
Abstract
Background
The incidence of cryptococcosis amongst HIV-negative persons is increasing. Whilst the excellent performance of the CrAg testing in people living with HIV is well described, the diagnostic performance of the CrAg LFA has not been systematically evaluated in HIV-negative cohorts on serum or cerebrospinal fluid.
Methods
We performed a systematic review to characterise the diagnostic performance of IMMY CrAg® LFA in HIV-negative populations on serum and cerebrospinal fluid. A systematic electronic search was performed using Medline, Embase, Global Health, CENTRAL, WoS Science Citation Index, SCOPUS, Africa-Wide Information, LILACS and WHO Global Health Library. Studies were screened and data extracted from eligible studies by two independent reviewers. A fixed effect meta-analysis was used to estimate the diagnostic sensitivity and specificity.
Results
Of 447 records assessed for eligibility, nine studies met our inclusion criteria, including 528 participants overall. Amongst eight studies that evaluated the diagnostic performance of the IMMY CrAg® LFA on serum, the pooled median sensitivity was 96% (95% Credible Interval (CrI) 68–100%) with a pooled specificity estimate of 96% (95%CrI 84–100%). Amongst six studies which evaluated the diagnostic performance of IMMY CrAg® LFA on CSF, the pooled median sensitivity was 99% (95%CrI 95–100%) with a pooled specificity median of 99% (95%CrI 95–100%).
Conclusions
This review demonstrates a high pooled sensitivity and specificity for the IMMY CrAg® LFA in HIV-negative populations, in keeping with findings in HIV-positive individuals. The review was limited by the small number of studies. Further studies using IMMY CrAg® LFA in HIV-negative populations would help to better determine the diagnostic value of this test.
Similar content being viewed by others


Background
Cryptococcosis is a fungal infection caused by the pathogenic Cryptococcus species, of which there are seven recognised species: C. neoformans variety grubii, C. neoformans variety neoformans and five species within C. gatti [1]. Infection occurs following inhalation of fungal cells which may lead to either asymptomatic colonisation or pulmonary cryptococcal disease [2] presenting with cough, fever, shortness of breath and/or pulmonary nodules on chest radiographs [3]. Cryptococcus spp. may disseminate to cause cryptococcal antigenaemia, with or without progression to multi-organ disease. Dissemination to the central nervous system causes cryptococcal meningitis, which typically presents with fever, headache, neck stiffness, altered mental status and visual disturbance [2]. Other body sites such as liver, spleen skin and bone are less commonly affected [3].
Cryptococcal infection most often occurs in people living with HIV (PLWH); however, the proportion of cases in HIV-negative patients is increasing in high income countries [4, 5], in part due to increasing use of immunosuppressive therapies for cancer chemotherapy and organ transplantation [4, 6].
In addition to immunosuppressive therapy or solid organ transplantation, hematopoietic and other malignancies, innate immune defects, advanced renal or liver disease, diabetes mellitus, rheumatologic diseases and sarcoidosis increase the risk of cryptococcal infection [3, 7, 8]. Clinical cases of cryptococcal disease have also been reported in apparently immunocompetent individuals [2, 3, 9].
Cryptococcal antigen (CrAg) is a biomarker of cryptococcosis, and detection of CrAg in cerebrospinal fluid (CSF), serum, plasma or whole blood either by lateral flow assay (LFA), latex agglutination (LA) or enzyme-linked immunosorbent assays (ELISA) is the cornerstone in diagnosing cryptococcosis. Other diagnostic modalities include basic CSF analysis (white cell count, protein, glucose), India ink staining, cryptococcal culture on Sabouraud’s dextrose agar, and histology. Multiplex polymerase chain (PCR) platforms including Cryptococcus spp. as a target pathogen have also been evaluated as a diagnostic tool for cryptococcosis; and matrix-assisted laser desorption ionization–time-of-flight mass spectrometry (MALDI-TOF) has also been reported to detect Cryptococcus spp. in clinical specimens [10]. The World Health Organization (WHO) recommends rapid Ag-detection assays for diagnosis of cryptococcal disease in PLWH [11].
