
Abstract
Background
An assessment of the factors that interfere with serum levels and the persistence of anti-SARs-CoV-2 IgG antibodies is essential in order to estimate the risk of reinfection and to plan vaccination. We analyzed the impact of the severity of coronavirus disease 2019 (COVID-19) and the clinical and biological factors regarding the persistence of SARs-CoV-2 anti-spike protein (IgG-S) antibodies at 12 months.
Methods
This was an observational, longitudinal study with individuals who had recovered from COVID-19 between August 2020 and June 2021. Peripheral blood samples were collected from volunteers who were hospitalized (SERIOUS COVID-19) and those who required no hospitalization (COVID-19 LIGHT). Samples were grouped according to days after symptom onset: up to 90, between 91 and 180, ≥ 180 days after symptom onset. A semiquantitative test for IgG anti-spike protein S1(IgG-S1) was used.
Results
We analyzed 238 individuals who had recovered from COVID-19, of whom 87 had been hospitalized and 151 had not. They provided 148 and 220 samples, respectively. Among those hospitalized, males (65.5%), volunteers aged over 60 years (41.1%), comorbidities such as arterial hypertension (67.8%) and diabetes mellitus (37.9%) were most frequent. We observed higher median serum IgG-S1 titers among those who had recovered from COVID-19 and had been hospitalized, at all collection time intervals (p < 0.001). We observed a weak correlation of increasing age with humoral IgG-S1 response (Spearman correlation = 0.298). There was a greater probability of IgG-S1 antibody persistence over time among samples from hospitalized individuals compared to samples from non-hospitalized participants (p = 0.001).
Conclusion
This study has revealed higher titers and a higher probability of the persistence of IgG-S1 in severe cases after SARs-CoV-2 primary infection in unvaccinated recovered patients. Thus, in this study, the severe clinical presentation of COVID-19 was the main factor influencing serum levels and the persistence of IgG-S1 antibodies in COVID-19.
Similar content being viewed by others


Background
Since the beginning of the coronavirus disease 2019 (COVID-19) pandemic, efforts have been made to understand the kinetics of the anti-SARS-CoV-2 antibodies, particularly the duration of the levels of the immunoglobulin G (IgG) class, due to its protective role in reinfection [1,2,3]. Two hypotheses are of concern: the first is the decline in serum levels of IgG antibodies over time [4, 5] and the second is the greater chance of individuals with mild COVID-19 not seroconverting or generating a modest immune response compared to those with severe COVID-19 [6, 7].
Early studies have suggested a rapid decline in anti-spike IgG antibodies (IgG-S), the protein used by the coronavirus in order to enter cells, within three to six months after infection [8,9,10]. Subsequent data have demonstrated that IgG-S antibodies persist for up to eight months in non-hospitalized individuals [11, 12]. A prospective cohort with a 13-month follow-up period reported a significant drop in serum levels of IgG-S antibodies, and which occurred faster in males [3]. In the present study, it was not possible to verify an association with the severity of the disease, since only 4% of the individuals required hospitalization.
More recently, an assessment regarding how these molecules remain in the serum of individuals with the disease suggested that there are two types of anti-SARS-Cov-2 antibodies: antibodies with half-lives after 6 months and antibodies with half-lives for up to 14 months[13]. Most studies on humoral response in patients with severe COVID-19 have reported an association between disease severity and high antibody titers [14,15,16]. However, the short follow-up periods of these studies have not enabled the authors to assess the impact of COVID-19 severity on IgG antibodies that persist beyond 120 days.
The aim of this prospective study is to compare the serum levels and the longevity of IgG-S antibodies of individuals with severe and mild COVID-19, and to identify clinical and biological factors that may be associated with the dynamics of IgG-S antibodies in unvaccinated individuals who have recovered from COVID-19, after a primary infection with SARS-CoV-2 within 12 months of follow-up after symptom onset.
Methods
A prospective, descriptive longitudinal study with an analytical feature was conducted in two high-complexity public hospitals in the city of Recife, Pernambuco, Brazil. Between August 2020 and June 2021, individuals were recruited aged over 18 years, who were treated at outpatient clinics for patients, who have recovered from COVID-19. Admission to the outpatient clinic occurred by referral from the attending physician after hospital discharge, by spontaneous demand or after an invitation by telephone contact from the research team. The study was approved by the institutional Ethics Committee of the Hospital das Clínicas at the Universidade Federal de Pernambuco (CEP-HC-UFPE 46681521.7.0000.8807).
