
Abstract
Background
The Low Physical Activity Questionnaire (LoPAQ) was specifically developed to measure the low activity level observed in extremely inactive hemodialysis (HD) patients. This study aims to evaluate reliability and validity of Persian version of the LoPAQ.
Methods
This study was a cross sectional study, conducted in three HD centers in Iran. The LoPAQ was translated into Persian. After cultural adaptions, it was filled out by 120 HD patiens. Convergent validity, was evaluated by calculating the correlations among the Persian version of the LoPAQ and Persian version of the Community Healthy Adults Model Program for Seniors (CHAMPS) questionnaire, physical function scale of the SF-36 and physical function (Short Physical Performance Battery (SPPB) test) using Spearman’s correlation coefficients. The test-retest reliability was analyzed using the intraclass correlation coefficient (ICC).
Results
In total, 109 patients completed all of the questionnaires, took part in physical performance tests and had valid data. Their mean age was 64 ± 11 years, with a dialysis history of 31 ± 10 months. For total calories, there was a strong correlation between the Persian version of the LoPAQ and CHAMPS-measured physical activity (rho = 0.85, p < 0.001). In addition, the higher physical activity level reported by Persian version of the LoPAQ was also correlated with better self-reported physical function (rho = 0.7, p < 0.001) and better physical performance (rho = 0.67, p < 0.001). The ICC ranged from 0.65 to 0.78, indicating strong reliability.
Conclusion
The assessment of the validity and reliability of the Persian version of the questionnaire confirmed its suitability for evaluating the level of physical activity.
Trial registration
ClinicalTrials.gov Identifier: NCT05930964, Registered on 05/07/2023. Registered trial name: Validity and Reliability of Persian Version of Low Physical Activity Questionnaire (LoPAQ).
Similar content being viewed by others


Background
End-stage kidney disease patients, especially those undergoing hemodialysis (HD) and peritoneal dialysis, experience a high rate of dysfunction, complications, reduced quality of life, hospitalization, and mortality [1, 2]. The etiological factors of these consequences have a wide range, the most important of which are: cardiovascular disorders (CVD), muscle atrophy and malnutrition. All these factors start or intensify with a sedentary lifestyle [1].
Prospective studies on dialysis patients have shown that reducing the daily activity level increases the risk of death in these patients by 60% [3, 4]. Based on this, proper physical activity helps prevent muscle loss, control associated diseases, improve quality of life and reduce mortality in hemodialysis patients [5, 6]. Guidelines for improving the quality of outcomes in dialysis patients state that increased physical activity and regular exercise should be considered as a cornerstone of treatment approaches for patients undergoing dialysis, especially when the goal is to control risk factors of CVD [7, 8].
Due to its importance, a reliable and feasible method for measurement is needed [9, 10]. There are countless tools for quantifying physical activity. Among other considerations, the choice of tool depends on the activity level of the studied population and the results of interest [11]. A group of tools measures the level of physical activity objectively using a pedometer. This measurement method faces many problems, one of them is the lack of appropriate instructions for the number of measurement days [12,13,14] and the low adherence of patients to this method [15]. In addition, most of the studies that use objective measurement mainly include western countries with medium to high income [12, 14, 16]. Due to the increasing prevalence of kidney disease, especially in East Asian countries and the Middle East, it is necessary to use tools to measure physical activity that are easily available [16]. In addition, a tool such as a pedometer cannot provide us with information about the type and intensity of the activity performed [11].
A number of different physical activity questionnaires have been used to evaluate patients undergoing hemodialysis treatment. It should be noted that this group is very inactive. However, previous studies have relied on questionnaires that were not specifically designed for this population [17, 18]. Many of these tools, focus on moderate-to-vigorous activities [12, 19,20,21], as these levels have been most associated with health benefits in healthy populations. As a result of focusing on higher intensity activity, this instrument may not accurately represent physical activity or changes in activity levels among highly inactive groups. Because it covers a wider range of activities than most questionnaires and does not evaluate the activity at the lower end of the spectrum [11]. Previous studies have shown that physical activity, even at low levels, is related to the survival of dialysis patients [3, 22]. However, although scores on common physical activity questionnaires categorize participants according to their general activity level, they do not specify the amount or intensity of physical activity performed and therefore do not correspond well to measures that can be used by clinicians and scores may not be sensitive to change with intervention [11]. There are increasing observations that, especially among sedentary populations, time spent sitting may have adverse effects on outcomes independent of activity participation [23,24,25,26].
