
Abstract
Background
The association between serum 25-hydroxy vitamin D (25(OH)D) status and gestational diabetes mellitus (GDM) gained attention in recent years, however the conclusion is still controversial due to many interfering factors, such as region of living, environment, lifestyle, and food supplements. Other metabolites (laboratory parameters) are also important in reflecting gestational states. This study aimed to investigate the association of serum 25(OH)D status in early pregnancy with GDM and other laboratory parameters in pregnant women.
Methods
A total of 1516 pregnant women whose blood glucose were normal before pregnancy in the city of Foshan in Guangdong, China were enrolled in this study. GDM was diagnosed between 24 to 28 weeks of pregnancy following the guidelines from the American Diabetes Association. Maternal serum 25(OH)D and other laboratory parameters—including hematology, coagulation, chemistry, and bone density—were measured utilizing various analytical methods in clinical laboratory at gestational weeks 11 to 14.
Results
The average 25(OH)D concentration was 59.1 ± 12.6 nmol/L. None of the study subjects had 25(OH)D < 25 nmol/L; 434 (28.6%) women had 25(OH)D deficiency (< 50 nmol/L), 882 women (58.2%) had 25(OH)D insufficiency (50–74 mmol/L) and 200 women (13.2%) had 25(OH)D sufficiency (≥ 75 nmol/L). There were 264 (17.4%) women diagnosed with GDM. There was not, however, an association between serum 25(OH)D in early pregnancy and GDM. Interestingly, women with more parity and high serum alkaline phosphatase levels had higher serum 25(OH)D levels. There was a possible positive association between serum 25(OH)D and pre-albumin, and a possible negative association between serum 25(OH)D, creatinine, and thrombin time. This study did not find an association between serum 25(OH)D and bone density.
Conclusions
There were no associations between maternal serum 25(OH)D concentration in early pregnancy and the risk of GDM or bone density. There were, however, correlations between serum 25(OH)D and parity, seasoning at sampling, serum alkaline phosphatase, creatinine, pre-albumin, and coagulation factor thrombin time, which need further study to explain their pathophysiology and clinical significance.
Similar content being viewed by others


Background
Vitamin D is a fat-soluble vitamin, which plays an important role in bone mineralization, calcium and phosphorus absorption, parathyroid status, and immune system functionality [1]. In the human body, vitamin D from sunlight and food is hydroxylated to 25-hydro vitamin D (25(OH)D) in the liver and is subsequently activated with a second hydroxylation to 1,25-dihydroxy vitamin D in the kidney [2].
Studies have found that during pregnancy calcitriol increases in early gestation to meet a mother’s needs, and maternal serum 25(OH)D crosses into the placenta for use in fetus development [3]. Serum 25(OH)D below 50 nmol/L is defined as vitamin D deficiency, while it is defined as insufficiency if the level of 25(OH)D is in between 52–74 nmol/L, only when the level reaches 75 nmol/L or higher is deemed sufficient [4,5,6,7,8]. Insufficient vitamin D levels may cause some adverse pregnancy complications, including polycystic ovary syndrome, gestational diabetes mellitus (GDM), pre-eclampsia, infertility, endometriosis, and cancers [9,10,11,12]. Studies on the association between vitamin D status and pregnancy complications are still controversial because serum vitamin D level is affected by many factors, such as climate, region of living, life style and diet, physical exercise, and food supplements that pregnant women may have consumed during pregnancy. A meta-analysis of 29 observational studies indicated that vitamin D deficiency was related to increased risk of gestational diabetes [13]. Nevertheless, Pérez-López et al. found that there was no association between vitamin D supplementation and the risk of GDM in a systematic review and meta-analysis of randomized controlled trials [14]. Thus, in this study, we wanted to see whether there is an association between serum 25(OH)D level and adverse pregnancy effects, including GDM, in pregnant women living in the Foshan area of Guangdong Province in China.
