
Abstract
Background
Dengue is one of the most common arboviral diseases with increased outbreaks annually in tropical and subtropical areas. In Ethiopia, there are no data regarding clinical, hematological and biochemical parameters which are very important in the clinical management of dengue patients. Hence this study was carried out to provide the first baseline data of clinical, hematological and biochemical profiles of patients infected with dengue virus.
Methods
A cross-sectional study was carried out among febrile patients in northwest Ethiopia from March 2016 to May 2017. Blood samples were collected from dengue presumed cases and tested against dengue specific IgM antibody by enzyme-linked immunosorbent assay (ELISA). Those study participants who fulfilled the inclusion criteria were enrolled in the study. Clinical examination findings were recorded, hematological and biochemical parameters tests were done.
Results
During the study period, a total of 102 dengue cases were included in the study. Of these, there were 16 (15.7%) children and 86 (84.3%) adults between 1 and 76 year age. The most common clinical presentations followed by fever (100%) were a headache 89 (87.3%), myalgia 82 (80.4%), nausea/vomiting 71 (69.6%). The common hematological findings were thrombocytopenia 61 (59.8%), followed by anemia 45 (44.1%) and leucopenia 27 (26.5%) and the elevated levels of biochemical parameters were AST 46 (45.1%) and ALT in 18 (17.6%).
Conclusions
This study highlights the most common clinical and laboratory profiles of dengue viral infections that could alert physicians to the likelihood of dengue virus infections in the study area.
Similar content being viewed by others

Background
Dengue is a mosquito-borne arboviral disease and is a major global public health threat that is prevalent in tropical and sub-tropical regions of the world, mostly in urban and semi-urban areas [1]. The WHO estimates, more than 2.5 billion individuals live at risk of dengue transmission in more than 100 countries and approximately 50-100 million individuals have infected with dengue annually [2]. Of these, 500,000 severe dengue cases are diagnosed each year resulting in 24,000 deaths per year [3,4,5,6]. Dengue is endemic in the WHO regions of Africa, the Americas, the Eastern Mediterranean, South-East Asia, and the Western Pacific regions and the Caribbean [7]. In the recent decades, the global incidence of dengue virus (DENV) infection has increased with increasing geographic expansion to new countries [8]. The threat of a possible outbreak of dengue for the first time reported from Ethiopia in 2013 in Dire Dawa. In this outbreak, 11, 409 dengue suspected cases within four months were reported. Fifty (50/88; 56.8%) samples were reported positive for dengue infection and mostly affected age groups were 15-44 year-olds [9]. Dengue cases were also later reported in 2014 from Somali Regional state of Ethiopia, in which 33 (33/57, 57.9%) samples were reported positive for dengue [10].
The leading contributing factors for widespread and increasing dengue incidences are rapid unplanned urbanization and migration of population to urban areas, poor sanitation facilities contributing fertile breeding areas for mosquitoes, lack of vector control and climatic changes [11]. As mosquitoes are widely distributed in Africa and can serve as vectors of dengue virus, when these combined with rapid population growth, unplanned urbanization, and increased international travel, could increase the epidemic risk in African countries [12].
Specific treatment for dengue is not available, but early detection and fluid replacement therapy and use of analgesics and antipyretics with good nursing care ensures marked reduction of the mortality rates 20% to less than 1% due to severe cases [13]. In clinical practice, as it is known, the patient's diagnosis and management are based on clinical manifestations and abnormal laboratory findings [14]. Initial DENV infection may be asymptomatic [15] or may result in a nonspecific febrile illness typically present with the sudden onset of fever, severe headache, bone, joint and muscular pains, mild bleeding manifestation, weakness, myalgia, and rash [16]. All these clinical presentations are similar to many other febrile diseases prevalent in the country; such as malaria, Kala-azar and typhoid fever which pose a diagnostic challenge of dengue [17].
