
Abstract
Introduction
Maintaining the pituitary function after surgery is highly important. The aim of this study was to investigate the relationship between preoperative magnetic resonance imaging (MRI) characteristics and pituitary function after surgery of non-functional pituitary macroadenoma.
Methods
This retrospective study was performed between 2016 and 2018. Preoperative and postoperative MRI imaging data were retrieved from electronic registration system. The relationship between preoperative MRI characteristics and postoperative pituitary function as well as reconstruction of pituitary gland was investigated using regression models.
Results
Complete data were available for 44 patients. Before surgery, invisible normal tissue was observed in 23 patients (53.5%). Suprasellar extension and cavernous sinus invasion were seen in 36 patients (each one 49.1%). There was a significant reverse relationship between preoperative tumor size and postoperative thyroid stimulating hormone (TSH) (odds ratio (OR): − 0.99 (− 0.18, − 0.003), p = 0.04). In addition, we found a significant positive correlation between prolactin level after surgery and tumor size before surgery, (OR: 5.29 (1.65, 8.92), p = 0006). Moreover, postoperative panhypopituitarism was observed in 25% of patients with complete morphologic reconstitution of pituitary tissue. While the rate was 50% in patients with no or partial morphologic reconstruction of pituitary tissue.
Conclusion
Preoperative MRI characteristics predict TSH and prolactin level after operation. Furthermore, the adenoma size and volume prior to surgery are the main determinants of normal morphologic reconstruction of pituitary gland.
Similar content being viewed by others

Introduction
Non-functional pituitary macroadenomas (more than one centimeter in diameter) comprise about one-third of all pituitary adenomas and are managed with trans sphenoidal surgery [1, 2]. Restoration of normal pituitary function after surgery is important and has been reported in various studies from 20 to 50% [3, 4]. Panhypopituitarism, deficiency in production of at least two pituitary hormones, is a most common complication after pituitary surgery [5]. Inadequate secretion of luteinizing hormone (LH) and follicle stimulating hormone (FSH), growth hormone (GH), thyroid stimulating hormone (TSH) and adrenocorticotropic hormone (ACTH) were observed after pituitary surgery in 99%, 98.6%, 96% and 81.8% of cases after pituitary surgery [6, 7]. Methods for predicting the possible occurrence of these complications have also been studied. Various studies have shown that some findings in magnetic resonance imaging (MRI) are associated with post-operative complications. Therefore, identification of these findings in patients' MRI can be helpful in prediction and, possibly, prevention of the related complications [8, 9]. Researches evaluated the post-operative MRI characteristics over one year after trans sphenoidal surgery of the non-functional pituitary macroadenomas. The results showed the residual of pituitary adenoma in 18% of patients at 3 months after surgery [10, 11]. On the other hand, since the pituitary gland plays an essential role in the control of other endocrine glands, maintaining the function of this gland after surgery is very important and determinating the amount of the normal pituitary tissue after surgery can be very helpful in predicting of the reversibility of pituitary function [12, 13]. Due to the fact that MRI is the method of choice for imaging pituitary tumors and evaluation of changes in the tumor after surgery, MRI before and after surgery is necessary for selection of proper treatment and appropriate postoperative management [12]. Therefore, the aim of this study was to investigate the relationship between pituitary function after trans sphenoidal surgery and MRI characteristics in non-functional pituitary macroadenoma.
Method
Study design and data collection
This study was a retrospective cohort study which included patients with non-functional pituitary macroadenoma registered at Iran Pituitary tumor registry (IPTR) between 2016 and 2018. The written informed consent was obtained from the participants and the study was approved by the Ethical Committee at Iran University of medical sciences. (Approval number: IR.IUMS.FMD.REC.1398.154).
Patients
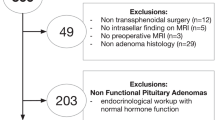
This study included patients with non-functional pituitary macroadenoma who underwent trans sphenoidal surgery. Inclusion criteria were all patients with biochemically and histologically confirmed non-functional pituitary macroadenoma with available MRI scan who had hormone profile before and after surgery. Patients with a history of radiotherapy as well as those with repeated pituitary surgery were excluded from the study.
