
Abstract
Aim
Diarrhea is a common disease in immunocompromised patients and can be associated with greater morbidity and even mortality. Therefore, the present study was designed to determine the prevalence of Aeromonas spp., Campylobacter spp., and C. difficile among immunocompromised children.
Methods
This study was conducted on 130 stool samples from patients with diarrhea who had defects in the immune system and were referred to Hazrat Masoumeh Children’s Hospital in Qom. Demographic information, clinical symptoms, immune status, and duration of chemotherapy were also recorded for each child. DNAs were extracted from the stool, and then direct PCR assays were done by specific primers for the detection of Aeromonas spp., Campylobacter spp., and toxigenic C. difficile, including tcdA/B and cdtA/B genes. Co-infection in patients was also evaluated.
Results
60.8% and 39.2% were male and female, respectively, with a m ± SD age of 56.72 ± 40.49 months. Most cases of immunocompromised states were related to Acute Lymphocytic Leukemia (77.7%) and Non-Hodgkin Lymphoma (14.6%). 93.1% of patients were undergoing chemotherapy during the study. Among patients, most clinical symptoms were related to bloody diarrhea (98.5%) and fever (92.3%). Based on PCR, 14.6, 9.2, and 1.5% were positive for Aeromonas spp., C. difficile, and C. jejuni, respectively. Among the C. difficile-positive cases, the tcdA gene was only detected in one patient. In total, three co-infections were identified, which included Aeromonas spp./C. difficile (tcdA+), C. jejuni/C. difficile, and C. jejuni/Aeromonas spp.
Conclusions
This is the first study in Iran to investigate the simultaneous prevalence of some pathogens in immunocompromised children with diarrhea. Because Aeromonas spp., Campylobacter spp., and C. difficile are not routinely detected in some laboratories, infections caused by them are underappreciated in the clinic. Our results showed that these pathogens are present in our region and can cause gastroenteritis in children, especially those with underlying diseases. Therefore, increasing the level of hygiene in some areas and controlling bacterial diarrheal diseases should be given more attention by health officials.
Similar content being viewed by others

Introduction
Infectious diarrhea is one of the most common gastroenterological diseases and a major problem worldwide. It is one of the most important causes of death, especially in children, in developed and developing countries [1,2,3,4]. In addition, patients with underlying conditions, such as an immunocompromised state, are at a higher risk for severe gastroenteritis infections caused by bacteria, viruses, fungi, and parasites, and the incidence of symptoms and lethality is higher than that of healthy people [5,6,7]. The most important bacteria causing diarrhea include Campylobacter spp., Salmonella spp., Shigella spp., Yersinia enterocolitica, Vibrio cholerae, Aeromonas spp., Clostridioides difficile, and intestinal pathotypes of Escherichia coli [8,9,10].
The genus Aeromonas (A.), with 36 species, belongs to the Aeromonadaceae family. These are rod-shaped, Gram-negative, and facultative anaerobic bacteria. This genus consists of mesophilic and psychrophilic bacteria that can grow in a wide range of temperatures from 10 to 42 °C. As environmental opportunists, these bacteria cause disease in a wide range of hosts, including humans, aquatic and terrestrial animals [11]. A. hydrophila, A. caviae, A. veronii biovar sobria, A. dhakensis, and A. trota are the most important species isolated from human feces [12]. In addition, these species can cause bacteremia, cellulitis, urinary tract infection, wound infection, and gastroenteritis in immunocompromised hosts. Gastrointestinal manifestations caused by these bacteria vary from mild diarrhea to cholera-like watery diarrhea and Shigella-like dysentery [13, 14]. Intestinal infection caused by these bacteria is mainly seen in children, adolescents, and people with underlying states, affecting 2–13% of children, 2–7% of adults with healthy immunity, and up to 13% of patients with immunocompromised states [15].
Clostridioides difficile (C. difficile), belongs to the Clostridiaceae family, is a Gram-positive, obligate anaerobic, rod-shaped, and spore-forming enteric bacterium. Strains producing toxins A (enterotoxin) and B (cytotoxin) are known as hospital-acquired pathogens and the causative agent of colitis and antibiotic-associated diarrhea. The symptoms and severity of the disease vary from simple colonization to the formation of the pseudomembranes on the colonic mucosal surfaces, sepsis, shock, and death [1, 16]. According to reports, immunocompromised people are more susceptible to C. difficile infections (CDIs) and show more severe clinical manifestations of this disease. In recent years, CDI cases have been increasing in hospitalized cancer patients, especially children, and have reached 25%. Many factors such as continuous contact with broad-spectrum antibiotics, inherent antimicrobial activity of some chemotherapy regimens, high contact with medical care devices, and the inhibitory effect of chemotherapy on the immune system increase the risk of CDIs in children [10, 17].
