
Abstract
Background
Walking is the primary and preferred mode of exercise for older adults. Walking to and from public transit stops may support older adults in achieving exercise goals. This study examined whether density of neighborhood public transit stops was associated with walking for exercise among older adults.
Methods
2018 National Health and Aging Trends Study (NHATS) data were linked with the 2018 National Neighborhood Data Archive, which reported density of public transit stops (stops/mile2) within participants’ neighborhood, defined using census tract boundaries. Walking for exercise in the last month was self-reported. The extent to which self-reported public transit use mediated the relationship between density of neighborhood public transit stops and walking for exercise was examined. Covariates included sociodemographic characteristics, economic status, disability status, and neighborhood attributes. National estimates were calculated using NHATS analytic survey weights.
Results
Among 4,836 respondents with complete data, 39.7% lived in a census tract with at least one neighborhood public transit stop and 8.5% were public transit users. The odds of walking for exercise were 32% higher (OR = 1.32; 95% confidence interval: 1.08, 1.61) among respondents living in a neighborhood with > 10 transit stops per mile compared to living in a neighborhood without any public transit stops documented. Self-reported public transit use mediated 24% of the association between density of neighborhood public transit stops and walking for exercise.
Conclusions
Density of neighborhood public transit stops was associated with walking for exercise, with a substantial portion of the association mediated by self-reported public transit use. Increasing public transit stop availability within neighborhoods may contribute to active aging among older adults.
Similar content being viewed by others


Background
Public transit use is positively associated with physical activity within the general United States population [1,2,3]. Using public transit for everyday commuting facilitates routine-based physical activity. In a single public transit trip, a user will walk to a transit stop, potentially transfer to a connecting route(s), and walk from the final transit stop to an end destination. The first and last legs of a public transit trip make significant contributions to meeting physical activity recommendations [2], with a large proportion (29%) of transit users achieving 30 min of physical activity solely by walking to and from transit stops [1]. Overall, transit users spend a median of 20 min per day walking to and from transit stops, making it a sustainable source of physical activity [3]. Given the benefits of transit use for engagement in physical activity behavior, previous research has investigated if the accessibility of public transit is associated with public transit use and physical activity.
Evidence indicates that the built environment is an important contextual driver of individual public transit use and physical activity within the United States [4, 5]. The built environment comprises the physical environment that is directly created or modified by people [6]. Built environments contribute to the context in which people live and is an effective point for public health investigation given the broad reach of built environment interventions, sustainability of built environment modification, and reduced individual effort needed to shape behaviors over time [7]. Public transportation systems are a component of the built environment, and play a critical role in health and health behaviors of the population [8]. Previous research has found the density of neighborhood public transportation stops to be an important driver of individual public transit use in the United States [9]. Li and colleagues found that living in a neighborhood with high density of public transit stations was associated with more walking for transportation among adults in Portland, Oregon [9]. In addition, people living in areas with high density of public transit stations were more likely to meet physical activity recommendations [9]. However, studies using natural experiments to examine the relationship between the density of public transit stops and physical activity behavior in the United States have found mixed results [10]. Huang et al. found that installing 13 new light rail transit stations in Seattle, Washington resulted in increased transportation physical activity and decreased total physical activity among adults 18 and older [11]. In contrast, Miller et al. found that installing five new light rail transit stations in Salt Lake City, Utah resulted in increased transportation physical activity and total physical activity among adults 18 and older [12]. Additional research is needed to investigate if greater accessibility in public transportation stops is associated with walking behavior. Furthermore, the transferability of findings among the general United States population to older adults in the United States is not well understood.
The United States population is rapidly aging, making older adults an important public transportation user group. Public transportation is a key domain of urban life within the World Health Organizations framework for Global Age-Friendly Cities [13]. The accessibility of public transportation contributes to the process of active aging, defined as a process where opportunities are available for older adults to optimize their health, participation, and security as they age [13]. If public transit stops are available within the neighborhood, then older adults have greater opportunity to walk to public transit stops and maintain independent mobility. Alternatively, if there are no public transit stops within a neighborhood, older adults may have to rely on private transportation options (e.g., driving, family/friends) to maintain independent mobility. 20% of older adults do not drive, and most cease driving due to changes in capacity to drive a car because of age-related functional decline, disability, or both [14, 15]. Older adults with disabilities, who have an increased need for public transportation options, may face greater challenges accessing transit due to physical barriers in availability, accessibility, and delivery of public transportation services [16]. However, if public transportation is available and accessible to meet the needs of older adults with disabilities, it has the potential to enhance active aging.
