
Abstract
Background
Toll-Like receptors (TLRs) play an important role in the immune response during hepatitis B virus (HBV) infection. In this study, we evaluated the association between two SNP variants (TLR3 rs3775290 and TLR4 rs4986790) and susceptibility to chronic HBV infection in Mauritania.
Subjects and methods
: A total of 188 subjects were recruited for this study: 102 chronically infected patients and 86 individuals with spontaneously resolved HBV infection who were considered controls. Targeted PCR products were sequenced using Sanger sequencing.
Results
We found that TLR3 rs3775290 was significantly more frequent in patients with chronic HBV than in the control population (p = 0.03). However, no association was found between the TLR4 rs3775290 polymorphism and chronic infection.
Conclusion
Our results suggest that the TLR3 rs3775290 polymorphism may be a risk factor for susceptibility to chronic HBV infection in the Mauritanian population.
Similar content being viewed by others


Introduction
The WHO estimated that approximately 296 million people were affected by chronic hepatitis B virus (HBV) infection in 2019, with one of the highest burdens (81 million) found among African populations [1]. In Mauritania, although on a decreasing slope since the introduction of the hepatitis B virus (HBV) vaccination for children and newborns in 2000, the prevalence of hepatitis B surface antigen (HBsAg) remained relatively elevated, with more than 10% positivity in blood donors [2, 3]. A fraction of these cases, yet precisely undetermined, lead to HBV-related hepatocellular carcinoma (HCC) and cirrhosis [4,5,6].
Among the factors that control the course of HBV infection from spontaneous HBsAg seroclearance to long-term illness, the genetic background of the host is considered to be a major determinant of disease progression [7,8,9]. Numerous studies have indeed reported a connection between human Toll-Like receptors (TLRs) and HBV infection, for instance, the reduced expression of TLRs in patients with chronic hepatitis B [10, 11] or the effect of SNPs in TLRs on the immune control of HBV infection [12,13,14]. The main function of these receptors is to discern specific structurally conserved molecules derived from pathogens, called pathogen-associated molecular patterns (PAMPs), as well as endogenous molecules emitted from damaged cells (DAMPs) [15, 16]. The proposed mechanisms of their contribution to the outcome of HBV infection range from alteration of the extent of viral replication to activation of the body’s native immunity, leading to the development of an anti-HBV-specific adaptive response [17,18,19]. Despite the high prevalence of HBV infection in Mauritania and, globally, in sub-Saharan populations, data on the pathophysiological process of disease outcome and the role of TLRs remain scarce in our region. Data on TLR3 rs3775290 and TLR4 rs4986790 polymorphisms are often controversial with significant variability among different populations [13, 20,21,22]. TLR3 and TLR4 SNPs alter the interaction between the receptor and its ligand [23, 24]. A recent report have highlighted the association between TLR3 rs3775290 and TLR4 rs4986790 and chronic HBV infection within North African population [13]. Mauritania is known for its rich ethnic diversity, which includes multiple racial groups originating from both sub-Saharan Africa and North Africa [25].
In this study, we explored the relationship between TLR3 rs3775290 and TLR4 rs4986790 polymorphisms and susceptibility to chronic HBV infection in a cohort of Mauritanian HBV patients.
Subjects and methods
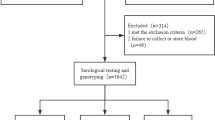
Sample size estimation was performed using an equation developed by Daniel (1999) [26]. It considered a 95% confidence interval [CI], a 5% margin of error, and an estimated prevalence of HBV at 10% [27]. The initial estimated sample size was 137 participants. However, to ensure sufficient statistical power for the analysis, the sample size was subsequently increased to 188 subjects previously infected with HBV.
The subjects included 102 patients with chronic HBV infection and 86 controls who had recovered spontaneously from the infection. Patients and controls were recruited at the National Institute of Hepato-Virology and the National Blood Transfusion Center, respectively, between 2020 and 2022. Chronic HBV patients were identified by the presence of HBsAg and HBV DNA for more than six months after their first positive blood test. Spontaneous hepatitis B seroclearance was tested in controls by HBsAg negativity in addition to hepatitis B core (total anti-HBc) and hepatitis B surface (anti-HBs) antibody-positive results. Patients were classified according to HBV viral load, alanine aminotransferase (ALT) levels and HBeAg status, as recommended by the European Association for the Study of the Liver (EASL). HBeAg negative chronic infection (inactive carriers) patients (N = 91) were identified by the absence of HBeAg, low levels of HBV DNA in the serum (< 2000 IU/mL) and consistently normal ALT levels. The HBeAg negative chronic hepatitis patients (N = 7) were characterized by HBeAg negativity, a high viral load (≥ 2000 IU/mL) and persistently elevated ALT levels. Patients with HBeAg positive chronic infection (immune tolerant) (N = 4) were characterized by the presence of HBeAg, high viral load and normal ALT levels.
