
Abstract
Background
Few drug dosing recommendations for patients receiving home hemodialysis (HHD) have been published which has hindered the adoption of HHD. HHD regimens vary widely and differ considerably from conventional, thrice weekly, in-center hemodialysis in terms of treatment frequency, duration and blood and dialysate flow rates. Consequently, vancomycin and daptomycin clearances in HHD are also likely to be different, consequently HHD dosing regimens must be developed to ensure efficacy and minimize toxicity when these antibiotics are used. Many HHD regimens are used clinically, this study modeled ten common HHD regimens and determined optimal vancomycin and daptomycin dosing for each HHD regimen.
Methods
Monte Carlo simulations using pharmacokinetic data derived from the literature and demographic data from a large HHD program treating patients with end stage kidney disease were incorporated into a one-compartment pharmacokinetic model. Virtual vancomycin and daptomycin doses were administered post-HHD and drug exposures were determined in 5,000 virtual patients receiving ten different HHD regimens. Serum concentration monitoring with subsequent dose changes was incorporated into the vancomycin models. Pharmacodynamic target attainment rates were determined for each studied dose. The lowest possible doses that met predefined targets in virtual patients were chosen as optimal doses.
Results
HHD frequency, total dialysate volumes and HHD durations influenced drug exposure and led to different dosing regimens to meet targets. Antibiotic dosing regimens were identified that could meet targets for 3- and 7-h HHD regimens occurring every other day or 4–5 days/week. HHD regimens with 3-day interdialytic periods required higher doses prior to the 3-day period. The addition of vancomycin serum concentration monitoring allowed for calculation of necessary dosing changes which increased the number of virtual subjects meeting pharmacodynamic targets.
Conclusions
Doses of vancomycin and daptomycin that will meet desired pharmacodynamic targets in HHD are dependent on patient and HHD-specific factors. Doses used in conventional thrice weekly hemodialysis are unlikely to meet treatment goals. The antibiotic regimens paired with the HHD parameters studied in this analysis are likely to meet goals but require clinical validation.
Similar content being viewed by others

Background
Home hemodialysis (HHD) offers a more flexible and convenient dialysis schedule for patients to treat their end stage kidney disease (ESKD), compared to in-center hemodialysis with its rigid thrice-weekly schedule. HHD also allows individualized dialysis delivery with more frequent and/or longer session to meet patient’s solute and fluid control needs. Studies report that HHD is associated with improved survival, cardiovascular outcomes, quality of life, and cost-effectiveness [1,2,3,4]. Despite increasing perception of these clinical and lifestyle benefits, HHD is underutilized in the United States. Between 2009 and 2019, the percentage of patients receiving home dialysis (peritoneal dialysis and HHD) only increased from 1.2% to 1.9% [5]. In 2019, only 0.3% of patients who initiate dialysis started with HHD [5].
Recently, the U.S. Department of Health and Human Services launched the Advancing American Kidney Health initiative to improve care for patients with kidney disease and set a goal to significantly increase access and uptake of HHD for ESKD patients [6]. HHD presents an opportunity to reach more ESKD patients to receive dialysis treatment, but several barriers exist preventing its wide utilization. One of them is lack of drug dosing information for HHD patients. HHD regimens vary in frequency, duration and dialysate volume from patient to patient and all differ from thrice-weekly in-center hemodialysis treatments. Thus, optimal dosing of dialyzable drugs for HHD patients may differ from the dosing used in thrice-weekly in-center hemodialysis patients.
Infection remains the second leading cause of morbidity and mortality in ESKD patients [5]. Vancomycin and daptomycin are two most commonly prescribed antibiotic agents to treat methicillin-resistant Staphylococcus aureus (MRSA) infections in outpatient dialysis centers [7]. The pharmacokinetics of vancomycin and daptomycin have been well characterized in ESKD patients receiving typical thrice-weekly intermittent hemodialysis (IHD), and both agents are cleared by high-flux dialyzers [8, 9]. No regulatory authorities mandate conducting clinical pharmacokinetic trials of marketed drugs in HHD patients. FDA guidance recommends that pharmacokinetics of drugs be investigated in ESKD patients receiving dialysis, but it primarily refers to thrice-weekly IHD, the most common dialysis modality in the U.S. [10]. Few clinical pharmacokinetic studies of commonly used antibiotics in HHD have been conducted. In lieu of such trials, modeling and simulation can predict the influence of HHD on drug exposure [11, 12] and support clinical dosing decisions. The purpose of the present study was to predict the optimal initial vancomycin and daptomycin dosing regimens in patients receiving common HHD settings using pharmacokinetic modeling and Monte Carlo simulation techniques. Additionally, this study attempted to develop a therapeutic drug monitoring (TDM) strategy to further individualize the subsequent vancomycin regimens in HHD patients because vancomycin serum concentration monitoring is readily available.