To date, evidence of the relationship between density of neighborhood public transportation stops and walking behavior has been limited in geographic scope and has yet to investigate this relationship among older adults in the United States. The United States is a unique context to study public transportation impacts on walking behavior among older adults. The United States has long relied on automobiles as a primary form of individual transportation, however, with recent passing of the Infrastructure Investment and Jobs Act there may be a shift in transportation culture. The United States is investing $66 billion in passenger and freight rail and $39 billion in public transportation over the next five years to make public transportation more accessible [17]. Understanding relationships between the public transportation environment and older adults’ health behaviors is needed to inform future public transportation improvements. To date, the proportion of the relationship between neighborhood public transit stop density and physical activity mediated through individual public transit use among older adults has yet to be explored. Identification of relationships between neighborhood public transit density, individual public transit use, and individual walking behavior among older adults would provide foundational evidence to inform future physical activity promotion efforts among older adults through modification of the urban environment. Therefore, the primary aim of this study is to examine the relationship between the density of neighborhood public transportation stops and walking for exercise among older adults. It was hypothesized that greater density of fixed route transit stops within the neighborhood would be associated with greater likelihood to walk for exercise. As a secondary aim, this study investigates if the relationship between density of neighborhood public transit stops and walking for exercise is mediated by individual public transit use.
Methods
Data sources and study sample
This cross-sectional study uses data from the 2018 (round 8) wave of National Health and Aging Trends Study (NHATS). NHATS is a nationally representative sample of Medicare beneficiaries aged 65 and older living in the contiguous United States [18]. A stratified three-stage sampling design was used to construct the sampling frame, with counties or groups of counties as the primary sampling unit, ZIP codes or ZIP code fragments as the secondary sampling unit, and Medicare beneficiaries as the third sampling unit. Oldest age groups and Black non-Hispanic Medicare beneficiaries were oversampled. In 2018, the weighted response rate of participants was 94.0% [19]. Additional details on study design have been previously published [20]. Data collection has occurred on an annual basis since 2011, with detailed information collected through in-home interviews about participants’ health, well-being, and surrounding environments. The majority of NHATS participants responded to interview questions for themselves. However, 12.0% of participants during the 2018 NHATS interview could not respond, and information was collected through proxy report. The current study makes use of NHATS data collected in 2018, representing adults aged 68 and older, to align with the primary exposure data which was captured in 2018. Participants provided written informed consent to be a part of NHATS, and this study was approved by a local Institutional Review Board.
Primary exposure
Density of neighborhood public transit stops within participant’s census tract was obtained from the National Neighborhood Data Archive [21]. The National Neighborhood Data Archive calculates density of neighborhood public transit stops within each census tract in the United States using data from the National Transit Map (NTM). NTM compiles General Transit Feed Specification data provided by 270 regional transit authorities in the United States and is continually updated by participating agencies [22]. The 270 participating regional transit authorities represented in the NTM dataset includes static information on locations where fixed-guideway and fixed-route pick up and drop off riders (i.e., transit stops). Stops within the NTM dataset include various modes of public transport (e.g., bus, subway, rail) available. Number of neighborhood transit stops in 2018 were captured and aggregated by researchers in April 2019 [21]. Density of neighborhood transit stops were calculated per square mile within 2010 census tract boundaries. Density of neighborhood transit stops was categorized into three groups: no transit stops documented, at least one transit stop and less than 10 transit stops per square mile, and greater than 10 transit stops per square mile.
Primary outcome
Walking for exercise was measured during the annual interview using self-report by asking participants whether they ever walked for exercise in the last month. A binary response of ‘Yes’ or ‘No’ was recorded.
Mediator
Individual public transit use was self-reported by participants during the annual interview. Participants were asked “In the last month, how did you get to places outside your home? Did you take public transportation (the bus, subway, or train)?” Participants provided a binary response of ‘Yes’ or ‘No’.
