
Abstract
Hepatitis E virus (HEV) is an important emerging pathogen producing significant morbidity in immunosuppressed patients. HEV has been detrimental to solid organ transplant (SOT) patients, cancer patients, and HIV-positive patients, where chronic HEV infections occur. Blood-borne transfusions and multiple cases of chronic HEV infection in transplant patients have been reported in the past few decades, necessitating research on HEV pathogenesis using immunosuppressed animal models. Numerous animal species with unique naturally occurring HEV strains have been found, several of which have the potential to spread to humans and to serve as pathogenesis models. Host immunosuppression leads to viral persistence and chronic HEV infection allows for genetic adaptation to the human host creating new strains with worse disease outcomes. Procedures necessary for SOT often entail blood transfusions placing immunosuppressive patients into a “high risk group” for HEV infection. This scenario requires an appropriate immunosuppressive animal model to understand disease patterns in these patients. Hence, this article reviews the recent advances in the immunosuppressed animal models for chronic HEV infection with emphasis on pathogenesis, immune correlates, and the liver pathology associated with the chronic HEV infections.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Hepatitis E virus (HEV) is an interesting topic in the field of emerging infectious diseases. HEV ranks 6th on a list of spillover viruses with significant health risks to humans [1]. HEV causes both acute and chronic infection in humans and is the leading cause of acute viral gastroenteritis worldwide [2]. Chronic HEV infection has been reported in patients receiving a solid organ transplant (SOT) [3], with blood disorders [4], and in human immunodeficiency virus (HIV)-positive patients [5]. A sustained rise in liver enzyme levels and viral RNA detection in the blood and feces for at least six months following the acute phase of infection are considered indicators of a chronic HEV infection [3]. Chronic HEV infection is becoming more common, especially in patients receiving SOTs who require long term immunosuppression to prevent organ rejection [6, 7].
HEV is a non-enveloped, positive-sense RNA virus approximately 27–34 nm in diameter and contains a 6.4–7.2 kb viral genome encoding three primary open reading frames (ORFs). HEV is a member of the family Hepeviridae comprised of two subfamilies, five genera, and at least ten species [8]. Within the Hepeviridae, the Orthohepevirinae subfamily has several genera known to infect mammalian species. To date only Paslahepevirus genus members (previously known as Orthohepevirus A) and some members of the Rocahepevirus (previously known as Orthohepevirus C) genus have been found to infect immunosuppressed humans. More specifically, Paslahepevirus balayani genotype (gt)3, gt4, gt7, and Rocahepevirus ratti gt1 have been reported to infect immunosuppressed patients [3,4,5, 9,10,11,12,13].
A dearth of robust and tractable animal and cell culture models that accurately and fully mimic hepatitis E disease as observed in humans has made studying the pathogenesis of HEV a difficult undertaking. For instance, although the fecal-oral pathway is the main means of HEV transmission, the exact mechanism by which the virus particles move from the gastrointestinal system to the liver remained mostly unknown. Recently, clinical samples from a patient with a chronic HEV infection were shown to have intestinal crypts containing HEV RNA and ORF2 antigens leading to crypt cells being tested and confirmed as supporting HEV replication in vitro [14]. Animal models in which the immune response can be modified are necessary to uncover nuances of the HEV lifecycle that are otherwise suppressed and unobservable during natural infection. Furthermore, most HEV infections in immunocompromised individuals tend to become chronic infections [15] resulting in differential and prolonged pathogenesis compared to immunocompetent hosts. These persistent HEV infections can result in nodules, fibrotic remodeling, and eventually cirrhosis in the liver [16]. Consequently, it is imperative to comprehend the consequences of hepatitis E in individuals with impaired immune systems, necessitating the use of reliable and physiologically applicable animal models.
Here we have delineated HEV pathological features in humans resulting from chronic HEV infections during generalized immunosuppression. This information is intended to help readers understand the need for an appropriate immunosuppressive animal model for HEV. We discuss the pathogenesis of HEV in immunosuppressed cynomolgus monkeys, pigs, rabbits, mice, rats, and Mongolian gerbils while comparing the pathology, immune correlates, and drug screening between animal models that produce chronic HEV infection.
Chronic HEV infection pathology in humans
Persistent HEV replication for at least six months, moderate increase of liver enzymes, and an infrequent correlation with clinical indications commonly seen in immunosuppressed patients are characteristics of chronic human HEV infections [17]. Generally, gt1 and gt2 Paslahepevirus balyani strains are not attributed to chronic HEV infections whereas gt3 and gt4 are much more frequently associated with chronic infections making these strains a priority for animal infection models. The majority of otherwise healthy patients with P balayani gt3 or gt4 infection have no symptoms, but these viruses can have catastrophic consequences for immunocompromised or immunodeficient individuals [15]. Developed nations are seeing an increase in P balayani gt3 or gt4 infections, and immunocompromised persons are particularly vulnerable to persistent HEV-related liver fibrosis. Recently, chronic HEV infection of immunosuppressed patients has been reported to be caused by Rocahepevirus ratti gt1, despite the fact that this HEV strain significantly differs genetically from P balayani HEV strains [9].
In real-world clinical situations, chronic HEV infection develops in approximately 60% of transplant patients who have preexisting HEV infections or are exposed during transplantation via transfusion with 10% of these chronic patients developing cirrhosis [18, 19]. When hepatitis E is diagnosed in SOT patients undergoing tacrolimus medication, the risk is elevated [18]. Following SOT, reports have been made regarding the incidence of a de novo HEV infection as well as the risk of reinfection in the patients suggesting this may occur in 1 to 1.5% of patients [20, 21]. Interestingly, a case of chronic HEV gt3 has been reported in a pregnant woman who was under immunosuppressive agents for ulcerative colitis [22]. Even though the chronicity was observed, no adverse event during pregnancy was reported and resolution after delivery was without complications [22]. Another case of chronic HEV in pregnancy was reported in a kidney transplant patient. HEV gt3 infection was diagnosed during the first trimester of pregnancy [23]. Interestingly, HEV RNA increased by more than 1.5 log factor at the beginning of the third trimester but after the Cesarean section at the 38th week of gestation, the newborn and the placenta tested negative for HEV RNA. HEV was not detectable in the mother either in serum or stool even after six months [23] suggesting the role of pregnancy in HEV sustainability. A recent report of a pregnant woman who had undergone liver transplantation demonstrated the presence of HEV gt3 infection at the 34th week of gestation [24]. Placenta and breast milk tested positive for HEV RNA [24]. However, the newborn did not demonstrate HEV RNA either in serum or stool (tested at 1–5, 15th days and 1 month) and was negative for anti-HEV IgM but was positive for anti-HEV IgG [24]. In contrast to the previous case, HEV did not clear even after 3 months of delivery and thus, the mother was treated with the ribavirin for 16 months until the HEV RNA was undetectable in the serum and stool [24].
Clinical research has shown that for treatment plan guidance fecal HEV shedding is a more accurate indicator for relapse prediction in chronic HEV infection than viremia [25,26,27]. Nonetheless, it has been shown that immunosuppressed individuals’ blood and urine contain substantial concentrations of HEV antigens [28, 29]. Liver fibrosis and cirrhosis can develop quickly in SOT patients who have a persistent HEV infection [18, 30]. As expected, overexpression of host genes implicated in fibrogenesis was also discovered by RNA sequencing of host transcripts in fibrotic liver tissues [31].
