
Abstract
Background
Since its emergence in November 2021, SARS-CoV-2 Omicron clade has quickly become dominant, due to its increased transmissibility and immune evasion. Different sublineages are currently circulating, which differ in mutations and deletions in regions of the SARS-CoV-2 genome implicated in the immune response. In May 2022, BA.1 and BA.2 were the most prevalent sublineages in Europe, both characterized by ability of evading natural acquired and vaccine-induced immunity and of escaping monoclonal antibodies neutralization.
Case presentation
A 5-years old male affected by B-cell acute lymphoblastic leukemia in reinduction was tested positive for SARS-CoV-2 by RT-PCR at the Bambino Gesù Children Hospital in Rome in December 2021. He experienced a mild COVID-19 manifestation, and a peak of nasopharyngeal viral load corresponding to 15.5 Ct. Whole genome sequencing identified the clade 21 K (Omicron), sublineage BA.1.1. The patient was monitored over time and tested negative for SARS-CoV-2 after 30 days. Anti-S antibodies were detected positive with modest titre (3.86 BAU/mL), while anti-N antibodies were negative. 74 days after the onset of the first infection and 23 days after the last negative test, the patient was readmitted to hospital with fever, and tested positive for SARS-CoV-2 by RT-PCR (peak of viral load corresponding to 23.3 Ct). Again, he experienced a mild COVID-19. Whole genome sequencing revealed an infection with the Omicron lineage BA.2 (21L clade). Sotrovimab administration was started at the fifth day of positivity, and RT-PCR negativity occurred 10 days later. Surveillance SARS-CoV-2 RT-PCR were persistently negative, and in May 2022, anti-N antibodies were found positive and anti-S antibodies reached titres > 5000 BAU/mL.
Conclusions
By this clinical case, we showed that SARS-CoV-2 reinfection within the Omicron clade can occur and can be correlated to inadequate immune responses to primary infection. We also showed that the infection’s length was shorter in the second respect to first episode, suggesting that pre-existing T cell-mediated immunity, though not preventing re-infection, might have limited the SARS-CoV-2 replication capacity. Lastly, Sotrovimab treatment retained activity against BA.2, probably accelerating the viral clearance in the second infectious episode, after which seroconversion and increase of anti-S antibodies titres were observed.
Similar content being viewed by others


Background
Risk of SARS-CoV-2 reinfection has been widely described since the first phases of the pandemic, regardless of the community infection rates, and mainly in immunocompromised individuals. This fragile population is indeed particularly susceptible to flare and lack of response to vaccination due to impaired humoral immunity and ability to produce neutralizing antibodies [1,2,3,4].
While no change in the SARS-CoV-2 reinfection risk was observed in the general as well as in paediatric population throughout all the first epidemic waves [5], the frequency of SARS-CoV-2 reinfection cases has started to significantly increase concomitantly with the emergence of the Omicron variant [6].
SARS-CoV-2 Omicron lineage was first reported in November 2021 in South Africa and quickly spread, immediately becoming the dominant lineage worldwide [7, 8]. This lineage is characterised by several mutations in key regions of the SARS-CoV-2 genome, as well as RDB domain in the spike protein, that confer to Omicron increased transmissibility and escape against naturally acquired, vaccine-induced immunity, and mAbs treatment [9,10,11]. BA.1 and BA.2 were the most prevalent sublineages characterizing Omicron clade in Europe since May 2022 [12]. These 2 lineages do not differ for infectivity and neutralization sensitivity to omicron-infected and vaccinated patients’ sera, [13, 14] notwithstanding some amino acid mutations and deletions occurring in SARS-CoV-2 spike protein differentiated them [15]. Most of mAbs lost their efficacy against all Omicron lineages, and initial in vitro data reports a 27-fold decrease in the neutralizing activity of Sotrovimab against the BA.2 respect to BA.1 [16], suggesting a potentially reduced efficacy of Sotrovimab against BA.2 and forthcoming Omicron lineages.