Methods
Part I. Prediction of optimal vancomycin and daptomycin dosing regimens in patients with HHD
Development of pharmacokinetic models
One compartment, first order pharmacokinetic models were developed to construct vancomycin [13, 14] and daptomycin exposure in virtual patients with ESKD receiving HHD. Table 1 outlines the input parameters used in the models. Patients’ body weight data was obtained from a large population of ESKD patients receiving HHD at Fresenius outpatient dialysis centers [internal data] and pharmacokinetic parameters with variances were derived from published vancomycin and daptomycin studies in ESKD patients receiving high-flux dialysis treatments [9, 14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Numerous possible scenarios exist regarding when each HHD session occurs during the week and when to administer drug in relation to HHD session. However, it is not feasible to simulate all possible HHD scenarios. Thus, we devised a fixed HHD schedule for each HHD setting utilizing most frequently used settings in real-world HHD. The models were constructed for 10 different HHD settings with different dialysate flow rates (Qd) and dialysis treatment durations as displayed in Fig. 1. Transmembrane drug clearance in hemodialysis is a function of Qd and saturation coefficient (ratio of dialysate concentration to plasma concentration). Regression analyses were conducted using published data on transmembrane drug clearance and effluent flow rates to estimate saturation coefficients at various Qd in HHD [14, 16, 17, 19, 22,23,24,25,26,27,28,29,30,31,32,33]. The best fitting relationships were modeled to estimate saturation coefficient at the desired Qd in HHD. The variability of the saturation coefficient expressed as 20% of the standard deviation was incorporated into the models. Body weight was truncated at less than 40 kg with the assumption that virtual patients were adults that weighed at least 40 kg. Patients were assumed to be anuric and therefore had no endogenous renal clearance. All input parameters were assumed to display log-Gaussian distribution. The equations used in the model were as follows:
where CLHHD is the transmembrane clearance during HHD, SA is the saturation coefficient, Qd is the dialysate flow rate, Ke_on is the elimination rate constant during HHD, CLNR is non-renal clearance, Vd is volume of distribution, and Ke_off is the elimination rate constant inter-HHD period.

Simulated Home Hemodialysis Schedules
Pharmacodynamic targets
The vancomycin target for MRSA infection in patients with normal kidney function is the 24-h area under the curve:minimum inhibitory concentration (AUC24h:MIC) ratio of 400–600 assuming a MIC of 1 mg/L [34]. This target balances efficacy and the risk of vancomycin-associated nephrotoxicity. However, the upper AUC24h threshold of 600 mg∙h/L associated with nephrotoxicity is of less concern to ESKD patients already receiving dialysis. The simulated HHD patients in this study were assumed to be anuric. Thus, AUC24h ≥ 400 mg∙h/L was used as the primary vancomycin target to find the optimal dose. Additionally, the dose with the mean AUC24h of 400–600 mg∙h/L was preferred to avoid excessive drug exposure and other toxicities.
For daptomycin, the AUC:MIC ratio is also the pharmacodynamic index that is most predictive of bactericidal effect [35, 36], but the precise target of AUC:MIC ratio has not been clearly established. The interquartile ranges (IQR) of AUC24h 465–761 mg∙h/L was suggested as the target efficacy exposure based on the data of patients with severe S. aureus infection and CrCl ≥ 30 ml/min, receiving daptomycin 6 mg/kg every 24 h in the largest clinical trial [37, 38]. Additionally, the 75th percentiles of AUC24h 1422 mg∙h/L was proposed as a reasonable safety threshold in another study with individuals with normal renal function who received and well tolerated the highest test dose (12 mg/kg every 24 h) [37, 39]. Thus, we used the IQR of AUC24h 465–1422 mg∙h/L as primary target to determine optimal daptomycin dosing regimens in simulated HHD patients [37].
Monte Carlo simulations and prediction of optimal dosing regimen
Various weight-based vancomycin and daptomycin dosing regimens were evaluated in this analysis. All doses were simulated to be infused after HHD ended. Vancomycin infusion time was 1 h for the doses ≤ 10 mg/kg, 2 h for the doses > 10 mg/kg and ≤ 20 mg/kg, and 3 h for the doses > 20 mg/kg. The maximum loading dose (LD) and maintenance dose (MD) for vancomycin were capped as 3 g and 2 g respectively based on the guidelines [34]. Daptomycin infusion time was consistent with 0.5 h for all doses. The maximum LD and MD for daptomycin were capped as 1.5 g [39]. Monte Carlo simulation (MCS)(Crystal Ball Classroom Edition, Oracle) was performed to generate a week of plasma drug concentration–time profiles of 5,000 virtual patients for each tested vancomycin and daptomycin regimen in each of 10 different HHD settings for one week. The AUC24h for each day of vancomycin and daptomycin therapy was computed using the linear trapezoidal rule.