To address these limitations, the “Low Physical Activity Questionnaire (LoPAQ)” was designed by Jansen et al. [11], which emphasizes very low levels of physical activity, especially walking (representing low-level physical activity), determines the amount of calorie consumption for all leisure time activities and takes sitting time as one of the negative evaluation criteria. These characteristics make this questionnaire suitable for hemodialysis patients according to the physical activity characteristics of hemodialysis patients mentioned above. In addition, this questionnaire enables researchers to estimate whether a hemodialysis patient has reached the activity level recommended in the dialysis patient guidelines on a relatively accurate scale. In addition, the English version of this questionnaire has good validity and has a high correlation with one of the most widely used questionnaires for evaluating physical activity in dialysis patients, Minnesota Leisure Time Activity Questionnaire, and various physical performance indicators [11]. Currently, the LoPAQ in hemodialysis patients is only available in English and Chinese and Japanese [11, 27, 28]. The purpose of this study is to translate and adapt it to Persian language and determine its reliability and validity in hemodialysis patients.
Method
Trial design & participants
This study was a cross-sectional study conducted to translate, culturally adapt and evaluate the validity and reliability of the Persian (Farsi) version of the LoPAQ in dialysis patients.
Patients undergoing hemodialysis treatment were recruited from three hemodialysis unit in Iran from May 2023 to June 2023.
The inclusion criteria were as follows: (1) age ≥ 18 years; (2) on hemodialysis for ≥ 3 months; (3) able to walk without assistance (walking device such as cane or walker allowed); and (4) ability to provide informed consent and complete the questionnaires. The exclusion criteria were as follows: (1) diagnosis of mental or cognitive disorders; (2) unstable conditions; and (3) hospitalization in the previous 3 months.
Trial procedures
After providing written informed consent, eligible patients received a demographic questionnaire. Data were collected on demographic characteristics (age, sex, and time on hemodialysis), primary cause of kidney failure, and comorbidities (atherosclerotic heart disease, congestive heart failure, cerebrovascular accident/transient ischemic attack, peripheral vascular disease, dysrhythmia, and other cardiac diseases, chronic obstructive pulmonary disease, gastrointestinal bleeding, liver disease, cancer, and diabetes). Comorbidities were quantified using Charlson comorbidity index (CCI) established for dialysis patients, which included the underlying cause of kidney failure, as well as 11 comorbidities [29].
Participants were interviewed during dialysis (in a midweek session) to complete the questionnaires. Physical performance was measured on the same day before the dialysis session. After two weeks, the participants were interviewed to complete the Persian version of the LoPAQ again to evaluate test-retest reliability.
Low physical activity questionnaire (LoPAQ)
The Low Physical Activity Questionnaire (LoPAQ) was initially developed by Johansen et al. [11] to evaluate physical activities at a low level for patients with HD. The questionnaire consists of 11 items that assess various parameters of physical activity within the past 7 days as follows:
Walking activities
Participants report the frequency and duration of walking for neighborhood strolls, transportation, fitness, or pleasure, as well as instances of no walking.
Light activities
Inquiries about engagement in light activities that increase heart rate slightly, such as gardening, bowling, or light housework, with details on frequency and duration.
Moderate activities
Questions on participation in moderate activities that cause a noticeable increase in heart rate and limit the ability to sing, including aerobics or moderate housework.
Vigorous activities
Assessment of involvement in vigorous activities that significantly raise heart rate and breathing, such as running or playing basketball.
Muscle strengthening exercises
Determination of whether participants performed exercises specifically for muscle strengthening.
Flexibility exercises
Evaluation of participation in stretching or flexibility exercises.
Sedentary behavior
Measurement of time spent in sedentary activities like sitting, watching television, or using a computer.
Napping habits
Inquiry about daytime napping habits, including frequency and duration.
Sleep duration
Reporting of average nightly sleep duration over the past week. Work-Related Questions regarding the physical nature of participants’ work, if applicable, including walking and physical exertion like lifting.
Each item is designed to capture both the intensity and frequency of the activities, providing a comprehensive picture of the patient’s physical activity level. The questionnaire also calculates the kilocalories expended during light, moderate, vigorous, and total physical activities. The scoring system allows for categorization into different levels of physical activity, which can be crucial for managing hemodialysis treatment.
The validity of the English version of the LoPAQ was established by its substantial correlations with the Minnesota Leisure Time Activity Questionnaire (rho = 0.62, p < 0.001), the Physical Function score of the 36-item Short Form Health Survey (SF-36; rho = 0.64, p < 0.001), and physical performance indexes [11].