Here we describe a case of Omicron intra-clade reinfection efficiently resolved after Sotrovimab administration in a patient affected by a B-cell acute lymphoblastic leukaemia. Whole genome sequencing of samples from the two distinct infection episodes revealed the presence of BA.1 and BA.2 sublineages of the Omicron clade.
Case presentation
A 5-years old Caucasian male patient affected by B-cell acute lymphoblastic leukaemia (Table 1) treated according to the AIEOP BFM Protocol ALL 2017 (Protocol Identifier: NCT03643276) [17] was admitted at the Bambino Gesù Children Hospital IRCCS in Rome in December 2021 and was tested negative to SARS-CoV-2 by RT-PCR in the context of hospital screening (Additional file 1: Figure S1). The patient was not vaccinated against SARS-CoV-2. After 4 days from admission, he started to manifest fever and was subjected to a nasopharyngeal swab, which resulted positive to SARS-CoV-2 with a mean Ct value of 26.65 by RT-PCR (Fig. 1 and Additional file 2: Table S1) (day 1 of SARS-CoV-2 infection). The patient experienced a mild COVID-19 with fever and without symptoms at lower respiratory airways, except for a peribronchial thickening observed at the chest X-rays. The viral load peak was observed at day 4, when the mean Ct value was 15.55 (Fig. 1 and Additional file 2: Table S1). SARS-CoV-2 whole genome sequencing revealed the presence of clade 21 K (Omicron), sublineage BA.1.1 (Figs. 1 and 2). The patient continued to test positive at the nasopharyngeal swab by RT-PCR until day 31, when the RT-PCR resulted negative (Fig. 1 and Additional file 2: Table S1). At days 15 and 16, the antibodies against SARS-CoV-2 spike (anti-S) and nucleocapsid (anti-N) were monitored, revealing low levels of anti-S (3.85 and 3.86 BAU/mL, respectively; cut-off < 0.8) and absence of anti-N (Fig. 1). At day 52, 3 weeks after the RT-PCR negative result, a nasopharyngeal swab antigenic test was performed, confirming again the negativity to SARS-CoV-2.

SARS-CoV-2 viral load expressed as mean Ct values obtained by real time PCR over time. The dotted line indicates the SARS-CoV-2 undetectability. CT cycle threshold values, RT-PCR real-time polymerase chain reaction, TND target not detected, Ab antibodies

Phylogenetic tree. Estimated maximum likelihood (ML) phylogeny of SARS-CoV-2 genomes from two samples of the same patient (red). Representative Omicron BA.1 and BA.2 genomes retrieved by GISAID (n = 34) (black) were also included. The ML phylogeny was estimated with IqTree using the best-fit model of nucleotide substitution TrN + I + G4 with 1000 replicates fast bootstrapping
After 74 days since the onset of the first infection and 23 days after the last negativity, the patient was re-admitted at the hospital with fever. At day 1, a nasopharyngeal swab resulted positive for SARS-CoV-2 by RT-PCR, with a mean Ct value of 23.3 (Fig. 1 and Additional file 2: Table S1). The SARS-CoV-2 whole genome sequencing revealed an infection with the Omicron BA.2 sublineage, clade 21L (Figs. 1 and 2). At day 5, antibody testing revealed low levels of anti-S (3.05 BAU/mL; cut-off < 0.8), whereas no anti-N antibodies were detected (Fig. 2). As in the first episode, the patient experienced a mild infection, and exclusively reported fever and upper respiratory airways symptoms. At day 1, he presented low neutrophils counts and G-CSF was administered since day 4. At day 6, Sotrovimab was administered according to hospital’s policy [18] and its higher reported efficacy against Omicron BA.2 lineage compared to the combinations bamlanivimab plus etesevimab and casirivimab plus imdevimab [19]. Nasopharyngeal swabs were repeated at days 8 and 10, resulting in a progressive drop of viral load (mean Ct: 27.88 and 31.85, Fig. 1 and Additional file 2: Table S1).