The IMMY CrAg® LFA (Norman, Oklahoma, USA), approved by the U.S. Food and Drug Administration (FDA) in 2011, is an immunochromatographic dipstick assay that detects antigen with qualitative or semiquantitative results. The IMMY CrAg® LFA is currently the most sensitive commercially available cryptococcal diagnostic test, with superior sensitivity to India ink microscopy on CSF, CSF cryptococcal culture, Meridian Cryptococcal Antigen Latex Agglutination System (CALAS®), the Meridian EIA assay, and the BioFire® FilmArray® Meningitis/Encephalitis (ME) panel [12,13,14,15,16]. The IMMY CrAg® LFA was therefore employed as part of The Febrile Illness Evaluation in a Broad Range of Endemicities (FIEBRE) study; a prospective observational study to investigate the infectious causes of fever at four sites in Africa and Asia, collecting data and samples from PLWH and HIV-negative inpatients and outpatients [17]. FIEBRE focused on illnesses deemed preventable or treatable, of which cryptococcosis is an important example. Lumbar punctures were not routinely conducted as part of the FIEBRE diagnostic package, so the IMMY CrAg® LFA performed on serum samples was chosen as the diagnostic strategy for all FIEBRE participants.
The performance of CrAg testing for the diagnosis of cryptococcosis in HIV-negative populations has not previously been systematically reviewed. This review aims to assess diagnostic performance of the IMMY CrAg® LFA compared to other cryptococcal diagnostic tests for the diagnosis of cryptococcosis in HIV-negative persons.
Methods
This systematic review was registered at PROSPERO (www.crd.york.ac.uk/PROSPERO) as CRD42022314040 on 02/03/2022 and is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for the reporting of systematic reviews and meta-analyses [18].
Literature search strategy
The following searches were conducted with an aim of identifying all studies reporting on the diagnostic performance of the IMMY CrAg® LFA for the diagnosis of cryptococcosis in HIV-negative populations. The study population was HIV-negative adults and children. The index test was the IMMY CrAg® LFA and comparator tests were any alternative cryptococcal diagnostic test/s, including clinical composite end-points.
A systematic electronic search was conducted using Medline, Embase, Global Health, CENTRAL, WoS Science Citation Index, SCOPUS, Africa-Wide Information, LILACS and WHO Global Health Library. A draft search strategy was compiled in the OvidSP Medline database by an experienced information specialist (JF). The search strategy included strings of terms, synonyms and controlled vocabulary terms (where available) to reflect two concepts: Cryptococcus spp. and IMMY lateral flow assay. Further information on the search methodology is available in Additional file 1.
Information management
All citations identified were imported into EndNote™ X9 software (Pennsylvania, PA, USA). Duplicates were identified and removed using the method described on the London School of Hygiene & Tropical Medicine Library & Archives Service blog [19].
The OvidSP MEDLINE search was adapted for each of the bibliographic databases. The search period was 2009–July 2021, as the IMMY CrAg® LFA was introduced in 2009.
Study selection
A two-stage screening process was employed: (1) at title and abstract and (2) at full-text level according to eligibility criteria as detailed below. Screening was performed in duplicate independently by two reviewers (CM, JE), and any disagreements were resolved by discussion. Reports not meeting the eligibility criteria were excluded. Reference and citation checking were conducted for included articles.
Studies were eligible for inclusion if they reported on the use of the IMMY CrAg® LFA tested on serum and/or CSF, in HIV-negative persons, compared to any other test/s or composite used to diagnose cryptococcal disease. Studies including asymptomatic and/or symptomatic persons were included. We included all study types, irrespective of country, region, continent, or level of care (primary, secondary, or tertiary). Studies that did not have disaggregate data for HIV-negative participants were excluded.