For vancomycin, probability of target attainment (PTA) was calculated by summing up the number of virtual patients attaining the AUC24h ≥ 400 mg∙h/L and dividing by the total number (n = 5,000) of virtual patients. Optimal vancomycin doses were defined as the smallest dose attaining a PTA ≥ 90% preferably with the mean AUC24h 400–600 mg∙h/L in the simulated patients for each HHD setting. For daptomycin, a regimen is considered “optimal” if its resulted IQRs of AUC24h in 5,000 simulated patients was within the target IQR of AUC24h 465–1422 mg∙h/L in each HHD setting.
Part II. Development of vancomycin therapeutic drug monitoring strategy in patients with HHD
Therapeutic drug monitoring (TDM) is routinely performed for vancomycin therapy. Previously, we developed a technique to integrate TDM and subsequent vancomycin dose individualization into virtual patients receiving different types of renal replacement therapy [11, 40]. Using this technique, we modeled how TDM can be effectively utilized for HHD patients and attempted to develop a practical vancomycin dose adjustment protocol to guide clinicians. In the simulation, TDM in HHD patients used a single pre-dialysis concentration based on the current guideline recommendations [34] and the initial vancomycin doses were adjusted to attain and/or maintain AUC24h of 400–600 mg∙h/L.
The nomogram for dose adjustment protocol was developed based on the predicted vancomycin concentrations in virtual patients with HHD receiving one week of vancomycin dosing regimens recommended from Part I. A single pre-dialysis vancomycin concentration measured immediately prior to the last HHD session of the first week was used as the basis of TDM. The subsequent dose targeting to attain and/or maintain AUC24h of 400–600 mg∙h/L were given after the first HHD of the second week. For example, in a setting where HHD occurs 5 times per week (Mon-Tue-Wed-Thu-Fri), a pre-dialysis concentration was measured prior to HHD session on Friday of the first week of vancomycin therapy, and the adjusted dose was given after the first HHD session of the following week. The decision to adjust the first dose of the next Monday was made for practical reasons. Patients receiving HHD at home would be unlikely to receive TDM results in a timely enough manner to adjust doses any faster. The virtual vancomycin assay results were assumed to be accurate and reflect the model-derived concentrations at that time point. Using the predicted pre-dialysis concentrations and pharmacokinetic profiles selected in the simulation of Part I, the second week of vancomycin concentrations with the adjusted dose was further constructed to estimate AUC24h in each of 5,000 virtual patients. Finally, the equation was derived to individualize a subsequent dose achieving AUC24h of 400–600 mg∙h/L in most patients.
Results
Part I. Determination of optimal vancomycin and daptomycin dosing regimens
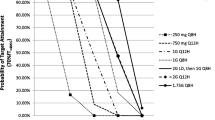
Tables 2 and 3 display PTA and predicted AUC24h of simulated vancomycin dosing regimens in 10 different HHD settings. MCS analyses indicate that dialysis factors (ie. dialysate flow rate, dialysis treatment duration and interdialytic period) influenced the PTA of simulated vancomycin doses in HHD patients, necessitating different initial dosing regimens in different HHD settings. It is predicted that the vancomycin regimens consisting of a LD of 25 mg/kg post-HHD, followed by MD 5–10 mg/kg administered after each HHD would attain the desired PD target (AUC24h ≥ 400 mg∙h/L) in ~ 90% of simulated patients on each day of the first week of vancomycin therapy with a mean AUC24h of closest to 400–600 mg∙h/L. Notably, for 3-h HHD occurring 4 times per week (Mon-Tue-Thu-Fri) and 7-h HHD occurring 5 times per week (Mon-Tue-Wed-Thu-Fri), a 30–50% higher Friday MD was required to maintain sufficient drug exposure for 3-day interdialytic periods compared to a MD for 1–2-day interdialytic period. Five times per week 3-h HHD occurring (Mon-Tue-Wed-Thu-Fri) with a Qd of 6.7 L/hr or 10 L/hr resulted in lesser dialytic removal (13–17%) during each HHD session, allowing vancomycin administration to occur after HHD only on Mon, Wed and Fri.