After 15 days since the onset of symptoms, the patient resulted negative to a nasopharyngeal antigenic test. Thirty-eight days after negative antigenic test, patient was subjected to serological tests that revealed high levels of anti-S (> 5000 BAU/mL; cut-off < 0.8) and anti-N antibodies (13.91 Index).
For details regarding material and methods refer to Additional file 3.
Discussion and conclusions
The case here described was categorized as a reinfection according to the US Center for Disease Control and Prevention (CDC) criteria for reinfection [20] and to the European Center for Disease Prevention and Control (ECDC) criteria [21]. In particular, both infections were mild symptomatic, and the second infection occurred 74 days after the onset of the first infection. Respiratory specimens were available for both episodes at different time points and every episode had at least one associated positive RT-PCR test.
The first infection, due to the BA.1.1 sublineage, was characterised by high viral load, and a rather long positivity (30 days). Final negativity was confirmed by two different tests at different time-points. Serological data revealed that anti-N antibodies were absent during and after the first infection, while the level of anti-S antibodies remained low. Low levels of anti-S and no anti-N antibodies were indeed evident at the day 5 of the second infection. These data confirm that the patient developed little or no detectable antibodies after the first infection, consistent with a failure in mounting an effective protective immunity, and thus associated to increased risk of reinfection [1,2,3,4]. These findings underlie the importance of vaccination in immunocompromised patients, to both elicit an immune response in those who responded to the primary infection, and to induce a de novo response in those who did not mount a detectable antibody response during primary infections [22].
Beyond the immune status, other factors may influence the risk of re-infection, like the spread of genetically distinct lineage of SARS-CoV-2, characterized by several non-synonymous mutations in the S region, that could lead to immune evasion [9,10,11,12]. At this regard, even if the sublineage BA.2 is not associated with an increased transmissibility and immune evasion than the lineage BA.1 [13, 14], reinfections by the BA.2 shortly after a previous BA.1 infection have been recently described, mostly in not vaccinated, young individuals [23]. Consistent with these findings, our clinical case was a SARS-CoV-2 unvaccinated immunocompromised child, experiencing a BA.2 reinfection after a previous BA.1.1 infection. Second infection was characterized by a shorter period of positivity (15 days) compared to the first infection. In absence of a few viral load quantification tests in the days of second infection and before Sotrovimab administration, we cannot speculate about a lower peak of viral load in the second infection respect to the first infection, but the shorter duration (15 days) of the second infection compared to the first (30 days) might indicate a more superficial and transient secondary infection. Of note, the rapid viral load drop observed in the second infection could be driven by the T cell-mediated immunity obtained during the first infection [24] supporting the hypothesis that the first infection might have acted by ‘priming’ the immune system. This drop could also have been accelerated by Sotrovimab administration at the beginning of the second episode. Although a decrease in the neutralizing activity of Sotrovimab against the BA.2 sublineage is suggested [16], in this clinical case Sotrovimab treatment retains activity. After the second infection, anti-N seroconversion and increase of anti-S titres were also observed. Interestingly, Sotrovimab administration has been recently suggested to enhance serum SARS-CoV-2 S antibody levels in patients infected with the SARS-CoV-2 Omicron clade [25]. Thus, T cell-mediated immunity and Sotrovimab administration might result in additive or synergistic effect able to finally promote the resolution of the second infection.
In conclusion, by this clinical case we showed that SARS-CoV-2 reinfection within the Omicron clade can occur and can be correlated to inadequate immune responses to primary infection. We also showed that nasopharyngeal viral load was lower in the second respect to first episode, suggesting that pre-existing T cell-mediated immunity, though not preventing re-infection, might have limited the nasopharyngeal viral load. Sotrovimab treatment also retained activity against BA.2, probably accelerating the viral clearance in the second infectious episode, after which seroconversion and increase of anti-S antibodies titres were observed. Lastly, our study highlights the importance of a full vaccination strategy in immunosuppressed individuals for the prevention of SARS-CoV-2 infection and for the mounting of an adequate immune response against viral replication.