Covariates
Several variables associated with physical activity [23] and access to transit [24,25,26] were included as confounders within our analysis. According to travel behavior theory, the major determinants of travel patterns are social class position, ethnicity, life cycle status, and residential location [27]. Therefore, potential confounding variables included sociodemographic characteristics (i.e., age, gender, race/ethnicity, marital status, number of people in social network), economic status (i.e., education, home ownership), disability status, and neighborhood attributes (i.e., geographic residence, duration of residence, neighborhood physical disorder, and social cohesion). Age was categorized into 5-year age brackets representing participants aged 68–69, 70–74, 75–79, 80–84, 85–89, and 90 or greater. Gender was self-reported as a binary variable for males and females. Race and ethnicity were self-reported and categorized into four groups including non-Hispanic White, non-Hispanic Black, non-Hispanic other, and Hispanic. Marital status was self-reported by participants and categorized into six groups representing married, living with a partner, separated, divorced, widowed, and never married. Number of people in social network was calculated from responses to a request to name the people the older adult talked with most often in the last year about important things. Up to five social network members could be named.
For economic status, participants were asked what the highest degree or level of school they completed. Education was then categorized into three groups representing less than high school, high school graduate, or more than high school. Homeownership, a measure of wealth, was self-reported during the interview and categorized as ‘Yes’ (i.e., own their home) or ‘No’ (i.e., rent their home, some other arrangement to live in their home).
Disability was captured via self-report and includes six indicator variables reflecting standard disability domains [28]: (1) visual impairment included reported blindness, difficulty seeing across the street even while wearing glasses, or difficulty reading newspaper print while wearing glasses [18]; (2) hearing impairment included reported deafness, use of a hearing aid or other hearing device, difficulty carrying a conversation with background noise, or inability to hear well enough to use a telephone [18]; (3) cognitive impairment included proxy or self-report rating that their memory was fair, or poor [18]; (4) mobility impairment included reported inability to walk 3 blocks or up 10 stairs [18, 29]; (5) self-care impairment included difficulty by oneself or never doing by oneself the following activities: eating, bathing, toileting, or dressing [18, 30]; and (6) communication impairment included reported difficulty speaking or making themselves understood while talking.
Four neighborhood attributes were treated as covariates within this study: (1) geographic residence was categorized as metropolitan or non-metropolitan county derived from Rural-Urban Continuum Codes [31, 32]; (2) duration of residence was categorized as living in their current location of less than five years or five year or more; (3) Neighborhood physical disorder was recorded by NHATS interviewers, where they recorded the extent of physical disorder (e.g., litter, graffiti, vacant houses, and continuous sidewalks) surrounding the participant’s home on a four-point scale and reduced to a binary variable representing any neighborhood physical disorder or no neighborhood physical disorder; and (4) NHATS respondents self-reported their perception of community (i.e., how well people know each other, if people are willing to help each other, and if people in the community can be trusted) on a three-point scale [33, 34] and social cohesion was categorized into tertiles.
Analytic strategy
This study focused on older adults living in the community or residential care settings other than nursing homes in 2018 to examine the association between density of neighborhood public transportation stops and walking for exercise. National estimates of density of neighborhood public transportation stops, disability status, and walking for exercise were obtained using analytic survey weights. The NHATS analytic survey weight accounts for differential selection probabilities and adjusts for nonresponse bias [20]. Our analysis was restricted to participants living in the community or residential care settings other than nursing homes who had non-missing data. Using the survey command suite within STATA, logistic regression was performed to assess associations between density of public transportation stops and walking for exercise. Using a sequential model building strategy, associations between density of public transit stops and odds of walking for exercise in the last month were assessed. Unadjusted estimates are evaluated in Model 1, Model 2 adjusts for demographic characteritiscs, Model 3 additionally adjusts for economic characteristics, Model 4 additionally adjusts for disability status, and Model 5 adjusts for all theorized covariates.
The extent to which individual public transit use mediated the association between density of neighborhood public transit stops and walking for exercise was assessed using the STATA medeff package for causal mediation analysis [35,36,37]. This study hypothesized that the relationship between density of neighborhood public transit stops and walking for exercise would be mediated through individual public transit use. However, there may be other mechanisms through which density of neighborhood public transit stops influence walking for exercise among older adults. For example, density of neighborhood public transit stops is correlated with other features of the neighborhood context known to be assoicated with physical activity, such as median household income [38] and land use [39]. Figure 1 displays the hypothesized causal mechanism through individual public transit use. The mediator was modeled with a logistic regression, using the same sequential model building strategy as described above. The outcome model was a logistic regression including the mediator and sequential model building strategy as described above. Average causal mediation effect was computed by taking the difference between the estimated total effect (Fig. 1, path C) and the average direct effect (Fig. 1, path c’). All analyses were conducted using STATA 16.1.