According to histopathological findings, lymphocytic portal infiltrates with piecemeal necrosis (interface hepatitis) have been observed in HEV-infected heart and liver transplant recipients [3, 20, 32, 33]. Patients with SOT who progressed to chronic infection have low peak levels of ALT (Alanine aminotransferases) and AST (Aspartate aminotransferases) [18]. In addition to SOT patients, rheumatological patients, hematological patients, HIV-infected patients, and hematopoietic stem cell transplant (HSCT) patients are in the high-risk group to develop severe chronic HEV infection [34, 35]. Furthermore, tacrolimus usage during HEV infection has been linked to immune-mediated and drug-induced severe thrombocytopenia [36, 37]. Moreover, neurological conditions, renal damage, severe pancreatitis, and hematological abnormalities are extrahepatic symptoms of chronic HEV infection [33]. To help the reader comprehend the pathogenicity of chronic HEV infection and the need for a suitable immunosuppressed animal model, immunosuppressed chronic HEV infection has been summarized (Table 1).
Ideal immunosuppressive animal model attributes
Replicating the exact clinical disease and pathology of chronic human HEV infection in an animal model is extremely difficult. For in-depth HEV research, the ideal immunosuppressive animal model would include all the following traits.
-
a)
Develops liver specific pathology such as fibrosis and cirrhosis with alteration in liver enzymes (ALT, AST, and gamma glutamyl transferases (GGT)).
-
b)
Immunosuppressive drugs used in humans should be effective in lowering the immune response in the animal model.
-
c)
Animals should be susceptible to human derived HEV strains.
-
d)
Immunological responses to HEV should mimic humans.
-
e)
Chronic HEV infection in the immunosuppressed animal should mimic the prolonged viremia and fecal viral shedding seen in humans.
-
f)
Animal organ anatomical structure and physiological function should be close to humans.
-
g)
Experimental tool kits and reagents should be readily available for the animal model.
-
h)
Animal models should be genetically manipulatable such that knock-in or knock-out studies can be conducted.
Immunosuppressed animal models for studying chronic HEV infection
To obtain precise and accurate results, it is imperative to consistently replicate the human disease state in an animal model. An important factor to consider when selecting an appropriate HEV model is the animal’s susceptibility to a natural HEV infection. Moreover, using a particular animal species as a model for HEV infectious disease requires careful evaluation of the species’ anatomical, physiological, genetic, and biochemical parallels to humans.
Uncertainty surrounds the dynamics of HEV adaptation and propagation within genotypes that permit host range expansion. Numerous animal species have been found to have unique circulating HEV strains since the first animal HEV was discovered in pigs in 1997, followed by the first bird strain in 1998, the first rabbit strain in 2009, and the first rat strain in 2010. Several of these strains have the potential to spread to humans and cause chronic HEV infection. In order to study the outcomes of persistent hepatitis E in immunocompromised people, current immunocompromised animal models that replicate chronic HEV have been summarized below (Table 2).
Cynomolgus monkeys
When assessing the zoonotic potential of HEV, non-human primates (NHPs) are frequently the most appropriate model. The principal models used to research the clinical course of HEV infection are nonhuman primates (NHP), such as Macaca fascicularis (cynomolgus monkeys) and Macaca mulatta (rhesus monkeys). Despite not being HEV’s natural host, NHPs are vulnerable to experimental infection with P balayani gt1, gt2, gt3, and gt4 [56,57,58,59]. Cynomolgus monkeys were the first NHPs employed in experimental HEV infection research [60]. Additionally, a wide range of immunosuppressive drugs, including tacrolimus, have been developed in preclinical trials using cynomolgus monkeys, which are thought to be an excellent model for human organ transplantation [61, 62].
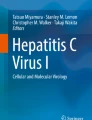
Experimental infection of cynomolgus monkeys under tacrolimus treatment and concurrent infection with P balayani gt3 Brazilian strain mimicked chronic HEV infection in humans. Chronic HEV signs such as persistent viremia, fecal viral shedding, and elevated liver enzymes, with gross and microscopic hepatitis observed in the liver (Fig. 1) [46].

Summary of immunosuppressed cynomolgus monkey model with intravenous (IV) HEV inoculation. HEV gt3 was used for the study. Interestingly, chronic hepatitis was evident but with the absence of fibrosis and cirrhosis in liver
Briefly, out of 4 NHPs used in the study, 3 of them became chronically infected. The clinical data presented during the acute phase of infection such as liver enzymes and antibody titers failed to predict chronicity in the monkeys. It’s interesting to note that three of the monkeys that had chronic infections showed signs of a very delayed seroconversion and a prolonged elevation in liver enzymes like ALT and AST [46]. Abnormal fat deposits in the liver parenchyma were directly correlated with decreased cholesterol in the plasma of chronically infected monkeys. There was no significant difference in the white blood cell (WBC) and platelet count due to the immunosuppressive drugs used in the monkeys before and after the infection [46].
Active replication in the liver and associated tissues such as gall bladder, spleen, and pancreas were demonstrated by the presence of HEV negative-stranded RNA [46]. Liver histopathology reported hepatocellular ballooning, scattered apoptosis, and lobular focal inflammation with microscopic necrotic features. After 4 months, immunosuppressed and HEV infected monkeys progressed to chronic hepatitis but there were no signs of liver fibrosis. Type 2 diabetes mellitus was reported in one of the monkeys under immunosuppression and HEV infection resolved after the discontinuation of the immunosuppressive drug [46].
Despite the fact that NHPs have been used in several studies, their inability to function as a natural host of HEV and the lack of liver fibrosis render them as a less suitable model for researching chronic HEV infection in humans. Furthermore, with chimpanzees and other great apes now subject to stringent restrictions on research, the use of these animals in future research is also constrained due to cost and ethical concerns with invasive biomedical research in primates.
Pigs
Pigs are the most studied source for xenotransplantation in humans [63]. Multiple immunosuppressive drugs used in humans during SOT have been studied in pigs [64, 65]. Pigs are anatomically, physiologically, and immunologically similar to humans and thus are a potentially good model for mimicking chronic hepatitis E in humans, particularly SOT patients [66, 67].
Zoonotic P balayani gt3 is responsible for many of the cases in humans leading to the development of chronic hepatitis [68, 69]. Pigs are a known reservoir for P balayani gt3 and gt4, allowing pigs to be used as a natural host model for pathogenesis and therapeutic studies [70].
Mycophenolate mofetil and tacrolimus are the most commonly used drugs in SOT patients. Experimental chronic HEV infection in pigs mimicked humans by utilizing a combinatorial approach of drugs and the human HEV P balayani gt3 (US2 strain) (Fig. 2) [67].