HBV serological markers and alpha-fetoprotein (AFP) levels were analyzed using a commercial kit (Vidas®; Biomérieux Diagnostics, France). HBV viral load was quantified in patient plasma using the GeneXpert® System. Both patients and controls were negative for HCV and HIV. Blood alanine transaminase (ALT) levels were measured using a Biosystems A25 analyzer (BioSystems S.A., Barcelona, Spain).
The study was conducted in accordance with the Helsinki Declaration and was approved by the ethics committee of the University of Nouakchott (ethics clearance letter No002/2020/CE/UNA). Participants signed an informed consent questionnaire at the time of inclusion.
TLR3 and TLR4 genotyping
Whole blood was collected in EDTA tubes, and genomic DNA was extracted using the QIAamp.
DNA Blood Mini kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Agarose 2% electrophoresis and a NanoDrop spectrophotometer (Jenway, USA) were used to assess the purity and DNA concentration in samples.
TLR3 (1377 C > T) (rs3775290) and TLR4 (896 A > G) (rs4986790) polymorphisms were amplified using forward and reverse primers previously used by Cheng et al., 2007 and Pandey et al. [28, 29]. , in a final volume of 50 µl. The PCR mix consisted of 25 µl dNTP (200 µM, Invitrogen, Carlsbad, CA, USA), 2 µl of each primer (2 pmol/µl, Sigma‒Aldrich, Germany), 3.2 µl of genomic DNA template (30–100 ng/µl), 17.3 µl of ultrapure H2O, and 0.5 µl of DNA polymerase (0.25 U/µl, GreenTaq DNA Polymerase, GenScript, USA). A 2% agarose gel was used to visualize the PCR products.
PCR products were purified on a membrane before fluorometric quantification using Pico Green reagent (Invitrogen). All validated samples were then sequenced in both directions using an ABI 3730XL DNA sequencer by Genoscreen (Genoscreen, Inc., Lille, France).
Statistics
Continuous demographic variables were compared by Student’s t test or the Mann‒Whitney test when adequate. We used the χ2 test to evaluate categorical data between patients and controls. Allele and genotype frequencies of TLR3 rs3775290 and TLR4 rs4986790 were evaluated by direct counting. Genotype distributions of SNPs between the expected and observed genotypes were assessed using Hardy-Weinberg equilibrium (HWE). The χ2 test was used to analyze the genotype and allele distributions. The odds ratios (ORs) and 95% confidence intervals (95% CIs) were also calculated. Statistical analyses were performed using SPSS ver.25.0 software (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
Results
The demographic characteristics and liver function tests of the participants are summarized in Table 1. The mean age was 41 ± 1.03 years and 36 ± 0.96 years for the 102 chronic HBV patients and 86 healthy controls enrolled, respectively. Males represented the majority of the recruited subjects (55.9% of chronic HBV patients and 71.3% of healthy controls). Age and sex distributions differed significantly between patients and controls (p = 0.001 and p = 0.03, respectively). The mean viral load recorded here for chronic HBV patients was 2.45 ± 34.23 log10 IU/ml, while the average hepatic alanine transaminase (ATL) level was 26.9 ± 0.97 IU/l.
AFP levels have been shown to be associated with liver fibrosis [30]. In our chronic HBV patient cohort, the mean AFP level was 1.69 ± 0.99 ng/ml and there was no statistical difference in AFP levels (p = 0.14) among chronic HBV patients with different disease stages (Fig. 1).

AFP levels in chronic HBV patient at different disease stages (page 9–10
Genotype distribution showed that the chronic HBV and control groups were in Hardy-Weinberg equilibrium for both TLRs: TLR3 (1377 C > T) (rs3775290) and TLR4 (896 A > G) (rs4986790) SNPs (p > 0.05) (Table 2).