Availability of data and materials
The two SARS-CoV-2 sequences characterizing the first and the second infection episode are openly available on GISAID portal under the accession numbers EPI_ISL_13810381 and EPI_ISL_13810380, respectively. All the other data generated or analysed during this study are included in this published article [and its additional information files].
Abbreviations
- BAU:
-
Binding arbitrary unit
- CDC:
-
US Center for Disease Control and Prevention
- COI:
-
Cut off index
- COVID-19:
-
Coronavirus disease 2019
- Ct:
-
Cycle threshold
- ECDC:
-
European Center for Disease Prevention and Control
- ECLIA:
-
Electro-chemiluminescence sandwich immunoassay
- G-CSF:
-
Granulocyte colony-stimulating factor
- mAbs:
-
Monoclonal antibodies
- N:
-
Nucleocapsid
- RT-PCR:
-
Real-time reverse transcription polymerase chain reaction
- S:
-
Spike
- SARS-CoV-2:
-
Severe Acute Respiratory Syndrome Coronavirus 2
References
Jeffery-Smith A, Rowland TAJ, Patel M, Whitaker H, Iyanger N, Williams SV, Giddings R, Thompson L, Zavala M, Aiano F, Ellis J, Lackenby A, Höschler K, Brown K, Ramsay ME, Gopal R, Chow JY, Ladhani SN, Zambon M. Reinfection with new variants of SARS-CoV-2 after natural infection: a prospective observational cohort in 13 care homes in England. Lancet Healthy Longev. 2021;2(12):e811–9. https://doi.org/10.1016/S2666-7568(21)00253-1.4.
Herishanu Y, Rahav G, Levi S, Braester A, Itchaki G, Bairey O, Dally N, Shvidel L, Ziv-Baran T, Polliack A, Tadmor T, Benjamini O. Efficacy of a third BNT162b2 mRNA COVID-19 vaccine dose in patients with CLL who failed standard 2-dose vaccination. Blood. 2022;139(5):678–85. https://doi.org/10.1182/blood.2021014085.
Booth S, Curley HM, Varnai C, Arnold R, Lee LYW, Campton NA, Cook G, Purshouse K, Aries J, Innes A, Cook LB, Tomkins O, Oram HS, Tilby M, Kulasekararaj A, Wrench D, Dolly S, Newsom-Davies T, Pettengell R, Gault A, Moody S, Mittal S, Altohami M, Tillet T, Illingworth J, Mukherjee L, Apperly J, Ashcroft J, Rabin N, Carmichael J, Cazier JB, Kerr R, Middleton G, Collins GP, Palles C, UKCCMP team. Key findings from the UKCCMP cohort of 877 patients with haematological malignancy and COVID-19: disease control as an important factor relative to recent chemotherapy or anti-CD20 therapy. Br J Haematol. 2022;196(4):892–901. https://doi.org/10.1111/bjh.17937.
Liebers N, Speer C, Benning L, Bruch PM, Kraemer I, Meissner J, Schnitzler P, Kräusslich HG, Dreger P, Mueller-Tidow C, Poschke I, Dietrich S. Humoral and cellular responses after COVID-19 vaccination in anti-CD20-treated lymphoma patients. Blood. 2022;139(1):142–7. https://doi.org/10.1182/blood.2021013445.
Nordström P, Ballin M, Nordström A. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: a retrospective, total population cohort study in Sweden. Lancet Infect Dis. 2022;22(6):781–90. https://doi.org/10.1016/S1473-3099(22)00143-8.
Pulliam JRC, van Schalkwyk C, Govender N, von Gottberg A, Cohen C, Groome MJ, Dushoff J, Mlisana K, Moultrie H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science. 2022;376(6593):e4947. https://doi.org/10.1126/science.abn4947.
Callaway E. Heavily mutated Omicron variant puts scientists on alert. Nature. 2021;600(7887):21. https://doi.org/10.1038/d41586-021-03552-w. (PMID: 34824381).
World Health Organisation (WHO). https://www.who.int/en/activities/tracking-SARS-CoV-2-variants. Accessed 17 May 2022.