Summary of immunosuppressed pig model with intravenous (IV) HEV inoculation. Th1, Th2 cytokines and CD4 + T cells were reduced during the acute phase, however, CD8 + T cells increased during the chronic phase of infection
Chronic HEV infection was produced in pigs as fecal viral shedding was seen for at least 5–14 weeks longer in comparison to the immunocompetent pigs [67]. On the other hand, viremia failed to be a predictor for chronic HEV infection demonstrating equal viral titers to immunocompetent pigs. Histopathology reports did not show any significant differences in the liver of immunocompetent infected pigs compared to chronically infected pigs [67]. The immunosuppressive drug treated and infected group showed reduction in Th1 cytokines (IL-2 and IL-12) and no significant changes in the IFN-γ cytokine levels in blood when compared to the immunocompetent and infected group. However, the CD4+CD8+ T cell activation was decreased in the drug treated and infected group. During the chronic phase of infection, CD4+ T cells producing IL-4 increased in the blood of the immunosuppressed and infected pigs. A clear disease progression was evident by the shift of the immune response from CD4+CD8− T-cell population to CD4+CD8+ T-cell population in the immunosuppressed pigs [67].
Another study utilized tacrolimus-based regimen demonstrating persistent viremia for 11 weeks post inoculation [48]. Liver inflammation and fibrosis were reported in the immunosuppressed pigs [48]. They revealed a unique compartmentalization of HEV genomes in the feces and intestinal tissues, supporting extrahepatic replication in the digestive tract [48].
Pigs only develop subclinical infection when infected with HEV thus the immunological response in symptomatic human HEV patients cannot be mimicked in pigs. The absence of liver fibrosis and decreased frequencies of HEV-specific T-cells in peripheral blood indicate that pigs are not the most suitable model to fully replicate the chronic HEV patient condition in humans. Long term dosing of pigs with immunosuppressive drugs may also be cost prohibitive due to their propensity for high weight gain.
Rabbits
Rabbits are a well-studied model for renal transplantation [71], stem cell therapy [72], and drug based immunosuppression studies [73]. Phylogenetically, rabbits are more closely related to primates than to rodents [74]. Zoonotic P balayani gt4 strains and rabbit specific strains (gt3) are capable of infecting rabbits [75, 76]. Extrahepatic replication of HEV in the brain, heart, lung, kidney, spleen, and placenta has been demonstrated in SPF rabbits [77,78,79]. Easy availability of rabbits and minimum handling requirements while mimicking extrahepatic tissue lesions seen in humans make them a good model. Furthermore, rabbits and humans share similarities in airway anatomy and inflammatory responses [80, 81]. The size of rabbits enables non-lethal observation of physiological alterations. Robust infection with P balayani-gt3ra was seen in rabbits when compared to experimental infection with P balayani gt3 and P balayani gt4. Consistent fecal viral shedding was observed more often than viremia, suggesting that fecal viral shedding could be the best predictor of persistent infection while studying chronic HEV infection [25, 27].
Immunosuppression in rabbits was achieved by using cyclosporine A (Fig. 3). Rabbit strain P balayani-gt3ra demonstrated higher chronicity levels measured by the fecal viral shedding titers when compared to the zoonotic human derived P balayani gt3 and gt4. Liver fibrosis was evident in chronically infected rabbits [49].

Summary of immunosuppressed rabbit model with intravenous (IV) HEV inoculation. Chronic infection in rabbits with HEV gt3 leads to the development of fibrotic liver lesions. Cyclosporine A (CsA), rabbit (ra)
P balayani-gt3ra was found to replicate primarily in the intestine of rabbits and further disseminates to extrahepatic tissues. Interestingly, P balayani-gt3ra antigen was detected in the urine, kidney, cerebrospinal fluid but no such results were demonstrated in the rabbits infected with non-rabbit specific strains of P balayani gt3 and gt4 [49]. Surprisingly, higher numbers of single nucleotide variants (SNVs) were seen in the absence of immunosuppressants in rabbits infected with P balayani-gt3ra [49], highlighting the importance of the immune system in the development of quasispecies.
Recapitulation of human treatment using ribavirin for 3 months cleared HEV in cyclosporine treated rabbits. The Hecolin vaccine only provided partial protection when rabbits were already treated with immunosuppressive drugs. However, full protection was seen in rabbits against zoonotic P balayani gt3 and gt4 when vaccination was given before the start of the immunosuppressive treatment [49]. In addition, 94 differentially expressed genes (DEGs) and 10 hub genes (interacts with multiple genes and play an essential role in gene regulation and biological processes) have been found in rabbits with chronic HEV infection. The interferon signaling pathway and immune-related pathways were the primary areas of enrichment for DEGs in samples with chronic HEV infection. Most importantly, it was shown that Hub genes, such as MX1, OAS2, and IFI44, were involved in the pathophysiology of long-term HEV infection [82].
There are some disadvantages, even though immunocompromised rabbits challenged with P balayani-3ra are a very good model for simulating chronic HEV infection as seen in SOT patients. P balayani gt3 has been linked to rabbits yet attempts to infect rabbits experimentally with human strains of P balayani gt3 were not successful in these studies [76, 83, 84]. In contrast, another study demonstrated successful experimental infection in rabbits with human strains P balayani gt3 and gt4 [85]. This finding suggests that P balayani-3ra and swine or human P balayani-gt3 may differ in several biological aspects depending upon the host and virus species utilized for the studies. Furthermore, a larger animal is better suited to simulate the pathophysiology of a human disease than a smaller one because of the similarity in complexity between their organ structures. Additionally, there are few mechanistic rabbit investigations, especially those involving genetics, because there are few knockout or transgenic animals [80]. The rabbit is an excellent animal model, but despite its many benefits, it has not been employed extensively in HEV research yet. Compared to other smaller species like mice or guinea pigs, rabbits are more expensive to use due to the expense of the animal itself, larger and unique housing requirements (cage), and more difficult to maintain as they can be more prone to handling injuries than other species [80].
Mice
The murine model has become more popular in the last decade for HEV pathogenesis studies due to the advances in murine genetics and the abundance of tools and reagents available to study viral replication in mice. Lack of thymus and T lymphocytes in nude mice results in the absence of adaptive immune responses [86]. Furthermore, both functioning T and B cells are absent in severe combined immunodeficiency disease (SCID) mice [87]. Nude and SCID mouse innovations have led to preclinical and translational HEV research using these models in the last few decades.
P balayani gt4 was used to experimentally infect BALB/c nude mice, simulating human chronic HEV infection [50]. Increased levels of liver enzymes and HEV-specific antibodies in the blood suggested that the inoculated mice were undergoing more severe disease than contact mice. Liver histopathology revealed necrotic lesions with inflammation, which are similar to chronic HEV infection in human patients [50].
In 2016, experimental infection of zoonotic P balayani gt3 infection in human liver chimeric mice (mouse liver is partially populated with human cells) [88] demonstrated virus replication within 2 weeks. Virus derived from feces or liver were replication competent in comparison to plasma derived virus samples [51]. HEV RNA was consistently present in 100% of chimeric mouse livers from week 2 to week 14, and mouse passaged HEV was found to propagate for up to 100 days in vitro [51].