Data extraction and synthesis
For all eligible studies two reviewers (CM, JE) independently extracted data using an Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) including sample size, study design, participant characteristics, sample characteristics, flow and timing of sample analysis and comparator test characteristics. For each study the performance results for the CrAg LFA test (Index, “I”) and the comparator test (“C”) were extracted into 2 × 2 tables. In studies using multiple comparator tests a 2 × 2 table was generated for each comparator.
Quality assessment
Two reviewers (CM, JE) used the QUADAS-2 (quality assessment of diagnostic-accuracy studies-2) tool for quality assessment to evaluate the risk of bias and applicability of all included studies [20]. Disagreements were resolved by discussion.
Statistical analysis and data synthesis
The original analysis plan included random effect meta-analysis. A random-effect meta-analysis accounting for between-study heterogeneity would usually be the model of choice in this scenario because we would not expect the sensitivity and specificity of the diagnostic test to be the same in each study. In this systematic review however, there were a limited number of studies and only one study that actively sought to investigate the specificity [21] of the diagnostic test of interest, making a random-effects model inappropriate [22]. A fixed-effect model was therefore used in this instance.
Modelled estimates for the sensitivity and specificity of the IMMY CrAg® LFA were calculated for each study, as well as a single pooled estimate. The studies were subdivided by sample type; the estimates were calculated for use of the CrAg LFA on both serum and CSF. For the analysis similar comparator tests, for example, different latex agglutination tests, were grouped to represent a single comparator test.
We chose to fit a Hierarchical Summary Receiver Operating Characteristic (HSROC) model [23] with fixed accuracy and threshold parameters. This model still ensures that sensitivity and specificity are jointly estimated as well as accounting for imperfect reference tests [24] while also allowing for asymmetry in the SROC curve. This model can be seen as a simplification of the random effects model fit in Jullien et al. [25] where the variances of the random effects are zero \((i.e. {\sigma }_{\theta }=0, \mathrm{and}\, {\sigma }_{\alpha }=0, \,\mathrm{such\,that} {\uptheta }_{j}\, \mathrm{and}\, {\alpha }_{j}\, \mathrm{are\,equal\,to}\,\Theta\, \mathrm{and}\,\Lambda\,, {\mathrm{respectively}})\).
All analyses were conducted in R with stan [26]. For model code see: https://github.com/shk313/diagnostic-test-metaanalysis/tree/main/CrAg.
Results
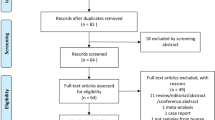
Our searches yielded 447 potentially eligible articles. After removal of duplicates (n = 12), screening of titles and abstracts (n = 435) and review of the full texts (n = 41), nine articles met our eligibility criteria for inclusion (Fig. 1 PRISMA diagram).

PRISMA diagram showing selection of studies for a systematic review of the diagnostic performance of the IMMY cryptococcal antigen lateral flow assay on serum and cerebrospinal fluid in HIV-negative patients. *No full text available (6), paper not written in English (2), samples tested not from HIV-negative persons (adults or children) – or no disaggregate data for HIV-negative persons (13), study reports on < 4 cases (8), does not report use of IMMY CrAg® LFA on serum or CSF (3)
Study description
The nine articles included and their key characteristics are summarised in Tables 1 and 2. In total, the included studies evaluated the diagnostic performance of the IMMY CrAg® LFA in 528 HIV-negative persons, across three continents. The reports were published between 2015 and 2021. The mean number of participants per study was 59, with a median of 37 participants per study. The age of study participants ranged from eight [27] to 88 years. [28, 29] The majority of participants were male, with the percentage of female participants ranging from 27 to 50% [28, 30]. All studies used cross sectional study design.