The genus Campylobacter (C.), belongs to the Campylobacteraceae family, comprises Gram-negative, motile, curved or spiral bacteria and can be seen in V or S shapes. These account for cases of gastroenteritis in developed and developing countries and causes a disease called campylobacteriosis. The most common species causing infection in humans are C. jejuni and C. coli with prevalence rates of about 90 and 10%, respectively [18,19,20]. This disease is a zoonotic disease and the main routes of its transmission to humans is through the consumption of contaminated water, vegetables, and food (including beef, pork, birds, and unpasteurized milk) [21]. The incubation period of the disease is 2–5 days and gastroenterological symptoms include diarrhea (which may be bloody), headache, nausea, vomiting, cramp, abdominal pain, cholecystitis, and fever [22]. Although Campylobacter infection is mostly non-fatal, there have been reports of patient deaths. For example, about 124 deaths caused by this infection are reported annually in the United States, and this rate is higher in developing countries [23]. Statistics also show that the prevalence of infection is high (even higher than shigellosis), especially in children under 5 years of age in developed and developing countries [24]. Prolonged infections and extra-intestinal manifestations caused by these bacteria have also been reported in patients with underlying conditions [25, 26].
Therefore, our aim was to detect the simultaneous presence of Aeromonas spp., C. jejuni, C. coli, and C. difficile in immunocompromised children with diarrhea, referred to a specialized children’s hospital using direct PCR, which was done for the first time in Iran.
Methods
Patients and sampling
This research was conducted on 130 immunocompromised patients with infectious gastrointestinal symptoms referred to Hazrat Masoumeh Children’s Hospital in Qom between 2018 and 2019. Sample size calculation was calculated considering the results of the Boustanshenas et al. study [27], which estimated the prevalence of Aeromonas spp. at 2.3%, confidence interval 95%, and error 0.03. Therefore, the minimum sample size was estimated to be 98 patients, and to increase the precision, 130 patients we enrolled in this study. Our inclusion criteria included consent, underlying disease, symptoms of infectious diarrhea, and no antibiotic use during diarrhea. Briefly, after obtaining written informed consent from the patients or their parents/guardians, 1 ml of fecal sample from each child was collected in a sterile container and then sent to the Cellular and Molecular Research Center of the university and stored at -20 °C until testing. In a questionnaire, demographic information, type of underlying disease, history of chemotherapy, and gastrointestinal symptoms for each patient including age, gender, travel, contact with animals, swimming, duration of diarrhea (days), bowel movements/day, fever, blood in feces, vomiting, cramp, and abdominal pain as well as some laboratory findings, were recorded.
DNA extraction and polymerase chain reaction (PCR) for direct diagnosis of infections
From the stool samples, DNA was extracted by a modified method provided by Yang et al. [28]. Briefly, 200 µl of stool was centrifuged at 10,000 g for 5 min. The obtained supernatant was transferred to a new microtube and then centrifuged again at 13,000 g for 10 min. Next, in order to remove the PCR inhibitors, the precipitate was washed three times with acetone (each time, centrifugation was performed at 13,000 g for 10 min). In the last step, the supernatant was discarded, and 200 µl of sterile distilled water was added to the pellet. Genome extractions were done using the boiling method and stored at -20 °C until PCR.
Molecular identification of C. jejuni and C. coli was performed by the duplex-PCR method described in our previous study [29] for the cadF gene, while C. difficile and Aeromonas spp. were detected by separate PCRs based on other articles using cdd3 and 16 S rRNA genes, respectively. The final volume of each reaction was 25 µL, including 10 µL of 1X Master mix (Ampliqon, Denmark), 1 µL of primers (10 pmol/µL) (Table 1), 3 µL of extracted DNA, and 10 µL of deionized water.
The amplification process consisted of an initial denaturation at 95 °C for 3 min (1 cycle), followed by 33 cycles including denaturation at 95 °C for 30 s, annealing temperature (Table 1), and elongation at 72 °C for 30 s. The final elongation step was performed at 72 °C for 5 min (1 cycle) (Thermocycler; Eppendorf, Hamburg, Germany). Aeromonas hydrophila ATCC 7966, C. difficile VPI10463, C. coli ATCC 43,478, and C. jejuni ATCC 29,428 were used as positive controls in the PCRs. The isolates that were positive for the cdd3 gene in PCR were re-evaluated for the presence of toxigenic genes tcdA, tcdB, cdtA, and cdtB. The PCR products were loaded on a 1% agarose gel and evaluated by a gel documentation device with UV light (Thermo Fisher Scientific, USA).
Statistical analysis
Results were reported using descriptive statistics including mean ± standard deviation (m ± SD) as well as frequency and frequency percentage. The frequency distribution of clinical symptoms and laboratory findings as well as the rate of infection and their comparison with other qualitative demographic variables, including the gender of the patients, were done using Fisher’s Exact and Chi-Square Tests. Independent t-test was also used to compare quantitative variables such as age in two groups of subjects. Statistical analysis was performed in SPSS 22 software (IBM, NY, USA) at a significance level of less than 0.05.
Results
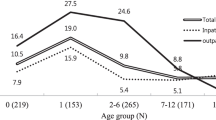
The m ± SD age of the patients was 56.72 ± 40.49 months, and 60.8% of whom were male (m ± SD age = 58.58 ± 43.99 months). Among them, 101 (77.7%), 19 (14.6%), and 10 (7.7%) had acute lymphocytic leukemia (ALL), non- Hodgkin lymphoma (NHL), and retinoblastoma cancer, respectively. 121 patients (93.1%) were undergoing chemotherapy during the study (with the m ± SD of 15.04 ± 11.95 months). In terms of clinical symptoms recorded in the questionnaire, 128 (98.5%), 120 (92.3%), 115 (88.5%), 98 (75.4%), 80 (61.5%), and 55 (42.3%) patients had bloody diarrhea, fever, anorexia, vomiting, weight loss, and cramp, respectively. The m ± SD of the number of days of diarrhea in our patients was determined as 2.93 ± 1.40 with a range of 1–9 bowel movements per day. None of the patients and their parents had detailed information about the consumption of contaminated food and water, the contact with animals, and travel related to the disease. According to the laboratory report of our hospital, the patient’s stool cultures were negative for Shigella spp., Salmonella spp., and Escherichia coli O157:H7.