In 2020, BALB/c mice were used as a model for chronic P balayani gt4 HEV infection [52]. The mice were infected with a rhesus macaque-adapted gt4 chronically-mutated HEV strain [52]. HEV replication was efficient, and viral titers were persistently increased. HEV RNA was detected in various extrahepatic tissues, and HEV antigens were observed. The mice also showed enlarged portal tracts and proliferative fibrosis, and muted immune responses (reduced IFNα and IFNβ expression levels) [52].
In 2022, humanized uPA+/+-SCID mice were inoculated with the BeSW67HEV4-2008 viral strain [53]. The BeSW67HEV4-2008 strain, according to phylogenetic studies, is of the P balayani-4b subtype, whereas other strains that infect mice are of the P balayani-4 h subtype [53]. Interestingly, onset of infection and higher titers were observed in the mice inoculated with the mouse-passaged virus than the pig derived virus [53]. The virus’s adaptation to the human environment due to the close interaction of mice and humans may have improved infection of the mouse passaged virus.
Despite the promising results from the mouse models infected with HEV, there remain several drawbacks to these models that require further refinement. Lack of adaptive immune response in the humanized liver mice, skew towards a Th2 immune response in BALB/c mice and the predominant Th1 immune response in the C57BL/6 mice makes it difficult to understand the role of the adaptive immune system during HEV infections (Fig. 4) [92]. Intrasplenic and intraperitoneal inoculation used in the mouse models do not recapitulate the natural fecal oral transmission seen in humans. Interestingly, oral inoculum used in the human liver chimeric mice failed to establish infection [93]. Furthermore, the innate immunity in nude mice and the remnant natural killer (NK) cells in SCID mice limits the options for studying the host and viral interactions [94]. It has been further reported that there is a direct correlation between the age of nude mice with a drop in T cells [95]. Hence, even though immunosuppressed mice produce fibrosis recapitulating chronic HEV scenarios, multiple host related factors cannot be studied in mice.

Summary of immunosuppressed mouse model with oral, intravenous (IV), intrasplenic (IS) and intraperitoneal (IP) HEV inoculation. HEV gt4 infection in Balb/c mice were more prominent to develop chronic HEV infection demonstrating necrotic and fibrotic liver lesions
Rats
Rats are a natural host of Rocahepevirus ratti and have the potential to be an ideal candidate for the study of zoonotic rat HEV strains recently shown to spillover into humans. Immunosuppression of rats has been demonstrated with a combination of drugs that has been commonly used in human transplant patients. Drug combinations of prednisolone, tacrolimus, and mycophenolate mofetil have been successfully used to develop the immunosuppressed rat model demonstrating the phenotype seen in chronic hepatitis E patients via the inoculation of a rat specific strains; CCY and SRN (Fig. 5) [54].

Summary of immunosuppressive rat model with intravenous (IV) HEV inoculation. Chronically infected rats demonstrated the enhanced ALT liver enzyme level. Resolution of chronic infection was seen after the decrease in the immunosuppressive drugs which is the routine treatment regime in humans
Pathological lesions in the liver with some alteration in the liver enzymes such as ALT were observed in infected high dose immunosuppressed rats when compared to the low dose immunosuppressed and overall immunocompetent rats [54]. In addition, lack of viremia and restoration of immune responses were clear after stoppage of immunosuppressive drugs in rats mimicking the scenario seen in chronic HEV human patients [54]. Intraperitoneal ribavirin treatment further reduced viral suppression demonstrating the efficiency of the rat model to recapitulate human patient HEV infection [54].
In general, rats have become a popular choice for studying human disease because of their similarity with human genes involved in immunity, metabolic detoxification, chemosensation, and disease-linked human genes [93]. Being larger in size than mice make handling, sampling, and performing procedures easier. Recent developments in the availability of rat genomic tools have made it easier to manipulate the rat genome producing specific gene knockouts and knock-ins [94] allowing for more in depth understanding of disease factors at the genetic level. Although rat models have several advantages mimicking chronic disease, rats have a different coagulation system than humans leading to delayed wound healing [95]. In addition, immunosuppressed rats were shown to be not susceptible to the human derived P. balayani gt4 strains [54] highlighting its disadvantage in mimicking pathology using human circulating strains.
Mongolian gerbils
Mongolian gerbils are a newly reemerging animal model to study HEV induced acute [96] and neurological infection [97] associated with P. balayani genotypes. Of all available animal models, gerbils are the second smallest in body size after mice and thus easy to handle and study in significant numbers. Immunosuppression in gerbils was achieved by the surgical implantation of a tacrolimus pellet in the neck [55]. Mongolian gerbils were inoculated with the P. balayani gt3 strain (derived from macaques) (Fig. 6).

Summary of immunosuppressed gerbil model with intravenous (IV) HEV inoculation. CD68 + macrophage was absent in the liver of chronically infected gerbils. Extrahepatic distribution of HEV was seen in the chronically infected gerbils
Elevation of ALT in the blood, persistent viremia in concomitance with fecal viral shedding was reported in gerbils treated with tacrolimus [55]. Weak serological responses were reported for the immunosuppressed group when compared to immunocompetent gerbils. Interestingly, the immunological response in the liver was associated with the presence of CD68 + macrophages at microscopic foci demonstrating some apoptosis in the immunocompetent group. CD68 + macrophages were absent in the tacrolimus treated and infected group suggesting immunological damage in the liver of immunocompetent individuals during HEV infection [55]. Interestingly, the gerbil model has demonstrated experimental infection with a gerbil adapted gt1 strain. Pregnant gerbils infected with the gt1 strains developed robust, acute HEV infection and induced maternal mortality [98]. In addition, transmission of the virus to the offspring was noted [98]. These findings are very insightful and demonstrates the importance of pregnant gerbil models to understand the mechanism behind pregnancy mortality associated with HEV infection and to provide a mechanistic view of HEV crossing the blood placental barrier. In addition, tacrolimus prolonged HEV gt1 infection in gerbils [98], highlighting the scenario seen in humans where immunosuppressive drugs are known to lengthen the duration of infection leading to chronicity. Thus, the HEV gt1 infection gerbil model could be an interesting model to investigate the in-depth HEV immunopathogenesis, genotype associated pregnancy mortality, testing vaccines and antivirals against HEV.
As for model drawbacks, the implantation of the immunosuppressed drugs does not mimic the drug dosage routine in humans. The implantation of tacrolimus allows for continuous effects of the drug in body homeostasis [55]. One can argue that the small size of the gerbil, its potential to mimic active and neurological infection makes it a good animal model for acute infection. However, anatomical differences in the organ size, structure and functions when compared to humans and the availability of reagents make it a less popular immunosuppressed model for HEV.