The allele frequencies of TLR3 and TLR4 polymorphisms in patients and healthy controls for each genotype are given in Table 3.
All three genotypes (CC, CT, and TT) were identified for the TLR3 (1377 C > T) (rs3775290) polymorphism (Fig. 2). Both patients and healthy control groups had the highest prevalence of the wild-type CC genotype (51% and 62%, respectively). The prevalence of the homozygous mutant TT genotype in HBV patients (12.7%) was significantly higher than that in controls (2%) (p = 0.03) (Table 3). This frequency was also higher in the chronic HBV infection group than in the non-TT genotype group. (P = 0.009) (Table 3).

Sanger sequencing chromatograms of the TLR3 rs3775290 and TLR4 rs4986790 polymorphisms. Arrows in panels A-C (left panel) show CC (wild type), TC (heterozygous) and TT (mutant) genotypes, respectively. The arrows in panels A-C (right panel) show AA (wild type), AG (heterozygous) and GG (mutant) genotypes, respectively. (page 9–10
Looking in allelic distribution, the prevalence of the C allele was 69% and 80% in HBV patients and controls, respectively (Table 4). The mutant T allele was significantly more prevalent in patients (31%) than in controls (20%) (OR = 0.57, 95% CI: 0.35–0.92, P = 0.02) (Table 4).
All three genotypes (AA, AG, and GG) were identified for the TLR4 (896 A > G) (rs4986790) polymorphism (Fig. 2). However, both genotype and allele analyses showed no significant difference in genotype and allele distribution between chronically infected patients and healthy controls (p = 0.11 and p = 0.57, respectively) (Tables 3 and 4).
The links between TLR3 and TLR4 SNPs and chronic HBV disease stages were examined and presented in Table 5. No statistically significant difference was observed in the frequency of the mutant TT genotype of the TLR3 rs3775290 among the various the HBV patient groups (p = 0.4). The homozygous mutant GG genotype of the TLR4 rs s4986790 was not detected in chronic HBV patients. Additionally, the frequency of AA genotype compared to non-AA genotype showed no significant variation among chronic HBV patients groups (p = 0.2).
Discussion
The role of TLRs in the host antiviral immune response during HBV infection has been extensively reviewed, particularly the disease manifestation from spontaneously resolved asymptomatic infection to long lasting chronic HBV infection [14, 31, 32]. In the first study exploring this effect in the Mauritanian population, 102 patients with chronic HBV infection and 86 controls were examined. The patient group mainly consisted of older males with normal ALT and AFP levels. The majority of patients had HBeAg negative chronic infection (inactive carriers), which is commonly seen in patients with chronic HBV infection in African regions [33, 34] and other parts of the world [35]. This HBV profile was generally associated with a positive prognosis and low severity of liver disease [36].
We showed that the TLR3 rs3775290 polymorphism was significantly associated with an increased probability of developing chronic HBV infection. The frequencies of both the minor T allele and TT homozygous genotype were indeed higher (p < 0.05) in chronic HBV infection carriers than in healthy controls. A similar result in our region has been reported for HBV infection in the Tunisian population; with a twofold higher risk of chronic HBV infection in TLR3 rs3775290 (T allele) carriers than in non-mutant controls [13]. This result is in agreement with previous studies showing a similar prevalence of various biomarkers of disease, reflecting the common ethnicity of the two populations [25]. Conversely, no overall risk of developing chronic HBV was found in the South China population, where the rs3775290 polymorphism of the TLR3 gene has a protective effect against the development of chronic HBV infection [22]. Our results were obtained using the reliable Sanger method in a reference sequencing facility (Genoscreen/France). Therefore, this inconsistency in HBV infection outcome between our population and the Chinese cohort may have resulted from differences in TLR3 rs3775290 levels in the respective populations. Worldwide, many studies have reported that variation in the level of genetic polymorphisms in populations of different ethnicities has an important role in disease susceptibility [9, 37, 38]. For instance, activation of the intracellular signaling pathway inducing TLR-mediated INF generation has been shown to play an important role in the natural course of HBV infection [19, 39], as revealed by the concomitant reduction in TLR3 expression and alteration of TNF-α in liver cell lines of chronic HBV patients compared to healthy controls [40]. In addition, restoration of TLR expression levels improved the immune response to HBV infection [41]. TLR3 deficiency has also been shown to increase the risk of other diseases, such as herpes simplex encephalitis and Coxsackie virus infection [42, 43], supporting the role of the TLR3-mediated immune response [44]. The difference in the prevalence of TLR3 rs3775291, another TLR3 variant, between chronic HBV patients and healthy Caucasian individuals with resolved infection was concluded to contribute to the lower risk of HBV persistence [45]. This polymorphism (substitution of G for A) changes leucine to phenylalanine at position 412. Its role in reducing antiviral immunity was explained by its action on TLR3 dimerization, resulting in reduced dsRNA binding affinity and, consequently, decreased production of interferon signaling activity. Because the TLR3 rs3775290 SNP (residue 459) was located in the same protein region, a comparable impact on transcriptional activity may be proposed here as also leading to a similar HBV infection in carriers of both SNPs. The TLR3 rs3775290 variant also showed conserved wild-type phenylalanine residues. Because silent mutations do not affect the amino acid sequence, they often have no observable effect on the phenotype. However, recent studies have suggested that these mutations may influence steps in the protein-making process, both in DNA transcription and translation of mRNA into proteins [44]. This process may be applicable to the impairment of TLR3 binding to dsRNA from pathogens that activate the immune response mentioned above.