At the first consultation, after signing the informed consent form, participants completed a questionnaire regarding sociodemographic characteristics, symptoms, comorbidities, and the need for hospitalization and were also submitted to peripheral blood collection. Those with no real-time polymerase chair reaction (RT-PCR) results or with a negative RT-PCR result for SARS-CoV-2 were excluded, as were individuals who had been vaccinated for COVID-19.
All RT-PCR tests for the detection of SARS-CoV-2 RNA, performed with nasopharyngeal swab samples, were analyzed at the Central Laboratory of Pernambuco (LACEN-PE).
Individuals were divided into two groups: Severe Cases: defined as those who required hospitalization; and Mild Cases: defined as those that did not require hospitalization. The Severe Cases group was further stratified according to oxygen demand: non-invasive oxygen therapy (nasal catheter and non-rebreathing mask) and invasive (invasive mechanical ventilation). The longevity and serum level of antibodies were assessed at three moments in time after the onset of symptoms: up to 90 days, between 91 and 180 days, after 180 days. Of the 238 individuals included in the study, 145 provided a single peripheral blood sample and 93 provided two or more samples.
For measuring the serum concentration of IgG-S1, the EUROIMMUN anti-SARS-CoV-2 ELISA kit (Lubeck, Germany) was used, one of the first diagnostic tests with the EC mark (European Conformity) to be developed, and available worldwide. The principle of this methodology is to quantify specific IgG to protein peak 1 (S1) of SARS-Cov-2 through an immunoenzymatic assay, where the results are presented in absorbance (optical density). This kit demonstrated a cumulative sensitivity of 82.6% for the detection of IgG in samples collected after 14 days of RT-PCR and a specificity of 86.9% [17]. To perform the test, the manufacturer's instructions were followed. The semi-quantitative test of the results was through the ratio between the absorbance level of the patient's sample by the absorbance level of the calibrator (Ratio). Ratio results < 0.8 were negative, ≥ 1.1 positive, and ≥ 0.8 and < 1.1 were indeterminate for the presence of IgG-S1.
Statistical analysis
For the statistical analysis, SPSS 13 (Statistical Package for the Social Sciences) for Windows was used. The chi-squared test and the Kruskal–Wallis rank sum test were conducted to identify significant differences in the categorical variables between the groups. The Mann–Whitney test was used to compare quantitative data between the groups. All tests were two-tailed with a level of 0.05. Missing data were excluded for analysis. The odds ratio (OR) with a confidence interval was calculated.
The variables included in the univariate analysis were as follows: hospitalization, sex, age, arterial hypertension, type 2 diabetes mellitus (T2DM), obesity, IgG-S1 antibody titers up to 90 days, between 91–180, and after 180 days. Variables that attained a level of p < 0.2 in the univariate analysis were entered in a linear regression model using the Enter method.
A quality control of the models was performed: the assumption of linearity and the quality of variance of the dependent variable across the range of values of the independent variable were assessed with scatterplots, and the assumption that the dependent variable is normally distributed was assessed with a normal probability plot (data not shown).
The researchers were not blinded when recruiting participants nor when they assessed the results. However, the tests for detecting IgG-S1 were completely blind, since identifying the biological samples did not define the stratification of the groups. Only the final analysis of the data revealed an overview of the results. Potential confounders were identified and controlled in the data analysis.
Results
A total of 245 individuals were referred to the outpatient clinic for those who have recovered from COVID-19, of whom, two were excluded for having presented a negative molecular test, and five were excluded for failing to present test results. Thus, 238 individuals were included in the study, who contributed 368 samples. The 87 participants who had been hospitalized provided 148 peripheral blood samples and the 151 participants who had not been hospitalized provided 220 peripheral blood samples over 386 days after symptom onset (Fig. 1).