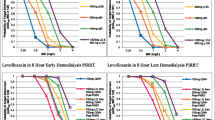
One week of predicted AUC24h IQRs of simulated daptomycin dosing regimens in 10 different HHD settings are reported in the supplementary material. MCS results indicated that daptomycin 4 mg/kg post-HHD with a 2 mg/kg supplemental dose on the 3rd day of 3-day interdialytic period would be optimal in asymmetrical HHD settings where HHD occurs 4–5 times per week. Daptomycin dosing regimens without a supplementary dose on the last day of 3-day interdialytic period did not meet the target IQR range of AUC24h (465–1422 mg∙h/L) during each day of 3-day interdialytic period. For symmetrical HHD settings where HHD occurs every other day, daptomycin 6 mg/kg given after HHD would be optimal, attaining the target IQR of AUC24h. Figure 2 depicts one week of the predicted IQR of AUC24h with our model-recommended daptomycin dosing regimens in ten different HHD settings.

One Week of Predicted AUC24h IQR with Model-recommended Daptomycin Regimens in Ten Home Hemodialysis Settings
Part II. Vancomycin therapeutic drug monitoring strategy in patients with HHD
MCS results suggested that TDM targeting a pre-dialysis concentration of 24 mg/L would ensure AUC24h ≥ 400 mg∙h/L in ≥ 90% of virtual patients in all HHD settings, following the model-recommended initial doses for a week. Thus, the new MD was to be proportionally adjusted from the initial MD to attain a pre-dialysis concentration of 24 mg/L as the equation below. Of note, in HHD settings where a HHD occurs 4–5 times per week (Mon-Tue-Thu-Fri or Mon-Tue-Wed-Thu-Fri), a 30% higher Friday dose was necessary to maintain PTA ≥ 90% on the third day of a 3-day interdialytic period.
Figure 3A-D illustrate the proportions of simulated patients (n = 5,000) attaining AUC24h < 400, 400–600, and ≥ 600 mg∙h/L during 2 weeks of vancomycin therapy (ie. initial recommended regimens for the first week, followed by subsequently adjusted MD directed by TDM for the second week). Overall, the TDM-guided individualized dosing strategy with a target pre-dialysis concentration of 24 mg/L yielded a higher proportion of patients attaining AUC24h 400–600 mg∙h/L, and decreased the proportions of those with sub-therapeutic (AUC24h < 400 mg∙h/L) or excessive drug exposure (AUC24h > 600 mg∙h/L), compared to those resulted from the initial regimens. The mean AUC24h on each day after dose adjustment with TDM ranged from 400 to 600 mg∙h/L, with an exception of 3-h HHDs occurring 5 times per week (Mon-Tue-Wed-Thu-Fri). In this setting, the recommended dosing regimen needed to be given less frequently (i.e. Mon-Wed-Fri only), but a higher MD was necessary to ensure the target attainment on days when vancomycin was not given.

Frequency of Mean Vancomycin AUC24h Before and After Virtual TDM
Discussion
This is the first in silico study to determine the optimal initial dosing recommendations of vancomycin and daptomycin in patients receiving HHD in various dialysis regimens. The MCS techniques enabled us to assess the PTA of various vancomycin and daptomycin dosing regimens in each of ten different HHD settings and to predict the ones that are likely to attain the therapeutic targets in most patients. As expected, optimal vancomycin and daptomycin dosing regimens for HHD (Table 4) would differ from usual doses recommended for thrice weekly high-flux IHD (25 mg/kg LD, 10 mg/kg MD post-dialysis for vancomycin and 4–6 mg/kg post-dialysis for daptomycin) [21, 34].
For vancomycin, HHD variables including the frequency, duration and dialysate flow rates influenced vancomycin exposure (AUC24h) thereby altering the optimal dosing regimen with different HHD regimens, as shown in Tables 2 and 3. For example, 7-h HHD occurring 5 times a week (Mon-Tue-Wed-Thu-Fri) with Qd of 4.3 L/hr required 25 mg/kg LD, 5–5-5–7.5 mg/kg post-HHD to attain the PD target on each day for one week, while the same HHD with Qd of 8.6 L/hr necessitated 25 mg/kg LD, 5–5-5–10 mg/kg dosing to meet targets. The optimal vancomycin doses for 7-h HHD with Qd 4.3 L/hr was 25 mg/kg LD, 7.5 mg/kg post-HHD if occurring every other day, but 25 mg/kg LD, 5–5-5–7.5 mg/kg would be optimal if the same HHD session occurred 5 times a week (Mon-Tue-Wed-Thu-Fri), highlighting the impact of HHD frequency on required dosing regimens. In addition to efficacy/safety targets, practical dosing considerations were explored via MCS. For 3-h HHD with Qd 6.7 L/hr occurring 5 times a week, we determined that 25 mg/kg LD, 0–7.5–0-7.5 mg/kg post-HHD (ie. no dose given on Tue and Thur) would be better than 25 mg/kg LD, 5–5-5–7.5 mg/kg post-HHD (ie. 5–7.5 mg/kg given after each of all HHD sessions) because it reduced the dosing frequency with smaller total weekly doses while attaining the efficacy target with lower AUC24h on each day compared to the latter regimen.