Hypothesized direct and indirect pathways linking density of public transit stops to walking for exercise through public transit use among National Health and Aging Trends Study respondents living in the community or residential care settings other than nursing homes, United States, 2018
Results
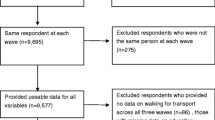
The 2018 round of NHATS collected data on 5,547 respondents. Respondents were excluded from the current study if they had died (n = 397), lived in a nursing home at the time of the interview (n = 232), were not administered an interview (n = 81), or had missing item-level information (n = 1). A total of 711 were excluded, resulting in a final analytic sample of 4,836.
As shown in Table 1, most participants (60.3%) lived in a neighborhood with no documented public transportation stops available, followed by 23.2% living in a neighborhood with more than 10 public transit stops per square mile and 16.5% living in a neighborhood with 0–10 public transit stops per square mile. Many participants reported walking for exercise in the last month (62.3%) and few participants used public transit (8.5%). Compared to the total study sample, a greater proportion of participants living within neighborhoods with high density of public transit stops self-identified as Black non-Hispanic (16.2% vs. 7.9%), Hispanic (11.1% vs. 7.4%), and separated/divorced (20.8% vs. 14.1%). In addition, a greater proportion of neighborhoods with high density of public transit stops had observed physical disorder (11.5% vs. 7.8%) and low levels of social cohesion (16.8% vs. 13.0%) compared to the total study sample. The proportion of participants who reported individual public transit use was differential by density of neighborhood public transit stops, ranging from 4.8% of participants using public transit among those living in a neighborhood with 0–10 public transit stops per square mile to 19.5% of participants using public transit among those living in a neighborhood with greater than 10 public transit stops per square mile. Additional details on descriptive statistics of individual and environmental characteristics can be found in Table 1.
Table 2 presents the sequentially adjusted odds ratios (OR) and 95% confidence intervals (CI) for walking for exercise. Within the unadjusted model (model 1) the odds of walking for exercise among participants living in a neighborhood with 0–10 transit stops per square mile was 1.32 (95% CI: 1.07, 1.63) times the odds of walking for exercise among participants living in a neighborhood with no transit stops. Similar effect estimates were observed among participants living in a neighborhood with more than 10 transit stops per square mile (OR = 1.36; 95% CI: 1.10, 1.67). Associations were attenuated after adjustment for demographic, economic, impairment, and neighborhood characteristics. Within the fully adjusted model, the odds of walking for exercise did not significantly differ between participants living in a neighborhood with 0–10 transit stops per square mile compared to participants living in a neighborhood with no transit stops (OR = 1.20; 95% CI: 0.96, 1.49). Odds of walking for exercise among participants living in a neighborhood with more than 10 transit stops per square mile was 1.32 (95% CI: 1.08, 1.61) times the odds of walking for exercise among participants living in a neighborhood with no transit stops. In addition to the density of public transit stops in the neighborhood, several sociodemographic variables significantly contributed to the likelihood of walking for exercise. Participants who self-identified as Hispanic (OR = 1.61) or Other (OR = 1.66) race and ethnicity compared to non-Hispanic White and greater educational attainment (OR = 1.23) had significantly higher odds of walking for exercise. One additional person within a participant’s social network was associated with 15% higher odds (OR = 1.15; 95% CI: 1.09, 1.22) of walking for exercise. Lastly, mobility impairment (OR = 0.27), longer residential duration (OR = 0.68), and lower social cohesion (OR = 0.73 & OR = 0.65) were all significantly associated with lower likelihood of walking for exercise.
Table 3 presents our sequentially adjusted mediation analysis. Within unadjusted models, individual public transit use mediated 46.6% of the association between density of neighborhood public transit stops and walking for exercise. After adjustment for all covariates the proportion of association mediated by individual public transit use decreased to 23.5%.
Discussion
In a nationally representative cohort study of older adults, this study found that living in an area with a high density of neighborhood public transit stops (i.e., more than 10 transit stops per square mile) was associated with greater odds of walking for exercise. The observed relationship was significant after accounting for sociodemographic characteristics, economic status, disability status, and neighborhood characteristics. Findings suggest that living in a neighborhood with better access to public transit service might shape individual public transit use and facilitate walking behavior. On a population health level, these findings have significant public health implications that point towards public transportation systems and urban development strategies as potential approaches to promote physical activity among older adults. Public transportation agencies can increase the number of stops within residential area to make transit more accessible to older adults.