Liu L, Iketani S, Guo Y, Chan JF, Wang M, Liu L, Luo Y, Chu H, Huang Y, Nair MS, Yu J, Chik KK, Yuen TT, Yoon C, To KK, Chen H, Yin MT, Sobieszczyk ME, Huang Y, Wang HH, Sheng Z, Yuen KY, Ho DD. Striking antibody evasion manifested by the Omicron variant of SARS-CoV-2. Nature. 2022;602(7898):676–81. https://doi.org/10.1038/s41586-021-04388-0.
Cele S, Jackson L, Khoury DS, Khan K, Moyo-Gwete T, Tegally H, San JE, Cromer D, Scheepers C, Amoako DG, Karim F, Bernstein M, Lustig G, Archary D, Smith M, Ganga Y, Jule Z, Reedoy K, Hwa SH, Giandhari J, Blackburn JM, Gosnell BI, Abdool Karim SS, Hanekom W, NGS-SA; COMMIT-KZN Team, von Gottberg A, Bhiman JN, Lessells RJ, Moosa MS, Davenport MP, de Oliveira T, Moore PL, Sigal A. Omicron extensively but incompletely escapes Pfizer BNT162b2 neutralization. Nature. 2022;602(7898):654–6. https://doi.org/10.1038/s41586-021-04387-1.
Hu J, Peng P, Cao X, Wu K, Chen J, Wang K, Tang N, Huang AL. Increased immune escape of the new SARS-CoV-2 variant of concern Omicron. Cell Mol Immunol. 2022;19(2):293–5. https://doi.org/10.1038/s41423-021-00836-z.
https://www.ecdc.europa.eu/en/covid-19/variants-concern. Last access May 24, 2022.
Arora P, Zhang L, Rocha C, Sidarovich A, Kempf A, Schulz S, Cossmann A, Manger B, Baier E, Tampe B, Moerer O, Dickel S, Dopfer-Jablonka A, Jäck HM, Behrens GMN, Winkler MS, Pöhlmann S, Hoffmann M. Comparable neutralisation evasion of SARS-CoV-2 omicron subvariants BA.1, BA.2, and BA.3. Lancet Infect Dis. 2022. https://doi.org/10.1016/S1473-3099(22)00224-9.
Evans JP, Zeng C, Qu P, Faraone J, Zheng YM, Carlin C, Bednash JS, Zhou T, Lozanski G, Mallampalli R, Saif LJ, Oltz EM, Mohler PJ, Xu K, Gumina RJ, Liu SL. Neutralization of SARS-CoV-2 Omicron sub-lineages BA.1, BA.1.1, and BA.2. Cell Host Microbe. 2022. https://doi.org/10.1016/j.chom.2022.04.014.
Majumdar S, Sarkar R. Mutational and phylogenetic analyses of the two lineages of the Omicron variant. J Med Virol. 2022;94(5):1777–9. https://doi.org/10.1002/jmv.27558.
Iketani S, Liu L, Guo Y, Liu L, Chan JF, Huang Y, Wang M, Luo Y, Yu J, Chu H, Chik KK, Yuen TT, Yin MT, Sobieszczyk ME, Huang Y, Yuen KY, Wang HH, Sheng Z, Ho DD. Antibody evasion properties of SARS-CoV-2 Omicron sublineages. Nature. 2022;604(7906):553–6. https://doi.org/10.1038/s41586-022-04594-4.
https://clinicaltrials.gov/ct2/show/NCT03643276. Accessed 30 January 2023.
Romani L, Calò Carducci FI, Chiurchiù S, Cursi L, De Luca M, Di Giuseppe M, Krzysztofiak A, Lancella L, Palma P, Vallesi L, Corsetti T, Campana A, Nicastri E, Rossi P, Bernardi S. Safety of monoclonal antibodies in children affected by SARS-CoV-2 infection. Children (Basel). 2022;9(3):369. https://doi.org/10.3390/children9030369.
https://covdb.stanford.edu/susceptibility-data/table-mab-susc/. Accessed 30 January 2023
Centers for Disease Control and Prevention. (CDC) https://www.cdc.gov/coronavirus/2019-ncov/php/invest-criteria.html. Accessed 17 May 2022.