Conclusions
The importance of chronically infected animal models in understanding HEV pathophysiology is of utmost importance in biomedical research. Advancements in the biomedical field have led to the development of immunosuppressed animal models either by the utilization of immunosuppressant drugs or by gene editing. To help the reader to understand the importance of utilizing a particular chronic HEV model, several potential questions that could be answered by the utilization of a model are listed below:
Potential questions answered by a chronic animal model recapitulating HEV infection | |
|---|---|
1. Does chronicity depend on HEV genotypes? | |
2. Are chronic liver lesions mediated by virus replication or the result of the host immune reaction? | |
3. Can pregnancy trigger HEV chronicity? | |
4. What are the roles of immune privileged sites during chronic HEV infection? | |
5. What is the role of HEV quasispecies in the maintenance of chronicity? | |
6. Can human derived HEV be infectious in an animal model recapitulating the chronic fecal viral shedding and viremia seen in humans? | |
7. Can higher antibody response and elevated liver enzymes be mimicked in an animal model? | |
8. Does reducing immunosuppression decrease HEV viral titers in an animal model? |
The above listed animal models such as cynomolgus monkeys, pigs, rabbits, mice, rats and gerbils have answered very important aspects of HEV pathophysiology during chronic HEV infection. Even though immunosuppressed cynomolgus monkeys, pigs, and rats recapitulate the chronic fecal viral shedding and viremia, they do not develop liver fibrosis as can be seen in chronic HEV model such as rabbits, mice, and gerbils. This suggests that even in animals recapitulating higher anatomical structure and physiological functions found in larger vertebrates more closely resembling humans, recapitulating all of the clinical manifestations of infectious disease is rare often necessitating multiple animals to answer some questions.
Existing literature suggests that the most chronic HEV cases are affiliated with zoonotic Paslahepevirus balayani gt3 and gt4 infections [3]. This suggests that the chronicity is related to certain genotypes of HEV. Recent advancement in understanding HEV have demonstrated the unique ability of HEV to cross the blood brain barrier (BBB) [99] and blood testis barrier (BTB) which are immune privileged sites in the body [100]. In addition, infectious HEV presence in the sperm head [101] demands the need to understand the ability of HEV to be transmitted sexually between partners. A recent study reported infectious HEV particles in semen of nine chronically infected men [102]. The viral load in semen was 100-fold higher when compared to the serum in five of the infected men [102]. Interestingly, few studies reported no evidence of the ability of HEV to transmit sexually between humans [103, 104]. These studies highlighted HEV infection based on seroconversion but the demonstration of higher HEV titers in the ejaculate of chronically infected men delineates the need to understand the importance of HEV concentration, duration of shedding in ejaculate and ability to transmit the virus during active shedding of HEV in semen. Hence, the interplay between HEV and the immunosuppressed host needs to be further investigated by utilizing the immunosuppressed animal models.
With recent advancements in scientific technology, future studies in HEV need to be directed in specific areas: (a) the exact cellular receptor(s) that HEV recognizes and allows cellular entry. (b) the mechanisms by which HEV produces liver injury and cirrhosis in chronic HEV patients. (c) quasispecies formation in the central nervous system and its role in the devastating neurological effects in chronic HEV patients. (d) the ability of HEV to cross the BTB and the investigation of quasispecies and their role in the reinfection in chronic HEV patients. (e) the transmission route of HEV other than the fecal-oral, blood transfusions, and mother-to-child transmission. Chronic HEV infection in the immunosuppressed patient needs to be emphasized to understand the underlying role of viral factors leading to worse disease outcomes.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- ALT:
-
Alanine Aminotransferase
- AST:
-
Aspartate Aminotransferase
- BBB:
-
Blood Brain Barrier
- BTB:
-
Blood Testis Barrier
- DEG:
-
Differentially Expressed Genes
- GGT:
-
Gamma Glutamyl Transferase
- HEV:
-
Hepatitis E Virus
- IV:
-
Intravenous
- ORF:
-
Open Reading Frame
- SCID:
-
Severe Combined Immunodeficiency Disease
- SNV:
-
Single Nucleotide Variants
- SOT:
-
Solid Organ Transplantation
References
Grange ZL, Goldstein T, Johnson CK, Anthony S, Gilardi K, Daszak P et al. Ranking the risk of animal-to-human spillover for newly discovered viruses. Proceedings of the National Academy of Sciences. 2021;118(15):e2002324118.
Lhomme S, Marion O, Abravanel F, Izopet J, Kamar N. Clinical manifestations, Pathogenesis and treatment of Hepatitis E Virus infections. J Clin Med. 2020;9(2).
Kamar N, Selves J, Mansuy JM, Ouezzani L, Péron JM, Guitard J, et al. Hepatitis E virus and chronic hepatitis in organ-transplant recipients. N Engl J Med. 2008;358(8):811–7.
Ollier L, Tieulie N, Sanderson F, Heudier P, Giordanengo V, Fuzibet JG, et al. Chronic hepatitis after hepatitis E virus infection in a patient with non-hodgkin lymphoma taking rituximab. Ann Intern Med. 2009;150(6):430–1.
Dalton HR, Bendall RP, Keane FE, Tedder RS, Ijaz S. Persistent carriage of hepatitis E virus in patients with HIV infection. N Engl J Med. 2009;361(10):1025–7.
Thakur V, Ratho RK, Kumar S, Saxena SK, Bora I, Thakur P. Viral Hepatitis E and chronicity: a growing Public Health concern. Front Microbiol. 2020;11:577339.
Thongprayoon C, Kaewput W, Pattharanitima P, Cheungpasitporn W. Progress and recent advances in solid organ transplantation. J Clin Med. 2022;11(8).
Tam AW, Smith MM, Guerra ME, Huang CC, Bradley DW, Fry KE, et al. Hepatitis E virus (HEV): molecular cloning and sequencing of the full-length viral genome. Virology. 1991;185(1):120–31.
Sridhar S, Yip CCY, Wu S, Cai J, Zhang AJ, Leung KH, et al. Rat Hepatitis E Virus as cause of Persistent Hepatitis after Liver Transplant. Emerg Infect Dis. 2018;24(12):2241–50.
Sridhar S, Yip CC, Wu S, Chew NF, Leung KH, Chan JF, et al. Transmission of Rat Hepatitis E virus infection to humans in Hong Kong: a clinical and epidemiological analysis. Hepatology (Baltimore MD). 2021;73(1):10–22.
Haagsma EB, van den Berg AP, Porte RJ, Benne CA, Vennema H, Reimerink JH, et al. Chronic hepatitis E virus infection in liver transplant recipients. Liver transplantation: official publication of the American Association for the study of Liver diseases. Int Liver Transplantation Soc. 2008;14(4):547–53.
Lee GH, Tan BH, Teo EC, Lim SG, Dan YY, Wee A, et al. Chronic infection with Camelid Hepatitis E Virus in a liver transplant recipient who regularly consumes Camel meat and milk. Gastroenterology. 2016;150(2):355–e73.
Shirazi R, Pozzi P, Gozlan Y, Wax M, Lustig Y, Linial M et al. Identification of Hepatitis E virus genotypes 3 and 7 in Israel. Public Health Concern? Viruses. 2021;13(11).
Marion O, Lhomme S, Nayrac M, Dubois M, Pucelle M, Requena M, et al. Hepatitis E virus replication in human intestinal cells. Gut. 2020;69(5):901–10.
Kamar N, Dalton HR, Abravanel F, Izopet J. Hepatitis E virus infection. Clin Microbiol Rev. 2014;27(1):116–38.
Gérolami R, Moal V, Colson P. Chronic hepatitis E with cirrhosis in a kidney-transplant recipient. N Engl J Med. 2008;358(8):859–60.
