: total calories, vegetable protein, animal protein, saturated fats, monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), total cholesterol, carbohydrates, added sugars, and alcohol; and micronutrients: Vitamin A, Beta-carotene, Thiamin, Riboflavin, Niacin, Pantothenic Acid, Pyridoxine, Folic Acid, Cyanocobalamin, Ascorbic Acid, Vitamin D2 and D3, Tocopherol, Calcium, Iron, Iodine, Potassium, Magnesium, omega-3 fatty acid, and omega-6 fatty acid.
In a previous study, exploratory dietary patterns were derived by Principal Component Analysis (PCA, FACTOR procedure; SAS software) of the 44 standardized food groups consumed by more than half the sample [28]. The number of retained factors was determined by eigenvalues (the Scree plot) and based on their interpretability. A ‘Healthy’ dietary pattern (i.e., characterized by a high intake in fruits, vegetables, high fat dairy products, fish, legumes, and whole grains) and a ‘Western’ dietary pattern (i.e., characterized by a high intake of cakes, snacks, processed meat, prepared meals, soda, and chocolate) were identified. These two dietary patterns explained 10.8% (Western) and 6.8% (Healthy) variance of the first and second component of the PCA. A standardized score was calculated for each individual and pattern to quantify the individual’s adherence to the pattern. The current study uses these scores in our estimated networks as a continuous variable.
Covariates
Information regarding covariates was collected between the 24th and 28th week of gestation via a face-to-face interview, examination, or medical record from the obstetrician’s office. Sociodemographic characteristics were age, migrant status, income, education level (years of formal education obtained), partner status, and parity. Covariates related to health include pre-pregnancy body mass index (BMI, kg/m2), gestational diabetes diagnosis, anemia diagnosis (pre-pregnancy), hypertension (pre-pregnancy), presence of nausea and vomiting, and vitamin supplementation during the 3rd trimester. Psychosocial covariates were Adverse Childhood Events (ACEs: yes vs. no), and history of mental health problems (yes vs. no).
Statistical analysis
R (version 4.0.4) statistical software was used for data analysis. Descriptive analyses were performed on our sample (n = 1438) selected for network analysis based on exposure and outcome variable availability. Covariates included in the adjusted networks were determined based on subject knowledge and preliminary statistical testing using a p-value of 0.2. As the proportion of missing data was small (0.6%), all missing data points were removed. A complete case analysis was performed with the final data set as the missingness was determined to be missing completely at random [29, 30]. Preliminary data preparation and visualization analyses were run according to the guidelines provided by Epskamp et al. Networks were estimated using the R package mgm and plotted using the qgraph package which uses the Frutcherman-Reingold algorithm [31, 32]. Relevant patterns of interaction between variables can be visualized in a network structure in which variables are represented as ‘nodes’ while the presence of an ‘edge’ between any 2 nodes represents a conditional dependence relation (red = negative, green = positive, grey = undefined) which accounts for all other nodes in the network. Thus, the presence of an edge indicates a statistical relation, however, does not specify the direction of the relation. The absence of an edge between two nodes signifies that they are conditionally independent and have no association within the network. The color saturation and width of an edge become darker and wider in proportion to the strength of relationship (weight) between variables. Sensitivity analysis (LASSO) was set to gamma of 0 and 0.25. Thus, we were able to see edges regardless of their capacity for shrinkage [33, 34]. We compared both models using the Pearson’s correlations test of the two pairwise weighted matrices and predictability estimates.
Predictability, Node Centrality and Accuracy of Networks
We assessed the accuracy and stability of each network using centrality and predictability indices. Predictability refers to how well a node is predicted by its connected nodes [35] and is indicated by the colored perimeter of each node; centrality refers to the degree of connectivity a node has within the network [36]. These procedures inform the level of accuracy with which we can make inferences from our networks [37].
Results
Sample characteristics
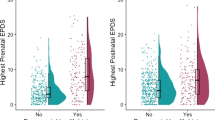
Table 1 presents the characteristics of our 1438 study participants who responded to the EPDS survey at 4 months. When compared to the initial cohort, respondents tended to be slightly younger, more educated, have a higher income, were married or in a legal partnership, and experienced fewer adverse childhood events. There were no differences in the means of the prenatal depression survey scores, while prenatal anxiety scores were slightly lower in respondents. Over half of participants (61%) reported giving up certain foods during pregnancy and 15.6% reported being diagnosed with anemia prior to pregnancy. Many women reported a history of mental health problems (22.4%) and/or experiencing adverse childhood events (35.9%). In our sample, 23.8% of women reported clinical level symptoms of prenatal depression (CES-D score ≥ 16), 20.2% clinical level symptoms of prenatal anxiety (STAI ≥ 17), and 14.9% clinical level symptoms of post-natal depression (EPDS score ≥ 11).