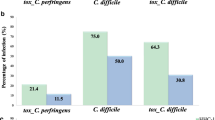
Among the patients, 19 (14.6%) cases were diagnosed as positive for infection with Aeromonas spp., of which 57.9% were male and 42.1% were female (with a m ± SD age of 55.31 ± 46.35 months). There was no significant relationship between age and gender with Aeromonas infection (P > 0.05). The duration of diarrhea among Aeromonas-positive patients showed 2.73 ± 1.28 days (mean of 5.05 bowel movements/day). 94.7% of them had bloody diarrhea and 3.5% had watery diarrhea. In addition, 94.7, 84.2, 68.4, 52.6, 42.1, and 78.9% of Aeromonas-infected patients had anorexia, fever, weight loss, cramp, abdominal pain, and vomiting, respectively, but no significant relationship between the presence of infection and clinical findings. The presence of Aeromonas infection in patients with ALL accounted for the most cases (73.7%), followed by NHL with 21.0%. According to the season, the highest positive rate was related to autumn with 13 cases (68.0%), followed by winter with 4 cases (21.0%), and summer with 2 cases (11.0%). No significant difference between the number of positive cases of Aeromonas spp. with the autumn season was obtained (P = 0.631).
Of the 130 children, 12 cases (9.2%) were positive for C. difficile with a m ± SD age of 75.0 ± 52.51 months. 58.3% of them were female, and 41.7% were male. Among them, one case was infected with a toxin-producing strain (tcdA+) and no case of the presence of double genes (tcdA/B and cdtA/B) was observed. The duration of diarrhea in patients was recorded as 3.83 ± 2.28 days (mean of 4.5 bowel movements/day). All patients (100.0%) had bloody diarrhea and abdominal pain, while 83.3% and 66.6% had anorexia and weight loss, respectively. In C. difficile-infected patients, ALL was diagnosed in 66.6% and NHL in 25.0%. According to the season, the highest positive rate was related to autumn (6 cases-50.0%), followed by winter and summer (3 cases each-25.0%), with a significant relationship between autumn and infection. In one case (0.76%), co-infection of Aeromonas spp. and toxigenic C. difficile (tcdA+) was detected.
Among our patients, 2 cases (1.5%) were positive for C. jejuni with the m ± SD age of 11.0 ± 0.0 months, and C. coli was not detected in any case. Both patients were infected in autumn, and were female and ALL+. All patients had bloody diarrhea with an average duration of 1.50 ± 0.70 days (mean of 6.5 bowel movements/day). In terms of clinical symptoms, fever, anorexia, and weight loss were seen in all of the cases, while cramp and abdominal pain were not observed in any of them. Interestingly, both C. jejuni-positive patients had a co-infection, one with non-toxigenic C. difficile and the other with Aeromonas spp.
Discussion
Bacterial gastroenteritis is one of the most important causes of health problems and even death of the elderly and children in different countries [35, 36]. Infectious diarrhea is very important in patients with special immune states in all age groups, especially those who are immunocompromised [37,38,39]. Of these, bacteria account for a significant number of infections and are considered the main cause of diarrheal disease [8, 15]. Few studies have been reported in the world about the incidence of diarrhea caused by Aeromonas spp., C. jejuni, C. coli, and toxigenic C. difficile among patients with underlying disorders. Part of the underreporting is due to the lack of isolation of these bacteria. Various methods are used to identify infectious agents, from conventional methods to rapid tests [19, 40, 41] and due to the special growth conditions of our target bacteria and the lack of molecular facilities in most clinical laboratories, the infection caused by them is not well diagnosed. Therefore, our aim was to simultaneously investigate the infection caused by them among immunocompromised hosts with diarrhea for the first time in Iran.
Our results showed that 14.6% of children with blood malignancies were positive for Aeromonas spp. infection, which was similar to other studies conducted among patients with special immune conditions. In a study by Obi et al., in Limpopo, South Africa, Aeromonas species were identified in 13.3% of HIV-infected patients with chronic diarrhea in a rural area [42]. In another study in Spain, patients with various diseases, including hematological malignancies, cirrhosis of the liver, hospitalized in ICU, organ transplants, and HIV+, were identified with a variety of Aeromonas infections, most of them had Aeromonas gastroenteritis [43]. Also, reports of rare species of Aeromonas in patients with special conditions are interesting. For example, Ana Fernández-Bravo et al. identified Aeromonas trota in the diarrhea sample of a 69-year-old Spanish woman with a history of ovarian cancer [15].
