
Abstract
Objective
To investigate the potential causal link between genetic variants associated with gut microbiome and risk of intracranial aneurysm (IA) using two-sample mendelian randomization (MR).
Methods
We performed two sets of MR analyses. At first, we selected the genome-wide statistical significant(P < 5 × 10–8) single nucleotide polymorphisms (SNPs) as instrumental variables (IVs). Then, we selected the locus-wide significant (P < 1 × 10–5) SNPs as IVs for the other set of analyses to obtain more comprehensive conclusions. Gut microbiome genetic association estimates were derived from a genome-wide association study (GWAS) of 18,473 individuals. Summary-level statistics for IA were obtained from 79,429 individuals, which included 7,495 cases and 71,934 controls.
Results
On the basis of locus-wide significance level, inverse variance weighted(IVW) showed that Clostridia [(odds ratio (OR): 2.60; 95% confidence interval (CI): 1.00—6.72, P = 0.049)], Adlercreutzia (OR: 1.81; 95% CI: 1.10—2.99, P = 0.021) and Victivallis (OR: 1.38; 95% CI: 1.01—1.88, P = 0.044) were positively related with the risk of unruptured intracranial aneurysm(UIA); Weighted median results of MR showed Oscillospira (OR: 0.37; 95% CI: 0.17—0.84, P = 0.018) was negatively with the risk of UIA and Sutterella (OR: 1.84; 95% CI: 1.04—3.23, P = 0.035) was positively related with the risk of UIA; MR-Egger method analysis indicated that Paraprevotella (OR: 0.32; 95% CI: 0.13—0.80, P = 0.035) was negatively with the risk of UIA and Rhodospirillaceae (OR: 13.39; 95% CI: 1.44—124.47, P = 0.048) was positively related with the risk of UIA. The results suggest that Streptococcus (OR: 5.19; 95% CI: 1.25—21.56; P = 0.024) and Peptostreptococcaceae (OR: 4.92; 95% CI: 1.32—18.32; P = 0.018) may increase the risk of UIA according to genome-wide statistical significance thresholds.
Conclusion
This MR analysis indicates that there exists a beneficial or detrimental causal effect of gut microbiota composition on IAs.
Similar content being viewed by others

Introduction
Intracranial aneurysm (IA) is confined, pathological dilatations of the walls of intracranial arteries that are at risk of rupture. About 85% of spontaneous subarachnoid hemorrhage(SAH) is due to ruptured IA [1]. The incidence of IA was reported to be about 3.2% in a worldwide study with a mean age of 50 years [2]. Aneurysmal subarachnoid hemorrhage(aSAH) often has a poor prognosis(30% of death, 30% of independence and 30% of dependence), with patients often suffering from a disability or even death [3, 4]. Nonetheless, the etiology of IAs is as yet not completely perceived. If the causes of intracranial aneurysms could be prevented this would greatly reduce human suffering.
Recently, the relationship between IAs and gut microbiome has attracted a lot of attention. Gut flora has been found to assume a part in cardiovascular diseases such as atherosclerosis and hypertension [5, 6]. Hypertension and other related factors have long been reported to be significantly associated with intracranial aneurysms [7]. Therefore, we can speculate that intestinal dysbiosis may increase the risk of intracranial aneurysm through these high-risk factors for intracranial aneurysm. One study reported that eliminating intestinal flora with antibiotics significantly reduced the incidence of IAs in mice [8]. Another study found the abundance of certain intestinal flora was higher in patients with aSAH than in those with unruptured intracranial aneurysm(UIA) [9]. A recent study reported that after transplanting feces from UIA patients into mice, mice implanted with feces from UIA patients had a greatly increased risk of aneurysm and aneurysm rupture compared to feces from healthy humans [10]. Nevertheless, whether there exists a clear causal connection between IAs and intestinal microbiota is unclear.