Data collection
All demographic, clinical, and biochemical information were extracted from the electronic record system at the Institute of Endocrinology and Metabolism affiliated to Iran University of Medical Sciences. Hormone profile before surgery and at the last follow-up visit were used in this analysis.
The pre-operative MRI scan as well as the first post-operative MRI scan obtained during 3 months after surgery were also reviewed using the picture archiving and communication system (PACS). The required information about size, volume, consistency and direction of mass displacement were evaluated by two expert radiologists. Size was obtained by measuring the tallest tumor diameter in coronal view. Macroadenoma was defined as greatest tumor diameter greater than 10 mm.
Adenoma volume was calculated using the largest anterior-posterior, external and rostrocaudal radius dimensions. To measure the consistency of macroadenoma, the signal intensity of macroadenoma and that of pons were calculated with quantitative analysis of MRI signal intensity. Then, the consistency was estimated in each case by calculating the ratio of signal intensity of adenoma to pons according to cut point of 1.49 in previous studies; consistency of less than 1.49 was considered as firm and fibrous and more than 1.49 as soft tumors [13]. In this study we used Knosb grading method for assessment of cavernous sinus invasion. Normal gland locations were demonstrated against the pituitary adenoma according to degree of enhancement on preoperative dynamic MR images. After surgery, the normal gland differentiation from the residual enhancing lesion were diagnosed by analyzing the preoperative location and degree of enhancement on dynamic MR imaging and also the position of hypophysial stalk in some cases. Normal hypophysial tissue enhancement is more than adenoma in overall.
Statistical analysis
The continuous and discrete variables are described using number (percent) and median [interquartile range (IQR)], respectively. To measure the impact of the preoperative MRI findings (tumor size, tumor volume, apparent normal pituitary tissue, and cystic change) on the pituitary function after surgery (TSH, ACTH, LH, GH, and PRL), the univariate regressions models were fitted. Moreover, to assess the MRI characteristics of patients with preoperative pituitary macroadenoma as predictors of normal pituitary gland normal residual pituitary gland (NRPG) after surgery, the univariate logistic regression models were fitted and odds ratios (ORs) were reported. The analyses were performed using the statistical software Stata (ver. 12). The significance level was set to be 0.05.
Results
Data were available for 44 patients who met the inclusion criteria. Demographic and clinical characteristics of the participants at the time of diagnosis are demonstrated in Table 1.
Hypothyroidism was detected before and after surgery in 20% and 61.9% of patients, respectively. Hypercortisolism was diagnosed in 32.3% of patients before and in 48.8% after surgery. Hypogonadism was also observed in 74.2% of patients before and 54.8% of patients after surgery. Low insulin-like Growth Factor-1 (IGF-1) was observed in 22.6% and 12% of patients before and after surgery, respectively. Moreover, hyperprolactinemia was detected in 45% of patients before surgery and in 27.8% of patients after surgery (Fig. 1).

Bar chart of hormonal changes before and after surgery [Insulin-like growth factor-1 (IGF-1), Prolactin (PRL)]
Preoperative MRI characteristics and postoperative pituitary function
There was a significant, adverse relationship between preoperative tumor size and serum TSH level after surgery (odds ratio (OR): − 0.99 (− 0.18, − 0.003), p = 0.04). There was also a significant relationship between preoperative tumor size and postoperative prolactin level (OR: 5.29 (1.65, 8.92), p = 0.006). Moreover, a significant relationship was observed between preoperative tumor volume and postoperative prolactin level (OR: 0.006 (0.0008, 0.01), p = 0.02) (Table 2). There was no significant relationship between preoperative imaging characteristics and the amount of other pituitary hormones after surgery (p ≥ 0.05).
Preoperative MRI characteristics and postoperative morphologic reconstruction of pituitary gland
Morphologic Reconstruction pattern of pituitary gland after surgery was as followed: invisible normal pituitary tissue in 21.4% (9/42) of patients, complete normal pituitary tissue in 45.3% (19/42), and partial remnants of normal pituitary tissue in 33.3% (14/42) patients. There was a significant, adverse relationship between tumor size before surgery and normal morphologic reconstruction of pituitary gland after surgery (OR: 0.80 (0.68, 0.94), p = 0.007). There was also a significant, adverse relationship between tumor volume before surgery and NRPG after surgery (OR: 0.99 (0.99, 0.99), p = 0.007) (Table 3).