In seven of the nine included studies, a proportion (12–55%) of the participants were reported to be immunosuppressed. Where documented, immunosuppression included long-term immunosuppressive therapy (1–20%) [21, 27, 28, 31], solid organ transplant (3–19%) [21, 27, 28, 31], malignancy (3–11%) [21, 28, 29, 31,32,33], innate immune defects (3–39%) [27, 32], liver disease (1–19%) [21, 27, 32], renal disease (3%) [32], diabetes (3–14%) [27,28,29, 32, 33] and rheumatological disease (1–14%) [21, 27, 33]. Other forms of reported immunosuppression included tuberculosis [27] and myasthenia gravis [32].
The majority of studies (six of seven) reported on the diagnostic performance of the IMMY LFA amongst symptomatic inpatients. This included patients with a range of cryptococcosis clinical phenotypes including cryptococcal antigenaemia (n = 56), cryptococcal meningitis (n = 103), pulmonary cryptococcosis (n = 233), and other cryptococcal disease including unspecified disseminated cryptococcosis (n = 39). There was significant heterogeneity between study cohorts with one study looking at cryptococcal meningitis only [27], two looking at only pulmonary cryptococcosis [31, 33], and the others including a combination of cryptococcal meningitis, pulmonary cryptococcosis and cryptococcal antigenaemia in varying proportions [28,29,30, 32, 34].
The diagnostic performance of the IMMY CrAg® LFA was compared to a wide range of comparators. Across all studies the results of IMMY CrAg® LFA testing on serum were compared with eight different cryptococcal diagnostic tests/composites: IMMY LA (n = 1), Meridian LA (n = 3), Biorad LA (n = 1) and Remel LA (n = 1) [21, 30, 32], Meridian EIA (n = 1) [32], culture of any site (n = 1) [28], histopathology (n = 2) [28, 31], and composites (n = 3) [29, 33, 34]. IMMY CrAg® LFA testing on CSF was compared with 10 different cryptococcal diagnostic tests/composites: IMMY LA (n = 1), Meridian LA (n = 3), Biorad LA (n = 1) and Remel LA (n = 1) [21, 30, 32], Meridian EIA (n = 1) [32], culture (n = 2) [27, 28], microscopy performed on India ink-stained samples (n = 1) [27], composites (n = 2) [28, 29], LAMP (n = 1) [27] and qPCR (n = 1) [27]. A total of three clinical composite end-point definitions were used, as described in the footnotes of Tables 1 and 2 [28, 33, 34].
Findings
Amongst eight studies which used the IMMY CrAg® LFA on serum to detect cryptococcal disease, the pooled sensitivity estimate, as compared to all comparator tests, was calculated as 96% (95%CrI 68–100%) and the pooled specificity estimate was calculated as 96% (95%CrI 84–100%). Amongst six studies which evaluated the diagnostic performance of IMMY CrAg® LFA on CSF, the pooled sensitivity was calculated as 99% (95%CrI 95–100%) and pooled specificity 99% (95%CrI 95–100%).
The estimated sensitivity and specificity of the IMMY CrAg® LFA in each study as well as the pooled estimates from testing on serum and CSF are shown in Figs. 2 and 3.

Forest plot of IMMY CrAg® lateral flow assay sensitivity and specificity on serum

Forest plot of IMMY CrAg® lateral flow assay sensitivity and specificity on cerebrospinal fluid
Methodological quality of included studies
Table 3 summarises the risk of bias and applicability concerns for each study. Overall there were no concerns about the applicability of the included studies. All studies were classified as having some risk of bias however, either with respect to (i) patient selection, (ii) interpretation of the index test, (iii) choice and/or interpretation of the reference standard, or (iv) sample flow and timing. In seven of nine studies, bias concerns were raised in ≥ 2 of the categories; three studies were classified as being at high risk of bias. The primary risk of bias category highlighted was in relation to interpretation of the index test, as in seven studies it was unclear whether the IMMY CrAg® LFA result was interpreted in isolation, without prior knowledge of the results of the comparator test/s. Additionally, four studies were classified as being an unclear risk of bias with respect to patient selection, because it was not reported if patient sampling was random and/or whether the study avoided inappropriate exclusions.