Network structure
Figures 2 and 3 present the fully regularized models (LASSO) unadjusted and adjusted network graphs. We report edge weights (r) and predictability (R2) that are most relevant to the study. All relationships between nodes as described below are in reference to Panel B, the adjusted models.

Network graph displaying the relationship between perinatal depression and anxiety scores symptoms and macronutrients before (panel A) and after controlling for covariates (panel B). Green edges signify positive partial correlations between variables, red edges signify negative partial correlations; shaded in dark purple rings around nodes relate the variance of that variable which represents to what extent it is explained by the nodes that connect to it
The network graphs for the Macronutrients (Fig. 2) show a relationship between the Western dietary pattern and the EPDS score (r = 0.022). The prenatal CES-D and STAI scores are connected to the postnatal EPDS by positive, strong edges. The Western and Healthy dietary patterns have an inverse relationship (r= -0.359). Inverse relationships with the education node also include Western dietary pattern, CES-D, and BMI (r= -0.114, r= -0.052, r= -0.077). Other edges that connect to the Western dietary pattern are total cholesterol, monosaturated fatty acids, added sugars, and alcohol (r = 0.176, r = 0.187, r = 0.383, r = 0.116).

Network graph displaying the relationship between perinatal depression and anxiety scores symptoms and micronutrients before (panel A) and after controlling for covariates (panel B)
For the Micronutrients networks (Fig. 3), the positive relationship between the Western dietary pattern and EPDS scores (r = 0.025) also appears. Additionally, associations amongst covariates and the Western dietary pattern are displayed in a similar fashion to the macronutrient model (‘education’ connects to the Western diet (r = -0.21), CES-D (r = -0.07), adverse childhood events (r = -0.18), and BMI (r = -0.08)). As with the macronutrient model, pre and postnatal mental health scores are also connected by green edges. The Healthy dietary pattern appears to be positively associated with many essential micronutrients (B9, r = 0.15, Beta-carotene, r = 0.24 Omega-3, r = 0.25, Vitamin E, r = 0.08). The Western dietary pattern is positively associated with the essential nutrient Iron (r = 0.2), vitamin D (r = 0.16), Omega-6 (r = 0.2) and vitamin A (r = 0.21).
Predictability, Node Centrality and Accuracy of Edges
The Healthy diet had the highest predictability indicating that it is highly dependent upon essential micronutrients (R2 = 0.849, Micronutrient adjusted). Node centrality measures are presented in Fig. 4 (Panel A macronutrient adjusted model; Panel B micronutrient adjusted model respectively). Results from the parametric bootstrap demonstrate that edges were estimated reliably (Additional files 1 and 1b). Additionally, the ‘edge difference test’ indicates that there is a statistically significant difference between the values of any two edges in our networks (Additional files 2 and 2b).

Node centrality measure of macronutrient (panel A) and micronutrient (panel B) network models. X-axis are z-scores
Discussion
To our knowledge, this is the first study to examine the relationship between prenatal nutrition and symptoms of depression and anxiety in the perinatal period using a network analysis approach. While previous literature has focused on either dietary patterns or isolated vitamins or minerals, we have elaborated on this research by identifying how both dietary patterns and their nutritional contents work in concert and may be associated with the intensity of perinatal depressive or anxious symptoms in the context of recognized risk factors. The intention of network analysis is not to present the traditional odds ratios, but rather to identify connections between a myriad of variables. In our networks, a Western dietary pattern was centrally located in both unadjusted and adjusted networks and either directly or indirectly connected with perinatal mental health and specific macro and micronutrients in a sample of women from the French general population. We found a small but positive association between postnatal depressive symptoms and prenatal Western dietary pattern score. Additionally, a Western dietary pattern and postnatal depressive symptoms were inversely linked by education. Contrary to previous findings [38, 39], we did not find associations between Healthy or Western diet patterns and symptoms of prenatal depression and anxiety or a relationship between postnatal depression scores and a Healthy dietary pattern. However, these results should be interpreted with caution, given the limitations of our study design and the possibility of reverse causality. History of mental health disorders and presence of prenatal mental health problems may likewise influence prenatal dietary choices, BMI, and a woman’s ability to adjust to the nutrient demands of pregnancy.