Pituitary function after surgery and NRPG in MRI scan
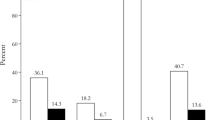
Among patients with no visible pituitary tissue (no morphologic reconstruction), normal pituitary function, partial hypopituitarism and pan hypopituitarism were observed in 16.7%, 33.3% and 50% of patients, respectively. In patients with partial morphologic reconstruction of pituitary tissue, these features were observed in 10% (1 patient), 40% (4 patients) and 50% (5 patients), respectively. The patients who had complete morphologic reconstruction of pituitary tissue experienced normal pituitary function (25%), partial hypopituitarism (50%) and panhypopituitarism (25%) (Fig. 2).

Ratio of patients with different pituitary functions according to the type of morphologic reconstruction of normal pituitary gland on MRI after surgery
Discussion
MRI is universally used in postoperative care pituitary adenomas, for the diagnosis of residual or recurrent tumors [11, 12]. This retrospective cohort study conducted among 44 patients who underwent TSS due to non-functional pituitary macroadenoma indicated post-operative TSH and prolactin levels are more likely to be associated with some MRI characteristics before surgery namely size and volume of the tumor. Moreover, size and volume of tumor in MRI images before trans sphenoidal surgery (TSS) showed an adverse association with the percentage of normal residual of pituitary gland. In the conducted study by Di Maio et al. in 2012, NRPG was identified in 79% of the patients on preoperative MRI [12]. Our research showed that NRPG was diagnosed in 21.4% of the patients on postoperative MRI, and there was a strong significant relationship between the size and volume of the tumor before surgery and NRPG. MRI with or without administration of gadolinium contrast agent also allows accurate assessment of the position and function of the tumor before and after surgery [12, 13]. But gadolinium uptake significantly improves diagnosis of the pituitary gland, especially in severe deformity cases of the pituitary gland. Improved diagnosis of the pituitary gland, after gadolinium uptake is due to the rapid and pronounced contrast of the pituitary gland, which is more than the adenoma [12].
In the study performed by Nomikos et al. in 2004, 721 patients with non-functional macroadenoma pituitary surgery were evaluated. 24.4% of patients had hypothyroidism after surgery, the prevalence of which was lower than our study (61.9%). Also in the Nomikos study, 1 year after surgery, preoperative prolactin levels were slightly increased in 25.3% (only 5 patients); increasing preoperative and postoperative prolactin was observed in 45% and 27.5% of patients in the present study, respectively; that was more that Nomikos study [14].
In 2015, Lee et al. conducted a study on 45 patients undergoing sphenoid surgery. In this study, hypogonadism was defined as total serum testosterone level < 4.2 ng/ml. Tumor volume was calculated based on MRI images before and after surgery. Examination of the MRI results showed that the need for long-term postoperative testosterone replacement was significantly associated with a larger volume of preoperative tumor and preoperative testosterone levels. Preoperative tumor volume and testosterone levels affect postoperative hypogonadism. By measuring tumor volume and testosterone levels, surgeons will be able to predict postoperative hypogonadism and the need for long-term hormone replacement [15].
In 2021, Ono et al. examined the clinical features and surgical outcomes of 79 patients with dysfunctional pituitary adenoma. Reduction of growth hormone levels was observed in 37.7% of patients. In our study, also a deficiency of postoperative IGF-1 was observed in 12% of patients, which indicated a lower prevalence of this disorder in the present study. Ono et al. also showed that, hypogonadism after surgery was developed in 19% of patients, but in our study, the prevalence of hypogonadism was 54.8% postoperatively, which was higher than the Ono et al. results. A deficiency of TSH was observed in 6.3% of patients in the Ono et al. results, deficiency of TSH was 61.9% in patients studied in our research, and this matter indicates the higher prevalence of this disorder in our study with compared with Ono et al. [16] results.