In addition, laboratory parameters and metabolites may indicate certain clinical complications of the pregnant women and thus guiding the clinical management. The greatest magnitude increase in multiple micronutrient supplements use occurred in women of parity ≥ 2 [15]. Li et al. reported that vitamin D played a role in promoting alkaline phosphatase (ALP) activity [16]. While a systematic review and meta-analysis of interventional studies showed association between serum 25(OH)D and bone density [17]. In addition, vitamin D supplementation might have contributed to liver and kidney fuction [18]. Interestingly, Bouillon [19] mentioned that vitamin D might affect blood coagulation. Therefore, we also had an interest in understanding whether parity, bone density, clinical chemistry and hematology parameters such as serum ALP, creatinine (Cre), pre-albumin (Pre-Alb), coagulation factors including thrombin time (TT), activated partial thromboplastin time (aPTT), D-dimer, and fibrinogen (Fib) level have anything to do with serum vitamin D, GDM, and pregnant adverse effects. Following these concepts, the routine clinical laboratory parameters as mentioned above were screened and analyzed as an important part of our observation in this study.
Our study followed the policies regarding the management and medical practice on pregnant women and newborns by the Chinese Medical Association and Chinese government, which require all pregnant women be closely monitored during pregnancy. We therefore proposed this study to offer a more detailed observation of the metabolic criteria, including the association between maternal serum 25(OH)D levels in early pregnancy, GDM, and other laboratory parameters in pregnant women. We hoped to better understand metabolic events and their potential effects on fetus development, as well as their potential diagnostic and prognostic applications.
Patients and methods
Patient enrollment and ethics approval
This was a prospective cohort study for a grant supported by the Foshan Science and Technology Bureau Project (2018AB000251) of Guangdong, China. During the study, a total of 241,651 pregnant women who visited our hospital for scheduled check-ups during the prenatal period at Foshan Women and Children’s Hospital of Southern Medical University, a specialized tier-3, grade-A hospital in South China, were examined. Of them, 12,536 women were giving birth, of which after excluding those with medical conditions such as diabetes and hypertension as described below, and also on voluntary enrollment basis, a total of 1,516 women, ages 18 to 46, were recruited from August 1, 2018 to August 31, 2019. The relevant information of those early pregnant women who met the criteria of the study was collected and serum 25 (OH) D and other laboratory testing were performed during early pregnancy. Pregnant women continued regular antenatal examination and follow-up until the termination of pregnancy. Women who had pregestational diabetes mellitus (PGDM), malignant diseases or missing OGTT data, or pregestational hypertension were excluded from the study. Exclusion criteria included pre-existing diabetes, hypertension or other chronic diseases, abnormal child-bearing history, a history of drug use, and vitamin supplements—including vitamin D and calcium—that may affect metabolism or unavailable data. Pregnant women with singleton pregnancies and conceiving naturally were included. All pregnant women exerted a normal daily life without special sunlight exposure or quarantines. All study subjects were living in the Foshan, Guangdong Province of South China. Ethics approval was obtained by the Institutional Review Board (IRB) and Ethics Committee of Foshan Women and Children’s Hospital of Southern Medical University. All methods were carried out in accordance with relevant guidelines and regulations. Methods and laboratory testing followed standard operating procedures required for medical practice in Guangdong Province, including in this hospital. All participants provided written informed consent.
Serum 25(OH)D analysis
Serum total 25(OH)D concentration was analyzed at gestational weeks 11 to 14 using a Mokosensor-A300 immune colloidal gold analyzer (MedicalSystems, Ningbo, China) following the manufacturer’s instructions. Briefly, 2 ml of blood was sampled from pregnant women at weeks 11–14 of gestation using an EDTA anti-coagulant blood tube. The blood sample was delivered to clinical laboratory immediately after sampling. Twenty microliters of whole blood were used for the analysis. The accuracy of the assay was from 85–115%, while the precision of the assay was ≤ 15% (coefficient of variation, CV). According to the Vitamin D Standardization-Certification Program (VDSCP) guidelines, a CV of < 15% is close to acceptable in the analysis [20,21,22].
The statuses of maternal serum 25(OH)D were categorized into three groups: 25(OH)D deficiency (< 50 nmol/L), 25(OH)D insufficiency (50–74 nmol/L), and 25(OH)D sufficiency (≥ 75 nmol/L).