Additionally, this study explored the extent to which individual public transit use mediates the association between density of neighborhood public transit stops and walking for exercise. This study found that individual public transit use mediated 24% of the relationship between density of neighborhood public transit stops and walking for exercise, indicating that greater availability of public transit stops within neighborhoods (i.e., density of public transit stops) is associated with higher individual public transit use and higher individual public transit use is associated with walking for exercise. Walking for exercise is an important health goal for older adults that is associated with reductions in mortality, cardiovascular disease, type 2 diabetes, musculoskeletal disorders, cancer, and obesity [40]. Furthermore, physical activity has important benefits to older adults’ quality of life through improvements in sleep, cognitive function, and mental health [40]. The remaining 76% of the relationship was not mediated through individual public transit use, suggesting there are other mechanisms through which density of neighborhood public transit stops is associated with walking for exercise among older adults. One potential theory is that areas with greater density of public transit stops may have other features of the built environment, such as diversity of land use, intersection density, and number of destinations, which have been shown to be strongly related to walking behavior [41]. For example, areas with greater density of public transit stops could also have greater access to retail establishments (e.g., grocery stores, shopping malls) or destinations for social engagement (e.g., coffee shops, places of worship) to which older adults may be motivated to walk [41]. Additional research is needed to investigate features of the built environment and behavioral components that either facilitate or hinder public transit access and walking for exercise among older adults.
The findings from the current study align with previous work investigating the association between public transit use and physical activity behavior in the general population [42,43,44]. Among a group of adults in King County, Washington, public transit use was associated with greater physical activity and walking behavior compared to no public transit use [42]. Furthermore, this relationship was greatest in magnitude among the most frequent transit users [42]. Similarly, public transit use was associated with greater physical activity behavior in Atlanta [43], New York City [44], and across North America [1]. Within the English Longitudinal Study of Ageing, research has demonstrated that access to a bus pass among older adults makes transportation more accessible and thereby associated with greater physical activity within this population subgroup [45, 46]. The current study adds to this body of literature by estimating relationships among a nationally representative sample of United States older adults, while accounting for disability status. This study found that density of neighborhood public transit stops in a census tract and individual public transit use were associated with walking for exercise among older adults, above and beyond disability. Taken together, our findings suggest that increasing density of public transit stops, and thereby facilitating greater individual public transit use, is one strategy to improve physical activity participation among older adults. Using catalytic forecasting to quantify public transit demand based on population demographics, including the composition of older adults within a community, is a promising strategy to improve access and equity in public transportation [47]. Older adults should be a priority population for public transit equity given the physical activity promotion benefits of public transit use and large proportion of non-driving older adults in the United States [48, 49].
Beyond facilitating improvements in walking for exercise among older adults, improving public transit infrastructure and facilitating access to transit has additional benefits for older adults [50, 51]. Older adults are at greater risk of transportation disadvantage compared to younger adults [52], and transportation is a common concern to accessing health care among older adults. Over 16% of older adults report transportation barriers to healthcare, and have missed care because of a problems with transportation in the United States [53]. Improving the density and accessibility of neighborhood public transit may mitigate the risks of transportation disadvantage among older adults and could provide greater access to the health care system. However, modifying and adapting the built environment to meet the needs of older adults will take time. Therefore, while addressing the physical barriers to public transit access there are other interventions (e.g., fare vouchers, travel training programs) that can be put into place to expand access and use of public transit among older adults. Public transit offers older adults’ greater autonomy, independence, and quality of life. Reduced or restricted transportation access has been associated with social isolation, depression, and mortality among older adults [54, 55]. As demonstrated by the results of the mediation analysis, individual public transit use promotes walking for exercise, making public transit use a key component of active aging.
This study has several strengths. We draw upon a novel national database objectively identifying neighborhood public transportation stops. The point locations of public transit stops were aggregated to the census tract level and linked with NHATS participants’ home addresses. In addition, this study adds to the current body of evidence by demonstrating the role that density of neighborhood public transportation stops has on walking for exercise among older adults. This is the first study to our knowledge that has examined the association between density of public transportation stops and walking for exercise among a geographically diverse, nationally representative sample of older adults. In addition, this study integrates rich detail on disability status, neighborhood physical disorder, and neighborhood social cohesion within our models providing robust effect estimates of the relationship between density of public transit use and walking for exercise. Furthermore, using a nationally representative sample of older adults brings greater external validity to the observed associations within this study.
