
Abstract
Background
The ethmoid sinus (ES) is a three-dimensional (3D) complex structure, a clear understanding of the ES anatomy is helpful to plan intranasal surgery. However, most prior studies use 2D measurements, which may not accurately depict the 3D structure. The current study measured the gender differences in ES morphology based on 3D reconstruction of computed tomography (CT) images.
Methods
The 3D models were reconstructed using CT images. Twenty-one males and 15 females were enrolled in the study. The ES dimensions, including width, height and aspect ratio (AR) of each cutting-plane section, were measured at 10% increments along with the anteroposterior axis of the ES. The gender differences in the above parameters were further evaluated by an independent t-test.
Results
The width of the ES for males is 12.0 ± 2.1 mm, which was significantly greater than that in females (10.0 ± 2.1 mm). The average height for males is 18.4 ± 3.5 mm, and 18.2 ± 3.4 mm for females. The AR of female (male) is around 0.56 (0.63) for the anterior ES and 0.66 (0.75) for the posterior. There are significant differences between genders in the parameters of width and AR (p < 0.05).
Conclusion
This study found that the aspect ratio greatly varies along the length of ES, indicating that the cross-section of the ES in the anterior is closer to an elliptical shape and turns closer to a circular shape near its posterior. There is a significant difference between genders in width and aspect ratio. The results would be helpful to know the complex anatomic details of the ethmoid sinus.
Similar content being viewed by others


Introduction
The paranasal sinuses are an anatomically complex, interconnected system with air pockets that are connected to the nasal passages by cavities. The morphology of the nasal sinus varies significantly and is influenced by genetic diseases, infectious diseases, or environmental conditions [1,2,3,4,5]. Modern medical imaging technology allows the detection of sinus lesions, which improves the accuracy of measurement and allows appropriate planning for intranasal surgery [6,7,8,9,10].
The ethmoid sinus (ES) is a part of the paranasal sinuses and is located between the nose and eyes, and its boundaries include lamina papyracea of the orbit (lateral), middle and superior turbinates (medial) fovea ethmoidalis (superior), and superior border of inferior meatus (inferior) [11]. Furthermore, the ES is a common site for functional endoscopic sinus surgery [12,13,14]. The size and appearance of ES are important indicators of preoperative planning before surgery. Many morphometrical studies used 2D plane image technology to depict the 3D ES anatomy [15,16,17,18,19,20,21]. Those results varies study to study. The average length of the ES ranged from 21.3 ± 5.0 to 41.5 ± 3.8 mm, and the width ranged from 10.3 ± 3.0 to 17.3 ± 3.5 mm [16, 20, 21]. The possible reason results in the bias can be owing to the methods of CT scan and images post-processing, such as the positioning or orientation of the patients’ head when taking CT images [22, 23]. Measurement errors happen especially in the situations like head tilting during scanning or slice is non-orthogonal with sinus (Fig. 1A).

Methodology of the 3D model reconstruction and measurement process
Moreover, traditional 2D image measures of the ES through X-rays and CT cannot have stereo observation on the complex anatomic structure of ES tunnels, but 3D model benefits in obtaining better visualization than 2D measures [24,25,26]. Besides, 3D model can be easily rotated and reoriented by changing the rotational axis or redefined the coordinate system through 3D reconstruction modeling technique, which have been used in the complex human skeletal structures [27,28,29,30,31].
Some morphological studies have reported racial and gender differences in sinus [15, 16, 20, 32]. One recent study showed that Chinese ES was about 16% wider than Caucasians. This study also reported that the ES width of Chinese was 13% higher in males than in females [20], but the opposite is true for Africans [15]. These studies showed that the anatomy of the sinus was affected by factors such as race, gender or the measurement method. Most of the data for previous studies was collected using 2D CT images. Although other studies used 3D measure strategies but they only calculated the volume [26, 32] or just used to classify the shape classifications [25, 33]. Three-dimensional data for the ES structure has yet to be collected.