Chemistry analysis
Other blood chemistry parameters also came from the samples collected during weeks 11 to 14 of gestation. Specifically, alkaline phosphatase, pre-albumin, creatinine, cystatin C, calcium, and magnesium were analyzed on a Beckman-Coulter Automatic Chemistry Analyzer platform (Beckman-Coulter, Brea, CA, USA) following the manufacturer’s instructions and laboratory operating procedures. The collection of blood samples, including the selection of a collecting tube, followed routine clinical laboratory procedures.
Glucose tolerance test
A 75 g oral glucose tolerance test (75 g OGTT) was performed between 24 and 28 weeks of gestation. Pregnant women who had a fasting glucose level < 5.1 before pregnancy were enrolled in the study. The diagnosis of GDM was defined according to the American Diabetes Association [23] using the following protocol: A 75 g oral glucose tolerance test (75 g OGTT) was performed between weeks 24 and 28 of gestation. Either of the following criteria met was diagnosed as GDM: fasting serum glucose ≥ 5.1 mmol/L, or 1 h of OGTT serum glucose ≥ 10 mmol/L, or 2 h of OGTT serum glucose ≥ 8.5 mmol/L).
Coagulation test
The blood coagulation test was performed on a Stago STA-R Evolution (Diagnostica Stago, Asnières sur Seine Cedex, France) platform following the manufacturer’s instructions using a heparin anti-coagulant blood collection tube collected during weeks 11 to 14 of gestation. The coagulation parameters include thrombin time (TT), activated partial thromboplastin time (aPTT), fibrinogen (Fib), and D-dimer.
Bone density examination
Bone density was measured using a Hong Yang BMD-1000 Ultrasound Bone Sonometer (Baoding, Hebei, China) by a specialist in our hospital following the protocol provided by the manufacturer. Pregnant women at weeks 11–14 of gestation were assigned for bone density measurement of the distal radius for 2 min. In brief, the Z value is obtained by comparing the sonographic value of the bone of a patient with a reference (same age, same sex). Thus, bone density was expressed as Z-scores.
Statistical analysis
Statistical analysis was performed using the SPSS (version 24). Continuous variables are reported as mean ± standard deviation or median (interquartile), while categorical variables are presented as frequencies and percentages. For continuous variables, hypothesis testing for significant differences was performed using One-Way ANOVA and Nonparametric Tests for normal and non-normal distribution data, respectively. Pearson’s chi-square was used for categorical variables. Post Hoc Multiple Comparison was used to further identify significant differences among groups. Possible confounding factors with p < 0.20 were entered into multiple linear regression analysis to explore independent influencing factors of 25(OH)D. Spearman coefficient was used to determine the correlation between 25(OH)D status and pregnant outcomes. Unadjusted and adjusted logistic regression analysis were used to calculate the crude or adjusted odds ratios (OR), and their 95% confidence intervals (CI) were used to evaluate the relationship between 25(OH)D and GDM and other parameters (gestational adverse events). Variables with p < 0.10 in unadjusted analysis and possible confounding factors were entered into multivariable logistic regression procedure. The model’s adequacy was assessed by predicting correct percentage. A p < 0.05 were considered statistically significant.
Results
Association between maternal and clinical characteristics and 25(OH)D status
In this observation, the average 25(OH)D concentration was 59.1 ± 12.6 nmol/L; none of the women had 25(OH)D < 25 nmol/L. Four hundred and thirty-four (434, 28.6%) women had 25(OH)D < 50 nmol/L, 882 women (58.2%) had 25(OH)D insufficiency (50–74 nmol/L), and 200 (13.2%) women had 25(OH)D ≥ 75 nmol/L. Pre-adjusted analysis using the Chi-square test, One-way ANOVA, and nonparametric test results that the maternal and clinical characteristics are listed in Table 1 on the basis of 25(OH)D status. Table 1 also shows that serum 25(OH)D varies significantly in regard to season at sampling. Serum alkaline phosphatase (ALP), pre-albumin, creatinine, and thrombin time (TT) also differed upon different serum 25(OH)D status (p < 0.05 for all). However, the categories of pre-albumin and creatinine, as well as the rest of variables in the list, do not show difference based on 25(OH)D status.