Western versus healthy dietary patterns and Perinatal Mental Health
When exploring the additional role of dietary patterns and nutrients in perinatal depression and anxiety, their interplay warrants diligent detangling. Strategically, we used dietary pattern scores to reflect general food consumption, as well as measured nutrient content (grams/milligrams) in each food item to explore how they might relate to perinatal mental health. While direct associations between specific micro or macronutrients and the studied mental health outcomes do not appear, the Western dietary pattern was associated with postnatal depression after adjustment for other factors.
At the macronutrient level, the Western dietary pattern was related to higher intakes of monounsaturated fatty acids and added sugars. There is biological plausibility such macronutrient imbalances may disrupt proper functioning of neurological pathways. For example, overconsumption of monounsaturated fatty acids leads to changes in the phospholipid neuromembrane altering the rate of transmission of serotonin, dopamine, and norepinephrine, and possibly increasing risk for perinatal mood disorders [40]. Of note, the pathophysiological and psychosocial challenges surrounding pregnancy could make it difficult for a woman to change her dietary pattern at a time when it is most important, leading to an exacerbation of an pre-existing imbalances [41]. In the context of other risk factors, a Western diet and its components could aggravate an underlying risk to experience increased depressive symptoms, whereas a Healthy diet pattern would not. However, more human research concerning the consequences of overconsumption of certain macronutrients typically found in the Western dietary pattern as it relates to the etiology of perinatal depression and anxiety mood is needed.
At the micronutrient level, the Western dietary pattern was associated with lower intakes of phytochemicals such as folate, cobalamin, and beta-carotene, found to be associated with mood in the general population [6, 42]. Systematic reviews examining micronutrient deficiencies in pregnant women reveal that iron, zinc, and selenium are associated with an increased risk of post-partum depression [43, 44]. Although it is likely that most of our study participants were not nutritionally deficient in micronutrients, building evidence suggests that an imbalance of essential micronutrients during pregnancy can also affect the mother’s biochemistry at the cellular level [45]. Specifically for pregnant women, meta-analyses indicate that an imbalance of polyunsaturated fatty acids (n-3 versus n-6) could be affiliated with perinatal depression [46, 47]. While we saw no direct link in our networks between increased omega-6 and perinatal depression and anxiety, the postnatal depression node was linked to omega-6 via the Western diet node (stronger, positive edge weight), suggesting that the imbalance in omega fatty acids could be of importance in the context of those at risk for postnatal depression symptoms.
Contributing factors
Finally, contrary to previous work, we have accounted for several contributing factors related to nutritional status and mental health. Previously studied risk factors of postnatal mood disorders appeared in our networks, namely prenatal symptoms of depression and anxiety, as well as mental health history. BMI is an important and well-studied confounder of diet patterns and mental health and risk of perinatal depression may be higher in women with increased BMI [48] Of note is that a prenatal Western dietary pattern was associated with a differentiated intake of certain nutrients and linked to BMI. An additional factor, education level, was associated with increased postnatal depression scores. Education level may reflect complexities regarding the ability to make appropriate choices about or access to nutrient-dense food. Higher education levels were previously associated with increased nutrient intake while lower income and educated groups were particularly lacking in micronutrients and diet quality. Moreover, it has been previously demonstrated that persons with a lower level of education or socioeconomic status experience a higher prevalence of mental health problems when compared to the general population [49]. Thus, it is possible that the consumption of a Western diet is one specific mechanism of action through which lower educational achievement, working in tandem with other biological and psychosocial risk factors, could contribute to postnatal depression.
Strengths and Limitations
A strength of our study is its comprehensive approach in its attempt to disentangle the contribution of nutritional components in perinatal depressive and anxiety symptoms. Previous studies have tested one or few nutritional components in relation to perinatal depression and anxiety and have shown that certain macro- and micronutrients are beneficial. We used network analysis to identify patterns among these nutrients and related variables, and in addition, show that the Healthy dietary pattern is a correlate of the beneficial components which are lacking in a Western dietary pattern. We consider our study robust in that data from a large cohort gave our networks sufficient power. Moreover, this cohort is similar to other European mother-child dyad cohorts which could be used to easily replicate our study. Finally, our data analysis included the most conservative estimates and sensitivity testing of our networks so that only the most rigorous networks remained.