Thus, current study attempted to measure the 3D structure of the ES by using a CT image reconstruction model. This model reconstruction and measurement method has been approved in the research team’s prior study when measuring the lower extremity of the human body [34]. The outline at each cutting-plane section of the ES was measured to determine the entire structure of the ES. The ES geometry for male and female subjects was also compared to determine the differences between genders in Asian populations. It is hypothesized that the ES of male subjects is significantly larger than that of females.
Materials and methods
This study included subjects from patients with nasolacrimal duct stenosis for dacryocystorhinostomy, pituitary or skull base tumors who underwent surgery, and those who complained of olfactory dysfunction but demonstrated normal sinonasal findings on their computed tomography scans. Patients with previous sinonasal surgery for anatomical or inflammatory conditions, head and neck cancer received radiotherapy, trauma, orthognathic surgery, or congenital sinonasal disorders were excluded from the enrollment. A total of 36 subjects (21 males and 15 females) were included in the study which was approved by the Institutional Review Board (201912187RINA). The average age of the subjects is 55.4 years (21 ~ 99): a mean of 52.0 years old for males and 59.2 for females. All subjects had intact sinuses on both sides so a total of 72 sinus data points (42 male and 30 female data) were analyzed.
Study design
The measurement process and study design for this study is shown in Fig. 1. CT scans were performed using a multi-slice CT machine (Sensation 16 SLICE, SIEMENS, Memphis, USA) with a 1 mm slice thickness (120 kV, 20 mA). Image segmentation and reconstruction used OOOPDS (Main Orthopedic Biotechnology Co., Ltd., Taichung City, Taiwan). The image was first correctly oriented using the criteria for the Frankfurt plane [35]. The ethmoid sinus (ES) level and the coordinates were then defined (Fig. 1A). The sinus cavity region is used to define the appearance of the sinus. The sphenoid sinus (SS), frontal sinus (FS), maxillary sinus (MS) and nasal cavity were segmented together with the ethmoid sinus, which are located at the specified level and coordinates and are in close proximity (Fig. 1B). The sinus cavity is reconstructed as a 3D model, and a boundary surface is defined by the standard anatomy of the ES (Fig. 1C-E). This study focuses on the standard anatomical narrative of the ES area [11, 36]. The ES model then removed the area outside the boundary surface and constructs cutting plane increments of 10% in the anterior–posterior (AP) direction for the remaining ES models (Fig. 1F). The cutting plane and the overlapping position of the ES model is the section contour of the ES. The total length of the ES and the width and height of each section were measured and the differences between genders were further determined (Fig. 1F).
Definition of the coordinate system and the correct orientation of the images
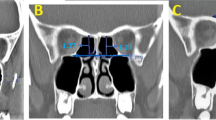
Different image orientations produce errors in measurement so the coordinate system is defined initially. The coordinate definition uses the Frankfurt plane [35]. The cranial base in the sagittal view is used as the horizontal basis to correct the Y-axis rotation of the model (Fig. 2A). The Z-axis rotation is corrected using the nasal septum in the axial view as the vertical basis (Fig. 2B). The X-axis rotation of the model is then corrected using the cranial base and the nasal septum in the coronal view as the vertical and horizontal basis (Fig. 2C).

Coordinate definition and correction of image orientation: A sagittal view, B axial view and C coronal view
Defining and constructing ES model and boundaries
The sphenoid, frontal, maxillary, ES and nasal cavities are segmented and reconstructed for this study (Fig. 1B and C). The correctness of the image segmentation was confirmed by two ENT surgeons who are co-authors of this study (Lin CF and Yang CC). The boundaries of the ES were defined based on standard anatomical descriptions (Fig. 1D) [11, 36]. The upper boundary is defined as the cranial base, the outer boundary is periorbital and the inner boundary is middle turbinate. The boundary of each section is reconstructed as a boundary surface of the 3D model (Fig. 1E). The irrelevant area beyond the boundary surface is removed, so the remaining area of ES is the target for subsequent measurements (Fig. 1F). All cavities of the sinuses are reconstructed as 3D models and the correctness of the division was verified by two coauthors to minimize the error in boundary definition.