Mendelian randomization (MR) is the use of genetic variation in non-experimental data to estimate the causal link between exposure and outcome, which can reduce the impact of behavioral, social, psychological, and other factors [11]. Using recently published summary data for gut microbiome and summary data for IA in genome-wide association study (GWAS), we aimed to analyze the causal connection between intestinal microbiota and IA through two-sample MR.
Material and methods
Genetic instruments and data sources
SNPs related with human gut microbiome were used in a GWAS. This GWAS included 18,340 individuals [11]. This is a large-scale multi-ethnic GWAS, mostly of European ancestry, containing 122,110 variant loci to explore the human genetic impact on gut microbiome composition.
SNPs associated with IA were extracted from a large GWAS [12]. This GWAS involved 71,934 controls and 7,495 cases. MR analysis was conducted using a summary data from this GWAS. This dataset is a GWAS of European ancestry individuals including UIA-only (n = 2,070) versus controls (n = 71,934).
To confirm the causal relationship between gut microbiome and IA risk, the best IVs were selected following the following steps. A threshold of significant association with the gut microbiome was set for the selection of SNPs as IVs as the first step. We screened for SNPs with genome-wide statistical significance (P < 5 × 10–8) as IVs. To achieve overall results, another set of locus-wide significant(P < 1 × 10–5) SNPs was used as IVs. Second, one of the principles of the MR method: There must be no linkage disequilibrium (LD) between the selected IVs, because the existence of strong LD may lead to biased results. During our MR analysis, we reduced the LD by clumping the selected SNPs (clumping distance = 10,000 kb, R2 < 0.001). Finally, during MR analysis, it is important to ensure that SNPs affect outcome and exposure with only one allele. According to this principle, SNPs of the palindrome structure will be removed.
Standard protocol approvals, registrations, and patient consents
The MR analysis used summary GWAS data publicly available from GWASs. Due to the fact that each of the original GWASs had obtained ethical approval and participant consent, they were not required.
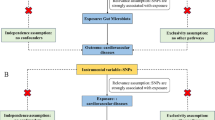
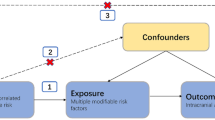
The assumptions of MR
In MR, genetic variation is viewed as an IV, and the basic conditions for genetic variation to satisfy this IV are listed: There are no confounding factors associated with gut microbiome or IA that correlate with IVs; IVs are directly associated with gut microbiome; unless exposure is associated with the IVs, the IVs do not affect the outcome [12]. It is commonly used to evaluate the strength of the correlation between exposure and IVs using the F statistic, whose formula is (R^2 (n-k-1))/(k (1-R^2)). The number of exposure samples in the GWAS study is n, the number of IVs is k, and the degree to which IVs explain exposure is R^2. It is usually considered a weak IV when the F statistic is less than 10, which may affect the results.
Statistical analysis
A causal link between IAs and intestinal microbes was investigated using the inverse variance weighted (IVW) method, MR-Egger, weighted median, and weighted mode. In the IVW method, the intercept term is not considered. In this method, weights are based on the inverse of variance (quadratic of standard error). A comprehensive estimate of the impact of gut microbiota on IA incidence was obtained using this method. IVW results would be highly biased if these SNPs were pleiotropic, and this must be ensured. With MR-Egger, causal estimates are unaffected by breaches of the standard IV assumptions and violations of the standard IV assumptions can be detected [13]. Weighted medians combine information from different hereditary variations into one causal gauge, which is predictably accurate even with half of the null IVs [14].
An MR-Egger regression was conducted to determine whether the SNPs included had horizontal pleiotropy. In order to monitor the presence of IVs with horizontal polymorphisms, mendelian randomized pleiotropy residuals and outliers (MR-PRESSO) was used because it had better statistical power and accuracy than MR-Egger regression. MR-PRESSO was also used to correct horizontal polymorphisms. We performed leave-one-out analysis in order to determine if causal effect estimates were reliable in the presence of potentially strong impact SNPs. We performed a leave-one-out analysis to determine if there are potentially strong impact SNPs. Thus, we are able to test whether the causal effect estimates are reliable. A further examination of the heterogeneity among selected SNPs was conducted with Cochran's Q statistics. We used the R (version 4.1.2) packages MRPRESSO and TwoSampleMR to perform MR analyses.