Furthermore, the TLR3 rs3775290 polymorphism is a hotspot mutation [46]. The significantly higher occurrence of these mutations in highly conserved TLR receptors makes them very likely functional, and many examples of their role in various regulatory pathways have been reported [47, 48].
In the second Toll-like receptor explored in this study, we found no association between TLR4 (896 A > G) (rs4986790) and susceptibility to chronic HBV infection in the Mauritanian cohort, as no significant differences were observed in the distribution of genotypes (p = 0.11) and mutant alleles (p = 0.57) between chronic HBV patients and healthy controls. Similar results were reported by Pires-Neto et al., where TLR4 rs4986790 was not associated with chronic carriers of HBV or HCV infections [49]. Katrinli et al. also found no relationship between TLR4 variants and the persistence of HBV infection [20].
Conclusions
In this study, the TT mutant genotype of the TLR3 rs3775290 polymorphism was significantly associated with an increased risk of chronic HBV infection, whereas the TLR4 rs4986790 polymorphism was not associated with long-term HBV chronicity in the Mauritanian population. This result supports the key role of this class of receptors in the immune response during HBV infection. No effect of the TLR4 (896 A > G) (rs4986790) polymorphism on the disease outcome was observed in this study. Further studies should include investigating the impact of these SNPs on HBV-related diseases such as liver cirrhosis and hepatocellular carcinoma. Additionally, it is important to examine the role of hepatitis D virus (HDV) as an aggravating factor in these diseases. Implication of TLR variants could also be carried out as part of the action against the spread of HBV infection, which remains prevalent in our region.
Limitations
A limitation of this study is that we did not assess the interaction between TLR3 SNP rs3775290 frequency and the level of known HBV infection biomarkers such as HBeAg and HBsAg both in chronic HBV patients and individuals with spontaneous clearance of HBV. These markers may inhibit TLR-induced antiviral activity, as evidenced by decreased activation of IRF-3, NF-κB and ERK1/2 in hepatic non-parenchymal cell (NPC) supernatants containing HBsAg, HBeAg, and HBV virions.
Data availability
The datasets generated and/or analyzed during the current study are available in the SRA repository, PRJNA1013319.
Abbreviations
- ALT:
-
Alanine transaminase
- CI:
-
Confidence intervals
- DAMP:
-
Damage-associated molecular patterns
- DNA:
-
Deoxyribonucleic acid
- HBsAg:
-
Hepatitis B surface antigen
- HBV:
-
Hepatitis B virus
- HCC:
-
Hepatocellular carcinoma
- HCV:
-
Hepatitis C virus
- HIV:
-
Human immunodeficiency virus
- HWE:
-
Hardy-Weinberg equilibrium
- INF:
-
Interferons
- NPC:
-
Non-parenchymal cell
- OR:
-
Odds ratios
- PAMP:
-
Pathogen-associated molecular patterns
- PCR:
-
Polymerase chain reaction
- RNA:
-
Ribonucleic acid
- SNP:
-
Single-nucleotide polymorphism
- TLR:
-
Toll-Like receptor
- TNF-α:
-
Tumor necrosis factor-alpha
References
Hepatitis B. data 2019. [cited 2022 Nov 25]. https://www.who.int/news-room/fact-sheets/detail/hepatitis-b.