Association between parity, season at sampling, and laboratory parameters and 25(OH)D concentrations
Tables 2 and 3 show the association between maternal serum 25(OH)D concentrations and parity, season at sampling, serum alkaline phosphatase. Women going into birth ≥ 2 times had a higher 25(OH)D concentration than those with 1 or 0 paritys (p = 0.018 and p = 0.044 respectively). The same result was found in adjusted linear analysis (p = 0.010 and p = 0.032, respectively). There was a significant difference in 25(OH)D concentrations among samples collected in different seasons; the 25(OH)D concentrations assended in the order of spring, winter, summer, and autumn. There was a significant difference between serum 25(OH)D concentration and alkaline phosphatase activities, of which a higher serum 25(OH)D concentration tended to have higher alkaline phosphatase activities (p = 0.005 and 0.004, respectively).
Correlation of 25(OH)D status with GDM and other pregnancy adverse events
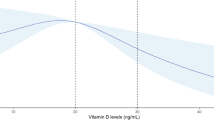
As shown in Table 4, results from spearman correlation analysis indicate that there is no correlation between vitamin D status and adverse outcomes in early gestating women (p > 0.05 for all). Interestingly, the rate of 1 h GTT positive (r = -0.037) and 2 h GTT positive (r = -0.037) was inversely correlated with the increament of serum 25(OH)D status, but with no significance (p = 0.145 and 0.534, respectively).
Association between maternal 25(OH)D status and gestational diabetes mellitus
Logistic regression analysis was performed to assess the association between serum 25(OH)D and gestational diabetes mellitus. In this study, we found that there was no association between 25(OH)D and the risk of GDM, as shown in Table 5. In unadjusted logistic regression analysis, no significant difference was observed between maternal 25(OH)D and GDM (p = 0.627). After adjusted by age, parity, and season at sampling, women with serum 25(OH)D ≥ 75 nmol/L (vitamin D sufficient) were grouped as the reference group, while women whose serum 25(OH)D between 50–74 nmol/L (vitamin D insufficient), or < 50 nmol/L (vitamin D defficient) groups were compared with the reference group. The results indicated that there was no association between serum 25(OH)D and GDM, with an odds ratio of 1.250 (95%CI 0.763–2.046, P = 0.376) and 1.224 (95%CI 0.794–1.888, P = 0.360), respectively. GDM women were more likely to be older than those without GDM.
Discussion
The aim of this study was to assess vitamin D status in pregnant women in the Foshan area of Guangdong, China and to test for an association between gestational diabetes and adverse pregnancy events, and to compare those results with other reports [24,25,26,27,28,29,30].
Our study results did not show an association between maternal serum 25(OH)D status and GDM and other types of pregnant adverse events, including gestational hypertension, premature rupture of membrane, postpartum hemorrhage, and low body weight of newborns. This result is similar with a previous meta analysis report [31]. A randomized controlled trial also showed a limitation of vitamin D supplementation for GDM prevention in vitamin D sufficient populations [32].
Our results showed that the mean 25(OH)D concentration of the subjects was 59.1 nmol/L. Comparing to other studies in China, our study indicated that serum 25(OH)D < 50 nmol/L in early pregnant women was a relatively low prevalence (28.6%). While another report showed that the mean serum 25(OH)D in pregnant women was 40.1 nmol/L and 25(OH)D < 50 nmol/L accounted for 76.4% in Hefei [33]; a study conducted by Song et al. [34] also reported that the mean maternal 25(OH)D concentration was 28.6 nmol/L and more than 90% of pregnant women had 25(OH)D < 50 nmol/L in Beijing. These contradictory results might be attributed to the analytical methods used in different studies. For instance, serum 25(OH)D analysis can be measured by LC–MS/MS spectrometry, chemiluminescent immunoassay, high performance chromatography (HPLC), and immune colloidal gold methods, etc. This phenomenon could be due to the climate and sun exposure difference between the South and the North. Our results showed that sampling at different seasons had an effect on serum 25(OH)D concentrations, in accordance with public understanding. There was also a correlation between serum alkaline phosphatase, pre-albumin, creatinine, and thrombin time and serum 25(OH)D concentrations.