Results
Instrumental variables selection
Firstly, we screened 461 (genome-wide statistical significance threshold, P < 5 × 10–8) and 10,417 (locus-wide significance level, P < 1 × 10–5) SNPs as IVs from a massive gut microbiome GWAS containing 211 taxa which consist of five biotypes of the genus, family, order, phylum, and class. After the removal of SNPs with LD and independent of IA, 12 (P < 5 × 10–8) and 1,291 (P < 1 × 10–5) SNPs remained as IVs. We collected important information of SNPs including beta, SE, P-value, effect allele, and other allele for further study.
Locus-wide significance level with UIA
Weighted median results of MR showed Oscillospira [(odds ratio (OR): 0.37; 95% confidence interval (CI): 0.17—0.84, P = 0.018)] was negative with the occurrence of UIA and Sutterella (OR: 1.84; 95% CI: 1.04—3.23, P = 0.035) was positively related with the occurrence of UIA (Supplementary Table 1). The results of the MR-Egger method analysis indicated that Paraprevotella (OR: 0.32; 95% CI: 0.13—0.80, P = 0.035) was negative with the occurrence of UIA and Rhodospirillaceae (OR: 13.39; 95% CI: 1.44—124.47, P = 0.048) was positively related with the occurrence of UIA (Supplementary Table 1). The results of the IVW method analysis indicated that Clostridia (OR: 2.60; 95% CI: 1.00—6.72, P = 0.049), Adlercreutzia (OR: 1.81; 95% CI: 1.10—2.99, P = 0.021) and Victivallis (OR: 1.38; 95% CI: 1.01—1.88, P = 0.044) were positively related with the occurrence of UIA (Supplementary Table 1).
We used MR-Egger regression to evaluate the horizontal pleiotropy between IVs and outcomes, which indicated there existed horizontal pleiotropy between the instrument variables of Paraprevotella and outcomes (P = 0.029), and there was no evidence of horizontal pleiotropy between other IVs and outcomes (Supplementary Table 1). However, when further analyzed by MR-PRESSO, none of them were found to be horizontally pleiotropic. There existed no outliers in the MR-PRESSO analysis of Clostridia (P = 0.359), Rhodospirillaceae (P = 0.372), Adlercreutzia (P = 0.474), Oscillospira (P = 0.137), Paraprevotella (P = 0.172), Sutterella (P = 0.201), and Victivallis (P = 0.448). Details of the instrument variables are shown in Supplementary Table 2. All F-statistic values are greater than 10, which indicates the absence of weak IVs (Supplementary Table 1). Therefore, this study found that Clostridia (Fig. 1), Rhodospirillaceae (Supplementary Fig. 1), Adlercreutzia (Supplementary Fig. 2), Sutterella (Supplementary Fig. 3), and Victivallis (Supplementary Fig. 4) were occurrence factors for UIA and that Oscillospira (Supplementary Fig. 5) and Paraprevotella (Supplementary Fig. 6) played protective roles in the development of UIA.

Forest plot (A), sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causal effect of Clostridia on IA risk
Genome-wide statistical significance threshold
When analyzing the association of intestinal microbiota overall with UIA, the results of MR Egger (OR: 0.92; 95% CI: 0.43—1.96, P = 0.837), weighted mode (OR: 1.13; 95% CI: 0.83—1.55; P = 0.458), weighted median (OR: 1.12; 95% CI: 0.83—1.52; P = 0.447) and IVW (OR: 1.19; 95% CI: 0.92—1.54; P = 0.187) showed that there exists no association between intestinal microbiota and UIA (Table 1 and Supplementary Fig. 7).