Discussion
In this review, we evaluated the diagnostic performance of the IMMY CrAg® LFA for diagnosis of cryptococcal disease amongst 528 HIV-negative persons from 9 studies. The point estimate for the sensitivity and specificity of the IMMY CrAg® LFA from the pooled values were good in both serum and CSF (> 95% for both), in keeping with estimates reported in HIV positive cohorts [12, 13, 15, 16]. This is an important finding because, although the greatest burden of cryptococcal disease occurs in PLWH, this globally endemic fungal pathogen also infects HIV-negative individuals in increasing proportions.
These findings are consistent with the diagnostic accuracy literature from HIV-positive cohorts. In all published studies in PLWH, the IMMY CrAg® LFA has been found to be more sensitive than all other cryptococcal diagnostic tests. In a large multi-site validation study amongst PLWH in Uganda and South Arica, the IMMY CrAg® LFA performed on CSF was more sensitive than CSF culture (99.3% vs 90.0%), and more sensitive and specific than India ink microscopy on CSF (99.3% vs 86.1% and 99.1% vs 97.3% respectively) [12]. A study comparing IMMY CrAg® LFA to Meridian Cryptococcal Antigen Latex Agglutination System (CALAS®) and Meridian enzyme immunoassay (EIA), which tested 1,000 specimens (589 serum and 411 CSF) in parallel demonstrated higher sensitivity of the IMMY CrAg® LFA due to improved sensitivity for serotype C Glucuronoxylomannan (GXM) [13]. Similarly, the IMMY CrAg® LFA has better diagnostic performance than current PCR-based cryptococcosis diagnostics [15]. Amongst 328 adult and 42 paediatric CSF specimens evaluated using a multiplex PCR-based commercial assay (the BioFire® FilmArray® Meningitis/Encephalitis (ME) panel; BioFire Diagnostics, Salt Lake City, Utah, USA), for Cryptococcus spp., sensitivity was 82% and specificity was 98%, using CSF CrAg testing as the reference standard [15].
A systematic review and meta-analysis of 11 studies compared CrAg testing, of serum or CSF, to CSF microscopy with India ink staining, and CSF culture for the diagnosis of cryptococcal meningitis in symptomatic PLWH [16]. In all studies fungal culture was the reference standard for confirming cryptococcal meningitis. The review calculated the sensitivity and specificity of both LA and LFA CrAg tests on serum and CSF, using pooled data from multiple studies. For LA on serum (five diagnostic cohorts, 256 participants) the pooled sensitivity estimate was 100% (99.5–100) with pooled specificity estimate 96.7% (93.8–98.9). For LFA on serum (three diagnostic cohorts, 1690 participants) the pooled sensitivity estimate was 97.9% (87.9–100) and pooled specificity estimate was 89.5% (74.3–98.5). LA showed similar sensitivity in serum as LFA (P = 0.08) and there was no statistically significant difference in specificity (P = 0.14). For LA on CSF (10 diagnostic cohorts, 1810 participants) the pooled sensitivity was 97.1% (91.9–99.0) and pooled specificity was 99.1% (93.8–99.9). For LFA on CSF (6 diagnostic cohorts, 3099 participants) the pooled sensitivity was 99.5% (97.2–99.9) and pooled specificity was 99.5% (94.2–99.9). There was some evidence that LFA may have better sensitivity in CSF (P = 0.07) than LA but specificities were comparable (P = 0.54) [16]. From our analysis the high sensitivity and specificity of IMMY CrAg® LFA in serum and CSF of HIV-uninfected people is in keeping with previously reported values in studies of CrAg testing on PLWH.