Screening, Enrollment and Stratification. Among the recruited, seven were excluded for having presented a negative molecular test or for failing to present test results. 238 participants provided 368 samples over 386 days after symptom onset. RT-PCR denotes Real-time polymerase chain reaction
Clinical and biological characteristics of individuals recovered from COVID-19 according to hospitalization (Table 1)
The most frequently hospitalized patients were male (65.5%, p = 0.01). In the hospitalized group, 36 (41.1%) patients were aged 60 years or older (< 0.001). Among the 151 non-hospitalized participants, symptoms such as smell or taste changes, sore throat and headache were significantly more frequent. On the other hand, fever, cough and dyspnea were more common in the hospitalized group.
The presence of specific IgG-S1 antibodies against SARS-CoV-2 was verified in 313 samples. Forty-two samples were classified as negative for specific IgG-S1 antibodies against SARS-CoV-2. Of these, 39 samples were from non-hospitalized patients who had recovered and three samples were from hospitalized patients who had recovered.
Comorbidities such as systemic arterial hypertension (SAH) and diabetes mellitus were more prevalent among hospitalized patients (p < 0.001). All hospitalized participants had received oxygen therapy. Among these, 69 (79.3%) received non-invasive oxygen therapy and 18 (20.7%) received invasive ventilatory support and 29 (33.3%) were admitted to an intensive care unit.
Factors that impact the response of specific IgG-S1 against SARS-CoV-2
A comparison of the median level of serum IgG-S1 antibodies between samples from the Mild Group and the Severe Group demonstrated higher serum IgG-S1 titers among patients from the Severe Group at all collection times analyzed over the 386 days (p < 0.001). On the other hand, a drop in serum IgG-S1 titers was observed in both groups, despite the persistence of IgG-S1 during the follow-up period of the study (Fig. 2). Significantly, higher levels of IgG-S1 were observed in samples collected up to 90 days after symptom onset compared to samples collected 90 days and 180 days after symptom onset (Table 2).

Antibody IgG-S1 serum titers in 238 individuals who recovered from COVID-19 according to hospitalization at 386 days after primary infection. A comparison of the median level of serum IgG-S1 antibodies between samples from the Mild Group (blue box) and the Severe Group (green box) demonstrated higher serum IgG-S1 titers among patients from the Severe Group at all collection times analyzed over the 386 days A drop in serum IgG-S1 titers was observed in both groups during the follow-up period of the study. OD ratio: denotes ratio between the absorbance level of the patient’s sample by the absorbance level of the calibrator
Higher levels of IgG-S1 were observed in male, obese, hypertensive individuals with T2DM and individuals with four or more symptoms at the time of diagnosing COVID-19 (Table 2). Although there was a weak correlation between increasing age and humoral IgG-S1 response (Spearman correlation = 0.298; Fig. 3), we noted that individuals aged over 45 years presented significantly higher median levels of IgG-S1 when compared to younger individuals (Table 2). On the other hand, there was no statistically significant difference between the samples of participants who received invasive and non-invasive oxygen therapy support at all intervals of days after the onset of the analyzed symptoms (Fig. 4).

Spearman correlation coefficient between serum titers according to age = 0.298. Although there was a weak correlation between increasing age and humoral IgG-S1 response (Spearman correlation = 0.298), we noted that individuals aged over 45 years presented significantly higher median levels of IgG-S1 when compared to younger individuals (Table 2). OD Ratio: denotes ratio between the absorbance level of the patient's sample by the absorbance level of the calibrator

Antibody IgG-S1 serum titers in 87 hospitalized individuals who recovered from COVID-19 according to oxygen demand (invasive and non-invasive oxygen therapy). There was no statistically significant difference between the samples of participants who received invasive and non-invasive oxygen therapy support at all intervals of days after the onset of the analyzed symptoms
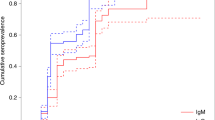
There was a greater probability of IgG-S1 antibody persisting over time among samples from hospitalized individuals when compared to samples from non-hospitalized participants (p = 0.001) (Fig. 5). Samples with IgG-S1 antibody titers below the cut-off point (negative) were more frequent in the non-hospitalized group, in those younger than 60 years and in those with no comorbidities.