Dengue is caused by infection with any one of the four serotypes of DENV which is an arbovirus single-stranded RNA virus of the genus Flavivirus [18]. Infection with one dengue serotype provides lifelong homotypic immunity to that particular serotype. Different serotypes can be in circulation during an epidemic, and thus, a person can eventually be infected as many as four times, once with each serotype [19]. It is well documented that subsequent infection with different DENV serotypes increases the risk of developing severe dengue [20, 21]. Infection with dengue can be diagnosed by using clinical presentations and laboratory tests. Of the laboratory tests, non-specific tests; like hematological parameters, liver function tests, and serum protein concentration and specific tests; such as viral antigen test, genomic sequence, and serology for antibody detection are used [22, 23].
Dengue was noticed recently in Ethiopia but there is no data concerning clinical and laboratory profiles of the cases with dengue in the country. Physicians should be aware of the most common clinical as well as hematological and biochemical presentations which are important for the clinical management of patients and thus crucial for saving a life. Therefore, this study aimed to highlight the most common clinical features, hematological and biochemical findings of dengue cases.
Methods
Study area and participants
A cross-sectional prospective, hospital-based study was carried out in Metema and Humera Kahsay Abera hospitals, northwest Ethiopia from March 2016 to May 2017.
Inclusion criteria
Febrile patients who were presumed for dengue infection based on 2009 WHO criteria [8] and serologically confirmed with dengue specific IgM antibody. The febrile patient is referred to one whose axillary temperature is ≥ 38 oC.
Exclusion criteria
Cases confirmed as malaria, Kala-azar, typhoid fever, and any other confirmed chronic diseases were excluded in the study.
Data collection
Clinical examinations were performed by a physician on each study participant. Demographic variables, as it has been published in previous work, [24] and clinical profiles of study participants were collected by nurses using the structured questionnaire. The diagnosis of dengue was made based on positive enzyme-linked immunosorbent (ELISA; manufactured by EUROIMMUN diagnostics) [25] assay result for specific IgM antibody for dengue in serum. All the routine investigations such as hematological determination like total leukocyte count (TLC), differential leukocyte count, platelet count; hemoglobin (Hgb) and hematocrit (Hct) were determined by the automated blood analyzer (CELL-DYN 1800, Abbott Laboratories Diagnostics Division, USA). Thick and thin blood smear for malaria parasite, biochemical tests; AST and ALT for liver function tests, creatinine, and BUN for renal function tests and total protein were done by the automated biochemistry analyzer (Vegasys) [26]. The cutoff values of each test results were considered based on reference ranges used by the laboratory. Furthermore, medical charts of all dengue specific IgM positive cases were reviewed for the collection of other information (i.e. Kala-azar, typhoid fever, and any other confirmed chronic cases).
Statistical analysis
Data were entered and analyzed using the SPSS 20.0 statistical software. Descriptive statistic was used to calculate frequency and percentage. Data were presented by using tables and figure.
Results
Clinical profiles of dengue cases during a hospital visit
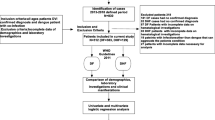
During the study period, 600 febrile patients who were presumed for dengue viral infections based on 2009 the WHO criteria were tested for dengue-specific IgM antibody. Of these, 114 patients were positive for dengue. Out of positive cases, 102 (89.5%) were included in this study while the remaining 12 (10.5%) were not included in the study due to co-morbidities (Fig. 1). Seventy-eight (78/102; 76.5%) study participants were males. A study participants’ age varied from 1 year to 76 years. Eighty sex (86/102; 84.3%) study participants were ≥ 15 years (Table 1). The commonest clinical feature was fever, 102 (100%), followed by headache in 89 (89/102; 87.3%), myalgia 82 (82/102; 80.4%), nausea/vomiting 71 (71/102; 69.6%), abdominal pain 61 (61/102; 59.8%), eye pain and mucosal bleeding 38 (38/102; 37.3%) in each of the cases, conjunctival hemorrhage and hepatomegaly 23 (23/102, 22.5%) in each of the cases. Rashes and tourniquet test in 13 (13/102; 12.7%) and 8 (8/102; 7.8%) of cases were seen, respectively (Table 2).