This present study also used the previously developed “virtual TDM” technique [11, 40] to mimic the clinical situation and further guide the subsequent dosing for clinicians. The MCS analysis indicated that targeting pre-dialysis concentrations of 20–24 mg/L after one week of our recommended initial regimens would attain and/maintain an AUC24h ≥ 400 mg∙h/L for the following week in most simulated patients with 10 different HHD (Fig. 3). Thus, virtual TDM was designed to target a pre-dialysis concentration of 24 mg/L to ensure the target attainment in virtual patients with all simulated HHD settings. This pre-dialysis concentration target may result in a slightly higher new MD than necessary in some HHD settings. For example, the adjusted MD after TDM using this target pre-dialysis concentration in 3-h HHD occurring 5 times a week resulted in the target (AUC24h ≥ 400 mg∙h/L) attainment in almost all virtual patients, but a higher proportion of patients had AUC24h ≥ 600 mg∙h/L. However, this pre-dialysis concentration of 24 mg/L was found to be the best predictor for attaining targets in all simulated HHD settings. This target pre-dialysis concentration of 24 mg/L is also higher than those (15–20 mg/L) recommended in patients receiving thrice weekly IHD in the vancomycin consensus guidelines [33]. Of note, this guideline recommendation is based on another MCS study showing that pre-dialysis vancomycin concentrations of 10–20 mg/L would results in mean AUC24h from 250 to 450 mg·h/L in patients receiving thrice IHD [34, 40]. The mean new TDM-based vancomycin MD in all HHD settings were not significantly different from the model-recommended initial MD in each HHD setting, but some virtual patients are predicted to need a new MD that was different from the initial dose to attain the target (Fig. 3). Based on these findings, we recommend weekly TDM to ensure all HHD patients to receive the optimal doses during prolonged vancomycin therapy. Any change in patient’s clinical condition and/or HHD modification also warrant TDM to ensure target attainment in these patients.
Optimal daptomycin dosing regimens (Table 4) differed whether HHD occurs symmetrically (ie. every other day) or asymmetrically (ie. 4–5 times a week). MCS predicted that daptomycin 6 mg/kg post-HHD would be optimal in simulated symmetrical HHD settings, but would not successfully attain the target range (IQR range of AUC24h 465–1422 mg∙h/L) in asymmetrical HHD settings. In asymmetrical HHD settings, modeled HHD had a 3-day interdialytic period (ie. Fri-Mon). Simulated fixed dosing regimens (4–8 mg/kg post-HHD) with or without a higher dose on the first day (ie. Fri) of 3-day interdialytic period did not fall within the target IQR range of AUC24h.. For example, in 3-h HHD with Qd 10 L/hr occurring 4 times a week (Mon-Tue-Thu-Fri), daptomycin 4 mg/kg post-HHD for a 3-day interdialytic period (Fri-Sun) attained the target IQR range of AUC24h during the first two days (ie. Fri and Sat), but was not sufficient to maintain the target on the last day (ie. Sun) with an AUC24h IQR range of 257–698 mg∙h/L. To meet the challenge of attaining the target on the Sunday, we simulated 4 mg/kg post-HHD with a 6 mg/kg post-HHD prior to the 3-day interdialytic period in the same HHD setting. Although daptomycin 6 mg/kg post-HHD on day 5 (ie. Fri) achieved the IQR AUC24h target range on the last day of 3-day interdialytic period (ie. Sun), this dose resulted in the IQR AUC24h range of 1146–1640 mg∙h/L on the first day (Fri) of 3-day interdialytic period, exceeding the target IQR range (465–1422 mg∙h/L). Thus, daptomycin dosing regimen utilizing a supplementary dose on the last day of 3-day interdialytic period was simulated to attain the target range during each day of 3-day interdialytic period. MCS showed that daptomycin 4 mg/kg post-HHD with a 2 mg/kg supplementary dose on 3rd day of 3-day interdialytic period would be optimal in all asymmetric HHD settings.