Although there has been no report on the prevalence of diarrhea caused by Aeromonas spp. in children with cancer in Iran, only a few researches in this field have been conducted on this age group with normal immune system. In some studies, the prevalence of Aeromonas spp. was 3.1% in Tehran [44], 0.5% in Zanjan and Qazvin [45], and 1.0% in Arak [46]. In the study done by Rahimi-Larki et al. on samples of children with diarrhea in India (2006), only 1.0% of the patients were positive for A. hydrophila [47]. In a study conducted in some Asian countries and several locations in Africa, the relationship between Aeromonas and the incidence of moderate-to-severe diarrhea (MSD) in children under 5 years of age was investigated, and their results showed that 22.2% of cases were positive [48].
According to the season, the highest positive rate was related to the autumn with 13 cases (68.0%), followed by winter with 4 cases (21.0%). This result is similar to the results obtained by Ghenghesh et al. in Libya, where the highest positive rate of Aeromonas was determined in autumn with 20.8% and in winter with 11.9% [49].
In our study, 9.2% of diarrheal samples were positive for C. difficile, and only in one case, the tcdA toxin gene was detected. A study by Zargar et al. in Qom, which surveyed C. difficile infection in adults with diarrhea, showed that 11 out of 68 patients were positive for this bacterium [50]. Other studies have been carried out in the presence of C. difficile in the feces of hospitalized patients in the world as well as in Iran. In Hematyar’s study in northeastern Iran, 4.7% of stool samples from patients hospitalized in several hospitals were positive for C. difficile [51]. In the study by Armin et al. in Tehran, C. difficile was detected in 45.2% of hospitalized children with diarrhea [52]. In a study in Kenya, 37.6% of children with diarrhea under 5 years of age [53], and in Brazil, 5.5% of children with acute diarrhea were positive for this bacterium [54].
Reports of C. difficile infections in immunocompromised children are rare worldwide. In a study conducted in Tehran (2008–2009), out of 152 children with underlying conditions, 25% were positive for C. difficile by culture, and 92% of these isolates harbored toxins A and B [55]. In another study in Tehran (2011–2012), C. difficile was detected in 17.14% of stool samples of children with cancer by multiplex PCR method, and 72% of the isolates were toxin-producing strains. Among their strains, A−/B+ (8 cases) were detected more than A+/B− (4 cases) [56]. Price and colleagues in Canada investigated the incidence and characteristics of CDI in children with acute myeloid leukemia (AML). CDI occurred in only 11.0% of children undergoing chemotherapy for AML, suggesting that the prevalence of CDI and its associated outcomes is not an important issue in children with AML [57].
In our study, the prevalence of C. jejuni was 1.5%, where both children were 11 months old and had ALL. Several studies have been conducted to investigate the prevalence of Campylobacter in children with a normal immune system in Iran and the world. Ghorbanalizadgan et al. in Iran found the prevalence of Campylobacter in children under 5 years to be 4%, of which 94% were C. jejuni and 6% were C. coli [58]. Terefe et al. in Ethiopia detected the prevalence of Campylobacter in children under 2 years old by PCR method to be 50% [59]. In Ecuador, the prevalence of this bacterium in healthy children was 13.4% [60]. Samie et al. in South Africa showed the prevalence of Campylobacter in children with diarrhea (13.2%) and without diarrhea (12.4%) [61].
The prevalence of Campylobacter spp. in children with the underlying disease has been investigated in limited studies worldwide. In a study in Pennsylvania, zoonotic infections in children with acute leukemia were investigated, and Campylobacter enteritis was one of the causes of infection among the patients [62]. Some other studies have presented reports of extraintestinal cases of Campylobacter species. For example, Anvarinejad in Iran identified bacteremia caused by C. jejuni in a 14-year-old child with ALL who was undergoing chemotherapy [63]. In a case report in Italy, C. jejuni was detected in the blood of two 4- and 7-year-old children with ALL [64]. Recurrent C. jejuni bacteremia was also reported in an 18-year-old patient with hypogammaglobulinemia in South Korea [65].
Infectious diseases are usually caused by one type of pathogen. In some cases, infections with two or more pathogens is observed [66]. Co-infections for the outcome of a disease, depending on the level of interactions such as fluctuating host immune response, and drug/diagnostic interventions can be detrimental, insignificant, or beneficial [67]. In our study, co-infections of C. jejuni with non-toxigenic C. difficile and Aeromonas spp.; and Aeromonas spp. with toxigenic C. difficile were observed in three patients. It seems that the cause of this co-infection can be related to the immunocompromised states of our patients due to cancer and as well as chemotherapy. These co-infections in children suffering from cancer and with gastrointestinal symptoms have not been discussed either in the world. However, co-infections from these bacteria have been reported in hosts with a normal immune system. Barati et al. in Iran reported that 3.5% of Campylobacter-positive children were co-infected with intestinal parasites [68]. De Graaf et al. reviewed co-infections in children with diarrhea who tested positive for C. difficile. In their study, the percentage of co-infections reported in C. difficile-positive children was 20.7% [69]. In addition, Vasilev and colleagues in Bulgaria identified three intestinal pathogens, including A. hydrophila, C. difficile, and rotavirus in the feces of a 41-year-old female patient who had recurrent diarrhea and abdominal pain [70].