Probability of IgG-S1 antibodies persisting according to severity in 238 individuals who recovered from COVID-19 over 386 days. (Kaplan Meier Curve: Log Rank (Mantel-Cox): Chi-Square 10.1575 df 1 p = 0.001 Testing equality of survival distributions for the different levels of Hospitalization.). There was a greater probability of IgG-S1 antibody persisting over time among samples from hospitalized individuals when compared to samples from non-hospitalized participants (p = 0.001)
In the multivariate analysis (Table 3), only hospitalization, age, number of symptoms at the time of diagnosis and the time of sample collection after the onset of symptoms continued to impact the humoral response. The severity of COVID-19 manifested the highest regression coefficient. It is estimated that, on average, the need for hospitalization increases the serum IgG-S1 titers by 2.91 units (coefficient 2.91, p = 0.001).
Our results presented higher median IgG-S1 antibody titers in the Severe Group samples in all the studied time intervals. Several studies have previously established the association between the severity of COVID-19 and the magnitude of the humoral response in the first four months after the onset of symptoms [14,15,16]. Our results also demonstrate that this association remains over twelve months. We believe that a higher viral and antigenic load in severe individuals [18,19,20] elicit a greater IgG-S1 antibody response and thereby justify the findings of our study. However, it is still controversial as to whether higher viral loads are associated with poorer outcomes in COVID-19 [21,22,23,24].
In the univariate analysis, hospitalization seemed to have an equal impact as the other variables on serum IgG-S titers. After multivariate analysis, it was observed in the final model that the variable with the greatest influence on the serum level of IgG-S1 antibodies was hospitalization, i.e., the severe presentation of COVID-19.
Despite the persistence of IgG-S1, there was a decrease in the antibody titers in both groups over the follow-up period. A negative association was observed between the variable days after symptom onset and the IgG-S1 antibody levels, suggesting that as time passes, the IgG-S1 antibody titer decreases in peripheral blood. A similar outcome to this has been reported in other studies [13, 25]. This dynamic of the humoral response in COVID-19 is analogous to many other viruses, including those that induce lifelong immunity, such as measles, experiencing a contraction phase [26, 27].
We observed a higher frequency of seronegativity and a greater probability of seronegativity for IgG-S1 during follow-up in the Mild Group. This finding was also reported by a study, which observed that 40% of asymptomatic individuals and 12% of symptomatic individuals presented with negative serology after a 90-day period [6]. While it is assumed that the risk of reinfection in this population is higher, it is not possible, however, to draw this conclusion, and more studies are required. A retrospective study reported no difference in the severity of COVID-19 when comparing individuals with the presence of IgG antibodies and individuals with no IgG antibodies [28].
In our sample, no association was observed between age and serum IgG-S1 titers in the final model. The link between age and antibodies in COVID-19 is controversial. However, advanced age was a predictive factor for hospitalization, in line with a number of other studies [29, 30]. It is known that immunosenescence promotes quantitative changes in cells and components of the immune system, together with more complex changes in the action of several immune responses. Older people are less able to respond effectively to new antigens, in addition to chronic low-grade inflammation brought about by an increase in the production of pro-inflammatory cytokines, acute-phase proteins and oxidative stressors [31].
Corroborating our findings, being male has been described as a risk factor for hospitalization [32, 33], but without influencing serum antibody titers. Gender differences in the immune response to COVID-19 have been described. Males present a pro-inflammatory response at the expense of IL-6, IL-8, GROα, sCD4L, MIP-1β, MCP-1. Some studies have demonstrated higher levels of the ACE2 receptor, used for viral entry into target cells, in males. The cellular serine protease TMPRSS2, responsible for activating the spike (S) protein of the coronavirus, is also highly expressed in the prostate epithelium and is sensitive to androgens [34]. However, in the present study, no difference was observed in serum IgG-S antibody titers between genders.
As with the variable sex, comorbidities such as SAH and T2DM demonstrated no association with the humoral response after adjusting for the other variables. They were more frequent in the Severe Group, thereby demonstrating a connection with the criticality of COVID-19. The link between SAH and the IgG-S antibody response has not been studied. There is controversy surrounding the hypothesis that hypertension is an independent predictor of severity [35].
The combination of SAH with T2DM or another comorbidity may be more relevant as a predictor of severe COVID-19 [36]. On the other hand, it is well established that T2DM and hyperglycemia increase the chance of hospitalization, but do not represent a decrease in serum levels of IgG-S antibodies after primary infection with SARS-CoV-2 [37], which is in agreement with our findings. Individuals with T2DM have an impaired proliferative response of lymphocytes, as well as disorders of the monocytes, macrophages, and neutrophils and in the complement activation [38].