Since the significance of association between parity and serum 25(OH)D concentration before adjustment was weak, we performed additional stratified analyses using One-Way ANOVA and Post Hoc Multiple Comparison, followed by multiple linear regression. Results indicated a positive association between maternal serum 25(OH)D concentration and the number of parity. One study mentioned that there was no significant difference between serum 25(OH)D concentration and age, parity, or gestational age [35], and no association between parity and 25(OH)D concentration was observed in another study [36]. While Shen et al. found that high parity was associated with increasing serum vitamin D status [37]. The mechanism underlying this phenomenon is therefore unclear. There could be certain compensation in metabolism function during pregnancy that requires further investigation. From our clinical experience in Foshan China, women gained experience in how to deal with pregnancy with more parity going; they tended to get more sun exposure and a nutrient-rich diet, and these facts could have contributed to the results.
Women who had high serum vitamin D also had higher alkaline phosphatase activity. A study observed that there was an association between alkaline phosphatase activity and moderate vitamin D deficiency group; however, the correlation was not significant [38]. Another study also found that there was no correlation between alkaline phosphatase activity and vitamin D status in school children [39].
Serum alkaline phosphatase activity is widely used in clinical practice as a marker of bone turnover [40]. Medical conditions with osteolysis had elevated serum alkaline phosphatase activity levels [41]. Based on our results, we hypothesize that there is a relationship between vitamin D and alkaline phosphatase in maintaining bone and mineral metabolic homeostasis—a hypothesis that merits further investigation.
Serum pre-albumin could be a marker indicating malnutrition and other potential pathological conditions, such as inflammation, in clinical practice [42]. In interpreting pregnant women who had low serum vitamin D status (vitamin D deficient) and low pre-albumin concentration, we hypothesize that there is a relationship between serum vitamin D and pre-albumin, either acting as a nutrition factor or inflammation index, as also suggested in other study [43]. The detailed mechanism of the association between these two factors requires further investigation. Liu et al. [44] found that serum pre-albumin levels were correlated with gestational diabetes mellitus status, and they hypothesized that pre-albumin can be used as an indicator to reflect the presence of gestational diabetes mellitus.
Serum creatinine is considered a useful biomarker for diagnosis of renal function and is widely used in clinical practice [45, 46]. One study found that vitamin D receptor activation increased creatinine generation and serum creatinine level and may play a role in renal function regulation [47]. Higher serum creatinine levels in vitamin D deficient pregnant women may imply the activation of the vitamin D receptor occurred as a compensatory effect and merits further investigation. Saibene et al. found that 25-hydroxy vitamin D insufficiency in total thyroidectomy patients was associated with lower serum creatinine, which indicated a possible role of creatinine in the risk of transient postoperative hypocalcemia and vitamin D metablic pathway [48].
Per the positive correlation between serum 25(OH)D concentration and thrombin time (TT) in pregnant women, our study implies that there is an association between 25(OH)D and blood coagulation. A previous study showed that treatment with vitamin D supplementation had a prothrombotic effect in patients with vitamin D insufficiency, an issue requiring further study [49].
Conclusions
This study did not show an association between maternal serum vitamin D status and GDM. There was a positive correlation between serum vitamin D and parity, serum alkaline phosphatase, pre-albumin levels, and a negative correlation between serum vitamin D and thrombin time and serum creatinine levels, which could have potential clinical significance and requires further investigation.
Limitations of this study
Since serum 25(OH)D concentrations is affected by several factors, such as seasons, geographical location, race, diet/lifestyle, medical conditions, etc., it is important to develop a more rigourous protocol when performing future vitamin D related studies. In this study, patients enrollment, diet and sun exposure, maternal nutrition supplement, etc. could be more accurately controlled. The analyzer used in 25(OH)D assay could be improved if the budget allowed, such as an LC–MS/MS spectrometer. Otherwise, more accurate methods and standardization of the assay should be performed in a future study and in clinical testing. For nstance, we would re-measure 100–150 samples based on a VDSCP assay along with standard reference materials (SRM) and applying Deming regression to standardize their values in the full sample. Socioeconomic status, lifestyle, the eating habits of pregnant woman, the monitoring and classification of gestational weight gain of the pregnancy women, and their exercise levels are factors of limitation in this study and should be considered in the future study. The study population mainly composed of Han Chinese women, which ensured data homogeneity, but it may under-represent population groups with different lifestyles and socioecomic situations, leading to biased results.