Measurement of the ethmoid sinus
Reverse engineering software RevCAD V1.50 (PouYuen Tech Corp., Taoyuan, Taiwan) was used to create cutting planes (Fig. 1F). In order to analyze the complex anatomical appearance of ES objectively, the total length of the ES is used as a benchmark and the starting plane is through the frontmost point of the ES and perpendicular to the Y axis. Cutting planes are established at every 10% increment of the total length. The vertical distance between the 0% and 100% cutting planes is defined as the ES length (L) (Fig. 1F).
The intersection of the cutting planes and ES are defined as cutting points. The closed curve is calculated using a B-spline curve fitting algorithm with the cutting points (Fig. 1G) [37]. The distance from maximum Zi to minimum Zi for the closed curve is the height (Hi) of this ES section (Fig. 1H), where i = 0%, 10%, 20%,…, and 100%. The distance from maximum Yi to minimum Yi for the closed curve is the width (Wi) of the ES section (Fig. 1H). For this study, the aspect ratio (AR) of width to height for each ES section is defined as ARi = Wi/Hi, ARi and is used to determine the change in shape for each section of the chamber, which clearly defines the anatomy.
Statistical analysis
To ensure that the data is normally distributed, the Kolmogorov–Smirnov test was used and proven for p > 0.05 in parametric statistics. G-power 3.1 was used for a post hoc power analysis of gender differences, with α = 0.05, and the calculated statistical power is 97%. Statistical data is analyzed using SPSS (version 20, SPSS Inc., Chicago, IL, USA) and independent t-tests are used to determine the significance of gender differences. A value of p < 0.05 indicates statistical significance.
Results
The average ES length for the male group is 40.1 ± 5.0 mm and for the female group is 41.3 ± 5.0 mm. There is no significant difference between genders (p = 0.140) (Table 1). As for the average width and height of the ES for males and females in each section (Fig. 3). The maximum width of the male ES is W60 = 12.0 ± 2.1 mm and the maximum width of the female ES is W80 = 10.0 ± 2.1 mm. The male ES is significantly wider than the female ES. Except for W10 (p = 0.064), there is a statistically significant difference in most of the sections (p < 0.05). The male and female ES has a maximum height at H40 (18.4 ± 3.5 mm and 18.2 ± 3.4 mm). The maximum height for the male group is slightly greater than that for the female group for all ES heights, but the only significant difference is at H60 (p = 0.045) and H80 (p = 0.048).

Average width and height of the ES for males and females in each section: A width and B height
The largest and smallest aspect ratio (AR) values for the male group are AR90 = 0.9 ± 0.5 and AR20 = 0.6 ± 0.2, respectively (Fig. 4A), and for the female group, these values are AR90 = 0.8 ± 0.2 and AR30 = 0.5 ± 0.1, respectively. The AR values for the male group are larger than those for the female group. There is a significant difference from AR40 to AR70 but the AR value for the anterior section (AR10- AR50) for the male group is 19.4% smaller on average than that for the posterior section (AR50- AR90). The anterior section for the female group is 18.3% smaller on average than the AR value for the posterior section. There are significant differences between AR10 vs. AR90, AR20 vs. AR80, AR30 vs. AR70, and AR40 vs. AR60. The AR for the left ES is slightly greater than the value for the right side (Fig. 4B) but there is no significant difference (p = 0.26).

Average aspect ratio of the ES in different sections: A for gender difference and B for symmetry difference
The AR of the cross-section is about 0.6 for the anterior sections, so the cross-section of the ES in the anterior sections is close to an elliptical cylinder (Fig. 5A). However, the AR values for the cross-section in the posterior part are about 0.7–0.9, so the cross-sections in the posterior parts is almost circular.