Kamar N, Rostaing L, Legrand-Abravanel F, Izopet J. How should Hepatitis E virus infection be defined in organ-transplant recipients? Am J Transplantation: Official J Am Soc Transplantation Am Soc Transpl Surg. 2013;13(7):1935–6.
Kamar N, Garrouste C, Haagsma EB, Garrigue V, Pischke S, Chauvet C, et al. Factors associated with chronic hepatitis in patients with hepatitis E virus infection who have received solid organ transplants. Gastroenterology. 2011;140(5):1481–9.
Legrand-Abravanel F, Kamar N, Sandres-Saune K, Garrouste C, Dubois M, Mansuy JM, et al. Characteristics of autochthonous hepatitis E virus infection in solid-organ transplant recipients in France. J Infect Dis. 2010;202(6):835–44.
Pischke S, Stiefel P, Franz B, Bremer B, Suneetha PV, Heim A, et al. Chronic hepatitis e in heart transplant recipients. Am J Transplantation: Official J Am Soc Transplantation Am Soc Transpl Surg. 2012;12(11):3128–33.
Haagsma EB, Niesters HG, van den Berg AP, Riezebos-Brilman A, Porte RJ, Vennema H, et al. Prevalence of hepatitis E virus infection in liver transplant recipients. Liver transplantation: official publication of the American Association for the Study of Liver Diseases and the International Liver. Transplantation Soc. 2009;15(10):1225–8.
Charre C, Ramière C, Dumortier J, Abravanel F, Lhomme S, Gincul R, et al. Chronic genotype 3 Hepatitis E in pregnant woman receiving infliximab and azathioprine. Emerg Infect Dis. 2018;24(5):941–3.
Mallet V, Le Mener S, Roque-Afonso AM, Tsatsaris V, Mamzer MF. Chronic hepatitis E infection cured by pregnancy. J Clin Virology: Official Publication Pan Am Soc Clin Virol. 2013;58(4):745–7.
Marion O, Abravanel F, Conan L, Dubucs C, Danjoux M, Izopet J, et al. Hepatitis E virus infection in a pregnant liver transplant recipient leading to chronic infection. Transplantation Direct. 2024;10(6):e1634.
Ambrosioni J, Mamin A, Hadengue A, Bernimoulin M, Samii K, Landelle C, et al. Long-term hepatitis E viral load kinetics in an immunocompromised patient treated with Ribavirin. Clin Microbiol Infection: Official Publication Eur Soc Clin Microbiol Infect Dis. 2014;20(10):O718–20.
Abravanel F, Lhomme S, Rostaing L, Kamar N, Izopet J. Protracted fecal shedding of HEV during Ribavirin therapy predicts treatment relapse. Clin Infect Diseases: Official Publication Infect Dis Soc Am. 2015;60(1):96–9.
Marion O, Lhomme S, Del Bello A, Abravanel F, Esposito L, Hébral AL, et al. Monitoring hepatitis E virus fecal shedding to optimize Ribavirin treatment duration in chronically infected transplant patients. J Hepatol. 2019;70(1):206–9.
Marion O, Capelli N, Lhomme S, Dubois M, Pucelle M, Abravanel F, et al. Hepatitis E virus genotype 3 and capsid protein in the blood and urine of immunocompromised patients. J Infect. 2019;78(3):232–40.
Zhang H, Rao H, Wang Y, Wang J, Kong X, Ji Y, et al. Evaluation of an antigen assay for diagnosing acute and chronic hepatitis E genotype 4 infection. J Gastroenterol Hepatol. 2019;34(2):458–65.
Kamar N, Mansuy JM, Cointault O, Selves J, Abravanel F, Danjoux M, et al. Hepatitis E virus-related cirrhosis in kidney- and kidney-pancreas-transplant recipients. Am J Transplantation: Official J Am Soc Transplantation Am Soc Transpl Surg. 2008;8(8):1744–8.
Kisseleva T, Brenner D. Molecular and cellular mechanisms of liver fibrosis and its regression. Nat Reviews Gastroenterol Hepatol. 2021;18(3):151–66.
Pischke S, Suneetha PV, Baechlein C, Barg-Hock H, Heim A, Kamar N, et al. Hepatitis E virus infection as a cause of graft hepatitis in liver transplant recipients. Liver transplantation: official publication of the American Association for the study of Liver diseases. Int Liver Transplantation Soc. 2010;16(1):74–82.
Kamar N, Marion O, Abravanel F, Izopet J, Dalton HR. Extrahepatic manifestations of hepatitis E virus. Liver International: Official J Int Association Study Liver. 2016;36(4):467–72.
Damiris K, Aghaie Meybodi M, Niazi M, Pyrsopoulos N. Hepatitis E in immunocompromised individuals. World J Hepatol. 2022;14(3):482–94.
Alexandrova R, Tsachev I, Kirov P, Abudalleh A, Hristov H, Zhivkova T, et al. Hepatitis E Virus (HEV) infection among immunocompromised individuals: a brief narrative review. Infect drug Resist. 2024;17:1021–40.
Colson P, Payraudeau E, Leonnet C, De Montigny S, Villeneuve L, Motte A, et al. Severe thrombocytopenia associated with acute hepatitis E virus infection. J Clin Microbiol. 2008;46(7):2450–2.
Fourquet E, Mansuy JM, Bureau C, Recher C, Vinel JP, Izopet J et al. Severe thrombocytopenia associated with acute autochthonous hepatitis E. Journal of clinical virology: the official publication of the Pan American Society for Clinical Virology. 2010;48(1):73–4.
Ma Z, de Man RA, Kamar N, Pan Q. Chronic hepatitis E: advancing research and patient care. J Hepatol. 2022;77(4):1109–23.
Pischke S, Peron JM, von Wulffen M, von Felden J, Höner Zu Siederdissen C, Fournier S et al. Chronic Hepatitis E in Rheumatology and Internal Medicine patients: a Retrospective Multicenter European Cohort Study. Viruses. 2019;11(2).
Ghandili S, Lindhauer C, Pischke S, Zur Wiesch JS, Von Kroge PH, Polywka S, et al. Clinical features of hepatitis E infections in patients with hematologic disorders. Haematologica. 2022;107(12):2870–83.
Rivero-Juarez A, Lopez-Lopez P, Frias M, Rivero A. Hepatitis E infection in HIV-Infected patients. Front Microbiol. 2019;10:1425.
Cruz S, Campos C, Timóteo M, Tavares A, José Nascimento MS, Medeiros R, et al. Hepatitis E virus in hematopoietic stem cell transplant recipients: a systematic review. J Clin Virol. 2019;119:31–6.
Ian R, Fox T, Irish D, Bharucha T, Thorburn D, Mark H, et al. Hepatitis E Viraemia in Transplant recipients. Blood. 2016;128(22):3846.
Swartling L, Nordén R, Samuelsson E, Boriskina K, Valentini D, Westin J, et al. Hepatitis E virus is an infrequent but potentially serious infection in allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2020;55(7):1255–63.
Michniacki TF, Choi SW, Peltier DC. Immune suppression in allogeneic hematopoietic stem cell transplantation. Handb Exp Pharmacol. 2022;272:209–43.