Availability of data and materials
Data is available from the corresponding author upon inquiry.
References
DeLuca HF. Overview of general physiologic features and functions of VD. Am J Clin Nutr. 2004;80(6 Suppl):1689S-S1696.
Schmid A, Walther B. Natural VD content in animal products. Adv Nutr. 2013;4(4):453–62.
Karras SN, Wagner CL, Castracane VD. Understanding VD metabolism in pregnancy: From physiology to pathophysiology and clinical outcomes. Metabolism. 2018;86:112–23.
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30 Erratum in: J Clin Endocrinol Metab. 2011;96:3908.
Bouillon R, Carmeliet G. Vitamin D insufficiency: Definition, diagnosis and management. Best Pract Res Clin Endocrinol Metab. 2018;32:669–84.
Fan H, Hui L, Yan X, et al. Serum 25 hydroxyvitamin D levels and affecting factors among preconception fertile women. BMC Womens Health. 2020;20:146.
Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74:1498–513.
Gowda U, Ruwanpathirana T, Fong DP, et al. Efficacy of high dose Vitamin D supplementation in improving serum 25(OH)D among migrant and non migrant population: a retrospective study. BMC Health Serv Res. 2016;16:579.
Colonese F, Laganà AS, Colonese E, et al. The pleiotropic effects of VD in gynaecological and obstetric diseases: an overview on a hot topic. Biomed Res Int. 2015;2015: 986281.
Wang M, Chen Z, Hu Y, et al. The effects of VD supplementation on glycemic control and maternal-neonatal outcomes in women with established gestational diabetes mellitus: A systematic review and meta-analysis. Clin Nutr. 2020;S0261–5614(20):30691–9. https://doi.org/10.1016/j.clnu.2020.12.016.
Albahlol IA, Almaeen AH, Alduraywish AA, et al. VD Status and Pregnancy Complications: Serum 1,25-di-hydroxyl-VD and its Ratio to 25-hydroxy-VD are Superior Biomarkers than 25-hydroxy-VD. Int J Med Sci. 2020;17:3039–48. https://doi.org/10.7150/ijms.47807.
Vivanti AJ, Monier I, Salakos E, et al. VD and pregnancy outcomes: Overall results of the FEPED study. J Gynecol Obstet Hum Reprod. 2020;49: 101883. https://doi.org/10.1016/j.jogoh.2020.101883.
Milajerdi A, Abbasi F, Mousavi SM, et al. Maternal vitamin D status and risk of gestational diabetes mellitus: A systematic review and meta-analysis of prospective cohort studies. Clin Nutr. 2021;40(5):2576–86. https://doi.org/10.1016/j.clnu.2021.03.037 Epub 2021 Apr 2 PMID: 33933723.
Pérez-López FR, Pasupuleti V, Mezones-Holguin E, et al. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: a systematic review and meta-analysis of randomized controlled trials. Fertil Steril. 2015;103(5):1278-88.e4. https://doi.org/10.1016/j.fertnstert.2015.02.019 Epub 2015 Mar 23 PMID: 25813278.
Bian H, Tang Y, Zhou Y, et al. Demographic variations and temporal trends in prenatal use of multiple micronutrient supplements in Beijing, 2013–2017. Public Health Nutr. 2021;24(5):826–33. https://doi.org/10.1017/S1368980020004905 Epub 2020 Dec 2 PMID: 33261684.
Li J, Gao Y, Yu T, et al. Obesity and leptin influence vitamin D metabolism and action in human marrow stromal cells. J Steroid Biochem Mol Biol. 2020;198:105564. https://doi.org/10.1016/j.jsbmb.2019.105564 Epub 2019 Dec 3 PMID: 31809868.
Tangestani H, Djafarian K, Emamat H, et al. Efficacy of vitamin D fortified foods on bone mineral density and serum bone biomarkers: A systematic review and meta-analysis of interventional studies. Crit Rev Food Sci Nutr. 2020;60:1094–103.
Parizadeh SM, Rezayi M, Jafarzadeh-Esfehani R, et al. Association of vitamin D status with liver and kidney disease: A systematic review of clinical trials, and cross-sectional and cohort studies. Int J Vitam Nutr Res. 2021;91:175–87.