Mansour W, Bollahi MA, Hamed CT, Brichler S, Le Gal F, Ducancelle A, et al. Virological and epidemiological features of hepatitis delta infection among blood donors in Nouakchott, Mauritania. J Clin Virol. 2012;55(1):12–6.
Boushab BM, Melaïnine Mohamed Limame OC, Zahra FMF, Mamoudou S, Roseline Darnycka BM, Saliou SM. Estimation of seroprevalence of HIV, hepatitis B and C virus and syphilis among blood donors in the hospital of Aïoun, Mauritania. Pan Afr Med J. 2017 [cited 2023 Jul 1];28. http://www.panafrican-med-journal.com/content/article/28/118/full/.
Suzuki Y, Maekawa S, Komatsu N, Sato M, Tatsumi A, Miura M, et al. Hepatitis B virus (HBV)-infected patients with low hepatitis B surface antigen and high hepatitis B core‐related antigen titers have a high risk of HBV‐related hepatocellular carcinoma. Hepatol Res. 2019;49(1):51–63.
Nguyen VTT, Law MG, Dore GJ. Hepatitis B-related hepatocellular carcinoma: epidemiological characteristics and disease burden. J Viral Hepat. 2009;16(7):453–63.
Bixler D, Zhong Y, Ly KN, Moorman AC, Spradling PR, Teshale EH, et al. Mortality among patients with chronic Hepatitis B infection: the chronic Hepatitis Cohort Study (CHeCS). Clin Infect Dis. 2019;68(6):956–63.
Ma Z, Zhang E, Yang D, Lu M. Contribution of toll-like receptors to the control of hepatitis B virus infection by initiating antiviral innate responses and promoting specific adaptive immune responses. Cell Mol Immunol. 2015;12(3):273–82.
King H, Xing J, Dean HD, Holtzman D. Trends in Prevalence of protective levels of Hepatitis B surface antibody among adults aged 18–49 years with risk factors for Hepatitis B Virus infection—United States, 2003–2014. Clin Infect Dis. 2020;70(9):1907–15.
Zhang Z, Wang C, Liu Z, Zou G, Li J, Lu M. Host genetic determinants of Hepatitis B Virus infection. Front Genet. 2019;10:696.
Chen Z, Cheng Y, Xu Y, Liao J, Zhang X, Hu Y, et al. Expression profiles and function of toll-like receptors 2 and 4 in peripheral blood mononuclear cells of chronic hepatitis B patients. Clin Immunol. 2008;128(3):400–8.
Li N, Li Q, Qian Z, Zhang Y, Chen M, Shi G. Impaired TLR3/IFN-β signaling in monocyte-derived dendritic cells from patients with acute-on-chronic hepatitis B liver failure: relevance to the severity of liver damage. Biochem Biophys Res Commun. 2009;390(3):630–5.
Kayesh MEH, Kohara M, Tsukiyama-Kohara K. Toll-like receptor response to Hepatitis B Virus infection and potential of TLR agonists as Immunomodulators for Treating Chronic Hepatitis B: an overview. Int J Mol Sci. 2021;22(19):10462.
Sghaier I, Zidi S, Mouelhi L, Ghazoueni E, Brochot E, Almawi WY et al. TLR3 and TLR4 SNP variants in the liver disease resulting from hepatitis B virus and hepatitis C virus infection. Br J Biomed Sci. 2018 Dec 3 [cited 2022 Jun 23]; https://www.tandfonline.com/doi/abs/https://doi.org/10.1080/09674845.2018.1547179.
Al-Qahtani A, Al-Ahdal M, Abdo A, Sanai F, Al-Anazi M, Khalaf N, et al. Toll-like receptor 3 polymorphism and its association with hepatitis B virus infection in Saudi Arabian patients. J Med Virol. 2012;84(9):1353–9.
El-Zayat SR, Sibaii H, Mannaa FA. Toll-like receptors activation, signaling, and targeting: an overview. Bull Natl Res Cent. 2019;43(1):187.
Kawai T, Akira S. Toll-like receptors and their crosstalk with other Innate receptors in infection and immunity. Immunity. 2011;34(5):637–50.
Du Y, Wu J, Liu J, Zheng X, Yang D, Lu M. Toll-like receptor-mediated innate immunity orchestrates adaptive immune responses in HBV infection. Front Immunol. 2022;13:965018.