Gardinali NR, Guimarães JR, Melgaço JG, Kevorkian YB, Bottino FO, Vieira YR, et al. Cynomolgus monkeys are successfully and persistently infected with hepatitis E virus genotype 3 (HEV-3) after long-term immunosuppressive therapy. PLoS ONE. 2017;12(3):e0174070.
Cao D, Cao QM, Subramaniam S, Yugo DM, Heffron CL, Rogers AJ et al. Pig model mimicking chronic hepatitis E virus infection in immunocompromised patients to assess immune correlates during chronicity. Proceedings of the National Academy of Sciences. 2017;114(27):6914-23.
León-Janampa N, Caballero-Posadas I, Barc C, Darrouzain F, Moreau A, Guinoiseau T et al. A pig model of chronic hepatitis E displaying persistent viremia and a downregulation of innate immune responses in the liver. Hepatol Commun. 2023;7(11).
He Q, Zhang F, Shu J, Li S, Liang Z, Du M, et al. Immunocompromised rabbit model of chronic HEV reveals liver fibrosis and distinct efficacy of different vaccination strategies. Hepatology (Baltimore, Md; 2022.
Huang F, Zhang W, Gong G, Yuan C, Yan Y, Yang S, et al. Experimental infection of Balb/c nude mice with Hepatitis E virus. BMC Infect Dis. 2009;9:93.
Allweiss L, Gass S, Giersch K, Groth A, Kah J, Volz T, et al. Human liver chimeric mice as a new model of chronic hepatitis E virus infection and preclinical drug evaluation. J Hepatol. 2016;64(5):1033–40.
Li Y, Long F, Yang C, Hao X, Wu J, Situ J, et al. BALB/c mouse is a potential animal Model System for studying Acute and Chronic Genotype 4 Hepatitis E virus infection. Front Microbiol. 2020;11:1156.
Collignon L, Verhoye L, Hakze-Van der Honing R, Van der Poel WHM, Meuleman P. Study of Hepatitis E Virus-4 infection in human Liver-Chimeric, Immunodeficient, and Immunocompetent mice. Front Microbiol. 2022;13:819877.
Sridhar S, Wu S, Situ J, Shun EH, Li Z, Zhang AJ, et al. A small animal model of chronic hepatitis E infection using immunocompromised rats. JHEP Rep. 2022;4(10):100546.
Subramaniam S, Fares-Gusmao R, Sato S, Cullen JM, Takeda K, Farci P, et al. Distinct disease features of acute and persistent genotype 3 hepatitis E virus infection in immunocompetent and immunosuppressed Mongolian gerbils. PLoS Pathog. 2023;19(9):e1011664.
Krawczynski K, Meng XJ, Rybczynska J. Pathogenetic elements of hepatitis E and animal models of HEV infection. Virus Res. 2011;161(1):78–83.
Purcell RH, Engle RE, Govindarajan S, Herbert R, St Claire M, Elkins WR, et al. Pathobiology of hepatitis E: lessons learned from primate models. Emerg Microbes Infections. 2013;2(3):e9.
Tsarev SA, Tsareva TS, Emerson SU, Govindarajan S, Shapiro M, Gerin JL, et al. Successful passive and active immunization of cynomolgus monkeys against hepatitis E. Proc Natl Acad Sci U S A. 1994;91(21):10198–202.
Tsarev SA, Tsareva TS, Emerson SU, Yarbough PO, Legters LJ, Moskal T, et al. Infectivity titration of a prototype strain of hepatitis E virus in cynomolgus monkeys. J Med Virol. 1994;43(2):135–42.
Balayan MS, Andjaparidze AG, Savinskaya SS, Ketiladze ES, Braginsky DM, Savinov AP, et al. Evidence for a virus in non-A, non-B hepatitis transmitted via the fecal-oral route. Intervirology. 1983;20(1):23–31.
Kinugasa F, Nagatomi I, Ishikawa H, Nakanishi T, Maeda M, Hirose J, et al. Efficacy of oral treatment with tacrolimus in the renal transplant model in cynomolgus monkeys. J Pharmacol Sci. 2008;108(4):529–34.
Haustein SV, Kolterman AJ, Sundblad JJ, Fechner JH, Knechtle SJ. Nonhuman primate infections after organ transplantation. ILAR J. 2008;49(2):209–19.
Sykes M, Sachs DH. Transplanting organs from pigs to humans. Sci Immunol. 2019;4(41):eaau6298.
Pirenne J, Benedetti E, Gruessner A, Moon C, Hakim N, Fryer JP, et al. Combined transplantation of small and large bowel. FK506 versus cyclosporine A in a porcine model. Transplantation. 1996;61(12):1685–94.
Grant D, Duff J, Zhong R, Garcia B, Lipohar C, Keown P, et al. Successful intestinal transplantation in pigs treated with cyclosporine. Transplantation. 1988;45(2):279–84.
Dalton HR, Webb GW, Norton BC, Woolson KL, Hepatitis E, Virus. Time to change the textbooks. Digestive diseases. (Basel Switzerland). 2016;34(4):308–16.
Cao D, Cao QM, Subramaniam S, Yugo DM, Heffron CL, Rogers AJ, et al. Pig model mimicking chronic hepatitis E virus infection in immunocompromised patients to assess immune correlates during chronicity. Proc Natl Acad Sci U S A. 2017;114(27):6914–23.
Murali AR, Kotwal V, Chawla S. Chronic hepatitis E: a brief review. World J Hepatol. 2015;7(19):2194–201.
Singh A, Seth R, Gupta A, Shalimar, Nayak B, Acharya SK, et al. Chronic hepatitis E - an emerging disease in an immunocompromised host. Gastroenterol Rep. 2018;6(2):152–5.
Meng XJ, Hepatitis E. Virus: animal reservoirs and zoonotic risk. Vet Microbiol. 2010;140(3–4):256–65.
Jacobsen IA. Renal transplantation in the rabbit: a model for preservation studies. Lab Anim. 1978;12(2):63–70.
Kamaruzaman NA, Kardia E, Kamaldin NA, Latahir AZ, Yahaya BH. The rabbit as a model for studying lung disease and stem cell therapy. Biomed Res Int. 2013;2013:691830.
Jeklova E, Leva L, Jaglic Z, Faldyna M. Dexamethasone-induced immunosuppression: a rabbit model. Vet Immunol Immunopathol. 2008;122(3–4):231–40.
Graur D, Duret L, Gouy M. Phylogenetic position of the order Lagomorpha (rabbits, hares and allies). Nature. 1996;379(6563):333–5.
Ma H, Zheng L, Liu Y, Zhao C, Harrison TJ, Ma Y, et al. Experimental infection of rabbits with rabbit and genotypes 1 and 4 hepatitis E viruses. PLoS ONE. 2010;5(2):e9160–e.
Cheng X, Wang S, Dai X, Shi C, Wen Y, Zhu M, et al. Rabbit as a novel animal model for hepatitis E virus infection and vaccine evaluation. PLoS ONE. 2012;7(12):e51616–e.
Liu P, Bu QN, Wang L, Han J, Du RJ, Lei YX, et al. Transmission of hepatitis E virus from rabbits to cynomolgus macaques. Emerg Infect Dis. 2013;19(4):559–65.