Specific information on IVs is provided in Table 2. MR-Egger regression indicated no horizontal pleiotropy in the analysis of the relationship between total gut microbiome and aneurysms (P = 0.495 for UIA). Besides, F statistics were more than 10, and Cochrane Q statistics showed no significant heterogeneity (P = 0.156 for UIA). The results of the intestinal microbiota classification suggested that Streptococcus (OR: 5.19; 95% CI: 1.25—21.56; P = 0.024) and Peptostreptococcaceae (OR: 4.92; 95% CI: 1.32—18.32; P = 0.018) may increase the occurrence of UIA (Table 1). The limited number of SNPs included prevented examination of horizontal pleiotropy and heterogeneity.
Discussion
Our MR analysis gives proof to prove that Streptococcus, Adlercreutzia, Clostridia, Rhodospirillaceae, Sutterella, Victivallis and Peptostreptococcaceae increase the occurrence of IA, Oscillospira and Paraprevotella are protective factors for IA. However, only a few IVs reached genome-wide statistically significant levels, making the accuracy of the results of Streptococcus and Peptostreptococcaceae potentially subject to some bias.
It has been realized by more and more neurosurgeons that environmental factors act a more significant role than inherited factors in the pathophysiology of IAs [15, 16]. Pyysalo et al. have reported the association of IAs with oral bacteria, suggesting a link between aneurysms and bacteria [17]. The gut microbiota may influence IA formation and rupture by modulating local inflammation and affecting blood pressure [18]. Streptococcus may increase the release of inflammatory factors such as IL-1β, IFN-γ, and IL-6 [19]. One study reported that Streptococcus is usually in higher abundance in hypertensive patients [20]. Peptostreptococcaceae promote the progression of atherosclerosis, which may promote aneurysm formation [21]. Prevotella was found in high levels in patients with rheumatoid arthritis and has been found to be associated with chronic inflammation [22, 23]. These reports are consistent with our findings. Nevertheless, specific ways of the effects of these intestinal florae on inflammation and aneurysms remain to be further investigated.
Although some studies have shown the presence of intestinal flora disorders in patients with IAs, this may only be a clinical symptom of IAs and there appears to be no causal association between IAs and intestinal flora disorders. On the one hand, the components of the intestinal microbiota might differ due to inconsistent sex ratios and ethnicity across studies. On the other hand, although IA patients were found to have dysbiosis of the intestinal microbiota, there is no agreement as to which strains play a key role. These unresolved issues have prevented inferring a causal association between the intestinal microbiota and the occurrence and rupture of IAs. In the treatment of intracranial aneurysms, it may be possible in the future to reduce the risk of occurrence and rupture of intracranial aneurysms by targeting certain bacteria for eradication.
To our knowledge, the present study is the first MR analysis of the relationship between IAs and intestinal microflora. The fundamental benefit of this MR analysis is that estimates of the causal effect of MR are not distorted by confounding factors and reverse causal associations found in traditional epidemiological studies. Therefore, compared to observational studies, it may be more persuasive. Yet, several limitations remain. First, in the two-sample MR analysis, we could not confirm whether overlapping participants participated in the exposures and outcomes GWAS. We use F statistics to minimize the bias of overlapping participants. Second, due to its biological plausibility and multistage statistical process, it may be too conservative and may omit potential strains that are causally associated with IA when applying rigorous multiple test correction. Therefore, we did not consider multiple tests. Third, due to most participants in GWAS being of European origin, it may be not applicable to other groups of people. Fourth, the original study lacked detailed demographic information, and further subgroup analysis was not possible. Finally, some studies have reported a progressive increase in the age of onset of subarachnoid hemorrhage [24]. Although it is true that studies have shown that the structure and species of the gut microbiota change with age, there may be some bias due to the absence of a specific age classification for the exposure factors selected for our study [25].
In summary, this MR research identified a causal impact of intestinal flora on IAs. Several intestinal microbiomes identified in this study that are associated with the occurrence and rupture of IAs may have the prospect of preventing IAs.
Availability of data and materials
The data used in the article is presented in the article/supplementary material. Please contact the corresponding author for further information.