Conclusion
This is the first study that investigates the simultaneous presence of a number of important bacteria, including Aeromonas spp., C. jejuni, C. coli, and toxigenic C. difficile, in children with immunocompromised states who have diarrhea. Although there was no significant relationship between the type of infection and other variables, our results showed that these bacteria have a relatively low prevalence in our region and their presence is important and can cause gastroenteritis in children, especially during underlying diseases. Co-infections with these bacteria were also significant for us. It seems that clinical laboratories should pay more attention to the isolation and identification of these bacteria. Improving the level of hygiene and increasing monitoring of food and water can be effective in controlling diarrheal diseases caused by bacteria. In addition, it is recommended to investigate the origin of these bacteria along with the evaluation of their virulence factors in future studies. Also, most of the patients were undergoing chemotherapy during this study, and the presence of bloody or watery diarrhea may be due to the side effects of this therapeutic procedure. This is a confounding variable and needs further investigation in further research. In addition, viral agents or other pathogens could also have caused the disease in our patients, which is under investigation in our future project. Since asymptomatic colonization with some bacteria is common, it is recommended to perform quantitative-PCR to distinguish infection from colonization in subsequent studies.
Limitations of the study
One of our limitations was not using conventional methods to isolate target bacteria due to their fastidious nature and time constraints. Investigation of other bacterial agents causing diarrhea was not evaluated at this phase due to financial constraints. Another limitation was not adding a control group with normal immune states associated with infectious diarrhea and/or with immunocompromised states associated with non-infectious diarrhea. Therefore, diarrhea may be caused by side effects of chemotherapy rather than pathogens [10], which could not be investigated in this study. In addition, since the clinical spectrum caused by C. difficile varies from asymptomatic colonization to sepsis and death [71], unfortunately, in this study, it was not possible to investigate the colonization from infection for non-toxigenic C. difficile with PCR alone.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CDIs:
-
C. difficile infections
- ALL:
-
Acute lymphocytic leukemia
- NHL:
-
Non-hodgkin’s lymphoma
- PCR:
-
Polymerase chain reaction
- ATCC:
-
American type culture collection
- tcd :
-
Toxigenic C. difficile
- cadF :
-
Campylobacter adhesion to fibronectin
- cdt :
-
C. difficile binary toxin
- 16S rRNA:
-
16 S ribosomal RNA
- cdd3 :
-
C. difficile downstream 3
References
Krones E, Högenauer C. Diarrhea in the immunocompromised patient. Gastroenterol Clin. 2012;41(3):677–701.
Shams S, Nasab SDM, Heydari H, Tafaroji J, Ahmadi N, Afzali ES. Detection and characterization of rotavirus G and P types from children with acute gastroenteritis in Qom, central Iran. Gastroenterol Hepatol Bed Bench. 2020;13(Suppl1):S128.
Shams S, Tafaroji J, Aghaali M, Ahmadi N, Heydari H, Nasab SDM, Maurya VK. Prevalence of enteric adenovirus and co-infection with rotavirus in children under 15 years of age with gastroenteritis in Qom, Iran. Gastroenterol Hepatol Bed Bench 2022, 15(3).
Mohebi S, Saboorian R, Shams S. The first report of Vibrio fluvialis isolated from a clinical sample in Iran. Iran J Microbiol. 2022;14(5):677.
Thom K, Forrest G. Gastrointestinal infections in immunocompromised hosts. Curr Opin Gastroenterol. 2006;22(1):18–23.
Sell J, Dolan B. Common gastrointestinal infections. Prim Care: Clin Office Pract. 2018;45(3):519–32.
Lamps LW, Lai KK, Milner DA Jr. Fungal infections of the gastrointestinal tract in the immunocompromised host: an update. Adv Anat Pathol. 2014;21(4):217–27.
Janda JM, Abbott SL. The genus Aeromonas: taxonomy, pathogenicity, and infection. Clin Microbiol Rev. 2010;23(1):35–73.
Shen H, Zhang J, Li Y, Xie S, Jiang Y, Wu Y, Ye Y, Yang H, Mo H, Situ C. The 12 gastrointestinal pathogens spectrum of acute infectious diarrhea in a sentinel hospital, Shenzhen, China. Frontiers in microbiology 2016, 7:1926.
Schmidt-Hieber M, Bierwirth J, Buchheidt D, Cornely O, Hentrich M, Maschmeyer G, Schalk E, Vehreschild J, Vehreschild MJ, Group AW. Diagnosis and management of gastrointestinal complications in adult cancer patients: 2017 updated evidence-based guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann Hematol. 2018;97:31–49.
Naharro G, Riano J, de Castro L, Alvarez S, Luengo J. Aeromonas: molecular detection of foodborne pathogens (Liu D. Ed). In.: CRC. North Ryde;; 2009.
Figueras M. Clinical relevance of Aeromonas sM503 (16, pg 145, 2005). REVIEWS Med Microbiol. 2006;17(3):91–91.
Schuetz AN. Emerging agents of gastroenteritis: Aeromonas, Plesiomonas, and the diarrheagenic pathotypes of Escherichia coli. Seminars in Diagnostic Pathology: 2019. Elsevier; 2019. pp. 187–92.
van Zwetselaar M, Nyombi B, Sonda T, Kumburu H, Chamba N, Dekker MC, Kilonzo KG, Urasa SJ, Mmbaga BT. Aeromonas caviae mimicking Vibrio cholerae infectious enteropathy in a cholera-endemic region with possible public health consequences: two case reports. J Med Case Rep. 2018;12:1–6.