However, this study is not without limitations. The study findings are limited in external validity. These results are generalizable to adults 68 years or older living in the community or residential care settings other than nursing homes. Additionally, due to voluntary participation in NTM, a value of 0 may indicate either an absence of transit stops within a census tract, or the non-participation of a regional transit authority in NTM [21]. Since values of 0 have different meanings, this introduces information bias. Specifically, differential misclassification of our primary exposure can bias our effect estimates. We expect that misclassification of census tracts to a value of 0 due to non-participation of regional transit authorities in the NTM would bias estimates towards the null. This means that the effect estimates potentially underestimate the true association between public transit stop density on walking for exercise among older adults. Although NTM participation was voluntary, it includes data from over 270 transit agencies, providing information on over 398,000 stops and stations along 10,000 routes within the United States [22]. Furthermore, our research is limited by the quantity of neighborhood public transit stops and were unable to collect information about the quality of neighborhood public transportation stops (e.g., shelter, bench, lighting), which may serve as a major facilitator for older adults’ use of the public transit system. Participants also self-reported if they walked for exercise in the last month, a crude estimate for physical activity participation [56]. The binary measurement of metro area used in this research does not fully capture the heterogeneity in the rural-urban continuum. Previous research has shown that the relationship between environmental features and physical activity varies by urbanicity [57]. Additional research is needed to investigate effect measure modification by urbanicity with great representation of the heterogeneity among non-urban participants. There is the potential that unmeasured confounders, such as climate and weather, may be present and distort the true underlying relationship between transit stop density and walking for exercise among older adults. Lastly, there are many components of the travel chain that were not captured within this project, including the walkability of the neighborhood environment (e.g., residential density, street connectivity, and land use mix). Previous research has shown that neighborhood walkability is associated with greater likelihood of individual transit use, and future research should take these attributes into consideration [58].
Conclusions
Within a nationally representative sample of older adults within the United States, this study found that the density of neighborhood public transit stops was associated with walking for exercise in the last month. A substantial portion of this association (24%) mediated through self-reported individual public transit use. Increasing the availability of public transit within neighborhood environments may contribute to active aging among older adults and facilitate aging in place within the United States. Therefore, increasing the density and availability of public transit stops may be a modifiable intervention target to promote public transit use and walking for exercise among older adults.
Data Availability
The datasets generated and/or analyzed during the current study are available in the NHATS and NaNDA repositories, www.nhats.org and https://nanda.isr.umich.edu/data/.
Abbreviations
- NHATS:
-
National Health and Aging Trends Study
- NTM:
-
National Transit Map
References
Besser LM, Dannenberg AL. Walking to public transit: steps to help meet physical activity recommendations. Am J Prev Med. 2005;29(4):273–80.
Freeland AL, Banerjee SN, Dannenberg AL, Wendel AM. Walking associated with public transit: moving toward increased physical activity in the United States. Am J Public Health. 2013;103(3):536–42.
Le VT, Dannenberg AL. Moving toward physical activity targets by walking to transit: National Household Transportation Survey, 2001–2017. Am J Prev Med. 2020;59(3):e115–e23.
Travert A-S, Sidney Annerstedt K, Daivadanam M. Built environment and health behaviors: deconstructing the black box of interactions—a review of reviews. Int J Environ Res Public Health. 2019;16(8):1454.
Sallis JF, Floyd MF, Rodríguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation. 2012;125(5):729–37.
Srinivasan S, O’fallon LR, Dearry A. Creating healthy communities, healthy homes, healthy people: initiating a research agenda on the built environment and public health. Am J Public Health. 2003;93(9):1446–50.
Frieden TR. A framework for public health action: the health impact pyramid. Am J Public Health. 2010;100(4):590–5.
Brownson RC, Hoehner CM, Day K, Forsyth A, Sallis JF. Measuring the built environment for physical activity: state of the science. Am J Prev Med. 2009;36(4):99–S123. e12.
Li F, Harmer PA, Cardinal BJ, Bosworth M, Acock A, Johnson-Shelton D, et al. Built environment, adiposity, and physical activity in adults aged 50–75. Am J Prev Med. 2008;35(1):38–46.
Hirsch JA, DeVries DN, Brauer M, Frank LD, Winters M. Impact of new rapid transit on physical activity: a meta-analysis. Prev Med Rep. 2018;10:184–90.