In the present study, obesity, after the multivariate analysis, demonstrated no impact on the serum levels of the IgG-S antibody. However, Frasca et al. reported lower anti-IgG-S antibody titers in individuals with obesity, and a body mass index negatively associated with serum levels of IgG-S1 antibodies in COVID-19 [39]. These findings are consistent with the knowledge that obesity is associated with chronic low-grade inflammation and, in turn, a dysfunctional immune system [40, 41].
Although it is not a viral neutralization test, the semiquantitative EUROIMMUN IgG-S1 Kit was described as having a strong correlation with the neutralization test [42]. It is important to note that the small number of asymptomatic patients was due to the difficulty in finding these patients in the first wave of the pandemic, when tests for COVID-19 were scarce in Brazil and were reserved only for those with symptoms.
Other limitations included the fact that most study subjects only provided a single blood sample, and there was no continuous follow-up. Additionally, the study solely analyzed IgG-S1 antibodies. Due to limited resources, it was not possible to include tests for IgA and IgM antibodies, as well as against targets other than the spike protein.
Conclusions
In sum, this study has revealed higher antibody titers and a higher likelihood of IgG-S persisting in severe cases after SARS-CoV-2 primary infection in unvaccinated patients who have recovered. Thus, in this study, the severe clinical presentation of COVID-19 was the main factor influencing serum levels of IgG-S1 antibodies in COVID-19.
Availability of data and materials
Data are available upon request from the corresponding author.
Abbreviations
- SARS-CoV-2 :
-
Severe acute respiratory syndrome-coronavirus
- COVID-19 :
-
Coronavirus disease 2019
- SARS :
-
Severe acute respiratory syndrome
- ARDS :
-
Acute respiratory distress syndrome
- IgG :
-
Immunoglobulin G
- IgG-S :
-
Anti-spike Immunoglobulin G
- RT-PCR :
-
Real-time polymerase chain reaction
- LACEN-PE :
-
Central Laboratory of Pernambuco
- SAH:
-
Systemic arterial hypertension
- T2DM :
-
Type 2 diabetes mellitus
References
Long QX, Liu BZ, Deng HJ, Wu GC, Deng K, Chen YK, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat Med. 2020;26:845–8.
Lumley SF, O’Donnell D, Stoesser NE, Matthews PC, Howarth A, Hatch SB. Oxford University Hospitals Staff Testing Group. Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers. N Engl J Med. 2021;384:533–40.
Gallais F, Gantner P, Bruel T, Velay A, Planas D, Wendling MJ, et al. Evolution of antibody responses up to 13 months after SARS-CoV-2 infection and risk of reinfection. EBioMedicine. 2021;71:103561.
Seow J, Graham C, Merrick B, Acors S, Pickering S, Steel KJA, et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat Microbiol. 2020;5:1598–607.
COVID-19 Community Research Partnership Study Group. Duration of SARS-CoV-2 sero-positivity in a large longitudinal sero-surveillance cohort: the COVID-19 Community Research Partnership. BMC Infect Dis. 2021;21:889.
Long QX, Tang XJ, Shi QL, Li Q, Deng HJ, Yuan J, et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med. 2020;26:1200–4.
Kowitdamrong E, Puthanakit T, Jantarabenjakul W, Prompetchara E, Suchartlikitwong P, Putcharoen O, et al. Antibody responses to SARS-CoV-2 in patients with differing severities of coronavirus disease 2019. PLoS ONE. 2020;15:e0240502.
Figueiredo-Campos P, Blankenhaus B, Mota C, Gomes A, Serrano M, Ariotti S, et al. Seroprevalence of anti-SARS-CoV-2 antibodies in COVID-19 patients and healthy volunteers up to 6 months post disease onset. Eur J Immunol. 2020;50:2025–40.
Gaebler C, Wang Z, Lorenzi JCC, Muecksch F, Finkin S, Tokuyama M, et al. Evolution of antibody immunity to SARS-CoV-2. Nature. 2021;591:639–44.
Dan JM, Mateus J, Kato Y, Hastie KM, Yu ED, Faliti CE, et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science. 2021;371:6529.