Translation and cultural adaption of the Persian version of the LoPAQ
Once we received permission from the original authors for the linguistic adjustments and validation, the Persian version of the LoPAQ was culturally and linguistically adapted. Following the existing guidelines on translation and matching [30, 31] and World Health Organization recommendations [32], two native Persian translators independently translated the questionnaire from English to Persian, with an emphasis on preserving the content instead of conducting a literal translation. One translator was an exercise physiologist who was aware of the study’s purpose and translation, while the other was an official translator who had no knowledge of the study’s purpose. After the translators completed their work, the two versions were compared, and any contradictions or differences were reviewed by the two translators to produce a single translation of the questionnaire. In the next step, two native Persian-speaking translators who had lived in English-speaking countries for an extended period of time translated the Persian translation into English without knowing the study’s purpose. Next, an expert committee composed of various members, including an epidemiologist, two nephrologists, a general practitioner, two sports medicine specialists, and two academic translators, reviewed and discussed the differences between the English translations and the main questionnaire to verify both the linguistic and conceptual alignment of the LoPAQ.
Measurements
To measure current physical activity behaviors in dialysis patients, we utilized the Community Healthy Adults Model Program for Seniors (CHAMPS) questionnaire. The CHAMPS questionnaire contains 41 questions, each split into two parts, which evaluate the frequency and duration of various physical and non-physical leisure time activities, ranging from light to intense. Each question inquires whether an individual has engaged in a certain activity over the past four weeks, specifically during an average week. If the participant has taken part in the activity during a typical week, they are then asked to specify the frequency and duration for that week. The activities described span from light activities, like casual walking and water exercises, to moderate ones such as cycling or general conditioning to vigorous ones, like jogging or fast-paced swimming [33].
CHAMPS was chosen due to its previous use in similar populations [34,35,36] and its ability to measure various activities beyond just exercises. The measure provides two scores, including the frequency of activity per week and the estimated caloric expenditure per week. Each activity listed in the questionnaire was assigned a metabolic equivalent of task (MET) value based on the values reported by Ainsworth and colleagues [37], which is a physiological measure expressing the energy cost of physical activities. By multiplying the estimated duration of each activity by the MET value and summing these across all relevant activities, the duration and intensity of total physical activity reported were estimated.
Self-reported physical function was evaluated by administering the Physical Function (PF) scale of the SF-36 [38], which comprises 10 activities that participants are asked to perform and score from 0 to 100. Higher scores indicate better physical function.
Physical performance was assessed using the Short Physical Performance Battery (SPPB) [39] and its individual components, which comprise gait speed, a timed sit-to-stand test, and balance tests. Performance tests were performed immediately before a midweek dialysis session. Gait speed was measured twice over a 15-foot course, and the fastest time was recorded. Patients were timed while performing five consecutive sit-to-stand movements from a standard chair as quickly as possible without the support of their arms. Additionally, patients were timed while standing with their feet side by side, in a semi-tandem position, and in a tandem position for up to 10 s each. A total SPPB score was computed based on the results of the performance tests, with each component scored from 0 (unable to perform) to 4 (best performance), resulting in a total score ranging from 0 to 12 [39].
Sample size
In data analysis and validity review, the ratio of sample size to the number of items should be at least five to one, and it is better to consider ten to one [40]. This questionnaire has 11 items and considering possible drop-outs 120 participants were required.
Statistical analysis
Descriptive statistics, including mean, standard deviation (SD), and percentage, were used to present the demographic information. The normality of each variable was assessed by determining the levels of skewness and kurtosis [41]. The content validity of the questionnaire was measured using the content validity index (CVI). A CVI higher than 0.78 is generally considered to indicate good content validity [42].
To assess convergent validity, correlations among the Persian version of LoPAQ and Persian version of the CHAMPS questionnaire, PF scale of the SF-36 and SPPB test were examined using Spearman’s correlation coefficients. A correlation of above 0.40 was considered acceptable [43].
Bland-Altman analyses were used to determine the level of agreement for total energy expenditure per week, derived from the Persian version of LoPAQ and CHAMPS. The test-retest reliability was determined by calculating the intraclass correlation coefficient (ICC, two-way mixed analysis of variance). An ICC > 0.75 represents excellent test-retest reliability, 0.60–0.74 represents good reliability, 0.40–0.59 represents fair reliability, and < 0.4 indicates poor reliability [44]. The LoPAQ has questions, where ask about participation in exercises, and questions ask about participation in regular activities. These two types of questions cover different topics and are inconsistent in essence. Additionally, the first type of questions has three parts asking about different exercise intensities, including strenuous, moderate, and mild exercise, which are also inconsistent intrinsically. Therefore, the authors did not measure Cronbach’s alpha for the whole questionnaire. All statistical tests were two-tailed, and p < 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS software 25.