This study has several limitations to consider before clinicians apply the findings from the MCS analysis in practice. First, pharmacokinetic modeling and simulations were performed based on the assumption that patients are > 40 kg adults receiving HHD and were anuric. It was also assumed that no changes in pharmacokinetic parameters and HHD regimen occurred during the modeled period. Virtual patients were constructed based on demographic information from ESKD patients receiving HHD and pharmacokinetic characteristics with variances from the published studies conducted in ESKD patients receiving dialysis. It should be noted that we did not model all possible HHD scenarios, but only in ten common HHD Qd and treatment durations within a fixed schedule where antibiotic doses are initiated on Monday after HHD. Hence, our model-recommended doses should be applied to only anuric patients with similar demographic characteristics and HHD scenarios. If vancomycin therapy is initialed on Friday, we would recommend a 30% higher LD with a maximum dose of 3,000 mg [34] for a 3-day interdialytic period. The recommended initial MD can be given for the following week and TDM can be performed on Friday of that same following week to determine the subsequent MD attaining the target for an individual patient. In contrast, daptomycin therapy started on Friday in patients receiving asymmetric HHD, 4 mg/kg dose can be given after HHD on Friday with a supplemental dose of 2 mg/kg on Sunday. Thereafter our model-recommended daptomycin doses can be followed for the following week. Secondly, we modeled vancomycin infusion rates to be 1 h for the doses ≤ 10 mg/kg, 2 h for the doses > 10 mg/kg and ≤ 20 mg/kg, and 3 h for the doses > 20 mg/kg with max doses of 3 g and 2 g for LD and MD respectively. This would result in faster infusion rates than typical practice (e.g. 1 g over 1 h or 2 g over 2 h) in larger virtual patients (ie. body weight > 100 kg). However, such standardization was necessary to simulate each vancomycin dosing in 5,000 patients simultaneously. Third, we primarily used the “efficacy” target (AUC24h ≥ 400 mg∙h/L assuming the MRSA MIC of 1 mg/L) to select initial vancomycin dosing recommendation and the target pre-dialysis concentration for TDM. However, these selected doses and the target pre-dialysis concentration resulted in high drug exposure exceeding the toxicity threshold (AUC24h ≥ 600 mg∙h/L) in some virtual patients. Vancomycin-induced nephrotoxicity may be less of concern, but potentially increased risk of other vancomycin toxicity including ototoxicity should be noted. Thus, prior to the application of our model-recommended initial vancomycin dose, we recommend clinicians consider patient’s body weight, HHD setting and clinical status to weigh the benefit vs. toxicity risk. TDM should be performed to further optimize individual patient’s subsequent vancomycin dose. Finally, daptomycin dosing regimens were simulated only for 1 week to determine optimal dose in each of ten HHD settings in this present study. However, HHD patients may receive more than one week of daptomycin therapy. As patients continue our recommended initial daptomycin doses, drug accumulation may occur in some patients. Unfortunately, TDM with daptomycin therapy is not commonly available. Thus, we strongly recommend clinicians monitor CPK at least once a week to assess the increased risk of muscle toxicity, as well as the related symptoms such as myopathy or weakness of the extremities.
Conclusion
As the use of HHD grows, vancomycin and daptomycin will be used increasingly to treat gram-positive infections. While clinical validation of our findings is necessary, this MCS suggests that the variety of HHD regimens used in clinical practice affects vancomycin and daptomycin doses required to achieve therapeutic target. We were able to develop initial vancomycin and daptomycin dosing regimens and vancomycin TDM strategies for ten of the most used HHD regimens.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AUC24h :
-
24-Hour area under the curve
- MIC:
-
Minimum inhibitory concentration
- ESKD:
-
End stage kidney disease
- HHD:
-
Home hemodialysis
- IHD:
-
Intermittent hemodialysis
- IQR:
-
Interquartile ranges
- LD:
-
Loading dose
- MCS:
-
Monte Carlo simulation
- MD:
-
Maintenance dose
- Qd:
-
Dialysate flow rate
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- PTA:
-
Probability of target attainment
- TDM:
-
Therapeutic drug monitoring
References
McCullough PA, Chan CT, Weinhandl ED, Burkart JM, Bakris GL. Intensive hemodialysis, left ventricular hypertrophy, and cardiovascular disease. Am J Kidney Dis. 2016;68(5S1):S5–14.
Rydell H, Ivarsson K, Almquist M, Segelmark M, Clyne N. Improved long-term survival with home hemodialysis compared with institutional hemodialysis and peritoneal dialysis: a matched cohort study. BMC Nephrol. 2019;20(1):52.
Kraus MA, Fluck RJ, Weinhandl ED, Kansal S, Copland M, Komenda P, Finkelstein FO. Intensive hemodialysis and health-related quality of life. Am J Kidney Dis. 2016;68(5S1):S33–42.
Howell M, Walker RC, Howard K. Cost effectiveness of dialysis modalities: a systematic review of economic evaluations. Appl Health Econ Health Policy. 2019;17(3):315–30.
United States Renal Data System. 2021 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2021.
Advancing American Kidney Health: 2020 Progress Report. ASPE. Available at: https://aspe.hhs.gov/pdf-report/advancing-americankidney-health-2020-progress-report. Accessed 13 May 2022.