Sherina N, Piralla A, Du L, Wan H, Kumagai-Braesch M, Andréll J, et al. Persistence of SARS-CoV-2-specific B and T cell responses in convalescent COVID-19 patients 6–8 months after the infection. Med. 2021;2:281–95.
Tian X, Jiang W, Zhang H, Lu X, Li L, Liu W, Li J. Persistence of the SARS-CoV-2 Antibody Response in Asymptomatic Patients in Correctional Facilities. Front Microbiol. 2021;12:789374.
Rosati M, Terpos E, Ntanasis-Stathopoulos I, Agarwal M, Bear J, Burns R, et al. Sequential Analysis of Binding and Neutralizing Antibody in COVID-19 Convalescent Patients at 14 Months After SARS-CoV-2 Infection. Front Immunol. 2021;12:793953.
Imai K, Kitagawa Y, Tabata S, Kubota K, Nagura-Ikeda M, Matsuoka M, et al. Antibody response patterns in COVID-19 patients with different levels of disease severity in Japan. J Med Virol. 2021;93:3211–8.
Röltgen K, Powell AE, Wirz OF, Stevens BA, Hogan CA, Najeeb J, et al. Defining the features and duration of antibody responses to SARS-CoV-2 infection associated with disease severity and outcome. Sci Immunol. 2020;5:54.
Ren L, Zhang L, Chang D, Wang J, Hu Y, Chen H, et al. The kinetics of humoral response and its relationship with the disease severity in COVID-19. Commun Biol. 2020;3:780.
Gededzha MP, Mampeule N, Jugwanth S, Zwane N, David A, Burgers WA, et al. Performance of the EUROIMMUN Anti-SARS-CoV-2 ELISA Assay for detection of IgA and IgG antibodies in South Africa. PLoS ONE. 2021;16:6.
El Zein S, Chehab O, Kanj A, Akrawe S, Alkassis S, Mishra T, et al. SARS-CoV-2 infection: Initial viral load (iVL) predicts severity of illness/outcome, and declining trend of iVL in hospitalized patients corresponds with slowing of the pandemic. Plos One. 2021;16(9):e0255981.
Tsukagoshi H, Shinoda D, Saito M, Okayama K, Sada M, Kimura H, Saruki N. Relationships between Viral Load and the Clinical Course of COVID-19. Viruses. 2021;13:304.
Fajnzylber J, Regan J, Coxen K, Corry H, Wong C, Rosenthal A, et al. SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nat Commun. 2020;11:5493.
Kim Y, Cheon S, Jeong H, Park U, Ha NY, Lee J, et al. Differential Association of Viral Dynamics With Disease Severity Depending on Patients’ Age Group in COVID-19. Front Microbiol. 2021;12:712260.
Abdulrahman A, Mallah SI, Alqahtani M. COVID-19 viral load not associated with disease severity: findings from a retrospective cohort study. BMC Infect Dis. 2021;21:688.
Knudtzen FC, Jensen TG, Lindvig SO, Rasmussen LD, Madsen LW, Hoegh SV, et al. SARS-CoV-2 viral load as a predictor for disease severity in outpatients and hospitalised patients with COVID-19: A prospective cohort study. PLos One. 2021;16:10.
Trunfio M, Calcagno A, Bonora S, Di Perri G. Lowering SARS-CoV-2 viral load might affect transmission but not disease severity in secondary cases. Lancet Infect Dis. 2021;21:914–5.
Peghin M, De Martino M, Fabris M, Palese A, Visintini E, Graziano E, et al. The Fall in Antibody Response to SARS-CoV-2: a longitudinal study of asymptomatic to critically Ill patients up to 10 months after recovery. J Clin Microbiol. 2021;59:11.
Hu Y, Lu P, Deng X, Guo H, Zhou M. The declining antibody level of measles virus in China population, 2009–2015. BMC Public Health. 2018;18:906.
Gibney KB, Attwood LO, Nicholson S, Tran T, Druce J, Healy J, et al. Emergence of Attenuated Measles Illness Among IgG-positive/IgM-negative Measles Cases: Victoria, Australia, 2008–2017. Clin Infect Dis. 2020;70:1060–7.
Ding J, Liu C, Wang Z, Guo H, Zhang K, Ma L, et al. Characteristics and Prognosis of Antibody Non-responders With Coronavirus Disease 2019. Front Med (Lausanne). 2022;9:813820.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–62.