However, we should also acknowledge some limitations. First, both the dietary patterns and nutrient intakes were derived from a single time point food frequency questionnaire. We are limited in our lack of postnatal FFQs to verify the sustainability of the identified diet patterns and health behaviors that tend to fluctuate around the pregnancy period. Additionally, dietary patterns were assessed retrospectively at birth, introducing recall bias, and may not accurately measure nutrient intake during pregnancy. Although the FFQ has been validated, increasing confidence in the accuracy of its scores, biological samples of serum blood would be a more precise way to assess perinatal nutritional status at the micronutrient level and would allow to highlight nutrient deficiencies. Notwithstanding, it may take months before changes in dietary pattern are reflected in plasma levels of macro- and micronutrients, thus it is possible that the FFQ may be a more proximate measure to the time period in which our outcomes were assessed. Other methods to assess dietary intake, such as glycemic load, could lend further insights to the mechanism of action among these associations. For example, Wilson et al. found in a cohort of obese women that increased glycemic load was associated with a slight increase in depressive symptoms during the perinatal period [50]. Longitudinal cohort studies in which time-series data are collected would be needed to specify the evolution of nutritional status changes often associated with pregnancy and further clarify the exact role of dietary patterns in the context of perinatal mental health. Second, women’s mental health scores were self-reported and do not represent any official clinical evaluation of mental health status. It is important to highlight that the CES-D, STAI, and EPDS are not diagnostic tools and although used frequently in epidemiological studies, were created as screening devices to assess the presence of symptoms. However, all three scales have previously been validated in French and their continuous scores enabled us to study variations in symptomatology at the population level. Lastly, while network analysis allows for valuable global insights and pattern identification, it is statistically limited in its ability to make causal inferences and quantify risks. Our analysis uses the mixed graphical model which treats all variables equally and does not address temporality. In the instance that time-series data is available, more robust conclusions would be possible using the Vector Autoregressive Model to account for changes in nutrition status across time [31].
Recommendations
Perinatal depression and anxiety are far-reaching public health issues that influence the health of mother, baby and the family unit. Improving dietary patterns and nutritional intake could be a safe, low-risk option to prevent or improve symptoms of depression and anxiety, and inherently has added benefits related to general health and wellness of the mother and development of the fetus. Nutritional intake is measurable, and deficits are easily recognized during preconception and in early pregnancy. Early discussion of dietary requirements and subsequent nutritional counseling is paramount in standard prenatal care. While very few nutritional counseling programs have been proven effective in the public sector, a recent systematic review assessed dietary intervention programs for pregnant women. It found that while effectiveness of the programs varied, almost half of the programs demonstrated an improvement in dietary behaviors and nutrition status of the women [51]. Nevertheless, more research is needed about the effectiveness of nutritional intervention programs and specifically, programs geared towards at-risk populations. In addition, whether improvement in nutritional intake during pregnancy leads to positive improvements with respect to maternal mental health status is still to be shown.
Conclusion
The current study was the first to use network analysis to explore the associations between perinatal mental health and nutrition. Overall, our study provides additional evidence to support the theory that dietary pattern is related to the intake of essential micronutrients, and that a Western dietary pattern might adversely affect maternal postnatal mental health. As nutritional status is linked to dietary pattern, which is potentially influenced by education level, future studies should evaluate the effects of nutritional status on perinatal mental health within the context of other psychosocial risks.
Data Availability
The data that support the findings of this study are available from the EDEN consortium but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the EDEN consortium.