Flow chart of the study
Hematological profiles of dengue cases during a hospital visit
The most common hematological finding observed was thrombocytopenia (platelet count < 140,000/cumm) in 61 (61/102; 59.8%), followed by anemia (hemoglobin level < 11.5 g/dl) in 45 (45/102; 44.1%) and leucopenia (total leukocyte count < 4,000/cumm) in 27 (27/102; 26.5%) of the cases. Hematocrit > 44% were noted in 10 (10/102; 9.8%) of the cases and it ranged between 9-51%. Neutrophil < 1500 in 16 (16/102; 15.7%) and lymphocyte > 2900 in 2 (2/102; 2%) of the cases were noticed (Table 3).
Biochemical parameters of dengue cases at the time of hospital visit
The results of the biochemical investigation revealed that alanine aminotransferase (ALT) level > 42 IU/L was observed in 18 (18/102; 17.6%) of cases and aspartate aminotransferase (AST) level > 37 IU/L observed in 46 (46/102; 45.1%) of cases. The levels of ALT and AST ranged between 4-347 IU/L and 8-320 IU/L, respectively. Creatinine level > 1.1 mg/dl was observed in 20 (20/102; 19.6%) and BUN > 23.5 mg/dl noted in 15 (15/102; 14.7%) of cases. Hypoproteinaemia (total protein value < 6.6 mg/dl) was observed in 22 (22/102; 21.6%) cases (Table 4).
Discussion
In recent decades, the global prevalence of dengue has increased dramatically due to the limitations of currently available control strategies, such as vaccines and pesticides [27, 28]. Hence early diagnosis and proper medical management are of prime importance. As dengue is a recently known problem in Ethiopia [9, 10], the knowledge regarding its clinical presentations along with laboratory tests is vital for patient management. Hence, this study emphasized to document the first baseline data on clinical manifestations, hematological and biochemical parameters of patients with dengue illness in the country. The evidence generated is crucial for proper management of dengue patients.
In this study, the most frequent clinical presentation was fever, followed by a headache, myalgia, nausea/vomiting and abdominal pain, which is in agreement with the other studies [29, 30]. Rash was seen in 12.7% and hepatomegaly in 22.5% of the cases in our study while in another similar study 28.1% and 12.5% of patients presented with rash and hepatomegaly, respectively [31]. Bleeding diathesis is a common clinical presentation of dengue due to low platelet count and leakage from blood vessels. This is due to the interaction of dengue virus with host cells which cause the release of excess cytokines and stimulation of immunologic mechanism causing vascular endothelial alteration, infiltration of mononuclear cells and perivascular edema [32]. In our study mucosal bleeding was observed in most of the patients, which is in agreement with the other study [33], but in contrast to another study which showed cutaneous bleeding as the most common hemorrhagic manifestation [34]. In another study, hemorrhagic manifestation in the form of petechiae only was reported [31]. The variations in the clinical presentation of different studies might be due to the difference in the strain of the virus and its virulence factor.
Among the hematological profiles, thrombocytopenia was the most common finding in the present study which is consistent with the other studies [35, 36]. Thrombocytopenia might be due to decreased production of platelets due to suppression of the bone marrow by a virus and also due to binding of dengue antigens to platelets and increased antibody mediated immunological destruction of platelets [37, 38]. Leucopenia is one of the hematological parameters which occurs in people who were afflicted with dengue bone marrow suppression [38]. In our study, leucopenia was observed in 26.5% of the cases while in other studies elsewhere leucopenia was observed in 56.9% [39] and in 50% of the cases [40].
Hemoglobin levels less than the cutoff values were observed in 45 (44.1%) of the cases. This could be due to mucosal bleeding in which 38 (37.3%) of the cases had bleeding. This finding is consistent with another study [41]. Increased hematocrit was observed in 6.9% of cases in our study while it is less than the observation of the others studies which was reported 50% [42] and 27% [40] rise in hematocrit value. This might be related to increased severity and is elucidated by the hemoconcentration due to increased intravascular plasma permeability which is the basic pathophysiological changes in dengue.