O’Driscoll M, Ribeiro Dos Santos G, Wang L, Cummings DAT, Azman AS, Paireau J, et al. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature. 2021;590:140–5.
Aiello A, Farzaneh F, Candore G, Caruso C, Davinelli S, Gambino CM, et al. Immunosenescence and its hallmarks: how to oppose aging strategically? A review of potential options for therapeutic intervention. Front Immunol. 2019;10:2247.
Marina S, Piemonti L. Gender and Age Effects on the Rates of Infection and Deaths in Individuals With Confirmed SARS-CoV-2 Infection in Six European Countries. 2020. https://ssrn.com/abstract=3576790. Accessed 21 Fev 2023.
Islam N, Shkolnikov VM, Acosta RJ, Klimkin I, Kawachi I, Irizarry RA. Excess deaths associated with covid-19 pandemic in 2020: age and sex disaggregated time series analysis in 29 high income countries. BMJ. 2021;373:n1137.
Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020;181:271–80.
Bauer AZ, Gore R, Sama SR, Rosiello R, Garber L, Sundaresan D, et al. Hypertension, medications, and risk of severe COVID-19: a Massachusetts community-based observational study. J Clin Hypertens. 2020;23:21–7.
Sun Y, Guan X, Jia L, Xing N, Cheng L, Liu B, et al. Independent and combined effects of hypertension and diabetes on clinical outcomes in patients with COVID-19: a retrospective cohort study of Huoshen mountain hospital and Guanggu Fangcang Shelter Hospital. J Clin Hypertens. 2020;23:218–31.
Lampasona V, Secchi M, Scavini M, Bazzigaluppi E, Brigatti C, Marzinotto I, et al. Antibody response to multiple antigens of SARS-CoV-2 in patients with diabetes: an observational cohort study. Diabetologia. 2020;63:2548–58.
Daryabor G, Atashzar MR, Kabelitz D, Meri S, Kalantar K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front Immunol. 2020;11:1582.
Frasca D, Reidy L, Cray C, Diaz A, Romero M, Kahl K, Blomberg BB. Influence of obesity on serum levels of SARS-CoV-2-specific antibodies in COVID-19 patients. PLos One. 2021;16(3):e0245424.
Franceschi C, Bonafè M, Valensin S, Olivieri F, De Luca M, Ottaviani E, De Benedictis G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann N Y Acad Sci. 2000;908:244–54.
Mayer-Pickel K. Obesity and antiphospholipid syndrome: a particular challenge in pregnancy. Obes Res Open J. 2015;2:46–56.
Montesinos I, Dahma H, Wolff F, Dauby N, Delaunoy S, Wuyts M, et al. Neutralizing antibody responses following natural SARS-CoV-2 infection: Dynamics and correlation with commercial serologic tests. J Clin Virol. 2021;144:104988.
Acknowledgements
We would like to thank all the volunteers who agreed to participate in this study and the Central Administration of Postgraduate Studies at the Universidade Federal de Pernambuco.
Funding
This study was funded by the Financial Aid to Researchers project from the Central Administration of Postgraduate Studies at the Universidade Federal de Pernambuco (Number 078608/2020–11).
Author information
Authors and Affiliations
Contributions
MIO conceived the project, wrote the article, and provided outpatient care to individuals who had recovered from COVID-19 and who participated in the study. VPOS and MPOS interviewed and completed a questionnaire. PANF received, identified, processed and stored peripheral blood samples from volunteers in the project collection library. MRA and VMBL processed and performed the enzyme immunoassays. MIO performed the statistical analysis. VMBL and PSRA reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This project was submitted to and approved by the Human Research Ethics Committee of the Hospital das Clínicas at the Universidade Federal de Pernambuco (CEP-HC-UFPE 46681521.7.0000.8807) in compliance with the guidelines and regulatory standards for research involving human beings. Individuals who agreed to participate in the study signed an informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
de Oliveira, M.I., Aciole, M.R., Neves, P.A.F. et al. A stronger antibody response in increased disease severity of SARS-CoV-2. BMC Infect Dis 24, 17 (2024). https://doi.org/10.1186/s12879-023-08923-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08923-4