Snyder GM, Patel PR, Kallen AJ, Strom JA, Tucker JK, D’Agata EM. Antimicrobial use in outpatient hemodialysis units. Infect Control Hosp Epidemiol. 2013;34(4):349–57.
Scott MK, Mueller BA, Clark WR. Vancomycin mass transfer characteristics of high-flux cellulosic dialysers. Nephrol Dial Transplant. 1997;12(12):2647–53.
Salama NN, Segal JH, Churchwell MD, Patel JH, Gao L, Heung M, Mueller BA. Intradialytic administration of daptomycin in end stage renal disease patients on hemodialysis. Clin J Am Soc Nephrol. 2009;4(7):1190–4.
Food and Drug Administration, Center for Drug Evaluation and Research. Pharmacokinetics in patients with impaired renal function - study design, data analysis, and impact on dosing. https://www.fda.gov/media/78573/download Cited (2020). Accessed 20 June 2022.
Lewis SJ, Mueller BA. Development of a vancomycin dosing approach for critically ill patients receiving hybrid hemodialysis using Monte Carlo simulation. SAGE Open Med. 2018;6:2050312118773257.
Lewis SJ, Kays MB, Mueller BA. Use of Monte Carlo simulations to determine optimal carbapenem dosing in critically ill patients receiving prolonged intermittent renal replacement therapy. J Clin Pharmacol. 2016;56(10):1277–87.
Wu G, Furlanut M. Prediction of serum vancomycin concentrations using one-, two- and three-compartment models with implemented population pharmacokinetic parameters and with the Bayesian Method. J Pharm Pharmacol. 1998;50(8):851–6.
Ariano RE, Fine A, Sitar DS, Rexrode S, Zelenitsky SA. Adequacy of a vancomycin dosing regimen in patients receiving high-flux hemodialysis. Am J Kidney Dis. 2005;46(4):681–7.
Internal data from the Fresenius/NxStage
DeSoi CA, Sahm DF, Umans JG. Vancomycin elimination during high-flux hemodialysis: kinetic model and comparison of four membranes. Am J Kidney Dis. 1992;20(4):354–60.
Salama NN, Segal JH, Churchwell MD, Patel JH, Gao L, Heung M, Mueller BA. Single-dose daptomycin pharmacokinetics in chronic haemodialysis patients. Nephrol Dial Transplant. 2010;25(4):1279–84.
Benziger DP, Pertel PE, Donovan J, Yankelev S, Schwab RJ, Swan SK, Cannon C. Pharmacokinetics and safety of multiple doses of daptomycin 6 mg/kg in noninfected adults undergoing hemodialysis or continuous ambulatory peritoneal dialysis. Clin Nephrol. 2011;75(1):63–9.
Patel N, Cardone K, Grabe DW, Meola S, Hoy C, Manley H, Drusano GL, Lodise TP. Use of pharmacokinetic and pharmacodynamic principles to determine optimal administration of daptomycin in patients receiving standardized thrice-weekly hemodialysis. Antimicrob Agents Chemother. 2011;55(4):1677–83.
Tan CC, Lee HS, Ti TY, Lee EJC. Pharmacokinetics of intravenous vancomycin in patients with end-stage renal failure. Ther Drug Monit. 1990;12:29–34.
Daptomycin. [package insert]. Lexington: Merck:Revised June 2011.
Welage LS, Mason NA, Hoffman EJ, Odeh RM, Dombrouski J, Patel JA, Swartz RD. Influence of cellulose triacetate hemodialyzers on vancomycin pharmacokinetics. J Am Soc Nephrol. 1995;6(4):1284–90.
Foote EF, Dreitlein WB, Steward CA, Kapoian T, Walker JA, Sherman RA. Pharmacokinetics of vancomycin when administered during high flux hemodialysis. Clin Nephrol. 1998;50(1):51–5.
Petejova N, Martinek A, Zahalkova J, Duricova J, Brozmanova H, Urbanek K, Grundmann M, Kacirova I. Vancomycin removal during low-flux and high-flux extended daily hemodialysis in critically ill septic patients. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012;156(4):342–7.
Economou CJP, Kielstein JT, Czock D, Xie J, Field J, Richards B, Tallott M, Visser A, Koenig C, Hafer C, Schmidt JJ, Lipman J, Roberts JA. Population pharmacokinetics of vancomycin in critically ill patients receiving prolonged intermittent renal replacement therapy. Int J Antimicrob Agents. 2018;52(2):151–7.
Lin SY, Shen LJ, Wu VC, Ko WJ, Wu CC, Wu FL. Pharmacokinetics and dosing of vancomycin in patients undergoing sustained low efficiency daily diafiltration (SLEDD-f): A prospective study. J Formos Med Assoc. 2021;120(1 Pt 3):737–43.