Results
Overall, 151 patients were assessed for eligibility, of whom 120 were consented and recruited for validity test. Among them, 109 patients who completed all of the questionnaires, took part in physical performance tests and had valid data, were included in the data analysis. 85 participants completed Persian version of the LoPAQ for test-retest reliability.
Baseline characteristics
Characteristics of the patients are displayed in Table 1. This table also includes the total energy expenditure reported on the LoPAQ and CHAMPS questionnaire, as well as sitting time and physical function of participants.
Validity estimate
For content validity, the expert panel made some changes to the original English version of the LoPAQ. They commented that the use of “golfing”, “bowling” and “boating (motor)” as examples of “light activity” was not appropriate for Persian HD patients, as they do not typically engage in those exercises. Therefore, these examples were replaced with “watering the plants” and “walking downstairs.” In the subscale of “moderate activity,” “swimming (the side stroke or breast stroke)” were replaced by “Tai-Chi”. Additionally, “softball” and “downhill skiing” were deleted. In the subscale of “vigorous activity,” “playing soccer” and “cross-country skiing” were removed and replaced with “carrying heavy loads” as per the expert panel’s suggestions. These changes were made to ensure that the Persian version of the LoPAQ was culturally appropriate for Persian HD patients.
The CVI was used to measure the content validity of the Persian version of the LoPAQ, and the expert panel’s modifications improved the CVI score to 0.86, indicating good content validity.
Convergent validity
Based on the Spearman coefficient analysis, the study found strong correlation between the Persian version of the LoPAQ and CHAMPS-measured physical activity for total calories (rho = 0.85, p < 0.001). The total physical activity level reported by Persian version of the LoPAQ was also correlated with self-reported physical function (rho = 0.7, p < 0.0.5) and better physical performance (rho = 0.67, p < 0.05). Additionally, there was a negative correlation between LoPAQ-measured sedentary time and each component of SPPB and self-reported function (Table 2). These findings indicate that the Persian version of the LoPAQ has good criterion validity as it correlates well with the other physical activity level measurements.
Bland-Altman analysis
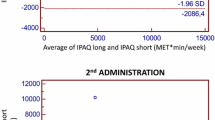
The Bland-Altman plot was used to assess the agreement between the Persian version of the LoPAQ and CHAMPS measurements (Fig. 1). The results showed a mean difference of 44.4 kcal of energy expenditure per week between the two methods. The limits of agreement for total calories between the Persian version of the LoPAQ and CHAMPS had narrow ranges, from − 191.7 to 102.9, with 4 outliers (3.7%). These findings suggest that there is consistency between Persian version of the LoPAQ and CHAMPS measurements.

The Blant-Altman plot for total energy expenditure using the LoPAQ and CHAMPS questionnaire
Reliability
The mean total energy expenditure of the Persian version of the LoPAQ was 780.5 ± 292 at the first test and 850 ± 310.5 kcal/week at retest.
As stated in the given text, due to the inconsistencies between questions of the LoPAQ, the authors did not measure Cronbach’s alpha for the whole questionnaire. Instead, they reported the intra-class correlation coefficient (ICC) for each question to assess the test-retest reliability of the questionnaire. This approach is appropriate when the questionnaire has multiple subscales or when the questions are not highly correlated with each other, as in the case of the LoPAQ. The ICC assesses the consistency of responses across time for each individual question, rather than measuring the internal consistency of the whole questionnaire. The ICCs ranged from 0.65 to 0.78 for the subscale scores, indicating good to excellent test-retest reliability. The detailed results are shown in Table 3.
Discussion
The physical activity level of patients undergoing HD treatment is low and significantly lower than the same inactive control groups [14, 45]. Research has shown that the level of physical activity of HD patients gradually decreases by approximately 4.5% per month during the entire period of the disease [20]. In addition, Li et al. [21] found that the activities related to the work done at home constitute the largest part of the energy consumption of hemodialysis patients, which means that the types of activities of hemodialysis patients are usually limited to the lower category [12]. Inactivity sets off a vicious cycle in which energy imbalances can increase comorbidities such as hypertension, diabetes, coronary artery disease, depressive disorders, hospitalization rates, and disability. Each of these conditions aggravates the decrease in the quality of life and increases the mortality of patients [15, 14].
Despite numerous studies casing the positive impacts of physical activity on health, there is a notable lack of well-defined, evidence-based exercise programs for patients with chronic kidney disease [46]. For a better understanding of the benefits of physical activity in these patient groups, it’s crucial to have valid methods to assess their physical activity levels. Such measurement tools can potentially encourage these patients to be more active and enhance their physical activity levels [47]. Recall questionnaires are the most frequently used measure for assessing physical activity because of their simplicity, cost-effectiveness, and ease of administration compared to more objective measures [48, 49]. A newly valid assessment tool, LoPAQ has been designed to capture the low activity level among typically sedentary HD patients [11], which includes a 1-week assessment period.