Diagram showing the shape of the ES in the anterior and posterior sections (A) the AR of the ES in the anterior and posterior sections (B) reconstructing ES model according section curve
Discussion
The ethmoid sinus is the most anatomically complex part of the paranasal sinuses. It is created by the ethmoid bone, forming multiple pyramidal air cells. For this study, the 3D model is reconstructed to measure the detail of the ES section. This study allows a more accurate description of the anatomy of the ES than the 2D measurements. Most studies use 2D or planar images to measure the length of ES [15,16,17,18,19,20,21]. Those studies use one image that is the uppermost edge of the optical canal in several axial-view images and measure the length of ES using this image. However, the orientation of the 2D image is affected by the subject’s posture during the CT scan (Fig. 2). In standard scanning process, subjects used a head fixation device when taking CT images. However, the average orientation difference between the original CT and the corrected model is 9.1° ± 10.6, 1.8° ± 2.4 and 2.1° ± 2.7 in the sagittal, axial and coronal plane (Fig. 6). Especially in the sagittal plane, the orientation difference is 3.3 times and 4.2 times than the axial and coronal plane, respectively.

The average orientation difference between the original CT and the corrected model
Two-dimensional (2D) imaging has notable limitations in medical contexts, particularly in assessing complex sinus anatomy. A primary issue is the flat representation, which lacks depth and fails to accurately depict spatial relationships between anatomical structures. Additionally, overlapping structures in 2D images make it challenging to distinguish boundaries and relationships, obscuring crucial details necessary for precise surgical planning. Measurement errors are another concern with 2D imaging. The accuracy of measurements can be compromised by the angle at which images are taken, resulting in inaccurate dimensions and shapes of anatomical structures. Without depth perception, it is difficult to understand the true extent and position of abnormalities such as polyps or tumors. Besides, 2D images are typically analyzed in a single plane (axial, coronal, or sagittal), restricting the ability to understand complex anatomy that exists across multiple planes simultaneously.
Regarding three-dimensional (3D) imaging, it offers significant advantages for medical applications, especially in understanding complex sinus anatomy. A true 3D representation provides an accurate depiction of spatial relationships and structure depth, crucial for navigating intricate anatomical regions during surgery. With clear visualization from any angle, the risk of missing critical details is reduced. Surgeons can also simulate surgeries, practice procedures, and devise effective approaches using 3D models, leading to better outcomes and shorter operative times. These models allow for personalized surgical plans tailored to each patient’s unique anatomy, improving precision and safety. 3D measurements are consistent and precise, unaffected by imaging angles, reducing the risk of errors related to anatomical misinterpretations. Detailed volume assessments of anatomical structures and pathological lesions are possible, aiding in disease extent evaluation and intervention planning.
While 2D measurements provide useful information, they fall short in accurately representing the complex and three-dimensional nature of sinus anatomy. 3D measurements and reconstructions offer a more comprehensive and precise understanding, significantly enhancing preoperative planning, surgical precision, and patient outcomes. The shift from 2 to 3D imaging represents a major advancement in medical imaging, particularly in fields requiring intricate anatomical navigation such as sinus surgery. Researches have shown that keeping consistently positioning and orientation of the patient’s head when taking CT images is a great challenge [22, 23]. It’s should be noted that the CT images are not definitely orthogonal to the standard landmarks (Frankfurt plane) of the ES structure. Accuracy ES dimension obtained from 2D image must be reoriented to ensure the measurement are done under the same coordinates. However, the reorientation for plane images is a complex process, and it is difficult to complete the reorientation process in traditional 2D image researches [15,16,17,18,19,20,21]. This study redefined the coordinate system based on the Frankfurt plane [35] and this process eliminated the possible deviations when measuring the dimensions of complex structures. Therefore, the current study can provide more relatively reasonable results and better visualization of the ethmoid sinus compared to previous studies [15,16,17,18].