There were several limitations to our review. Firstly, due to the lack of data on performance of IMMY CrAg® LFA in HIV-negative people, only nine studies reporting results from a total of 528 participants were suitable for inclusion in the review. Amongst these studies, the diverse patient characteristics, range of comparator tests and cryptococcal disease phenotype made comparison difficult. The majority of studies recruited symptomatic patients or tested samples of patients known to have cryptococcal disease, with only one study screening asymptomatic patients. This limited the statistical analysis as there were very few negative IMMY CrAg® LFA results in the 2 × 2 tables. For this reason, a fixed effect meta-analysis was used. As a consequence of using a fixed-effect framework we do not suggest that these results are generalizable to other studies not included in this review. A fixed-effect meta-analysis assumes that the sensitivity and specificity is homogenous across studies and so does not account for variability between studies. As a result, our pooled estimates will underestimate the uncertainty by failing to account for this variability. Although we did not account for between-study heterogeneity, we did account for within-study heterogeneity through the use of a fixed-effect conditional dependence structure between diagnostic tests in a study [35]. The small number of studies and limited data also prevented any further sub-analyses regarding the performance of the IMMY CrAg® LFA between different patient groups or between different cryptococcal species.
Another limitation was that the quality assessment using the QUADAS-2 tool identified unclear or high risk of bias in all studies. A key concern was that reference standard tests were interpreted with prior knowledge of the result of the index test and that populations being tested had already been classified as having cryptococcal infection. The flow and timing of testing was also unclear in a number of studies, with a lack of information regarding exclusions.
The main strengths of this review are that this is the first review looking at CrAg LFA testing of participants without HIV. It is also novel in calculating a value for specificity, where the majority of studies included in the review have focussed on sensitivity estimates only.
Conclusions
This review estimates a high sensitivity and specificity for IMMY CrAg® LFA in HIV-negative populations, as previously described for PLWH. However, our review was limited by a small number of disparate studies reporting IMMY CrAg® LFA testing on HIV-negative persons. Further studies using IMMY CrAg® LFA on both symptomatic patients being evaluated for cryptococcal disease and asymptomatic screening cohorts in HIV-negative populations are required to better predict the diagnostic value of this test. This is important given the increasing proportion of HIV-negative patients with cryptococcal infection.
Availability of data and materials
Code used for meta-analysis is publicly available at: https://github.com/shk313/diagnostic-test-metaanalysis/tree/main/CrAg. Data included in analyses can be found in Tables 1 and 2.
Abbreviations
- CALAS:
-
Cryptococcal Antigen Latex Agglutination System
- CSF:
-
Cerebrospinal fluid
- CrAg:
-
Cryptococcal antigen
- EIA:
-
Enzyme immunoassay
- ELISA:
-
Enzyme-linked immunosorbent assay
- GXM:
-
Glucuronoxylomannan
- HIV:
-
Human immunodeficiency virus
- HSROC:
-
Hierarchical Summary Receiver Operating Characteristic
- LA:
-
Latex agglutination
- LFA:
-
Lateral flow assay
- MALDI-TOF:
-
Matrix-assisted laser desorption ionization–time-of-flight mass spectrometry
- PCR:
-
Polymerase chain reaction
- PLWH:
-
People living with HIV
- QUADAS:
-
Quality assessment of diagnostic-accuracy studies
- RCT:
-
Randomised controlled trial
References
Hagen F, et al. Recognition of seven species in the Cryptococcus gattii/Cryptococcus neoformans species complex. Fungal Genet Biol. 2015;78:16–48.
Kronstad JW, et al. Expanding fungal pathogenesis: Cryptococcus species break out of the opportunistic box James. Nat Rev Microbiol. 2011;9:193–203.
MacDougall L, Fyfe M, Romney M, Starr M, Galanis E. Risk factors for Cryptococcus gattii infection, British Columbia, Canada. Emerg Infect Dis. 2011;17:193–9.