In this study, higher levels than the normal values of AST in 45.1% and ALT in 17.6% of the cases were observed which showed elevated levels of AST in a greater proportion of cases than ALT. This is in agreement with the other studies elsewhere that reported AST and ALT higher levels in 68.5% and 39.2% of the cases, respectively [43] and similar findings were also reported elevated AST in 72.7% and ALT in 27.3% of cases elsewhere [44]. Dengue virus is hepatotrophic and also damages other organs; hence the observed pattern could be explained due to excess release of AST from damaged muscle cells (nonhepatic source) during infection that leads to more deranged AST than ALT. The ALT is mainly associated with hepatocytes, with the smallest activity in cardiac and skeletal muscle and AST is found in erythrocytes, kidney and brain tissue, cardiac and skeletal muscle and is usually raised because of damage to those sources and response to hepatic damage [45].
The serum creatinine and blood urea (BUN) levels were raised in 19.6% and 14.7% of the cases, respectively. These could be due to a direct viral effect on the glomerular and tubular cells or as a result of tissue injury caused by deregulated host immune response against the viral antigens [46]. Hypoproteinemia was observed in 21.6% of the cases. This could be probable that the complex interaction between virus, host immune response and endothelial cells, may affect the barrier integrity and functions of the vascular endothelial cells leading to plasma leakage causing hypoproteinemia [47].
Although this is the first effort to study clinical, hematological and biochemical profiles of dengue viral infection in Ethiopia, the study has several limitations. Comparisons of those dengue cases with the control group and serial hematological and biochemical changes were not done due to the nature of cross-sectional study design. These could be done in the future for better understanding of dengue viral infection presentation. Regardless of the depicted limitations, this preliminary study ultimately provides the first baseline data on clinical and laboratory profiles of dengue viral infection in the country.
Conclusion
Awareness of clinical features, as well as laboratory findings like hematological and biochemical parameters, are the most important guide to therapy and prognosis of dengue. In this study, fever followed by a headache and myalgia were commonest presenting complaints of dengue patients. Thrombocytopenia, anemia, leucopenia and elevated levels of AST were identified as the most common findings. Thus, these findings should prompt physicians on the probability of dengue infection in the study area.
Abbreviations
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- BUN:
-
Blood Urea
- DENV:
-
Dengue Virus
- ELISA:
-
Enzyme-Linked Immunosorbent Assay
- HCT:
-
Hematocrit
- IgM:
-
Immunoglobulin M
References
Engelthaler D, Fink T, Levy C, Leslie M. The reemergence of Aedes aegypti in Arizona. Emerg Infect Dis. 1997;3:241–2.
WHO. dengue and severe dengue. Fact sheet N 117 [cited 2018]. available from: http://www.searo.who.int/thailand/factsheets/fs0008/en/.
Gubler D. The global emergence/resurgence of arboviral diseases as public health problems. Arch Med Res. 2002;33:330–42.
Shepard D, Coudeville L, Halasa Y, Zambrano B, Dayan G. Economic impact of dengue illness in the Americas. Am J Trop Med Hyg. 2011;84:200–7.
Guha-Sapir D, Schimmer B. Dengue fever: new paradigms for a changing epidemiology. Emerg Themes Epidemiol. 2005;2. https://doi.org/10.1186/742-7622-2-1.
Natasha A, Mikkel B, Wilder-Smith A. Epidemiology of dengue: past, present and future prospects. Cl in Epidemiol. 2013;5:299–309.
Khan A, Hayat A, Masood N, Solangi N, Shaikh T. Frequency and clinical presentation of dengue fever at tertiary care hospital of Hyderabad/ Jamshoro. JLUMHS. 2010;9:88–94.
WHO-TDR. Dengue: guidelines for diagnosis, treatment, prevention and control- New Edition. Geneva: World Health Organisation; 2009.
Abyot BW, Mesfin M, Wubayehu K, Esayas K, Milliyon W, Abiy G, et al. The first acute febrile illness investigation associated with dengue fever in Ethiopia, 2013: A descriptive analysis. Ethiop J Health Dev. 2014;28:155–61.