Ait-goughoulte M, Lucifora J, Zoulim F, Durantel D. Innate antiviral Immune responses to Hepatitis B Virus. Viruses. 2010;2(7):1394–410.
Zhang E, Lu M. Toll-like receptor (TLR)-mediated innate immune responses in the control of hepatitis B virus (HBV) infection. Med Microbiol Immunol (Berl). 2015;204(1):11–20.
Katrinli S, Nigdelioglu A, Ozdil K, Dinler-Doganay G, Doganay L. The association of variations in TLR genes and spontaneous immune control of hepatitis B virus. Clin Res Hepatol Gastroenterol. 2018;42(2):139–44.
Wu JF, Chen CH, Ni YH, Lin YT, Chen HL, Hsu HY, et al. Toll-like receptor and Hepatitis B Virus Clearance in Chronic Infected patients: a long-term prospective cohort study in Taiwan. J Infect Dis. 2012;206(5):662–8.
Huang X, Li H, Wang J, Huang C, Lu Y, Qin X, et al. Genetic polymorphisms in toll-like receptor 3 gene are associated with the risk of hepatitis B virus-related liver diseases in a Chinese population. Gene. 2015;569(2):218–24.
Pandey S, Mittal B, Srivastava M, Singh S, Srivastava K, Lal P, et al. Evaluation of toll-like receptors 3 (c.1377 C/T) and 9 (G2848A) gene polymorphisms in cervical cancer susceptibility. Mol Biol Rep. 2011;38(7):4715–21.
Cussigh A, Fabris C, Fattovich G, Falleti E, Cmet S, Bitetto D, et al. Toll like receptor 4 D299G Associates with Disease Progression in caucasian patients with chronic HBV infection: relationship with gender. J Clin Immunol. 2013;33(2):313–6.
Hamed CT, Meiloud G, Veten F, Hadrami M, Ghaber SM, Boussaty EC, et al. HLA class I (-A, -B, -C) and class II (-DR, -DQ) polymorphism in the Mauritanian population. BMC Med Genet. 2018;19(1):2.
Metcalfe C, Biostatistics WW, Daniel. Wiley, 1999. No. of. pages: xiv + 755 + appendices. Price: £28.95. ISBN 0-471-16386-4. Stat Med. 2001;20(2):324–6.
Polaris Observatory Collaborators. Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: a modelling study. Lancet Gastroenterol Hepatol. 2023;8(10):879–907.
Cheng PL, Eng HL, Chou MH, You HL, Lin TM. Genetic polymorphisms of viral infection-associated toll-like receptors in Chinese population. Transl Res. 2007;150(5):311–8.
Pandey NO, Chauhan AV, Raithatha NS, Patel PK, Khandelwal R, Desai AN, et al. Association of TLR4 and TLR9 polymorphisms and haplotypes with cervical cancer susceptibility. Sci Rep. 2019;9(1):9729.
Yang K, Pan Y, Liu L, Sun B, Shi W. Serum Alpha-Fetoprotein as a predictor of liver fibrosis in HBeAg-Positive chronic Hepatitis B patients. Med (Mex). 2023;59(5):923.
Xu Y, Xue W, Gao H, Cui J, Zhao L, You C. Association of toll-like receptors single nucleotide polymorphisms with HBV and HCV infection: research status. PeerJ. 2022;10:e13335.
An P, Xu J, Yu Y, Winkler CA. Host and viral genetic variation in HBV-Related Hepatocellular Carcinoma. Front Genet. 2018;9:261.
Riches N, Vinikoor M, Guingane A, Johannessen A, Lemoine M, Matthews P, et al. Hepatitis B in Africa Collaborative Network: cohort profile and analysis of baseline data. Epidemiol Infect. 2023;151:e65.
Somé EN, Guingané AN, Zongo I, Sané D, Drabo KM, Sombié R. Chronic viral HBeAg-negative hepatitis B: Epidemiological, clinical and biochemical characteristics in an outpatient descriptive cohort in Burkina Faso. Clin Epidemiol Glob Health. 2021;11:100799.
Chevaliez S, Roudot-Thoraval F, Brouard C, Gordien E, Zoulim F, Brichler S, et al. Clinical and virological features of chronic hepatitis B in the French national surveillance program, 2008–2012: a cross-sectional study. JHEP Rep. 2022;4(12):100593.