Abbreviations
- ACE:
-
adverse childhood events
- SES:
-
socioeconomic status
- EDEN:
-
Etude sur les déterminants pré et post natals précoces du Développement psychomoteur et de la santé de l’Enfant
- CES-D:
-
Center for Epidemiological Studies-Depression Scale
- STAI:
-
State-Trait Anxiety Inventory
- EDPS:
-
Edinburgh Postnatal Depression Scale
- FFQ:
-
Food Frequency Questionnaire
- SU.VI.MAX:
-
Supplementation en Vitamines et Mineraux Antioxydants
- MUFA:
-
monounsaturated fatty acids
- PUFA:
-
polyunsaturated fatty acids
- PCA:
-
principal component analysis
- BMI:
-
body mass index
- LASSO:
-
least absolute shrinkage and selection operator
References
Aktar E, Qu J, Lawrence PJ, Tollenaar MS, Elzinga BM, Bögels SM et al. Fetal and infant outcomes in the offspring of parents with Perinatal Mental Disorders: Earliest Influences. 2019;10(391). Available from: www.frontiersin.org.
Woody CA, Ferrari AJ, Siskind DJ, Whiteford HA, Harris MG. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. 2017;219:86–92.
Dennis CL, Falah-Hassani K, Shiri R. Prevalence of antenatal and postnatal anxiety: systematic review and meta-analysis. Br J Psychiatry. 2017;210(5):315–23.
Hutchens BF, Kearney J. Risk factors for Postpartum Depression: an Umbrella Review. J Midwifery Womens Health. 2020;65(1):96–108.
Guintivano J, Manuck T, Meltzer-Brody S. Predictors of Postpartum Depression: a Comprehensive Review of the last decade of evidence. Clin Obstet Gynecol. 2018;61(3):591–603.
Arab A, Mehrabani S, Moradi S, Amani R. The association between diet and mood: a systematic review of current literature. Psychiatry Res. 2019;271:428–37.
Fish-Williamson A, Hahn-Holbrook J. Nutritional factors and cross-national postpartum depression prevalence: an updated meta-analysis and meta-regression of 412 studies from 46 countries. Front Psychiatry. 2023;14:1193490.
Rippin HL, Hutchinson J, Greenwood DC, Jewell J, Breda JJ, Martin A, et al. Inequalities in education and national income are associated with poorer diet: pooled analysis of individual participant data across 12 european countries. PLoS ONE. 2020;15(5):e0232447–7.
Most J, Dervis S, Haman F, Adamo KB, Redman LM. Energy Intake requirements in pregnancy. Nutrients. 2019;11(8):1812.
Davis C, Bryan J, Hodgson J, Murphy K. Definition of the mediterranean diet: a literature review. Nutrients. 2015;7(11):9139–53.
Khan R, Waqas A, Bilal A, Mustehsan ZH, Omar J, Rahman A. Association of maternal depression with diet: a systematic review. Asian J Psychiatry. 2020;52(102098):1–11.
Baskin R, Hill B, Jacka FN, O’Neil A, Skouteris H. The association between diet quality and mental health during the perinatal period. A systematic review. Appetite. 2015;91:41–7.
Wang P, Yim IS, Lindsay KL. Maternal Diet quality and prenatal depressive symptoms: the moderating role of Economic Well-Being. Nutrients. 2023;15(12):2809.
Sparling TM, Nesbitt RC, Henschke N, Gabrysch S. Nutrients and perinatal depression: a systematic review. J Nutr Sci. 2017;6(e61):1–13.
Luke DA, Harris JK. Network analysis in public health: history, methods, and applications. Annu Rev Public Health. 2007;28:69–93.
Park J, Choi J, Choi JY. Network Analysis in Systems Epidemiology. J Prev Med Pub Health. 2021;54(4):259–564.
Dammann O, Gray P, Gressens P, Wolkenhauer O, Leviton A. Systems Epidemiology: what’s in a name? Online J Public Health Inform. 2014;6(3):e198.
Heude B, Forhan A, Slama R, Douhaud L, Bedel S, Saurel-Cubizolles MJ, et al. Cohort Profile: the EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int J Epidemiol. 2016;45(2):353–63.
Radloff LS, The CES-D, Scale. A self-report Depression Scale for Research in the General Population. Appl Psychol Meas. 1977;1(3):385–401.
Fuhrer R, Rouillon F. La version française de l’échelle CES-D (center for epidemiologic Studies-Depression Scale). Description et traduction de l’échelle d’autoévaluation. [The french version of the CES-D (center for epidemiologic Studies-Depression Scale)]. Psychiatr Psychobiol. 1989;4(3):163–6.
Joiner TE, Walker RL, Pettit JW, Perez M, Cukrowicz KC. Evidence-based assessment of depression in adults. Psychol Assess. 2005;17(3):267–77.
Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the state-trait anxiety inventory. Consult Psychol Press Palo Alto; 1983.
Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry J Ment Sci. 1987;150:782–6.
Gauthier J, Bouchard S. Adaptation canadienne-française de la forme révisée du state–trait anxiety Inventory de Spielberger. [A french-canadian adaptation of the revised version of Spielberger’s state–trait anxiety Inventory]. Can J Behav Sci Rev Can Sci Comport. 1993;25(4):559–78.
Guedeney N, Fermanian J. Validation study of the french version of the Edinburgh postnatal depression scale (EPDS): new results about use and psychometric properties. Eur Psychiatry J Assoc Eur Psychiatr. 1998;13(2):83–9.
Hercberg S. The SU.VI.MAX study, a randomized, placebo-controlled trial on the effects of antioxidant vitamins and minerals on health. Ann Pharm Fr. 2006;64(6):397–401.
Deschamps V, de Lauzon-Guillain B, Lafay L, Borys JM, Charles MA, Romon M. Reproducibility and relative validity of a food-frequency questionnaire among french adults and adolescents. Eur J Clin Nutr. 2009;63(2):282–91.
Yuan WL, Nicklaus S, Lioret S, Lange C, Forhan A, Heude B, et al. Early factors related to carbohydrate and fat intake at 8 and 12 months: results from the EDEN mother–child cohort. Eur J Clin Nutr. 2017;71(2):219–26.
Ross RK, Breskin A, Westreich D. When is a complete-case Approach to Missing Data Valid? The importance of effect-measure modification. Am J Epidemiol. 2020;189(12):1583–9.
RUBIN DB. Inference and missing data. Biometrika. 1976;63(3):581–92.
Haslbeck JMB, Waldorp LJ. MGM: estimating time-varying mixed graphical models in high-dimensional data. J Stat Softw. 2020;93(Feb).
Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of Relationships in Psychometric Data. J Stat Softw. 2012;48:1–18.
Tibshirani R. Regression shrinkage and selection via the Lasso. J R Stat Soc Ser B Methodol. 1996;58(1):267–88.
Fried EI, Von Stockert S, Haslbeck JMB, Lamers F, Schoevers RA, Penninx BWJH. Using network analysis to examine links between individual depressive symptoms, inflammatory markers, and covariates. Psychol Med. 2020;(October):2682–90.
Haslbeck JMB, Waldorp LJ. How well do network models predict observations? On the importance of predictability in network models. Behav Res Methods. 2018;50(2):853–61.
Fried EI, Epskamp S, Nesse RM, Tuerlinckx F, Borsboom D. What are “good” depression symptoms? Comparing the centrality of DSM and non-DSM symptoms of depression in a network analysis. J Affect Disord. 2016;189:314–20.
Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2017;50(1):195–212.
Avalos LA, Caan B, Nance N, Zhu Y, Li DK, Quesenberry C, et al. Prenatal Depression and Diet Quality during pregnancy. J Acad Nutr Diet. 2020;120(6):972–84.
Barker ED, Kirkham N, Ng J, Jensen SKG. Prenatal maternal depression symptoms and nutrition, and child cognitive function. Br J Psychiatry. 2013;203(6):417–21.
Rechenberg K, Humphries D. Nutritional interventions in depression and perinatal depression. Yale J Biol Med. 2013;86(2):127–37.
Ker CR, Wu CH, Lee CH, Wang SH, Chan TF. Increased sugar-sweetened beverage use tendency in pregnancy positively associates with peripartum Edinburgh postpartum depression scores. Sci Rep. 2021;11(1):15324.
Bahramsoltani R, Farzaei MH, Farahani MS, Rahimi R. Phytochemical constituents as future antidepressants: a comprehensive review. Rev Neurosci. 2015;26(6):699–719.
Azami M, Badfar G, Khalighi Z, Qasemi P, Shohani M, Soleymani A, et al. Review article the association between anemia and postpartum depression: a systematic review and meta-analysis. Casp J Intern Med. 2019;10(2):115–24.
Ellsworth-Bowers ER, Corwin EJ. Nutrition and the psychoneuroimmunology of postpartum depression. Nutr Res Rev. 2012;25(1):180–92.
Bordeleau M, Fernández de Cossío L, Chakravarty MM, Tremblay M. From maternal Diet to Neurodevelopmental Disorders: A Story of Neuroinflammation. Front Cell Neurosci. 2020;14:612705.