The aim of this study was to develop the Persian version of LoPAQ and to determine its validity and reliability for measuring low levels of physical activity compared with CHAMPS questionnaire and other tools.
It’s important to bear it in mind that Farsi is the primary language spoken across Iran, and it is taught in schools from the early grades, making the questionnaire easy-to-understand for all Iranian citizens. Accordingly, the findings from this questionnaire could be considered applicable throughout various regions of Iran [50]. To ensure that the translated version of the document was consistent with the original, the focused was put on four key areas of equivalence: semantic, idiomatic, experiential, and conceptual [51]. The translation and cultural adaptation process was thoroughly based upon the four-stage framework suggested by Herdman et al. [52].
The main findings indicated that the total energy expenditure reported by the Persian version of LoPAQ also correlated well with the kilocalories obtained from the CHAMPS questionnaire.
Theses finding is in line with the results presented by the initial study for characterization of the LoPAQ, which also used a subjective tool for criterion validity [11].
Furthermore, energy expenditure from the LoPAQ was associated with patients’ self-reported physical functioning and with several tests of physical performance. Sedentary behavior was associated with worse self-reported function and worse performance on the SPPB.
These results were consistence with previous studies with similar comparisons [11, 28], indicating the generalizability of our findings.
The Persian version of the LoPAQ has shown exceptional test-retest reliability, outperforming its Chinese counterpart across all subscales [27]. This discrepancy may be attributed to cultural differences in daily activities and walking behaviors, which are inherently influenced by the distinct social norms and environmental contexts of each region. The original and Japanese versions have not reported on test-retest reliability [11, 28], highlighting a potential area for further research. Additionally, the timing of the studies could contribute to the variability in results; the present study was conducted in Spring, whereas the Chinese study was carried out in Winter. Seasonal weather conditions, including snow, rain, and wind, can introduce significant variability in walking behavior over a two-week period. Therefore, the reliability of the Chinese version of the LoPAQ may have been affected not only by true variability in walking activities but also by potential measurement errors over time.
Despite the LoPAQ demonstrating comparable performance to other validated physical activity questionnaires, it presents certain advantages. Primarily, the LoPAQ places emphasis on walking, making it more responsive to changes in routine physical activity, especially when implementing interventions to promote walking. Additionally, it is tailored to capture activities that are typically part of dialysis patients’ lifestyles and includes the assessment of sedentary behaviors. Lastly, the LoPAQ offers the benefit of brevity compared to widely used questionnaires such as CHAMPS, requiring only 10 min for administration, including instructions provided to participant.
The development of the Persian version of the LoPAQ represents a significant step forward in the assessment of physical activity among HD patients. Its design to capture low levels of activity, which is typical of this patient group, makes it a potentially powerful tool in clinical practice. By integrating the LoPAQ into routine assessments, clinicians can monitor patient activity levels more effectively and identify those who may benefit from interventions aimed at increasing physical activity. Moreover, the LoPAQ’s sensitivity to changes in activity levels makes it an ideal instrument for evaluating the effectiveness of such interventions, thereby contributing to the optimization of patient care and potentially improving health outcomes.
Our study has some limitations that should be addressed. This study focused solely on patients undergoing hemodialysis and did not include an examination of the screening ability of the LoPAQ in patients on peritoneal dialysis (PD). Given the shorter daily dialysis time constraints for PD patients, their lifestyle may differ from that of hemodialysis patients, who typically visit hospitals or clinics three times a week according to their dialysis schedule. Therefore, it is important to further investigate the LoPAQ’s screening ability in dialysis patients, including those on PD. Additionally, this study did not assess the extent to which the LoPAQ is responsive to changes in physical activity. Moreover, there is a limitation in our analysis concerning the impact of dialysis duration on physical activity levels. The literature suggests a negative correlation between extended dialysis treatment and physical activity [53,54,55], which our study was not equipped to explore due to the limited number of participants stratified by dialysis duration.
Despite this, our findings contribute to the body of knowledge and echo the need for a comprehensive assessment of physical activity in patients undergoing dialysis. We propose that future research should focus on larger cohorts that allow for stratification by dialysis duration to determine if the reliability of the LoPAQ is affected by the length of dialysis treatment.
Understanding this relationship has significant implications for clinical practice, as it may guide healthcare professionals in tailoring interventions to enhance the physical activity and overall well-being of patients on long-term dialysis.