Huang R, Moudon AV, Zhou C, Stewart OT, Saelens BE. Light rail leads to more walking around station areas. J Transp Health. 2017;6:201–8.
Miller HJ, Tribby CP, Brown BB, Smith KR, Werner CM, Wolf J, et al. Public transit generates new physical activity: evidence from individual GPS and accelerometer data before and after light rail construction in a neighborhood of Salt Lake City, Utah, USA. Health Place. 2015;36:8–17.
World Health Organization. Global age-friendly cities: a guide. France: WHO Press; 2007.
Bailey L. Surface Transportation Policy Project. Washington, DC; 2004. Report No.: 1.
MacLeod KE, Satariano WA, Ragland DR. The impact of health problems on driving status among older adults. J Transp Health. 2014;1(2):86–94.
Remillard ET, Campbell ML, Koon LM, Rogers WA. Transportation challenges for persons aging with mobility disability: qualitative insights and policy implications. Disabil Health J. 2022;15(1):101209.
Bipartisan Infrastructure Law Washington, DC: U.S. Department of Transportation Federal Highway Administration. ; 2022 [Available from: https://www.fhwa.dot.gov/bipartisan-infrastructure-law/.
Freedman VA, Kasper JD. National Health and Aging Trends Study user guide: rounds 1–10 final release. Baltimore, MD: Johns Hopkins University School of Public Health; 2021.
DeMatteis JM, Freedman VA, Kasper JD. National Health and Aging Trends Study Development of Round 8 Survey weights. Baltimore, MD: Johns Hopkins University School of Public Health; 2019.
Montaquila J, Freedman VA, Edwards B, Kasper JD. National Health and Aging Trends Study round 1 sample design and selection. NHATS Tech Paper. 2012;1:1–8.
Clarke PJ, Melendez R. National Neighborhood Data Archive (NaNDA): Public Transit Stops by Census Tract, United States, 2016–2018. Ann Arbor, MI: Inter-university Consortium for Political and Social Research 2019.
Bureau of Transportation Statistics. The National Transit Map: United States Department of Transportation. ; 2021 [Available from: https://www.bts.gov/national-transit-map/about.
Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–e639.
McKenzie BS. Neighborhood access to transit by race, ethnicity, and poverty in Portland. OR City & Community. 2013;12(2):134–55.
Kahn ME. Gentrification trends in new transit-oriented communities: evidence from 14 cities that expanded and built rail transit systems. Real Estate Econ. 2007;35(2):155–82.
Golub A, Marcantonio RA, Sanchez TW. Race, space, and struggles for mobility: transportation impacts on African Americans in Oakland and the East Bay. Urban Geogr. 2013;34(5):699–728.
Fried M, Havens J, Thall M. Travel behavior-a synthesized theory. 1977.
Madans JH, Loeb ME, Altman BM, editors. Measuring disability and monitoring the UN Convention on the Rights of Persons with Disabilities: the work of the Washington Group on Disability Statistics. BMC Public Health; 2011: Springer.
Freedman VA, Kasper JD, Cornman JC, Agree EM, Bandeen-Roche K, Mor V, et al. Validation of new measures of disability and functioning in the National Health and Aging Trends Study. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences. 2011;66(9):1013–21.
Allen SM, Mor V. The prevalence and consequences of unmet need: contrasts between older and younger adults with disability. Med Care. 1997:1132–48.
Butler MA, Beale CL. Rural-urban continuum codes for metro and nonmetro counties, 1993. 1994.
Economic Research Service. Rural–Urban Continuum Codes: US Department of Agriculture; [Available from: https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/.
Cagney KA, Glass TA, Skarupski KA, Barnes LL, Schwartz BS, Mendes de Leon CF. Neighborhood-level cohesion and disorder: measurement and validation in two older adult urban populations. Journals of Gerontology: Series B. 2009;64(3):415–24.
Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: a multilevel study of collective efficacy. Science. 1997;277(5328):918–24.
Hicks R, Tingley D. Causal mediation analysis. Stata J. 2011;11(4):605–19.
Imai K, Keele L, Tingley D. A general approach to causal mediation analysis. Psychol Methods. 2010;15(4):309.
Imai K, Keele L, Yamamoto T. Identification, inference and sensitivity analysis for causal mediation effects. 2010.