Yusuf M, Salah A. Epidemiology of Dengue Fever in Ethiopian Somali Region: Retrospective Health Facility Based Study. Central African Journal of Public Health. 2016;2:51–6.
Dash A, Bhatia R, Sunyoto T, Mourya D. Emerging and re-emerging arboviral diseases in Southeast Asia. J Vector Borne Dis. 2013;50:77–84.
Gubler D. The changing epidemiology of yellow fever and dengue, 1900 to 2003. Immunol Microbiol Infect Dis. 2004;27:319–30.
WHO report on global surveillance of epidemic prone infectious diseases. World Health Organization, Geneva. 2005.
Kalayanarooj S, Vaughn D, Nimmannitya S, Green S, Suntayakorn S, Kunentrasai N, et al. Early clinical and laboratory indicators of acute dengue illness. J Infect Dis. 1997;176:313–21.
Sabin A. Research on dengue during World War II. Am J Trop Med Hyg. 1952;1:30.
Karabatsos N. International catalogue of arthropod-borne viruses. 3rd ed. American Society for Tropical Medicine and Hygiene 1985
Ananda A, Joel N, Kuritsky G, William L, Harold S, Margolis H. Dengue virus infection in Africa. Emerg Infect Dis. 2011;17:1349–54.
Nisalak A, Endy T, Nimmannitya S, Kalayanarooj S, Thisayakorn U, Scott R, et al. Serotype specific Dengue Virus Circulation and Dengue disease in Bangkok, Thailand from 1973 - 1999. Am J Trop Med Hyg. 2003;68:191–202.
CDC. Imported Dengue--United States, 1998 and 1998. Morb MortalWkly Rep. 2000;49:248–5.
Narayanan M, Aravind M, Thilothammal N, Prema R, Sargunam C, Ramamurty N. Dengue fever epidemic in Chennai - A study of clinical profile and outcome. Indian Pediatr. 2002;39:1027–33.
Malavige G, Fernando S, Fernando D, Seneviratne S. Dengue viral infections. Postgrad Med J. 2004;80:588–601.
DePaula S, Fonseca B. Dengue: A review of the laboratory tests a clinician must know to achieve a correct diagnosis. Braz J Infect Dis. 2004;8:390–8.
Srichaikul T, Nimmannita S. Haematology in dengue and dengue haemorrhagic. Baillieres Best Pract Res Clin Haematol. 2000;13:261–76.
Getachew F, Moges T, Ebba A, Yitayih W, Demekech D, Endalamaw G, et al. A serologic study of dengue in northwest Ethiopia: Suggesting preventive and control measures. PLoS Negl Trop Dis. 2018;12:e0006430.
EUROIMMUN. Medizinische Labordiagnostika AG, Lübeck, Germany. Available from: http://www.euroimmun.com/products/techniken/mikrototer-elisa-beschreibung.html. Cited 2018.
Vegasys. Biochemistry analyzer. Available from: www.amsalliance.com/product/vegasys . Cited 2018.
Kyle J, Harris E. Global spread and persistence of dengue. Annu Rev Microbiol. 2008;62:71–92.
World Health Organization. Global Strategy for dengue prevention and control, 2012-2020. France: World Health Orgainzation; 2012. ISBN: 9789241504034
Rajesh D, MdIshaque Q, Raj S. Clinical and laboratory profile in seropositive dengue cases at a tertiary care hospital, South India. WJPPS. 2017;6:1571–81.
Niloy C, Vithyavathi S, Sankar K. Clinical and laboratory profile of different dengue sub types in dengue virus infection. Int J Res Med Sci. 2016;4:743–8.
Badawy A, Sharaf H, AdelMahmoud A. Clinical and Hematological Effects of Dengue Viruses Infection. Am J Infect Dis Microbiol. 2016;4:74–8.
Nadia A, Malik M, Jamil A, Jahangir M, Tirmiz N, Majid A, et al. Cutaneous manifestations in patients of dengue fever. J Pak Assoc Dermatologists. 2012;22:320–4.