Although the spoken Persian language may vary across regions and countries, the written language remains largely consistent. However, it is essential to consider the potential cultural and socioeconomic variations among Persian-speaking countries that might influence the generalizability of the findings. Cultural sensitivity is crucial in healthcare, as the cultural background of HD patients can significantly affect their treatment compliance and interaction with healthcare services [56]. Moreover, socioeconomic factors such as education level, income, and living conditions have been associated with health disparities and could impact the management and outcomes of HD patients [57]. Therefore, while the linguistic consistency provides a solid foundation for the study, a comprehensive understanding of the cultural and socioeconomic context is imperative to fully appreciate and apply the research outcomes to the broader Persian-speaking countries.
Conclusion
The Persian version of the LoPAQ had validity and excellent reliability. In addition, it was easier and less time-consuming than previously validated physical activity questionnaires. The LoPAQ demonstrated a good correlation with physical function among dialysis patients and can be used for assessing their physical activity level as well as predicting their performance.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- LoPAQ:
-
Low Physical Activity Questionnaire
- HD:
-
Hemodialysis
- CHAMPS:
-
Community Healthy Adults Model Program for Seniors
- CVD:
-
Cardiovascular Disease
- CCI:
-
Charlson Comorbidity Index
- MET:
-
Metabolic Equivalent of Task
- PF:
-
Physical Function
- SPPB:
-
Short Physical Performance Battery
- SD:
-
Standard Deviation
- CVI:
-
Content Validity Index
- ICC:
-
Intraclass Correlation Coefficient
- PD:
-
Peritoneal Dialysis
- GREX:
-
Global Renal Exercise
References
Deligiannis A, D’Alessandro C, Cupisti A. Exercise training in dialysis patients: impact on cardiovascular and skeletal muscle health. Clin Kidney J. 2021;14(Supplement2):ii25–33.
Ortiz A, Covic A, Fliser D, Fouque D, Goldsmith D, Kanbay M, et al. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet. 2014;383(9931):1831–43.
Johansen KL, Kaysen GA, Dalrymple LS, Grimes BA, Glidden DV, Anand S, et al. Association of physical activity with survival among ambulatory patients on dialysis: the comprehensive dialysis study. Clin J Am Soc Nephrology: CJASN. 2013;8(2):248.
Lopes AA, Lantz B, Morgenstern H, Wang M, Bieber BA, Gillespie BW, et al. Associations of self-reported physical activity types and levels with quality of life, depression symptoms, and mortality in hemodialysis patients: the DOPPS. Clin J Am Soc Nephrology: CJASN. 2014;9(10):1702.
Morishita Y, Nagata D. Strategies to improve physical activity by exercise training in patients with chronic kidney disease. Int J Nephrol Renovascular Disease. 2015:19–24.
Sugaya K, Hokama A, Hayashi E, Naka H, Oda M, Nishijima S, et al. Prognosis of bedridden patients with end-stage renal failure after starting hemodialysis. Clin Exp Nephrol. 2007;11:147–50.
KD W. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45:S1–153.
Parker K. Intradialytic exercise is medicine for hemodialysis patients. Curr Sports Med Rep. 2016;15(4):269–75.
Johannsen DL, Calabro MA, Stewart J, Franke W, Rood JC, Welk GJ. Accuracy of armband monitors for measuring daily energy expenditure in healthy adults. Med Sci Sports Exerc. 2010;42(11):2134–40.
Painter P, Marcus RL. Assessing physical function and physical activity in patients with CKD. Clin J Am Soc Nephrol. 2013;8(5):861–72.
Johansen KL, Painter P, Delgado C, Doyle J. Characterization of physical activity and sitting time among patients on hemodialysis using a new physical activity instrument. J Ren Nutr. 2015;25(1):25–30.
Avesani CM, Trolonge S, Deléaval P, Baria F, Mafra D, Faxén-Irving G, et al. Physical activity and energy expenditure in haemodialysis patients: an international survey. Nephrol Dialysis Transplantation. 2012;27(6):2430–4.
Gomes EP, Reboredo MM, Carvalho EV, Teixeira DR, Carvalho LFCO, JCAd O et al. Physical activity in hemodialysis patients measured by triaxial accelerometer. Biomed Res Int. 2015;2015.
Baria F, Kamimura MA, Avesani CM, Lindholm B, Stenvinkel P, Draibe SA, et al. Activity-related energy expenditure of patients undergoing hemodialysis. J Ren Nutr. 2011;21(3):226–34.
Mafra D, Fouque D. Lower physical activity and depression are associated with hospitalization and shorter survival in CKD. Clin J Am Soc Nephrology: CJASN. 2014;9(10):1669.