In other hand, one of the most common symptoms of dysfunctional pituitary macroadenomas is hypogonadism, which may require long-term hormone replacement. In addition, reducing the pressure on the normal pituitary gland may lead to postoperative recovery of the pituitary gland [15, 17].
The rate and type of changes in hormone’s level after surgery can be different because pituitary function and preservation of normal pituitary tissue after surgery depends on several factors such as tumor characteristic, the amount of pressure caused by the tumor on normal pituitary tissue, the type of surgery selected (for example, in patients undergoing cranial surgery, the incidence of this deterioration is significantly higher) and the age of patients [7, 13, 18, 19].
For example in study performed by Jahangiri et al. in 2016, patients with preoperative endocrine deficits (n = 153, 50%) were significantly older (mean age 60) and had larger adenomas. Postoperative endocrine deficits occurred in 42 (13.7%) patients (Thyroid axis 3%, cortisol axis 6%, and GH/IGF-1 axis 4%). In our study, decreased cortisol was observed in 32.3% and 48.8% of patients before and after surgery, respectively and a deficiency of postoperative IGF-1 was observed in 12% of patients. In similar to Jahangiri et al. [20] results, deficits were occurred in hormones production. Disorders of cortisol levels can also vary before and after pituitary surgery. For example, in patients who have had low blood pressure during anesthesia, or who have been taking medications such as phenytoin, ketoconazole, corticosteroid, and narcotics, the disorder is more pronounced [21, 22].
Guinto-Nishimura et al. in 2020 performed preoperative MRI in patients with non-functional pituitary macroadenoma to determine tumor severity alone and in association with the right cerebellar peduncle in 26 patients. Tumor consistency was assessed as soft in 20 (76.92%) patients. In the present study, 93% of the tumors had a soft consistency, which was higher than the Guinto-Nishimura study. Guinto-Nishimura et al. also showed that preoperative tumor volume was 28.7 ± 26.3 cm3 and the rate of tumor resection was not significantly associated with tumor consistency [23].
Onofrj et al. in 2018 reported that the mean preoperative tumor volume was 24.66 cm3. A progressive tumor volume decrease was noted during follow-up, and symptoms improved in 78% of patients. They conducted the duration of symptoms prior of surgery is a more important factor than tumor resection volume alone when considering the long-term outcome of symptoms. In our study preoperative mean tumor volume was 6845.5 mm3 and a significant relationship was observed between preoperative tumor volume and postoperative production of prolactin hormone [24].
Juthani et al. in 2020 performed a study on the 212 patients with pituitary MRI before and after surgery. 62% of patients underwent resection of the tumor based on postoperative MRI findings and comparison with preoperative resection, and as a result, the remnants of the tumor had to be removed. Tumor resection due to postoperative MRI results was significantly associated with increased survival and pituitary function as well as hormone therapy. These results suggest that using preoperative MRI is a safe method leading to the increase in the resection rate of pituitary adenomas. Especially when MRI is combined with endoscopy, it provides the ability to adapt to the removal of tumors while optimizing pituitary function, resulting in a high rate of recovery of secretory hormone [25].
In the results of the present study, normal tissue was not observed in 21.4% of MRI cases after surgery. MRI with or without administration of gadolinium contrast agent also allows accurate assessment of the position of the tumor before surgery and staging of pituitary tumors [13, 23]. Manifestations of normal pituitary gland tissue on MRI images include the size and shape of the gland reflecting pituitary function, which depends on the patient's position, the intensity of the adenohypophysis and neurohypophysis signals [13].
Given the prevalence of pituitary adenomas and especially their non-functional types, often diagnosed at higher stages, pre- and post- operative MRI scan can be used to choose the right treatment approach before.
Conclusion
There was a significant relationship between preoperative tumor size and volume and postoperative pituitary hormone production. Moreover, preoperative MRI characteristics could predict normal pituitary morphologic reconstruction after pituitary surgery.