Pyrgos V, Seitz AE, Steiner CA, Prevots DR, Williamson PR. Epidemiology of cryptococcal meningitis in the US: 1997–2009. PLoS ONE. 2013;8:e56269.
Bratton E, et al. Comparison and temporal trends of three groups with Cryptococcosis: HIV-infected, solid organ transplant, and HIV-negative/non-transplant. PLoS ONE. 2012;7:e43582.
Silveira FP, et al. Cryptococcosis in liver and kidney transplant recipients receiving anti-thymocyte globulin or alemtuzumab. Transpl Infect Dis. 2007;9:22–7.
Vijay S, Ingole N, Wanjare S, Mehta P. Prevalence of cryptococcaemia in HIV seropositive patients in an Indian setting. J Clin Diagnostic Res. 2019;13:DC01–4.
Pappas PG. Cryptococcal infections in non-HIV-infected patients. Trans Am Clin Climatol Assoc. 2013;124:61–79.
Chen J, et al. Cryptococcus neoformans strains and infection in apparently immunocompetent patients. China Emerg Infect Dis. 2008;14:755–62.
Tarumoto N, et al. Identification of disseminated cryptococcosis using MALDI-TOF MS and clinical evaluation. Med Mycol J. 2016;57:E41–6.
World Health Organisation. The diagnosis, prevention and management of cryptococcal disease in HIV-infected adults, adolescents and children. 2018.
Boulware DR, et al. Multisite validation of cryptococcal antigen lateral flow assay and quantification by laser thermal contrast. Emerg Infect Dis. 2014;20:45–53.
Hansen J, et al. Large-scale evaluation of the immuno-mycologics lateral flow and enzyme-linked immunoassays for detection of cryptococcal antigen in serum and cerebrospinal fluid. Clin Vaccine Immunol CVI. 2013;20:52–5.
Percival A, Thorkildson P, Kozel TR. Monoclonal antibodies specific for immunorecessive epitopes of glucuronoxylomannan, the major capsular polysaccharide of Cryptococcus neoformans, reduce serotype bias in an immunoassay for cryptococcal antigen. Clin Vaccine Immunol. 2011;18:1292–6.
Bridge S, et al. Evaluation of the biofire filmarray meningitis/encephalitis panel in and adult and pediatric Ugandan population. J Med Mycol. 2021;31: 101170.
Temfack JJB, Spijker R, Loyse A, Chiller T, Pappas PG, Perfect J, Sorell TC, Harrison TS, Cohen JF, Lortholary OER. Cryptococcal antigen in serum and cerebrospinal fluid for detecting Cryptococcal meningitis in adults living with human immunodeficiency virus: systematic review and meta-analysis of diagnostic test accuracy studies. Clin Infect Dis. 2021;72:1268–78.
Hopkins H, et al. Febrile illness evaluation in a broad range of endemicities (FIEBRE): protocol for a multisite prospective observational study of the causes of fever in Africa and Asia. BMJ Open. 2020;10: e035632.
von Hagen A, Balbi A, Arbildi C, Bonilla M. International prospective register of systematic reviews Citation Review question Participants/population Intervention (s), exposure (s) Comparator (s)/control Main outcome (s) International prospective register of systematic reviews Additional. Int Prospect Regist Syst Rev. 2018;1–4.
Falconer J. Removing duplicates from an EndNote Library. Library & Archives Service Blog. London School of Hygiene & Tropical Medicine (2018). Available at: https://blogs.lshtm.ac.uk/library/2018/12/07/removing-duplicates-from-an-endnote-library/.
Whiting PF, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011. https://doi.org/10.7326/0003-4819-155-8-201110180-00009.
Harrington K, et al. Evaluation of a cryptococcal antigen lateral flow assay and cryptococcal antigen positivity at a large public hospital in Atlanta, Georgia. Open Forum Infect Dis. 2021;8:123.