Kanji S, Roberts JA, Xie J, Zelenitsky S, Hiremath S, Zhang G, Watpool I, Porteous R, Patel R. Vancomycin population pharmacokinetics in critically Ill adults during sustained low-efficiency dialysis. Clin Pharmacokinet. 2020;59(3):327–34.
Joy MS, Matzke GR, Frye RF, Palevsky PM. Determinants of vancomycin clearance by continuous venovenous hemofiltration and continuous venovenous hemodialysis. Am J Kidney Dis. 1998;31(6):1019–27.
Chaijamorn W, Jitsurong A, Wiwattanawongsa K, Wanakamanee U, Dandecha P. Vancomycin clearance during continuous venovenous haemofiltration in critically ill patients. Int J Antimicrob Agents. 2011;38(2):152–6.
DelDot ME, Lipman J, Tett SE. Vancomycin pharmacokinetics in critically ill patients receiving continuous venovenous haemodiafiltration. Br J Clin Pharmacol. 2004;58(3):259–68.
Vilay AM, Grio M, Depestel DD, Sowinski KM, Gao L, Heung M, Salama NN, Mueller BA. Daptomycin pharmacokinetics in critically ill patients receiving continuous venovenous hemodialysis. Crit Care Med. 2011;39(1):19–25.
Corti N, Rudiger A, Chiesa A, Marti I, Jetter A, Rentsch K, Müller D, Béchir M, Maggiorini M. Pharmacokinetics of daily daptomycin in critically ill patients undergoing continuous renal replacement therapy. Chemotherapy. 2013;59(2):143–51.
Wenisch JM, Meyer B, Fuhrmann V, Saria K, Zuba C, Dittrich P, Thalhammer F. Multiple-dose pharmacokinetics of daptomycin during continuous venovenous haemodiafiltration. J Antimicrob Chemother. 2012;67(4):977–83.
Rybak MJ, Le J, Lodise TP, Levine DP, Bradley JS, Liu C, Mueller BA, Pai MP, Wong-Beringer A, Rotschafer JC, Rodvold KA, Maples HD, Lomaestro BM. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 2020;77(11):835–64.
Louie A, Kaw P, Liu W, et al. Pharmacodynamics of daptomycin in amurine thighmodel of Staphylococcus au reus infection. Antimicrob Agents Chemother. 2001;45:845–51.
Sader Safdar N, Andes D, Craig WA. In vivo pharmacodynamic activity of daptomycin. Antimicrob Agents Chemother. 2004;48:63–8.
Chaves RL, Chakraborty A, Benziger D, et al. Clinical and pharmacokinetic considerations for the use of daptomycin in patients with Staphylococcus aureus bacteraemia and severe renal impairment. J Antimicrob Chemother. 2014;69:200–10.
Fowler VG Jr, Boucher HW, Corey GR, et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N Engl J Med. 2006;355:653–65.
Benvenuto M, Benziger DP, Yankelev S, Vigliani G. Pharmacokinetics and tolerability of daptomycin at doses up to 12 milligrams per kilogram of body weight once daily in healthy volunteers. Antimicrob Agents Chemother. 2006;50(10):3245–9.
Lewis SJ, Mueller BA. Evaluation and development of vancomycin dosing schemes to meet new AUC/MIC targets in intermittent hemodialysis using Monte Carlo simulation techniques. J Clin Pharmacol. 2021;61(2):211–23.
Acknowledgements
Not applicable.
Funding
This work was supported by NxStage/Fresenius Medical Care AG & Co.
Author information
Authors and Affiliations
Contributions
Drs. Lewis, Jang, and Mueller have contributed to the conception or design of the work, the execution, analysis and interpretation for the work and writing and revising the manuscript; approved the final version; and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. The study protocol was approved by the University of Findlay Institutional Review Board and was deemed exempt from a full review. This study used the internal aggregated data for a mean body weight from Fresenius outpatient dialysis center (ie. not open access data) and published data from the literature. Since this study did not involve human subjects, the University of Findlay Institutional Review Board waived the need for informed consent.
Consent for publication
Not applicable.
Competing interests
Dr. Mueller received grant funding from NxStage/Fresenius Medical Care AG & Co. to support this study. All other authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1
Predicted AUC24h interquartile range of daptomycin dosing regimens in patients receiving 3-hour home hemodialysis. Table 2 Predicted AUC24h interquartile range of daptomycin dosing regimens in patients receiving 7-hour home hemodialysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lewis, S.J., Jang, S.M. & Mueller, B.A. Vancomycin and daptomycin dosing recommendations in patients receiving home hemodialysis using Monte Carlo simulation. BMC Nephrol 24, 270 (2023). https://doi.org/10.1186/s12882-023-03314-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-023-03314-y