Fernández-Bravo A, Fort-Gallifa I, Ballester F, Pujol I, Gomez-Bertomeu F, Domínguez M, Micó M, Alcoceba E, Simó-Sisó JM, Figueras MJ. A case of Aeromonas trota in an immunocompromised patient with diarrhea. Microorganisms. 2020;8(3):399.
Rupnik M, Wilcox MH, Gerding DN. Clostridium difficile infection: new developments in epidemiology and pathogenesis. Nat Rev Microbiol. 2009;7(7):526–36.
Tamma PD, Sandora TJ. Clostridium difficile infection in children: current state and unanswered questions. J Pediatr Infect Dis Soc. 2012;1(3):230–43.
Eberle KN, Kiess AS. Phenotypic and genotypic methods for typing Campylobacter jejuni and Campylobacter coli in poultry. Poult Sci. 2012;91(1):255–64.
Shams S, Bakhshi B, Tohidi Moghadam T, Behmanesh M. A sensitive gold-nanorods-based nanobiosensor for specific detection of Campylobacter jejuni and Campylobacter coli. J Nanobiotechnol. 2019;17(1):1–13.
Bakhshi B, Shams S, Rezaie N, Reza MAS. Design of dot-blot hybridization assay for simultaneous detection of Campylobacter jejuni and Campylobacter coli: a preliminary study. Annals Med Surg. 2024;86(1):219–24.
Moballegh Naseri M, Shams S, Moballegh Naseri M, Bakhshi B. In silico analysis of epitope-based CadF vaccine design against Campylobacter jejuni. BMC Res Notes. 2020;13:1–6.
Waage AS, Vardund T, Lund V, Kapperud G. Detection of small numbers of Campylobacter jejuni and Campylobacter coli cells in environmental water, sewage, and food samples by a seminested PCR assay. Appl Environ Microbiol. 1999;65(4):1636–43.
Crushell E, Harty S, Sharif F, Bourke B. Enteric Campylobacter: purging its secrets? Pediatr Res. 2004;55(1):3–12.
Eiland LS, Jenkins LS. Optimal treatment of campylobacter dysentery. J Pediatr Pharmacol Ther. 2008;13(3):170–4.
Barker CR, Painset A, Swift C, Jenkins C, Godbole G, Maiden MC, Dallman TJ. Microevolution of Campylobacter jejuni during long-term infection in an immunocompromised host. Sci Rep. 2020;10(1):10109.
Schiaffino F, Kosek MN. Intestinal and extra-intestinal manifestations of Campylobacter in the immunocompromised host. Curr Treat Options Infect Dis. 2020;12:361–74.
Boustanshenas M, Akbari M, Rezaie N. Evaluation of two different laboratory methods for the identification of Aeromonas spp. in stool sample of patients with diarrhea. Infect Epidemiol Microbiol. 2016;2(1):18–21.
Yang J-L, Wang M-S, Cheng A-C, Pan K-C, Li C-F, Deng S-X. A simple and rapid method for extracting bacterial DNA from intestinal microflora for ERIC-PCR detection. World J Gastroenterology: WJG. 2008;14(18):2872.
Shams S, Bakhshi B, Tohidi Moghadam T. In Silico Analysis of the cadF gene and development of a duplex polymerase chain reaction for species-specific identification of Campylobacter jejuni and Campylobacter coli. Jundishapur J Microbiol. 2016;9(2):e29645.
Chang Y-C, Wang J-Y, Selvam A, Kao S-C, Yang S-S, Shih DY-C. Multiplex PCR detection of enterotoxin genes in Aeromonas spp. from suspect food samples in northern Taiwan. J Food Prot. 2008;71(10):2094–9.
Cohen SH, Tang YJ, Silva J Jr. Analysis of the pathogenicity locus in Clostridium difficile strains. J Infect Dis. 2000;181(2):659–63.
Tian T-t, Zhao J-h, Yang J, Qiang C-x, Li Z-r, Chen J, Xu K-y. Ciu Q-q, Li R-x: molecular characterization of Clostridium difficile isolates from human subjects and the environment. PLoS ONE. 2016;11(3):e0151964.
Lemee L, Dhalluin A, Testelin S, Mattrat M-A, Maillard K, Lemeland J-F, Pons J-L. Multiplex PCR targeting tpi (triose phosphate isomerase), tcdA (toxin A), and tcdB (toxin B) genes for toxigenic culture of Clostridium difficile. J Clin Microbiol. 2004;42(12):5710–4.
Persson S, Torpdahl M, Olsen KE. New multiplex PCR method for the detection of Clostridium difficile toxin A (tcdA) and toxin B (tcdB) and the binary toxin (cdtA/cdtB) genes applied to a Danish strain collection. Clin Microbiol Infection: Official Publication Eur Soc Clin Microbiol Infect Dis. 2008;14(11):1057–64.
Jomezadeh N, Farajzadeh Sheikh A, Khosravi AD, Amin M. Detection of Shiga Toxin Producing E. Coli strains isolated from Stool samples of patients with Diarrhea in Abadan Hospitals, Iran. J Biol Sci. 2009;9:820–4.