Bouillon R. Vitamin D and cardiovascular disorders. Osteoporos Int. 2019;30:2167–81.
Sempos CT, Binkley N. 25-Hydroxyvitamin D assay standardisation and vitamin D guidelines paralysis. Public Health Nutr. 2020;23:1153–64.
Binkley N, Dawson-Hughes B, Durazo-Arvizu R, Thamm M, Tian L, Merkel JM, Jones JC, Carter GD, Sempos CT. Vitamin D measurement standardization: The way out of the chaos. J Steroid Biochem Mol Biol. 2017;173:117–21.
Brooks SPJ, Sempos CT. The importance of 25-hydroxyvitamin D assay standardization and the Vitamin D Standardization Program. J AOAC Int. 2017;100:1223–4.
American Diabetes Association. Standards of medical care in diabetes–2014. Diabetes Care. 2014;37(Suppl 1):S14-80.
Arnold DL, Enquobahrie DA, Qiu C, et al. Early pregnancy maternal VD concentrations and risk of gestational diabetes mellitus. Paediatr Perinat Epidemiol. 2015;29:200–10.
Schneuer FJ, Roberts CL, Guilbert C, et al. Effects of maternal serum 25-hydroxyVD concentrations in the first trimester on subsequent pregnancy outcomes in an Australian population. Am J Clin Nutr. 2014;99:287–95.
McIntyre HD, Catalano P, Zhang C, et al. Gestational diabetes mellitus. Nat Rev Dis Primers. 2019;5:47.
Damm P, Houshmand-Oeregaard A, Kelstrup L, et al. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia. 2016;59:1396–9.
Norman AW, Frankel JB, Heldt AM, et al. VD deficiency inhibits pancreatic secretion of insulin. Science. 1980;209:823–5.
Hu L, Zhang Y, Wang X, et al. Maternal VD Status and Risk of Gestational Diabetes: a Meta-Analysis. Cell Physiol Biochem. 2018;45:291–300.
Wilson RL, Leviton AJ, Leemaqz SY, et al. VD levels in an Australian and New Zealand cohort and the association with pregnancy outcome. BMC Pregnancy Childbirth. 2018;18:251.
Martínez-Domínguez SJ, Tajada M, Chedraui P, et al. Systematic review and meta-analysis of Spanish studies regarding the association between maternal 25-hydroxyVD levels and perinatal outcomes. Gynecol Endocrinol. 2018;34:987–94.
Corcoy R, Mendoza LC, Simmons D, et al. The DALI VD randomized controlled trial for gestational diabetes mellitus prevention: No major benefit shown besides VD sufficiency. Clin Nutr. 2020;39:976–84.
Yin WJ, Tao RX, Hu HL, et al. The association of vitamin D status and supplementation during pregnancy with gestational diabetes mellitus: a Chinese prospective birth cohort study. Am J Clin Nutr. 2020;111(1):122–30. https://doi.org/10.1093/ajcn/nqz260 PMID: 31625576.
Song SJ, Si S, Liu J, et al. Vitamin D status in Chinese pregnant women and their newborns in Beijing and their relationships to birth size. Public Health Nutr. 2013;16(4):687–92. https://doi.org/10.1017/S1368980012003084 Epub 2012 Jul 16 PMID: 23174124.
Mahmoud SZ, Saad AA, Mohieldein AH, et al. Serum level of 25-hydroxyVD and obesity among early pregnant women. J Obstet Gynaecol Res. 2019;45:2338–42. https://doi.org/10.1111/jog.14114.
Woon FC, Chin YS, Ismail IH, et al. Vitamin D deficiency during pregnancy and its associated factors among third trimester Malaysian pregnant women. PLoS ONE. 2019;14(6): e0216439. https://doi.org/10.1371/journal.pone.0216439.PMID:31233513;PMCID:PMC6590777.
Shen Y, Pu L, Si S, et al. Vitamin D nutrient status during pregnancy and its influencing factors. Clin Nutr. 2020;39(5):1432–9. https://doi.org/10.1016/j.clnu.2019.06.002 Epub 2019 Jun 8 PMID: 31229327.