The height of ES is an important measure. A complete sinus model was used in this study, so the anatomical location and identification of the ES region is clearer. The height of each section of the ES and the width of the ES were measured continuously at every 10% interval of the ES length (Figs. 1H and 4). The results showed that the average height of the ES for a Chinese male was 13.7 ± 6.6 mm and for a Chinese female is 13.0 ± 6.2 mm. No significant difference in the height of the ES was found for male and female groups (p > 0.05) but there is a statistically significant difference in width. The average width of the ES for a Chinese male was 9.1 ± 4.1 mm and for a Chinese female was 7.8 ± 3.4 mm. The male ES is about 20.0% larger than that of the female.
The difference between the measurement results for this study and those of other studies, in terms of length, width and height are about -47%‒3%, -14%‒78% and 12%‒64%, respectively (Table 1). The results show that there is some discrepancy between the results of this study and those of other literature, possibly due to differences in 3D and 2D measurement methods, measure locations, or ethnic differences.
The reconstruction and measurement methods in this study have been recognized in previous studies by measuring the morphology of the femoral condyle [34]. This is the first study to measure the dimensions and aspect ratio of a detailed ES structure using a 3D reconstruction model and a cutting plane method. The shape of an ES section is defined using the aspect ratio of the width to the height of the ES. If AR = 1, the shape is a circle and if AR < 1, it is closer to an ellipse. The results of this study showed that the average shape of ES is closer to an ellipse, especially for the anterior ES (AR10-AR50), for which the AR value is about 0.60, and the posterior ES (AR50-AR90), for which the AR value is about 0.74 (Fig. 5A). The aspect ratio for the end of the ES (AR80-AR90) is about 0.9, so posterior ES is approximately like a circle in the final section. As for the AR value in male ES is significantly greater than that for a female, particularly in the range of AR40- AR70.
A large number of Asians suffer from chronic sinusitis [38, 39] and may require stents to prevent restenosis after ES surgery [40,41,42]. Determining the 3D structure of an ES cavity allows more accurate planning for nasal surgery. The current ES stent has a circular section after it is deployed [40], but the anterior part should be elliptical and the posterior part should be almost circular. So, it does not fit the cavity shape. Our previous biomechanics study [43] analyzed the contact behavior of a nasal stent that was deployed to the ES cavity and showed that there was a significant rise of contact stress on the inside of the ES and a part of the stent material has caused permanent plastic deformation possibly due to mismatch between the stent and nasal cavity. If the shape of the implant deviates too much from the shape of the ES, excessive stress can occur and the ES can become loose [43]. The design of a commercial stent should ensure optimal stent-ES contact in the ES cavity. The section curve and the aspect ratio of the ES can provide helpful information for the improvement of the nasal device (Fig. 5B).
This study has some limitations should be mentioned here. First, the subject number is not big enough. The current study primarily developed a new measurement method to obtain 3D results in this stage and we will keep enrolling more data in the near future. Second, in order to obtain the most typical measurement data, this study only included normal anatomy cases. However, the morphology of ES may differ from the typical one after FESS. Third, the standard anatomy of the ES defined the upper (cranial base), outer (periorbital), and inner boundary (middle turbinate), but not inferior boundary [11, 36]. Therefore, this study defined the inferior boundary by the lowest point of section curve (Fig. 1G). Finally, there are multiple ways to demarcate and measure the morphology but it is difficult to define the boundaries of these complex air sacs. In addition to the limitations mentioned above, the current study has put new information to know the continuous change of the ES.
Conclusion
This three-dimensional morphological analysis showed that the sinus cavity was constantly changing from anterior to posterior. The ethmoid sinuses are significantly wider in males than in females. Aspect ratio analysis showed that the ethmoid sinus near the anterior part was closer to the oval, but the shape of the posterior part resembled a circle. The aspect ratio of the middle part of the ethmoid sinus is significantly greater in males than in females.