Saberpour M, Najar-Peeraye S, Shams S, Bakhshi B. Effects of Chitosan nanoparticles loaded with mesenchymal stem cell conditioned media on gene expression in Vibrio cholerae and Caco-2 cells. Sci Rep. 2022;12(1):1–9.
Worku M, Belay G, Tigabu A. Bacterial profile and antimicrobial susceptibility patterns in cancer patients. PLoS ONE. 2022;17(4):e0266919.
Guerra IM, Fadanelli R, Figueiró M, Schreiner F, Delamare APL, Wollheim C, Costa SOP, Echeverrigaray S. Aeromonas associated diarrhoeal disease in south Brazil: prevalence, virulence factors and antimicrobial resistance. Brazilian J Microbiol. 2007;38:638–43.
Shams S, Rezaie N, Beltrame A, Moro L, Piubelli C, Amiri FB, Esmaeili S. Tropheryma whipplei intestinal colonization in immunocompromised children in Iran: a preliminary study. Future Microbiol. 2021;16(15):1161–6.
Bonaiuto E, Magro M, Fasolato L, Novelli E, Shams S, Piccirillo A, Bakhshi B, Moghadam TT, Baratella D, Vianello F. Versatile nano-platform for tailored immuno-magnetic carriers. Anal Bioanal Chem. 2018;410(29):7575–89.
Shams S, Bakhshi B, Nikmanesh B. Designing a rapid and accurate method for transportation and culture of the Campylobacter jejuni and Campylobacter coli-fastidious bacteria in the children with bacterial gastrointestinal symptoms. Koomesh 2016, 18(1).
Obi CL, Bessong PO. Diarrhoeagenic bacterial pathogens in HIV-positive patients with diarrhoea in rural communities of Limpopo Province, South Africa. J Health Popul Nutr 2002:230–4.
Nolla-Salas J, Codina-Calero J, Valles-Angulo S, Sitges-Serra A, Zapatero-Ferrandiz A, Climent M, Gómez J, Masclans J. Clinical significance and outcome of Aeromonas spp. infections among 204 adult patients. Eur J Clin Microbiol Infect Dis. 2017;36:1393–403.
Dallal MMS, Fard RMN, Talkhabi MK, Aghaiyan L, Salehipour Z. Prevalence, virulence and antimicrobial resistance patterns of Aeromonas spp. isolated from children with diarrhea. Germs. 2016;6(3):91.
Sadeghi H, Heidarzadeh S, Naghavi M, Rozeh ME, Afshar D. Molecular detection of Aeromonas and its virulence genes in hospitalized children with diarrhea in northwest of Iran. Hum Gene. 2022;33:201030.
Abbasi E, Khansari-nejad B, Abtahi H, Akbari M, Ghaznavi-rad E. Low prevalence of Aeromonas hydrophila in infectious diarrhea samples of pediatric patients in Arak, Iran. Rep Biochem Mol Biology. 2016;5(1):15.
Rahimi-Larki E, Nene S. The prevalence of Aeromonas hydrophila-induced diarrhoea in the pig, buffalo and human in Pune area, India. Iran J Veterinary Res. 2006;7(4):53–8.
Qamar FN, Nisar MI, Quadri F, Shakoor S, Sow SO, Nasrin D, Blackwelder WC, Wu Y, Farag T, Panchalingham S. Aeromonas-associated diarrhea in children under 5 years: the GEMS experience. Am J Trop Med Hyg. 2016;95(4):774.
Ghenghesh KS, Bara F, Bukris B, El-Surmani A, Abeid SS. Characterization of virulence factors of Aeromonas isolated from children with and without diarrhoea in Tripoli, Libya. J Diarrhoeal Dis Res 1999:75–80.
Zargar M, Ghadir MR, Javadi A, Morovvati A, Farahani FD. Drug Resistance Pattern of Toxigenic Clostridium difficile isolated from patients with diarrhea to conventional therapeutic drugs with chronic. Qom Univ Med Sci J. 2020;13(11):13–23.
Hematyar Y, Pirzadeh T, Moaddab SR, Rezaee MA, Memar MY, Kafil HS. Clostridium difficile in patients with nosocomial diarrhea, Northwest of Iran. Health Promotion Perspect. 2020;10(2):148.
Armin S, Babaie D, Karimi A, Fallah F. Toxigenic Clostridium difficile colonization in children. J Pediatr Infect Dis. 2009;4(04):375–8.
Plants-Paris K, Bishoff D, Oyaro MO, Mwinyi B, Chappell C, Kituyi A, Nyangao J, Mbatha D, Darkoh C. Prevalence of Clostridium difficile infections among Kenyan children with diarrhea. Int J Infect Dis. 2019;81:66–72.
Ferreira CE, Nakano V, Durigon EL, Avila-Campos MJ. Prevalence of Clostridium spp. and Clostridium difficile in children with acute diarrhea in Sao Paulo city, Brazil. Mem Inst Oswaldo Cruz. 2003;98:451–4.
Armin S, Shamsian S, Drakhshanfar H. Colonization with Clostridium difficile in children with Cancer. Iran J Pediatr. 2013;23(4):473.