Murad MH, et al. Fixed-effects and random-effects models. in users’ guides to the medical literature: a manual for evidence-based clinical practice. In: Guyatt G, Rennie D, Meade MO, Cook DJ. (eds) 3rd edn. McGraw-Hill Education; 2015.
Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med. 2001;20:2865–84.
Dendukuri N, Schiller I, Joseph L, Pai M. Bayesian meta-analysis of the accuracy of a test for tuberculous pleuritis in the absence of a gold standard reference. Biometrics. 2012;68:1285–93.
Jullien S, et al. Diagnostic accuracy of multiplex respiratory pathogen panels for influenza or respiratory syncytial virus infections: systematic review and meta-analysis. BMC Infect Dis. 2022;22:1–11.
Stan Development Team. Stan Modeling Language Users Guide and Reference Manual. (2019). Available at: https://mc-stan.org. Accessed: 12th Dec 2021.
Chen M, et al. Evaluation of five conventional and molecular approaches for diagnosis of cryptococcal meningitis in non-HIV-infected patients. Mycoses. 2016;59:494–502.
Dubbels M, Granger D, Theel ES. Low cryptococcus antigen titers as determined by lateral flow assay should be interpreted cautiously in patients without prior diagnosis of cryptococcal infection. J Clin Microbiol. 2017;55:2472–9.
Wang X, et al. Evaluation of low cryptococcal antigen titer as determined by the lateral flow assay in serum and cerebrospinal fluid among HIV-negative patients: a retrospective diagnostic accuracy study. IMA Fungus. 2020;11:6.
Tintelnot K, Hagen F, Seibold M, Bernhardt A, Boekhout T. Are cryptococcoses due to Cryptococcus gattii underdiagnosed in Europe? Mycoses. 2012;55:277–8.
Min J et al. Pulmonary cryptococcosis: comparison of cryptococcal antigen detection and radiography in immunocompetent and immunocompromised patients. BMC Infect Dis. 2020; 20.
Jitmuang A, et al. Performance of the cryptococcal antigen lateral flow assay in non-HIV-related cryptococcosis. J Clin Microbiol. 2016;54:460–3.
Wu HH, Chen YX, Fang SY. Clinicopathological features of isolated pulmonary cryptococcosis in HIV-negative patients. J Int Med Res. 2020;48:030006052092787.
Hevey IA, Rauseo AM, Larson L, Powderly W, Spec AMAG. Performance of the lateral flow assay and the latex agglutination serum cryptococcal antigen test in cryptococcal disease in patients with and without HIV. J Clin Microbiol. 2020;58:21.
Dendukuri N, Joseph L. Bayesian approaches to modeling the conditional dependence between multiple diagnostic tests. Biometrics. 2001;57:158–67.
De Pauw B et al. Revised definitions of invasive fungal disease from the european organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (EORTC/MSG) C. Clin Infect Dis. 2008;46:1813–21.
Acknowledgements
Not applicable.
Funding
SHK is supported by the Medical Research Council London Intercollegiate Doctoral. Training Partnership Studentship (MR/N013638/1). The funders had no role in study design, data collection and analysis, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
CM, JE, HH, SHK and JNJ conceived the study. CM and JE assessed the eligibility of the studies, extracted the data, and assessed the methodological quality of the included studies. JF developed the search strategy and conducted the literature search. SHK carried out the statistical analysis. JB, RK and OB advised on the statistical analysis. CM, JE and SHK prepared the original draft of the manuscript, with considerable input from HH and JNJ. All authors contributed to the interpretations of results and all authors reviewed, edited and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search Methodology.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Macrae, C., Ellis, J., Keddie, S.H. et al. Diagnostic performance of the IMMY cryptococcal antigen lateral flow assay on serum and cerebrospinal fluid for diagnosis of cryptococcosis in HIV-negative patients: a systematic review. BMC Infect Dis 23, 209 (2023). https://doi.org/10.1186/s12879-023-08135-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08135-w