Hutto B, Howard VJ, Blair SN, Colabianchi N, Vena JE, Rhodes D, et al. Identifying accelerometer nonwear and wear time in older adults. Int J Behav Nutr Phys Activity. 2013;10(1):1–8.
Arian M, Mortazavi H, TabatabaeiChehr M, Varvani Farahani A, Kamali A, Amini Z. Relationship between activity level and perceived barriers and motivations to exercise in hemodialysis patients. J North Khorasan Univ Med Sci. 2014;6(3):483–95.
Mahmoodi B, Asghari G, Yuzbashian E, Mirmiran P, Azizi F. Association between physical activity and incidence of chronic kidney disease in participants of Tehran Lipid and glucose study. J Mazandaran Univ Med Sci. 2020;30(190):24–33.
Johansen KL, Painter P, Kent-Braun JA, Ng AV, Carey S, Da Silva M, et al. Validation of questionnaires to estimate physical activity and functioning in end-stage renal disease. Kidney Int. 2001;59(3):1121–7.
Johansen KL, Chertow GM, Ng AV, Mulligan K, Carey S, Schoenfeld PY, et al. Physical activity levels in patients on hemodialysis and healthy sedentary controls. Kidney Int. 2000;57(6):2564–70.
Li M, Li L, Fan X. Patients having haemodialysis: physical activity and associated factors. J Adv Nurs. 2010;66(6):1338–45.
Tabibi MA, Cheema B, Salimian N, Corrêa HL, Ahmadi S. The effect of intradialytic exercise on dialysis patient survival: a randomized controlled trial. BMC Nephrol. 2023;24(1):100.
Hawkins M, Newman AB, Madero M, Patel KV, Shlipak MG, Cooper J, et al. TV watching, but not physical activity, is associated with change in kidney function in older adults. J Phys Activity Health. 2015;12(4):561–8.
Samitz G, Egger M, Zwahlen M. Domains of physical activity and all-cause mortality: systematic review and dose–response meta-analysis of cohort studies. Int J Epidemiol. 2011;40(5):1382–400.
Wen CP, Wai JPM, Tsai MK, Yang YC, Cheng TYD, Lee M-C, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011;378(9798):1244–53.
Woodcock J, Franco OH, Orsini N, Roberts I. Non-vigorous physical activity and all-cause mortality: systematic review and meta-analysis of cohort studies. Int J Epidemiol. 2011;40(1):121–38.
Huang R, Zhang H, Yang Y, Fang N, Liu Q, Ma J, et al. Validation of the Chinese version of the low physical activity questionnaire (LoPAQ) with ActiGraph accelerometer in hemodialysis patients. BMC Nephrol. 2021;22:1–8.
Yamabe S, Yamamoto S, Harada M, Suzuki Y, Imamura K, Yoshikoshi S, et al. Utility of the low physical activity questionnaire for hemodialysis patients with frailty: a cross-sectional study. Ren Replace Therapy. 2023;9(1):61.
Liu J, Huang Z, Gilbertson DT, Foley RN, Collins AJ. An improved comorbidity index for outcome analyses among dialysis patients. Kidney Int. 2010;77(2):141–51.
Eremenco S, Pease S, Mann S, Berry P. Patient-reported outcome (PRO) Consortium translation process: consensus development of updated best practices. J Patient-Reported Outcomes. 2018;2(1):1–11.
Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee-Lorenz A, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104.
Who. Process of translation and adaptation of instruments. World Health Organization; 2015.
Stewart AL, Mills KM, King AC, Haskell WL, Gillis D, Ritter PL. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med Sci Sports Exerc. 2001;33(7):1126–41.
Moore DS, Ellis R, Allen PD, Monroe PA, Cherry KE, O’Neil CE, et al. Construct validation of physical activity surveys in culturally diverse older adults: a comparison of four commonly used questionnaires. Res Q Exerc Sport. 2008;79(1):42–50.
Feldman LS, Kaneva P, Demyttenaere S, Carli F, Fried GM, Mayo NE. Validation of a physical activity questionnaire (CHAMPS) as an indicator of postoperative recovery after laparoscopic cholecystectomy. Surgery. 2009;146(1):31–9.
Rosario MG, Vázquez JM, Cruz WI, Ortiz A. Internal consistency of the CHAMPS physical activity questionnaire for Spanish speaking older adults. P R Health Sci J. 2008;27(3).
Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr, Montoye HJ, Sallis JF, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc. 1993;25(1):71–80.
Ware JE. SF-36 physical and mental health summary scales: a user’s manual. (No Title). 1994.
Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–94.