Availability of data and materials
The datasets analyzed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author on reasonable request.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- TSH:
-
Thyroid stimulating hormone
- IUMS:
-
Iran University of Medical Science
- FCRDC:
-
Firouzgar Clinical Research Development Center
- NRPG:
-
Normal reconstruction of pituitary gland
- LH:
-
Luteinizing hormone
- FSH:
-
Follicle stimulating hormone
- GH:
-
Growth hormone
- ACTH:
-
Adrenocorticotropic hormone
- IPTR:
-
Iran Pituitary tumor registry
- PACS:
-
Picture Archiving and Communication System
- IQR:
-
Interquartile range
- PRL:
-
Prolactin
- ORs:
-
Odds ratio
- IGF-1:
-
Insulin-like Growth Factor-1
- TSS:
-
Trans sphenoidal surgery
References
AlMalki MH, Ahmad MM, Brema I, AlDahmani KM, Pervez N, Al-Dandan S, AlObaid A, Beshyah SA. Contemporary management of clinically non-functioning pituitary adenomas: a clinical review. Clin Med Insights Endocrinol Diabetes. 2020;13:1179551420932921.
Hwang JY, Aum DJ, Chicoine MR, Dacey RG, Osbun JW, Rich KM, Zipfel GJ, Klatt-Cromwell CN, McJunkin JL, Pipkorn P, Schneider JS. Axis-specific analysis and predictors of endocrine recovery and deficits for non-functioning pituitary adenomas undergoing endoscopic transsphenoidal surgery. Pituitary. 2020;23(4):389–99.
Seejore K, Alavi SA, Pearson SM, Robins JM, Alromhain B, Sheikh A, Nix P, Wilson T, Orme SM, Tyagi A, Phillips N. Post-operative volumes following endoscopic surgery for non-functioning pituitary macroadenomas are predictive of further intervention, but not endocrine outcomes. BMC Endocr Disord. 2021;21(1):1–3.
Tatsi C, Neely M, Flippo C, Bompou ME, Keil M, Stratakis CA. Recovery of hypothalamic-pituitary-adrenal axis in paediatric Cushing disease. Clin Endocrinol. 2021;94(1):40–7.
Budny B, Karmelita-Katulska K, Stajgis M, Żemojtel T, Ruchała M, Ziemnicka K. Copy number variants contributing to combined pituitary hormone deficiency. Int J Mol Sci. 2020;21(16):5757.
Chen Q, Zhou D, Abdel-Malek Z, Zhang F, Goff PS, Sviderskaya EV, Wakamatsu K, Ito S, Gross SS, Zippin JH. Measurement of melanin metabolism in live cells by [U-13C]-tyrosine fate tracing using LC-MS. J Investig Dermatol. 2021;141:1810–8.
Ostrowski SM, Fisher DE. Biology of melanoma. Hematol Oncol Clin. 2021;35(1):29–56.
Staartjes VE, Togni-Pogliorini A, Stumpo V, Serra C, Regli L. Impact of intraoperative magnetic resonance imaging on gross total resection, extent of resection, and residual tumor volume in pituitary surgery: systematic review and meta-analysis. Pituitary. 2021;4:1–3.
Giustina A, Barkhoudarian G, Beckers A, Ben-Shlomo A, Biermasz N, Biller B, Boguszewski C, Bolanowski M, Bollerslev J, Bonert V, Bronstein MD. Multidisciplinary management of acromegaly: a consensus. Rev Endocr Metab Disord. 2020;21(4):667–78.
Yan JL, Chang CN, Chen PY. Endoscopic transsphenoidal surgery for resection of pituitary macroadenoma: a retrospective study. PLoS ONE. 2021;16(8):e0255599.
Alhilali LM, Little AS, Yuen KC, Lee J, Ho TK, Fakhran S, White WL. Early postoperative MRI and detection of residual adenoma after transsphenoidal pituitary surgery. J Neurosurg. 2020;134(3):761–70.
Di Maio S, Biswas A, Vézina JL, Hardy J, Mohr G. Pre- and postoperative magnetic resonance imaging appearance of the normal residual pituitary gland following macroadenoma resection: clinical implications. Surg Neurol Int. 2012;3:67.
Hofstetter CP, Nanaszko MJ, Mubita LL, Tsiouris J, Anand VK, Schwartz TH. Volumetric classification of pituitary macroadenomas predicts outcome and morbidity following endoscopic endonasal transsphenoidal surgery. Pituitary. 2012;15(3):450–63.