Hsu MC, Tung CY, Chen HE. Omega-3 polyunsaturated fatty acid supplementation in prevention and treatment of maternal depression: putative mechanism and recommendation. J Affect Disord. 2018;238(April):47–61.
Lin PY, Chang CH, Chong MFF, Chen H, Su KP. Polyunsaturated fatty acids in Perinatal Depression: a systematic review and Meta-analysis. Biol Psychiatry. 2017;82(8):560–9.
de Los Reyes S, Dude A, Adams M, Castille D, Ouyang DW, Plunkett BA. The association between maternal body Mass Index and the risk of Perinatal Depression. Am J Perinatol. 2023;40(2):222–6.
Steele L, Dewa C, Lin E, Lee K, Education, Level. Income level and Mental Health Services Use in Canada: Associations and Policy Implications. Healthc Policy Polit Santé. 2007;3(1):96–106.
Wilson CA, Seed P, Flynn AC, Howard LM, Molyneaux E, Sigurdardottir J, et al. Is there an Association between Diet, physical activity and depressive symptoms in the Perinatal Period? An analysis of the UPBEAT cohort of obese pregnant women. Matern Child Health J. 2020;24(12):1482–93.
Beulen YH, Super S, de Vries JHM, Koelen MA, Feskens EJM, Wagemakers A. Dietary interventions for healthy pregnant women: a systematic review of tools to promote a healthy antenatal dietary intake. Nutrients. 2020;12(7):1–23.
Acknowledgements
We express our deep gratitude for the mothers and families who have participated in the EDEN cohort and continue to volunteer their valuable time and energy in helping further this research. The EDEN mother–child cohort study group includes I Annesi-Maesano, JY Bernard, J Botton, M-A Charles, P Dargent-Molina, B de Lauzon-Guillain, P Ducimetière, M de Agostini, B Foliguet, A Forhan, X Fritel, A Germa, V Goua, R Hankard, B Heude, M Kaminski, B Larroque, N Lelong, J Lepeule, G Magnin, L Marchand, C Nabet, F Pierre, R Slama, MJ Saurel-Cubizolles, M Schweitzer, O Thiebaugeorges. The EDEN cohort study is supported by Foundation for Medical Research (FRM), National Agency for Research (ANR), National Institute for Research in Public Health (IRESP: TGIR cohorte santé 2008 programme), French Ministry of Health (DGS), French Ministry of Research, Inserm Bone and Joint Diseases National Research (PRO-A) and Human Nutrition National Research Programmes, Paris–Sud University, Nestlé, French National Institute for Population Health Surveillance (InVS), French National Institute for Health Education (INPES), the European Union FP7 programmes (FP7/2007–2013, HELIX, ESCAPE, ENRIECO, Medall projects), Diabetes National Research Programme (through a collaboration with the French Association of Diabetic Patients (AFD)), French Agency for Environmental Health Safety (now ANSES), Mutuelle Générale de l’Education Nationale (MGEN), French National Agency for Food Security and the French-speaking association for the study of diabetes and metabolism (ALFEDIAM). Funders had no influence of any kind on analyses or result interpretation.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceptualization BK and JW; Data curation BK; Methodology BK, CG, JW; Formal Analysis BK; Writing – Original Draft Preparation BK JW; Writing – Review & Editing BK, CG, ALSD, BH, BLG, JW; Supervision JW; Funding Acquisition BH.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Ethics approval and consent to participate
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from participants at study inclusion. Ethical approval for the collection and use of this data was approved by the ethics committee of Kremlin Bicêtre and by the Commission Nationale Informatique et Liberté.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplement 1:
Bootstrapped difference test Macronutrient network model, adjusted. The grey area represents the bootstrapped confidence intervals, while the black line represents the sample values (edges). Supplement 1b: Bootstrapped difference test Micronutrient network model, adjusted.
Supplement 2:
Edge-weight bootstrapped difference test, Macronutrient adjusted model. Supplement 2b: Edge-weight bootstrapped difference test, Micronutrient adjusted model.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Knox, B., Galera, C., Sutter-Dallay, AL. et al. A network analysis of nutritional markers and maternal perinatal mental health in the French EDEN cohort. BMC Pregnancy Childbirth 23, 603 (2023). https://doi.org/10.1186/s12884-023-05914-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05914-w