Barton MS, Gibbons J. A stop too far: how does public transportation concentration influence neighbourhood median household income? Urban Stud. 2017;54(2):538–54.
Center for Transit Oriented Development. Trends in transit-oriented Development 2000–2010. Washington, DC: Federal Tranist Administration; 2014.
Koster A, Stenholm S, Schrack JA. The benefits of physical activity for older people. The Palgrave Handbook of Ageing and Physical Activity Promotion. Springer; 2018. pp. 43–60.
Ewing R, Cervero R. Travel and the built environment: a meta-analysis. J Am Plann Association. 2010;76(3):265–94.
Saelens BE, Vernez Moudon A, Kang B, Hurvitz PM, Zhou C. Relation between higher physical activity and public transit use. Am J Public Health. 2014;104(5):854–9.
Lachapelle U, Frank LD. Transit and health: mode of transport, employer-sponsored public transit pass programs, and physical activity. J Public Health Policy. 2009;30(1):73–S94.
Wener RE, Evans GW. A morning stroll: levels of physical activity in car and mass transit commuting. Environ Behav. 2007;39(1):62–74.
Webb E, Laverty A, Mindell J, Millett C. Free bus travel and physical activity, gait speed, and adiposity in the English longitudinal study of ageing. Am J Public Health. 2016;106(1):136–42.
Laverty AA, Webb E, Vamos EP, Millett C. Associations of increases in public transport use with physical activity and adiposity in older adults. Int J Behav Nutr Phys Activity. 2018;15(1):1–10.
Allen DJ. Lost in the transit desert: race, transit access, and suburban form. Routledge; 2017.
Adminstration FH. Distribution of licensed drivers–2018 by sex and percentage in each age group and relation to population. 2020.
Foley DJ, Heimovitz HK, Guralnik JM, Brock DB. Driving life expectancy of persons aged 70 years and older in the United States. Am J Public Health. 2002;92(8):1284–9.
Dickerson AE, Molnar LJ, Bédard M, Eby DW, Berg-Weger M, Choi M, et al. Transportation and aging: an updated research agenda to advance safe mobility among older adults transitioning from driving to non-driving. Gerontologist. 2019;59(2):215–21.
Kerschner HK, Silverstein NM. Introduction to senior transportation: enhancing community mobility and transportation services. Routledge; 2018.
Ryvicker M, Bollens-Lund E, Ornstein KA. Driving status and transportation disadvantage among Medicare beneficiaries. J Appl Gerontol. 2020;39(9):935–43.
Wallace R, Hughes-Cromwick P, Mull H, Khasnabis S. Access to health care and nonemergency medical transportation: two missing links. Transp Res Rec. 2005;1924(1):76–84.
Chihuri S, Mielenz TJ, DiMaggio CJ, Betz ME, DiGuiseppi C, Jones VC, et al. Driving cessation and health outcomes in older adults. J Am Geriatr Soc. 2016;64(2):332–41.
Ratnapradipa KL, Wang J, Berg-Weger M, Schootman. Mario. Effects of older adult driving resumption on all-cause mortality. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2020;75(10):2263–7.
Schrack JA, Cooper R, Koster A, Shiroma EJ, Murabito JM, Rejeski WJ, et al. Assessing daily physical activity in older adults: unraveling the complexity of monitors, measures, and methods. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences. 2016;71(8):1039–48.
Abildso CG, Daily SM, Meyer MRU, Edwards MB, Jacobs L, McClendon M, et al. Environmental factors associated with physical activity in rural US counties. Int J Environ Res Public Health. 2021;18(14):7688.
Kwon K, Akar G. People with disabilities and use of public transit: the role of neighborhood walkability. J Transp Geogr. 2022;100:103319.
Acknowledgements
Not applicable.
Funding
Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers T32AG000247, K99AG081563, and U01AG032947. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
ET contributed significantly to the conception of this work, analyzed and interpreted the data, and played a major role in writing the manuscript. JF made substantial contributions to the conception and design of the study. PC, VF, and JS made significant contributions to the conception, design, and acquisition of data. JS was also a major contributor in writing the manuscript. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Existing data were collected using an informed consent document. IRB approval for NHATS individual and geographic data is held by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB#2083).
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Twardzik, E., Falvey, J.R., Clarke, P.J. et al. Public transit stop density is associated with walking for exercise among a national sample of older adults. BMC Geriatr 23, 596 (2023). https://doi.org/10.1186/s12877-023-04253-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04253-x