European Centre for Disease Prevention and Control. (ECDC). https://www.ecdc.europa.eu/en/publications-data/reinfection-sars-cov-2-implementation-surveillance-case-definition-within-eueea. Accessed 17 May 2022.
Parker EPK, Desai S, Marti M, et al. Response to additional COVID-19 vaccine doses in people who are immunocompromised: a rapid review. Lancet Glob Health. 2022;10(3):e326–8. https://doi.org/10.1016/S2214-109X(21)00593-3.
Stegger M, Edslev SM, Sieber RN, Ingham AC, Ng KL, Tang MHE, Alexandersen S, Fonager J, Legarth R, Utko M, Wilkowski B, Gunalan V, Bennedbaek M, Byberg-Grauholm J, Møller CH, Christiansen LE, Svarrer CW, Ellegaard K, Baig S, Johannesen TB, Espenhain L, Skov R, Cohen AS, Larsen NB, Sørensen KM, White ED, Lillebaek T, Ullum H, Krause TG, Fomsgaard A, Ethelberg S, Rasmussen M. Occurrence and significance of Omicron BA.1 infection followed by BA.2 reinfection. MedRxiv. 2022. https://doi.org/10.1101/2022.02.19.22271112.
Riou C, Keeton R, Moyo-Gwete T, et al. Escape from recognition of SARS-CoV-2 439 variant spike epitopes but overall preservation of T cell immunity. Sci Transl Med. 2022;14(631):e6824. https://doi.org/10.1126/scitranslmed.abj6824.
Fujimoto K, Mutsuo S, Yasuda Y, Arasawa S, Tashima N, Iwashima D, Takahashi K-I. Treatment with sotrovimab and casirivimab/imdevimab enhances serum SARS-CoV-2 S antibody levels in patients infected with the SARS-CoV-2 delta, omicron BA.1, and BA.5 variants. Infect Dis Rep. 2022;14:996–1003. https://doi.org/10.3390/idr14060099.
Acknowledgements
We thank Fondazione ANIA that financially supported this work. The authors also thank Valerio Di Gioacchino and the whole staff of the Microbiology Laboratory of Ospedale Pediatrico Bambino Gesù IRCCS for outstanding technical support in processing swab samples, performing laboratory analyses and data management.
Funding
This research was funded by Fondazione ANIA (Associazione nazionale fra le imprese assicuratrici). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
RS, VFo performed data analysis, data interpretation, writing; MADI, AM, FL performed clinical evaluation and help in data interpretation and writing; VFi, AG processed samples; LC and CR help in data processing; VC performed initial bioinformatic analyses; CA and CFP conceived the clinical case. All authors revised and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by local Research Ethics Committee of OPBG (prot. 2904/2022). This study was conducted in accordance with the principles of the 1964 Declaration of Helsinki. Written informed consent to participate in this study was obtained by the patient’s parents. The data used in this study were anonymized before use.
Consent to publication
Written informed consent was obtained by patient’s parents.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
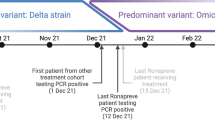
Additional file 1: Figure S1.
A timeline of the case. Hospitalization, symptoms, diagnosis test (Antigenic test and RT-PCR); serology, administered treatments, and date of sequencing were reported. aMild: including symptoms of upper respiratory airways (cough, sore throat, runny nose, sneezing, rhinitis, pharyngo-adenitis, laryngitis). Ab: antibody; CT: Cycle threshold values; RT-PCR: real-time polymerase chain reaction.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Scutari, R., Fox, V., De Ioris, M.A. et al. A case of SARS-CoV-2 Omicron reinfection resulting in a significant immunity boost in a paediatric patient affected by B-cell acute lymphoblastic leukemia. BMC Infect Dis 23, 133 (2023). https://doi.org/10.1186/s12879-023-08111-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08111-4