Shaheen S, Noor SS, Barakzai Q. Serum alkaline phosphatase screening for VD deficiency states. J Coll Physicians Surg Pak. 2012;22:424–7.
Pulungan AB, Soesanti F, Tridjaja B, et al. VD insufficiency and its contributing factors in primary school-aged children in Indonesia, a sun-rich country. Ann Pediatr Endocrinol Metab. 2021. https://doi.org/10.6065/apem.2040132.066.
Fernandez-Galan E, Bedini JL, Filella X. Analytical verification and method comparison of the ADVIA centaur intact parathyroid hormone assay. Clin Biochem. 2017;50:1222–7.
Kato H, Koga M, Kobayashi H, et al. Primary bone adult T cell lymphoma with multiple skeletal lesions and debilitating painful osteolysis: a case report. Osteoporos Int. 2020. https://doi.org/10.1007/s00198-020-05720-6.
Ranasinghe RN, Biswas M, Vincent RP. Prealbumin: The clinical utility and analytical methodologies. Ann Clin Biochem. 2020 Jun 11:4563220931885. https://doi.org/10.1177/0004563220931885. Epub ahead of print. PMID: 32429677.
Sawada M, Kubota N, Sekine R, et al. Sex-related differences in the effects of nutritional status and body composition on functional disability in the elderly. PLoS ONE. 2021;16(2):e0246276. https://doi.org/10.1371/journal.pone.0246276.PMID:33529213;PMCID:PMC7853464.
Liu H, Shao-Gang M, Liang C, et al. Surrogate markers of the kidney and liver in the assessment of gestational diabetes mellitus and fetal outcome. J Clin Diagn Res. 2015;9(1):OC14-7. https://doi.org/10.7860/JCDR/2015/11585.5475 Epub 2015 Jan 1. PMID: 25738017; PMCID: PMC4347108.
Levey AS, Perrone RD, Madias NE. Serum creatinine and renal function. Annu Rev Med. 1988;39:465–90.
Verma S, Kellum JA. Defining Acute Kidney Injury. Crit Care Clin. 2021;37:251–66.
Agarwal R, Hynson JE, Hecht TJ, et al. Short-term VD receptor activation increases serum creatinine due to increased production with no effect on the glomerular filtration rate. Kidney Int. 2011;80:1073–9.
Saibene AM, Rosso C, Felisati G, et al. Can preoperative 25-hydroxyvitamin D levels predict transient hypocalcemia after total thyroidectomy? Updates Surg. 2021 Sep 26. https://doi.org/10.1007/s13304-021-01158-5. Epub ahead of print. PMID: 34564834.
Saliba W, Awad K, Ron G, et al. The Effect of VD Supplementation on Thrombin Generation Assessed by the Calibrated Automated Thrombogram. Clin Appl Thromb Hemost. 2016;22:340–5.
Acknowledgements
None.
Funding
Foshan Science and Technology Bureau Project (2018AB000251) of Guangdong, China.
Author information
Authors and Affiliations
Contributions
C.L. is the principle investigator whom is also the corresponding author responsible for project conception; Z.L. and L.J. took charge of statistical analysis; Y.L., F.W., D.S., S.L., and A.C. took charge of patients’ enrolment and clinical information collection; Z.R., took charge of data collection and integration; R.J. performed laboratory analysis and data collection; F.H. performed Bone Densitometry; H.H. wrote the manuscript; X.G. participated in project organization and conception. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethics approval was obtained by the Institutional Review Board (IRB) and Ethics Committee of Foshan Women’s and Children’s Hospital of Southern Medical University. The approvel document number is FSFY-MEC-2018–014. The file will be provided upon inquiry. All experimental protocols were approved by the IRB of the hospital. All methods were carried out in accordance with relevant guidelines and regulations. Methods and laboratory testing are routine and standard operating required for medical practice in Guangdong Province including this hospital. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, C., Li, Z., Lu, Y. et al. Association of serum vitamin D status with gestational diabetes mellitus and other laboratory parameters in early pregnant women. BMC Pregnancy Childbirth 22, 400 (2022). https://doi.org/10.1186/s12884-022-04725-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-022-04725-9