Tavafi H, Owlia P, Shirvani F, Hashemie M, Shahrokhi N. Detection of virulence genes of Clostridium difficile in children with Cancer by Multiplex PCR. J Med Microbiol Infect Dis. 2014;2(3):95–9.
Price V, Portwine C, Zelcer S, Ethier M-C, Gillmeister B, Silva M, Schindera C, Yanofsky R, Mitchell D, Johnston DL. Clostridium difficile infection in pediatric acute myeloid leukemia: from the Canadian Infections in Acute Myeloid Leukemia Research Group. Pediatr Infect Dis J. 2013;32(6):610–3.
Ghorbanalizadgan M, Bakhshi B, Shams S, Najar-Peerayeh S. Pulsed-field gel electrophoresis fingerprinting of Campylobacter jejuni and Campylobacter coli strains isolated from clinical specimens, Iran. Int Microbiol. 2019;22:391–8.
Terefe Y, Deblais L, Ghanem M, Helmy YA, Mummed B, Chen D, Singh N, Ahyong V, Kalantar K, Yimer G. Co-occurrence of Campylobacter species in children from Eastern Ethiopia, and their association with environmental enteric dysfunction, diarrhea, and host microbiome. Front Public Health. 2020;8:99.
Toledo Z, Simaluiza RJ, Astudillo X, Fernández H. Occurrence and antimicrobial susceptibility of thermophilic Campylobacter species isolated from healthy children attending municipal care centers in Southern Ecuador. Revista do Instituto De Medicina Tropical De São Paulo 2017, 59.
Samie A, Moropeng RC, Tanih NF, Dillingham R, Guerrant R, Bessong PO. Epidemiology of Campylobacter infections among children of 0–24 months of age in South Africa. Archives Public Health. 2022;80(1):107.
Lothstein K, Fisher B, Li Y, Seif A, Harris T, Torp K, Kavcic M, Huang YSV, Rheingold SR, Aplenc R. Zoonotic infections in pediatric patients with acute leukemia. Pediatr Blood Cancer. 2013;60(12):E160–2.
Anvarinejad M, Shahidi MA, Pouladfar GR, Dehyadegari MA, Mardaneh J. Campylobacter jejuni bacteremia in a patient with acute lymphocytic leukemia. Iran Red Crescent Med J 2016, 18(6).
Martora F, Pagliuca C, Della Pepa ME, Della Rocca MT, Curto S, Iovene MR, Vitiello M. Campylobacter jejuni bacteremia in Italian pediatric patients with acute lymphoblastic leukemia: report of two cases. New Microbiol 2020, 43(2).
Kim Y, Shin JA, Han SB, Cho B, Jeong DC, Kang JH. Recurrent Campylobacter jejuni bacteremia in a patient with hypogammaglobulinemia: a case report. Med (Baltim). 2017;96(25):e7238.
Sharifipour E, Shams S, Esmkhani M, Khodadadi J, Fotouhi-Ardakani R, Koohpaei A, Doosti Z, Ej Golzari S. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect Dis. 2020;20(1):646.
Devi P, Khan A, Chattopadhyay P, Mehta P, Sahni S, Sharma S, Pandey R. Co-infections as modulators of disease outcome: minor players or major players? Front Microbiol. 2021;12:664386.
Barati M, Taghipour A, Bakhshi B, Shams S, Pirestani M. Prevalence of intestinal parasitic infections and Campylobacter spp. among children with gastrointestinal disorders in Tehran, Iran. Parasite Epidemiol Control. 2021;13:e00207.
de Graaf H, Pai S, Burns D, Karas J, Enoch D, Faust S. Co-infection as a confounder for the role of Clostridium difficile infection in children with diarrhoea: a summary of the literature. Eur J Clin Microbiol Infect Dis. 2015;34:1281–7.
Vasilev P, Ivanovska M, Lengerova G, Petrova A, Hristozova E, Murdjeva M, Stoycheva M. Coinfection of the intestinal tract with Aeromonas hydrophila, Clostridium difficile and Rotavirus-a case report. Folia Medica. 2021;63(4):576–81.
Schaeffler H, Breitrueck A. Clostridium difficile–from colonization to infection. Front Microbiol. 2018;9:646.
Acknowledgements
We wish to thank the Research Council of Qom University of Medical Sciences and the personnel of our hospitals for supporting the study.
Funding
We thank the Research Council of Qom University of Medical Sciences for supporting this project.
Author information
Authors and Affiliations
Contributions
HH, AI, and SS developed and supervised the work. SK, SASM, and AG performed the experiments. AM contributed to data interpretation. SS, SK, and AM drafted the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was performed according to the Helsinki Declaration protocol after obtaining the approval of the Ethics Committee of Qom University of Medical Sciences (Code No.: IR.MUQ.REC.1396.89). All methods were carried out in accordance with the relevant guidelines and regulations. The informed written consent of the children or their parents/ legal guardians was also obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Heydari, H., Iranikhah, A., Ghasemi, A. et al. Evaluation of the prevalence of Aeromonas spp., Campylobacter spp., and Clostridioides difficile in immunocompromised children with diarrhea. BMC Infect Dis 24, 512 (2024). https://doi.org/10.1186/s12879-024-09372-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09372-3