Availability of data and materials
Data availability The datasets generated and/or analyzed during the current study are not publicly available due to the nature of this study, but are available from the corresponding author on reasonable request.
References
Karatas D, Koç A, Yüksel F, Dogan M, Bayram A, Cihan MC. The effect of nasal septal deviation on frontal and maxillary sinus volumes and development of sinusitis. J Craniofac Surg. 2015;26(5):1508–12.
Natsis K, Karabatakis V, Tsikaras P, Chatzibalis T, Stangos A, Stangos N. Frontal sinus anatomical variations with potential consequences for the orbit. Study on cadavers. Morphologie. 2004;88(280):35–8.
Jang YJ, Park HM, Kim HG. The radiographic incidence of bony defects in the lateral lamella of the cribriform plate. Clin Otolaryngol Allied Sci. 1999;24(5):440–2.
Lorkiewicz-Muszyńska D, Kociemba W, Rewekant A, Sroka A, Jończyk-Potoczna K, Patelska-Banaszewska M, Przystańska A. Development of the maxillary sinus from birth to age 18. Postnatal growth pattern. Int J Pediatr Otorhinolaryngol. 2015;79(9):1393–400.
Degermenci M, Ertekin T, Ülger H, Acer N, Coskun A. The age-related development of maxillary sinus in children. J Craniofac Surg. 2016;27(1):e38–44.
Vaid S, Vaid N. Normal anatomy and anatomic variants of the paranasal sinuses on computed tomography. Neuroimaging Clin N Am. 2015;25(4):527–48.
Tingelhoff K, Moral AI, Kunkel ME, Rilk M, Wagner I, Eichhorn KWG, Wahl FM, Bootz F. Comparison between manual and semi-automatic segmentation of nasal cavity and paranasal sinuses from CT images. Conf Proc IEEE Eng Med Biol Soc. 2007;2007:5505–8.
Olson G, Citardi MJ. Image-guided functional endoscopic sinus surgery. Otolaryng Head Neck. 2000;123(3):188–94.
Hoang JK, Eastwood JD, Tebbit CL, Glastonbury CM. Multiplanar sinus CT: a systematic approach to imaging before functional endoscopic sinus surgery. Am J Roentgenol. 2010;194(6):W527–36.
Nikkerdar N, Eivazi N, Lotfi M, Golshah A. Agreement between cone-beam computed tomography and functional endoscopic sinus surgery for detection of pathologies and anatomical variations of the paranasal sinuses in chronic rhinosinusitis patients: a prospective study. Imaging Sci Dent. 2020;50(4):299.
Cappello ZJ, Minutello K, Dublin AB. Anatomy, head and neck, nose paranasal sinuses. In: StatPearls. Treasure Island: StatPearls Publishing; 2023.
Welch KC, Stankiewicz JA. A contemporary review of endoscopic sinus surgery: techniques, tools, and outcomes. Laryngoscope. 2009;119(11):2258–68.
Cashman EC, MacMahon PJ, Smyth D. Computed tomography scans of paranasal sinuses before functional endoscopic sinus surgery. World J Radiol. 2011;3(8):199.
Abdullah B, Lim EH, Husain S, Snidvongs K, Wang DY. Anatomical variations of anterior ethmoidal artery and their significance in endoscopic sinus surgery: a systematic review. Surg Radiol Anat. 2019;41:491–9.
Oghenero G, Oniovo K, Olotu B, Sagbodje D. Morphology and anatomical variations of ethmoidal sinus in adult Nigerians. Afr J Med Surg. 2017;4:095–100.
Ameye SA, Amusa YB, Eziyi JAE, Famurewa OC. Assessing the surgical anatomy of the ethmoid sinus in adult Nigerians using computerized tomography scan. Int J Med Med Sci. 2014;6(12):239–44.
Cankal F, Apaydin N, Acar HI, Elhan A, Tekdemir I, Yurdakul M, Kaya M, Esmer AF. Evaluation of the anterior and posterior ethmoidal canal by computed tomography. Clin Radiol. 2004;59(11):1034–40.