References
Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389:655–66. https://doi.org/10.1016/S0140-6736(16)30668-7.
Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10:626–36. https://doi.org/10.1016/S1474-4422(11)70109-0.
Chen Y, Wright N, Guo Y, Turnbull I, Kartsonaki C, Yang L, et al. Mortality and recurrent vascular events after first incident stroke: a 9-year community-based study of 0·5 million Chinese adults. Lancet Glob Health. 2020;8:e580–90. https://doi.org/10.1016/S2214-109X(20)30069-3.
Nieuwkamp DJ, Setz LE, Algra A, Linn FHH, de Rooij NK, Rinkel GJE. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 2009;8:635–42. https://doi.org/10.1016/S1474-4422(09)70126-7.
Tang WHW, Li DY, Hazen SL. Dietary metabolism, the gut microbiome, and heart failure. Nat Rev Cardiol. 2019;16:137–54. https://doi.org/10.1038/s41569-018-0108-7.
Jie Z, Xia H, Zhong S-L, Feng Q, Li S, Liang S, et al. The gut microbiome in atherosclerotic cardiovascular disease. Nat Commun. 2017;8:845. https://doi.org/10.1038/s41467-017-00900-1.
Ćmiel-Smorzyk K, Ładziński P, Kaspera W. Biology, physics and genetics of intracranial aneurysm formation: a review. J Neurol Surg A Cent Eur Neurosurg. 2022. https://doi.org/10.1055/a-1994-8560.
Shikata F, Shimada K, Sato H, Ikedo T, Kuwabara A, Furukawa H, et al. Potential Influences of Gut Microbiota on the Formation of Intracranial Aneurysm. Hypertension. 2019;73:491–6. https://doi.org/10.1161/HYPERTENSIONAHA.118.11804.
Kawabata S, Takagaki M, Nakamura H, Oki H, Motooka D, Nakamura S, et al. Dysbiosis of Gut Microbiome Is Associated With Rupture of Cerebral Aneurysms. Stroke 2021:STROKEAHA121034792. https://doi.org/10.1161/STROKEAHA.121.034792.
Li H, Xu H, Li Y, Jiang Y, Hu Y, Liu T, et al. Alterations of gut microbiota contribute to the progression of unruptured intracranial aneurysms. Nat Commun. 2020;11:3218. https://doi.org/10.1038/s41467-020-16990-3.
Davey Smith G, Hemani G. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Hum Mol Genet. 2014;23:R89–98. https://doi.org/10.1093/hmg/ddu328.
Didelez V, Sheehan N. Mendelian randomization as an instrumental variable approach to causal inference. Stat Methods Med Res. 2007;16:309–30. https://doi.org/10.1177/0962280206077743.
Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44:512–25. https://doi.org/10.1093/ije/dyv080.
Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet Epidemiol. 2016;40:304–14. https://doi.org/10.1002/gepi.21965.
Karhunen V, Bakker MK, Ruigrok YM, Gill D, Larsson SC. Modifiable Risk Factors for Intracranial Aneurysm and Aneurysmal Subarachnoid Hemorrhage: A Mendelian Randomization Study. J Am Heart Assoc. 2021;10:e022277. https://doi.org/10.1161/JAHA.121.022277.
Acosta JN, Szejko N, Both CP, Vanent K, Noche RB, Gill TM, et al. Genetically Determined Smoking Behavior and Risk of Nontraumatic Subarachnoid Hemorrhage. Stroke. 2021;52:582–7. https://doi.org/10.1161/STROKEAHA.120.031622.
Pyysalo MJ, Pyysalo LM, Pessi T, Karhunen PJ, Lehtimäki T, Oksala N, et al. Bacterial DNA findings in ruptured and unruptured intracranial aneurysms. Acta Odontol Scand. 2016;74:315–20. https://doi.org/10.3109/00016357.2015.1130854.
Chalouhi N, Hoh BL, Hasan D. Review of cerebral aneurysm formation, growth, and rupture. Stroke. 2013;44:3613–22. https://doi.org/10.1161/STROKEAHA.113.002390.
