
Abstract
Background
Attention is focused on the health and physical fitness of older adults due to their increasing age. Maintaining physical abilities, including safe walking and movement, significantly contributes to the perception of health in old age. One of the early signs of declining fitness in older adults is limited mobility. Approximately one third of 70-year-olds and most 80-year-olds report restrictions on mobility in their apartments and immediate surroundings. Restriction or loss of mobility is a complex multifactorial process, which makes older adults prone to falls, injuries, and hospitalizations and worsens their quality of life while increasing overall mortality.
Objective
The objective of the study is to identify the factors that have had a significant impact on mobility in recent years and currently, and to identify gaps in our understanding of these factors. The study aims to highlight areas where further research is needed and where new and effective solutions are required.
Methods
The PRISMA methodology was used to conduct a scoping review in the Scopus and Web of Science databases. Papers published from 2007 to 2021 were searched in November 2021. Of these, 52 papers were selected from the initial 788 outputs for the final analysis.
Results
The final selected papers were analyzed, and the key determinants were found to be environmental, physical, cognitive, and psychosocial, which confirms the findings of previous studies. One new determinant is technological. New and effective solutions lie in understanding the interactions between different determinants of mobility, addressing environmental factors, and exploring opportunities in the context of emerging technologies, such as the integration of smart home technologies, design of accessible and age-friendly public spaces, development of policies and regulations, and exploration of innovative financing models to support the integration of assistive technologies into the lives of seniors.
Conclusion
For an effective and comprehensive solution to support senior mobility, the determinants cannot be solved separately. Physical, cognitive, psychosocial, and technological determinants can often be perceived as the cause/motivation for mobility. Further research on these determinants can help to arrive at solutions for environmental determinants, which, in turn, will help improve mobility. Future studies should investigate financial aspects, especially since many technological solutions are expensive and not commonly available, which limits their use.
Similar content being viewed by others

Introduction
The ageing population is an important phenomenon faced by many countries in this century. While ageing is a triumph of development, the phenomenon and its impact on the society need to be managed [1]. Mobility is crucial for active ageing as it allows older adults to maintain their independence, participate in physical activities, engage in social and community life, and access necessary resources [2]. The ability to move around freely, safely, and independently is essential for promoting physical and mental well-being, preventing falls and injuries, and reducing the risk of disability and institutionalization [3]. Addressing mobility challenges for older adults involves a multidisciplinary approach involving healthcare providers, policymakers, urban planners, and families.
Access to transportation is one of the key social determinants of health for older adults, and the lack of access is associated with negative health outcomes, including social isolation, depression, and early entry into long-term care facilities. The National Institute on Aging [2] conducted a study on the mobility of elderly Americans that emphasized the significance of accessibility in preserving the autonomy and well-being of seniors. The study suggested enhancing the accessibility of transportation systems and infrastructure to facilitate the mobility of senior citizens. The age-friendly cities framework [4] is a global initiative aimed at making cities more accessible and accommodating for older adults. It focuses on eight domains, including transportation, housing, and social participation. The universal design framework focuses on designing buildings [5], products, and environments that are accessible to people of all ages, abilities, and disabilities. The European Union has established the European Accessibility Act [6], which requires that products and services in key areas, including transportation, are accessible to people with disabilities, including seniors. The Act provides guidelines for improving accessibility in transportation systems and infrastructure to support the mobility of seniors. Accessibility and solutions to increase accessibility are directly or indirectly linked to the space where a senior needs to be mobile.
The concept of life-space mobility (LSM) assesses functional, environmental, and social factors that affect how people live their everyday lives [7]. Johnson et al. [7] showed that that socio-demographic variables such older age, female gender, and lower level of education, fear of falling, limitations in activities of daily living (ADLs) and instrumental activities of daily living (IADLs), poor performance in gait speed and muscle strength, and transportation difficulties were associated with lower LSM. Life-space mobility has been found to be a predictor of cognitive decline, hospital readmission, quality of life, and admission to a nursing home. Life-space mobility allows the initiation, adaptation, or evaluation of intervention strategies [7]. Findings from such research continue to be used by many organizations to establish better conditions. The World Health Organization’s Global Age-Friendly Cities Guide [4] provides recommendations on how to design inclusive living spaces for seniors and supports the development of age-friendly communities. The European Innovation Partnership on Active and Healthy Aging has created the Covenant on Demographic Change, which encourages local and regional governments to develop strategies for creating age-friendly environments and living spaces.