Manno M, Cammà C, Schepis F, Bassi F, Gelmini R, Giannini F, et al. Natural history of chronic HBV carriers in northern Italy: morbidity and mortality after 30 years. Gastroenterology. 2004;127(3):756–63.
Chiarella P, Capone P, Sisto R. Contribution of genetic polymorphisms in Human Health. Int J Environ Res Public Health. 2023;20(2):912.
Yan ZH, Fan Y, Wang XH, Mao Q, Deng GH, Wang YM. Relationship between HLA-DR gene polymorphisms and outcomes of hepatitis B viral infections: a meta-analysis. World J Gastroenterol WJG. 2012;18(24):3119–28.
Takeuchi O, Akira S. Pattern Recognition Receptors and inflammation. Cell. 2010;140(6):805–20.
Huang YW, Lin SC, Wei SC, Hu JT, Chang HY, Huang SH, et al. Reduced toll-like receptor 3 expression in Chronic Hepatitis B patients and its restoration by Interferon Therapy. Antivir Ther. 2013;18(7):877–84.
Deng G, Ge J, Liu C, Pang J, Huang Z, Peng J, et al. Impaired expression and function of TLR8 in chronic HBV infection and its association with treatment responses during peg-IFN-α-2a antiviral therapy. Clin Res Hepatol Gastroenterol. 2017;41(4):386–98.
Guo Y, Audry M, Ciancanelli M, Alsina L, Azevedo J, Herman M, et al. Herpes simplex virus encephalitis in a patient with complete TLR3 deficiency: TLR3 is otherwise redundant in protective immunity. J Exp Med. 2011;208(10):2083–98.
Richer MJ, Lavallée DJ, Shanina I, Horwitz MS. Toll-Like Receptor 3 Signaling on Macrophages Is Required for Survival Following Coxsackievirus B4 Infection. Means T, editor. PLoS ONE. 2009;4(1):e4127.
Gosu V, Son S, Shin D, Song KD. Insights into the dynamic nature of the dsRNA-bound TLR3 complex. Sci Rep. 2019;9(1):3652.
Fischer J, Koukoulioti E, Schott E, Fülöp B, Heyne R, Berg T, et al. Polymorphisms in the toll-like receptor 3 (TLR3) gene are associated with the natural course of hepatitis B virus infection in caucasian population. Sci Rep. 2018;8(1):12737.
Wang BG, Yi DH, Liu YF. TLR3 gene polymorphisms in cancer: a systematic review and meta-analysis. Cancer Commun. 2015;34(3):19.
Miller ML, Reznik E, Gauthier NP, Aksoy BA, Korkut A, Gao J, et al. Pan-cancer analysis of mutation hotspots in protein domains. Cell Syst. 2015;1(3):197–209.
Mitchell AL, Attwood TK, Babbitt PC, Blum M, Bork P, Bridge A, et al. InterPro in 2019: improving coverage, classification and access to protein sequence annotations. Nucleic Acids Res. 2019;47(D1):D351–60.
Pires-Neto O, de Gomes S. STM. Lack of association between polymorphisms of the TLR4 gene and infection with the Hepatitis B and C viruses. Mediators Inflamm: 7.
Acknowledgements
This work was partially supported by the National Agency for Scientific Research and Innovation.
We thank the director of the National Blood Transfusion Center and all the workers there for their help.
Funding
This study was not funded.
Author information
Authors and Affiliations
Contributions
TS collected and organized patient files for genotyping and contributed to statistical analysis and manuscript writing. CB analyzed sequencing data; CH, FV, ZM and MY contributed to genotyping and statistical analysis; MH, AD; and MM carried out patient and control clinical assessments; AH carried out manuscript design and writing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the Helsinki Declaration and approved by the ethics committee of the University of Nouakchott (ethics clearance letter No002/2020/CE/UNA). Participants signed an informed consent questionnaire at the time of inclusion.
Consent for publication
Informed consent was obtained from all study participants. Informed consent of all patients was also obtained for data publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Soumbara, T., Bonnet, C., Hamed, C.T. et al. Genetic variation of TLR3 gene is associated with the outcome of hepatitis b infection in mauritanian patients: case control study. BMC Infect Dis 24, 616 (2024). https://doi.org/10.1186/s12879-024-09503-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09503-w