Park HJ, Kim SA, Kang WS, Kim JW. Early-Life Stress Modulates Gut Microbiota and Peripheral and Central Inflammation in a Sex-Dependent Manner. Int J Mol Sci. 2021;22:1899. https://doi.org/10.3390/ijms22041899.
Yan Q, Gu Y, Li X, Yang W, Jia L, Chen C, et al. Alterations of the Gut Microbiome in Hypertension. Front Cell Infect Microbiol. 2017;7:381. https://doi.org/10.3389/fcimb.2017.00381.
Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19:576–85. https://doi.org/10.1038/nm.3145.
Kishikawa T, Maeda Y, Nii T, Motooka D, Matsumoto Y, Matsushita M, et al. Metagenome-wide association study of gut microbiome revealed novel aetiology of rheumatoid arthritis in the Japanese population. Ann Rheum Dis. 2020;79:103–11. https://doi.org/10.1136/annrheumdis-2019-215743.
Ley RE. Gut microbiota in 2015: Prevotella in the gut: choose carefully. Nat Rev Gastroenterol Hepatol. 2016;13:69–70. https://doi.org/10.1038/nrgastro.2016.4.
Katsuki M, Yamamoto Y, Uchiyama T, Wada N, Kakizawa Y. Clinical characteristics of aneurysmal subarachnoid hemorrhage in the elderly over 75; would temporal muscle be a potential prognostic factor as an indicator of sarcopenia? Clin Neurol Neurosurg. 2019;186:105535. https://doi.org/10.1016/j.clineuro.2019.105535.
Badal VD, Vaccariello ED, Murray ER, Yu KE, Knight R, Jeste DV, et al. The Gut Microbiome, Aging, and Longevity: A Systematic Review. Nutrients. 2020;12:3759. https://doi.org/10.3390/nu12123759.
Acknowledgements
The authors thank Dr. Lu Hua for his excellent suggestions on the revision of this paper.
Funding
This work was supported by a grant from the National Natural Science Foundation of China (No. 81901258) and Natural Science Foundation of Jiangsu Province (No. H2017022).
Author information
Authors and Affiliations
Contributions
Data curation, Yuqi Shen; Formal analysis, Hanxiao Chang; Investigation, Lei Mao and Xiupeng Xu; Methodology, Chencheng Ma; Software, Weiwei Zhang; Supervision, Zheng Li; Validation, Huiru Jin; Writing – original draft, Guangjian Zhang; Writing – review & editing, Hua Lu.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable. The MR analysis used summary GWAS data publicly available from GWASs. Due to the fact that each of the original GWASs had obtained ethical approval and participant consent, they were not required.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
SupplementaryFigure 1. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of Rhodospirillaceae on UIA risk.
Additional file 2:
SupplementaryFigure 2. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of Adlercreutzia on UIA risk.
Additional file 3:
SupplementaryFigure 3. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of Sutterella on UIA risk.
Additional file 4:
SupplementaryFigure 4. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of Victivallis on UIA risk.
Additional file 5:
SupplementaryFigure 5. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of Oscillospira on UIA risk.
Additional file 6:
SupplementaryFigure 6. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of Paraprevotella on UIA risk.
Additional file 7:
SupplementaryFigure 7. Forest plot (A),sensitivity analysis (B), scatter plot (C), and funnel plot (D) of the causaleffect of the whole gut microbiome on UIA risk.
Additional file 8:
Supplementary Table 1. MR results of causallinks between gut microbiome and UIA risk (P < 1 × 10-5). Supplementary Table 2. SNPs used asinstrumental variables from gut microbiome and UIA GWASs (P < 1 × 10-5).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ma, C., Zhang, W., Mao, L. et al. Association of gut microbiome with risk of intracranial aneurysm: a mendelian randomization study. BMC Neurol 23, 269 (2023). https://doi.org/10.1186/s12883-023-03288-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03288-2