Siddiqui F, Haider S, Bhutta Z. Endemic dengue fever: A seldom recognized hazard for Pakistani children. J Infect Dev Ctries. 2009;3:306–12.
Adarsh E, Subramanian V. Clinical profile of dengue infection in a tertiary care hospital. Indian J Child Health. 2015;2:68–71.
Syed R, Musarrat R, Farhat A. Characteristics and outcome of dengue infection; clinical perspective from a secondary care hospital of Karachi. Pak J Med Sci. 2013;29:115–8.
Ahmed S, Ali N, Ashraf S, Ilyas M, Tariq W, Chotani R. Dengue fever outbreak: a clinical management experience. J Coll Physicians Surg Pak. 2008;18:8–12.
Lin C, Lei H, Liu C, Liu H, Yeh T, Wang S. Generation of IgM anti-platelet autoamibody in dengue patients. J Med Virol. 2001;63:143–9.
Jameel T, Mehmood K, Mujaba G, Choudhry N, Afzal N, Paul R. Changing haematological parameters in dengue viral infections. J Ayub Med Coll Abbottabad. 2012;24:3–6.
Kinjal P, Dipanki P, Hematological Parameters DV. ItsUtility in Dengue Fever: A Prospective Study. Int J Sci Res. 2016;5:1077–9.
Mohd Y, Shamim A. Evaluation of clinico-hematological and biochemical changes in dengue fever at CIMSH Lucknow. ijcmr. 2017;4:1527–9.
Mohamed M, Kalavathi G, Mehul R, Karthik M, Asfiya A, Vagesh S, et al. A Study of Clinical and Laboratory Profile of Dengue Fever in Tertiary Care Hospital in Central Karnataka, India. Glob J Med Res. 2014;14:7–12.
Achalkar G. Dengue: a clinic-pathological study of 50 cases. J Evol Med Den Sci. 2013;2:9380–5.
Mariappan T. Current emerging situation of dengue in India. Trop Doct. 2013;43:116–9.
Spoorti V, Yugandhar R, Prabhakar K. Study of clinical and laboratory profile of dengue fever patients. Eur J Pharm Med Res. 2016;3:613–6.
Wahid S, Sanusi S, Zawawi M. A comparison of the pattern of liver involvement in dengue hemorrhagic fever with classic dengue fever. South-east Asian j trop med public health. 2000;31:259–63.
Glassock R. Immune complex-induced glomerular injury in viral diseases: an overview. Kidney Int Suppl. 1991;35:S5–7.
Uday G, Jaya kS, Jnaneshwari M. Study of serum aminotransferase levels in dengue fever. Jemds. 2014;3:2445–55.
Acknowledgments
We would like to acknowledge the University of Gondar and Armauer Hansen Research Institute for financially supporting this study. The role of the Tropical and Infectious Diseases Research Center at the University of Gondar was an immense contribution to the process. We are very grateful to the patients who provided a sample and also physicians, nurses and laboratory technologists of the Metema and Kahsay Abera hospital for their contribution to data collection.
Ethical approval and consent to participate
The study was approved by Ethical Committees of the University of Gondar and Armauer Hansen Research Institute. A written informed consent was obtained from each study participant or assent from a parent/legal guardian of the children.
Funding
This study was funded by the University of Gondar and Armauer Hansen Research Institute. The funders had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
GF: participated in conception and design of the study, data collection, laboratory analysis, data analysis and interpretations of the findings, drafted the manuscript and write up. MT and EA: participated in the conception and design of the study, data analysis and interpretations of the findings. YW: participated in conception and design of the study, data collection, data analysis and interpretations of the findings. EG, RH, AA: participated in conception and design of the study, interpretations of the findings, BT: participated in conception and design of the study, data collection and laboratory analyses, data analysis and interpretations of the findings. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ferede, G., Tiruneh, M., Abate, E. et al. A study of clinical, hematological, and biochemical profiles of patients with dengue viral infections in Northwest Ethiopia: implications for patient management. BMC Infect Dis 18, 616 (2018). https://doi.org/10.1186/s12879-018-3557-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-018-3557-z