Nomikos P, Ladar C, Fahlbusch R, Buchfelder M. Impact of primary surgery on pituitary function in patients with non-functioning pituitary adenomas—a study on 721 patients. Acta Neurochir (Wien). 2004;146(1):27–35.
Lee CC, Chen CM, Lee ST, Wei KC, Pai PC, Toh CH, Chuang CC. Prediction of long-term post-operative testosterone replacement requirement based on the pre-operative tumor volume and testosterone level in pituitary macroadenoma. Sci Rep. 2015;5(5):16194.
Ono M, Fukuda I, Soga A, Tahara S, Morita A, Sugihara H. A survey of surgically resected pituitary incidentalomas and a comparison of the clinical features and surgical outcomes of non-functioning pituitary adenomas discovered incidentally versus symptomatically. Endocr J. 2021;EJ20-0335.
Esposito D, Olsson DS, Ragnarsson O, Buchfelder M, Skoglund T, Johannsson G. Non-functioning pituitary adenomas: indications for pituitary surgery and post-surgical management. Pituitary. 2019;22(4):422–34.
Webb SM, Rigla M, Wägner A, Oliver B, Bartumeus F. Recovery of hypopituitarism after neurosurgical treatment of pituitary adenomas. J Clin Endocrinol Metab. 1999;84(10):3696–700.
Yagasaki Y, Katayama Y, Kinoshita Y, Nagata T, Kawakami Y, Miyata M. Macrophages are activated in the rat anterior pituitary under chronic inflammatory conditions. Neurosci Lett. 2021;748:135688.
Jahangiri A, Wagner JR, Han SW, Tran MT, Miller LM, Chen R, Tom MW, Ostling LR, Kunwar S, Blevins L, Aghi MK. Improved versus worsened endocrine function after transsphenoidal surgery for nonfunctional pituitary adenomas: rate, time course, and radiological analysis. J Neurosurg. 2016;124(3):589–95.
Lechan RM, Arkun K, Toni R. Pituitary anatomy and development. In: Prolactin disorders. Humana, Cham; 2019. pp. 11–53.
El Sayed SA, Fahmy MW, Schwartz J. Physiology, pituitary gland. StatPearls [Internet]. 2020.
Guinto-Nishimura GY, Ramirez J, Ortega-Porcayo LA, Marrufo-Meléndez O, Alcocer V, Ballesteros-Zebadua P, Gómez-Amador J. Accuracy of preoperative MRI for predicting tumor consistency in non-functioning pituitary adenomas. Neurosurgery. 2020;67(Supplement_1):nyaa447_856.
Onofrj V, Vallejo C, Puac P, Zamora C, Castillo M. Relationship between postoperative volume of macroadenomas and clinical outcome after endoscopic trans-sphenoidal resection. Neuroradiol J. 2018;31(6):565–71.
Juthani RG, Reiner AS, Patel AR, Cowan A, Roguski M, Panageas KS, Geer EB, Karimi S, Cohen MA, Tabar V. Radiographic and clinical outcomes using intraoperative magnetic resonance imaging for transsphenoidal resection of pituitary adenomas. J Neurosurg. 2020;3:1–12.
Acknowledgements
N/A.
Funding
N/A.
Author information
Authors and Affiliations
Contributions
NHM, MAK and MEKh conceived of the present idea. MAK and BH designed the study. Data acquisition was performed by BH. BH, NHM and MAK contributed to the data analysis and interpretation. BH and NHM were major contributors and contributed equally to writing the manuscript. MEKh critically revised the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethical Committee at Iran University of medical sciences, and written informed consent was obtained from all participants. (Approval Code: IR.IUMS.FMD.REC.1398.154). All methods in the study were carried out in accordance with the Helsinki guidelines and declaration.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hassani, B., Hashemi-Madani, N., Ataee Kachuee, M. et al. Magnetic resonance imaging characteristics predict pituitary function in non-functional pituitary macro-adenoma undergoing trans-sphenoidal surgery. BMC Med Imaging 22, 60 (2022). https://doi.org/10.1186/s12880-022-00787-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-022-00787-5