Sarmad Z, Bazargan A, Hejazi E. Research methods in behavioral sciences. Tehran: Agah Publication. 2004;1:132–7.
Ghasemi A, Zahediasl S. Normality tests for statistical analysis: a guide for non-statisticians. Int J Endocrinol Metabolism. 2012;10(2):486.
Gélinas C, Puntillo KA, Boitor M, Bérubé M, Topolovec-Vranic J, Ramelet A-S, et al. Content validation of behaviours and autonomic responses for the assessment of pain in critically ill adults with a brain injury. Australian Crit Care. 2018;31(3):145–51.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. biometrics. 1977:159 – 74.
Cooperstein R, Young M. The reliability of lumbar motion palpation using continuous analysis and confidence ratings: choosing a relevant index of agreement. J Can Chiropr Assoc. 2016;60(2):146.
Kim J, Shapiro B, Zhang M, Li Y, Porszasz J, Bross R, et al. Daily physical activity and physical function in adult maintenance hemodialysis patients. J cachexia Sarcopenia Muscle. 2014;5:209–20.
Zelle DM, Klaassen G, Van Adrichem E, Bakker SJ, Corpeleijn E, Navis G. Physical inactivity: a risk factor and target for intervention in renal care. Nat Rev Nephrol. 2017;13(3):152–68.
Bravata DM, Smith-Spangler C, Sundaram V, Gienger AL, Lin N, Lewis R, et al. Using pedometers to increase physical activity and improve health: a systematic review. JAMA. 2007;298(19):2296–304.
Sylvia LG, Bernstein EE, Hubbard JL, Keating L, Anderson EJ. A practical guide to measuring physical activity. J Acad Nutr Dietetics. 2014;114(2):199.
Lagerros YT, Lagiou P. Assessment of physical activity and energy expenditure in epidemiological research of chronic diseases. Eur J Epidemiol. 2007;22:353–62.
Ghanbari H, Rahimian M. Persian language dominance and the loss of minority languages in Iran. Open J Social Sci. 2020;8(11):8–18.
Aaronson N, Acquadro C, Alonso J, Apolone G, Bucquet D, Bullinger M, et al. International quality of life assessment (IQOLA) project. Qual Life Res. 1992;1:349–51.
Herdman M, Fox-Rushby J, Badia X. A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approach. Qual Life Res. 1998;7:323–35.
Bakker EA, Zoccali C, Dekker FW, Eijsvogels TM, Jager KJ. Assessing physical activity and function in patients with chronic kidney disease: a narrative review. Clin Kidney J. 2021;14(3):768–79.
Lambert K, Lightfoot CJ, Jegatheesan DK, Gabrys I, Bennett PN. Physical activity and exercise recommendations for people receiving dialysis: a scoping review. PLoS ONE. 2022;17(4):e0267290.
Rosa CS, Bueno DR, Souza GD, Gobbo LA, Freitas IF, Sakkas GK, et al. Factors associated with leisure-time physical activity among patients undergoing hemodialysis. BMC Nephrol. 2015;16:1–7.
Khanijahani A, Iezadi S, Gholipour K, Azami-Aghdash S, Naghibi D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int J Equity Health. 2021;20:1–30.
Shali M, Bakhshi F, Hasanpour M. Culture of patient care among international nursing students: a focused ethnographic study. BMC Nurs. 2024;23(1):163.
Acknowledgements
The authors would like to express their heart-felt gratitude to all the investigators for their contribution to the trial, especially Dr. Kirsten L. Johansen and all the staff of the dialysis centers for their efforts and patience in helping to maintain the standards of the research, as well as all patients involved in this study. Also, the authors would like to thank Pardis Specialized Wellness Institute and all the personnel of the institute for their support throughout the study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
conceptualizing the study, conducting the study, writing of the manuscript, supervising of the manuscript, approval of the manuscript: MAT, RS, NS, SS, AA, FN, MG, SN, MH, MS, ZR, BK, ZK, AS, RE, SA; data analysis/interpretation: MAT, NS; statistical analysis: NAS; supervision or mentorship: MAT, RS, NS. Each author contributed with important intellectual content during the manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol and informed consent were approved by Iran National Committee for Ethics in Biomedical Research (approval number IR.MUI.NUREMA.REC.1401.161) and was conducted in accordance with principles of the Declaration of Helsinki. All patients provided written informed consent prior to enrollment.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tabibi, M.A., Samouei, R., Salimian, N. et al. Validity and reliability of Persian version of Low Physical Activity Questionnaire (LoPAQ). BMC Nephrol 25, 178 (2024). https://doi.org/10.1186/s12882-024-03615-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-024-03615-w