Bonfils P, Avan P, Palimi P, Malinvaud D. Evaluation of mucosal surface reduction after ethmoidal surgery in nasal polyposis. J Laryngol Otol. 2007;121(7):1–4.
Liu J, Liu Q, Wang N. Posterior ethmoid cell expansion towards the inferolateral region of the sphenoid sinus: a computed tomography study. Surg Radiol Anat. 2019;41:1011–8.
Chan MA, Ibrahim F, Kumaran A, Yong K, Chan ASY, Shen S. Ethnic variation in medial orbital wall anatomy and its implications for decompression surgery. BMC Ophthalmol. 2021;21:290.
Abdalla MA, Hussien RZ. CT Scans imaging of human ethmoid sinuses and gross anatomical dissection: a descriptive, projective, comparative, and dimensional study. Mod Med. 2022;29(3):213–26.
Yoo SK, Kim YO, Kim HJ, Kim NH, Jang YB, Kim KD, Lee HY. Alignment of CT images of skull dysmorphology using anatomy-based perpendicular axes. Phys Med Biol. 2023;48(16):2681.
Mangal U, Lee SM, Lee S, Cha JY, Lee KJ, Yu HS, Jung H, Choi SH. Reorientation methodology for reproducible head posture in serial cone beam computed tomography images. Sci Rep. 2023;13(1):3220.
Park SH, Yu HS, Kim KD, Lee KJ, Baik HS. A proposal for a new analysis of craniofacial morphology by 3-dimensional computed tomography. Am J Orthod Dentofacial Orthop. 2006;129(5):600-e23.
Li Y, Xu C, Yu D, Xiong T, Zhao H, Xue H, Liang WB, Deng ZH, Zhang L. Computer-aided superimposition of the frontal sinus via 3D reconstruction for comparative forensic identification. Int J Legal Med. 2021;135(5):1993–2001.
Zhao H, Li Y, Xue H, Deng ZH, Liang WB, Zhang L. Morphological analysis of three-dimensionally reconstructed frontal sinuses from Chinese Han population using computed tomography. Int J Legal Med. 2021;135:1015–23.
Yang G, Dai Y, Dong C, Niu Y, Kang H, Wang F. Two-type classification system for femoral trochlear dysplasia in recurrent patellar instability based on three-dimensional morphology. Knee Surg Sports Traumatol Arthrosc. 2023;31(5):1790–7.
Phombut C, Rooppakhun S, Sindhupakorn B. Morphometric analysis and three-dimensional computed tomography reconstruction of Thai distal femur. Appl Sci. 2021;11(3):1052.
Koh YG, Nam JH, Chung HS, Kim HJ, Baek C, Kang KT. Gender difference exists in sagittal curvature of the distal femoral condyle morphology for osteoarthritic population. Knee Surg Sports Traumatol Arthrosc. 2020;28:3740–6.
Zhang RY, Su XY, Zhao JX, Li JT, Zhang LC, Tang PF. Three-dimensional morphological analysis of the femoral neck torsion angle—an anatomical study. J Orthop Surg Res. 2020;15(1):1–8.
Cheng H, Liu L, Yu W, Zhang H, Luo D, Zheng G. Comparison of 2.5 D and 3D quantification of femoral head coverage in normal control subjects and patients with hip dysplasia. PLoS ONE. 2015;10(11):e0143498.
Wanzeler AMV, Alves-Júnior SM, Ayres L, da Costa Prestes MC, Gomes JT, Tuji FM. Sex estimation using paranasal sinus discriminant analysis: a new approach via cone beam computerized tomography volume analysis. Int J Legal Med. 2019;133:1977–84.
Pirinc B, Fazliogullari Z, Guler I, Unver Dogan N, Uysal II, Karabulut AK. Classification and volumetric study of the sphenoid sinus on MDCT images. Eur Arch Otorhinolaryngol. 2019;276:2887–94.