Han J, Lei Y, Liu L, Liu P, Xia J, Zhang Y, et al. SPF rabbits infected with rabbit hepatitis E virus isolate experimentally showing the chronicity of hepatitis. PLoS ONE. 2014;9(6):e99861.
Xia J, Liu L, Wang L, Zhang Y, Zeng H, Liu P, et al. Experimental infection of pregnant rabbits with hepatitis E virus demonstrating high mortality and vertical transmission. J Viral Hepatitis. 2015;22(10):850–7.
Keir S, Page C. The rabbit as a model to study asthma and other lung diseases. Pulm Pharmacol Ther. 2008;21(5):721–30.
Karol MH. Animal models of occupational asthma. Eur Respir J. 1994;7(3):555–68.
Li M, Wang Y, Li K, Lan H, Zhou C. Characterization of highly expressed novel hub genes in hepatitis E virus chronicity in rabbits: a bioinformatics and experimental analysis. BMC Vet Res. 2022;18(1):239.
Smith DB, Simmonds P, Members Of The International Committee On The Taxonomy Of Viruses, Study G, Jameel S, Emerson SU, Harrison TJ, et al. Consensus proposals for classification of the family Hepeviridae. J Gen Virol. 2014;95(Pt 10):2223–32.
Zhang Y, Gong W, Song WT, Fu H, Wang L, Li M, et al. Different susceptibility and pathogenesis of rabbit genotype 3 hepatitis E virus (HEV-3) and human HEV-3 (JRC-HE3) in SPF rabbits. Vet Microbiol. 2017;207:1–6.
He Q, Zhang F, Shu J, Li S, Liang Z, Du M, et al. Immunocompromised rabbit model of chronic HEV reveals liver fibrosis and distinct efficacy of different vaccination strategies. Hepatology (Baltimore MD). 2022;76(3):788–802.
Flanagan SP. Nude’, a new hairless gene with pleiotropic effects in the mouse. Genet Res. 1966;8(3):295–309.
Bosma GC, Custer RP, Bosma MJ. A severe combined immunodeficiency mutation in the mouse. Nature. 1983;301(5900):527–30.
Strom SC, Davila J, Grompe M. Chimeric mice with humanized liver: tools for the study of drug metabolism, excretion, and toxicity. Methods Mol Biol. 2010;640:491–509.
Sellers RS, Clifford CB, Treuting PM, Brayton C. Immunological variation between inbred laboratory mouse strains: points to consider in phenotyping genetically immunomodified mice. Vet Pathol. 2012;49(1):32–43.
Sayed IM, Verhoye L, Cocquerel L, Abravanel F, Foquet L, Montpellier C, et al. Study of hepatitis E virus infection of genotype 1 and 3 in mice with humanised liver. Gut. 2017;66(5):920–9.
Budzynski W, Radzikowski C. Cytotoxic cells in immunodeficient athymic mice. Immunopharmacol Immunotoxicol. 1994;16(3):319–46.
Giovanella BC, Fogh J. The nude mouse in cancer research. Adv Cancer Res. 1985;44:69–120.
Gibbs RA, Weinstock GM, Metzker ML, Muzny DM, Sodergren EJ, Scherer S, et al. Genome sequence of the Brown Norway rat yields insights into mammalian evolution. Nature. 2004;428(6982):493–521.
Parker CC, Chen H, Flagel SB, Geurts AM, Richards JB, Robinson TE, et al. Rats are the smart choice: Rationale for a renewed focus on rats in behavioral genetics. Neuropharmacology. 2014;76(0):250–8. Pt B(0.
Dorsett-Martin WA. Rat models of skin wound healing: a review. Wound Repair Regeneration. 2004;12(6):591–9.
Zhang W, Ami Y, Suzaki Y, Doan YH, Muramatsu M, Li TC. Mongolia Gerbils are broadly susceptible to Hepatitis E Virus. Viruses. 2022;14(6).
Shi M, Lin XD, Chen X, Tian JH, Chen LJ, Li K, et al. The evolutionary history of vertebrate RNA viruses. Nature. 2018;556(7700):197–202.
Liu T, He Q, Yang X, Li Y, Yuan D, Lu Q et al. An Immunocompetent Mongolian Gerbil Model for Hepatitis E Virus genotype 1 infection. Gastroenterology. 2024.
Tian D, Li W, Heffron CL, Wang B, Mahsoub HM, Sooryanarain H, et al. Hepatitis E virus infects brain microvascular endothelial cells, crosses the blood-brain barrier, and invades the central nervous system. Proc Natl Acad Sci U S A. 2022;119(24):e2201862119.
Horvatits T, Wißmann JE, Johne R, Groschup MH, Gadicherla AK, Schulze Zur Wiesch J, et al. Hepatitis E virus persists in the ejaculate of chronically infected men. J Hepatol. 2021;75(1):55–63.
Yadav KK, Boley PA, Laocharoensuk T, Khatiwada S, Lee CM, Bhandari M, et al. Infectious hepatitis E virus is associated with the mature sperm head. PLoS Pathog. 2024;20(5):e1012240.
Schemmerer M, Bock HH, Schattenberg JM, Huber S, Polywka S, Mader M, et al. Proof of infectivity of hepatitis E virus particles from the ejaculate of chronically infected patients. J Med Virol. 2024;96(6):e29735.
Schäfer G, Lübke R, Degen O, Mader M, Scheiter R, Wolski A, et al. Lack of evidence of acute HEV infections as a sexually transmitted disease: data from a German cohort of PrEP users. Brazilian J Infect Diseases: Official Publication Brazilian Soc Infect Dis. 2024;28(1):103720.
Chaix ML, Leturque N, Gabassi A, Charreau I, Minier M, Pialoux G et al. Prevalence and incidence of HEV among men using HIV pre-exposure prophylaxis: a sub-study of the ANRS IPERGAY trial. Journal of clinical virology: the official publication of the Pan American Society for Clinical Virology. 2023;160:105380.
Acknowledgements
Not applicable.
Funding
Additional salaries and research support were provided by state and federal funds appropriated to the Ohio Agricultural Research and Development Center, The Ohio State University, and from the research funds of National Institute of Allergy and Infectious Diseases (#R21AI151736).
Author information
Authors and Affiliations
Contributions
KKY and SK wrote the main manuscript text. KKY prepared the figures. KKY and SK revised the manuscript. SK provided the funding and oversight.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Authors information
KKY has 6 years of experience working with HEV and has utilized the immunosuppressed pig animal model to understand the pathology of HEV ribavirin resistant mutant viruses. SPK has more than 14 years of experience working with HEV and has been awarded by the National Institute of Health (NIH) to study the pathogenesis of ribavirin resistant mutants in an immunosuppressed pig model. KKY and SPK have experiences with various animal models including but not limited to pigs, chickens, turkeys, rabbits, ferrets, mice, and hamsters.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yadav, K.K., Kenney, S.P. Hepatitis E virus immunosuppressed animal models. BMC Infect Dis 24, 965 (2024). https://doi.org/10.1186/s12879-024-09870-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09870-4