Hsu CP, Lee PY, Wei HW, Lin SC, Lu YC, Lin JC, Huang CH. Gender differences in femoral trochlea morphology. Knee Surg Sports Traumatol Arthrosc. 2021;29:563–72.
Cheng Y, Leow WK, Lim TC. Automatic identification of Frankfurt plane and mid-sagittal plane of skull. In: 2012 IEEE Workshop on the Applications of Computer Vision (WACV). 2012. p. 233-238.
Gendeh HS, Gendeh BS. Paranasal sinuses anatomy and anatomical variations. In: Gendeh BS, editor. Paranasal Sinuses Anatomy and Conditions. Chapter 4. London: Intechopen; 2022. p. 49–76.
Ma W, Kruth JP. NURBS curve and surface fitting for reverse engineering. Int J Adv Manuf Technol. 1998;14:918–27.
Shi JB, Fu QL, Zhang H, Cheng L, Wang YJ, Zhu DD, Lv W, Liu SX, Li PZ, Ou CQ, et al. Epidemiology of chronic rhinosinusitis: results froma cross-sectional survey in seven Chinese cities. Allergy. 2015;70:533–9.
Wang XD, Zheng M, Lou HF, Wang CS, Zhang Y, Bo MY, Ge SQ, Zhang N, Zhang L, Bachert C. An increased prevalence of self-reportedallergic rhinitis in major Chinese cities from 2005 to 2011. Allergy. 2016;71:1170–80.
Schilling AL, Cannon E, Lee SE, Wang EW, Little SR. Advances in controlled drug delivery to the sinonasal mucosa. Biomater. 2022;282:121430.
Huang Z, Zhou B, Wang D, Zang H, Zhang H, Wang H, Wang S, Cheng L, Li J, Wu W, et al. Comparison of bioabsorbable steroid-eluting sinus stents versus nasopore after endoscopic sinus surgery: a multicenter, randomized, controlled, single-blinded clinical trial. Ear Nose Throat J. 2022;101(4):260–7.
Lim DJ, Cho DY. The next generation of sinus stents for chronic rhinosinusitis: a systematic review. Precis Futur Med. 2023;6(3):161–9.
Lu YC, Hsu LI, Lin CF, Hsu CP, Chang TK, Cheng CC, Huang CH. Biomechanical characteristics of self-expanding sinus stents during crimping and deployment_A comparison between different biomaterials. J Mech Behav Biomed Mater. 2023;138:105669.
Acknowledgements
We are also grateful to the National Science and Technology Council (NSTC 109-2221-E-195-001-MY2 and 111-2221-E-195-003-MY3) for providing financial support for our research. Their generous funding allowed us to conduct our study and complete our work.
Funding
This project was supported by cooperative research from National Science and Technology Council (NSTC 109-2221-E-195-001-MY2 and 111-2221-E-195-003-MY3). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the donor.
Author information
Authors and Affiliations
Contributions
Chi-Pin Hsu: Conceived the study design, helped to draft the manuscript and supervised the study, analyzed and interpreted the data. Chih-Feng Lin: Acquired the data, analyzed and interpreted the data, drafted the manuscript. Chih-Chi Yang: Acquired, analyzed and interpreted the data. Jeng-Ywan Jeng: Helped to draft the manuscript and supervised the study. Chang-Hung Huang: Conceived the study design, helped to interpreted the data, draft the manuscript and supervised the study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is approved by the Institutional Review Board of National Taiwan University Hospital (IRB number: 201912187RINA). Because of the retrospective nature of the study, the requirement for informed consent was waived. The study was performed in accordance with the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hsu, CP., Lin, CF., Yang, CC. et al. Gender differences in ethmoid sinus morphology_ 3D reconstruction of computed tomographic images. BMC Med Imaging 24, 139 (2024). https://doi.org/10.1186/s12880-024-01319-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-024-01319-z