Recent technological developments are intertwined with the aforementioned strategies, programs, and actions. They are an important aspect in the search for new solutions. Porter et al. [8] describe emerging technologies as those that could exert much-enhanced economic influence in the coming several years’ time horizon. Cozzens et al. [9] showed four characteristics: fast recent growth; in the process of transition and/or change; market or economic potential that is not exploited fully yet; increasingly science-based. Finally, Smalheiser et al. state that emerging technology can be incremental, originating from its potential to change an existing industry, in addition to being radical, originating from the potential to create a new industry [10].
To sustainably improve the conditions and quality of life of seniors, it is essential to regularly identify opportunities and monitor the development and usefulness of new solutions in mobility.
The objective of the study is to identify the determinants that have had a significant impact on mobility in recent years and currently, and to identify gaps in our understanding of these factors. The study aims to highlight areas where further research is needed and where new and effective solutions are required.
As part of scoping review, the PRISMA guidelines [11] and bibliometric mapping study method [12] were used to provide a systematic and holistic review of the determinants of older adults’ mobility. Bibliometric mapping provides an overview of the state-of-the-art of scientific knowledge on a given topic. The bibliometric analysis embraces the performance analysis of contributions on specific topics, and we are using a method of scientific mapping to analyse the evolution of specific research subjects [13] in order to identify subject fields and show their progress by employing different visualization tools in research planning.
Theoretical background
The above-mentioned studies and strategies demonstrate the importance of addressing the aspects of accessibility, living space, and technology in the context of mobility for seniors. The authors perceive the aspects of accessibility, life-space mobility, and developing technologies as intertwined, yet each of them individually significant. Accessibility, which is relevant for the given scope, is also related to the zones of the living space. Accessibility is considered to be one of the most important predictors of quality of life (QoL) for older adults [14]. The search for new solutions for the elderly is very often connected with technologies, as stated by many strategies and acts [15]. Therefore, attention will also be paid to this area within the scoping review, focusing on aspects accessibility, LSM, and technologies, to determine their objective importance in recent years. Overall, the below-described brief state of the art in the context of mobility in LSM, related accessibility, and ubiquitous technologies, shows how the field is perceived in the context of this paper.
Mobility and zones of living space
Zones of living space for the elderly are designed to meet their specific needs and support their mobility. These zones typically include residential areas that are designed to be accessible, with wide sidewalks, low curbs, and other features that make it easier for older adults to get around. In addition, these zones may also include essential services such as healthcare facilities, grocery stores, and public transportation that are easily accessible to older adults. The idea behind designing zones of living space for the elderly is to create an environment that supports their mobility, promotes their independence, and enhances their quality of life [16]. Webber et al. [16] introduced a model defining seven zones of living space for older adults: room, dwelling space, close neighbourhood, vicinity, service community, surrounding area, and the world. The cognitive, emotional, physical, environmental, and economic elements that determine mobility vary among zones and are heavily influenced by gender, culture, and individual biography. Similarly, Burlano and Cusano specify four types of neighbourhoods according to local accessibility and possibilities of travel to distant places [1]. Different zones are associated with different types of spatial mobility. Many authors emphasize the benefits of physical movement in maintaining physical and mental health and the positive impact of soft mobility (cycling, walking, etc.) in alleviating diseases. Cao et al. confirm that engaging in outside activities can improve older adults’ well-being. Mobility declines with age mainly due to health constraints and changes in activity patterns [17], which increase the risk of sedentarism and hypomobility. Spatial mobility is not only intended to fulfil physiological needs but is also an important part of social cohesion [18], social participation [19], and the basic condition required to maintain older adults’ independence and self-reliance [20]. Many studies [21,22,23,24] recommend engaging in out-of-home travel regularly to interact with friends and the broader community to reduce social isolation.
Accessibility
Accessibility studies reflect spatial mobility opportunities and conditions. Geurs [25] defined accessibility as “the extent to which the land-use transport system enables (groups of) individuals or goods to reach activities or destinations by means of a (combination of) transport mode(s)”. It is evaluated using different measures. Geurs specified the following four basic types of measures: infrastructure-, location-, person-, and utility-based.
Location-based measures focus on potential and connectivity, but they typically do not take into account individuals’ behaviour, capacity restrictions, return routes, chaining of destinations, or temporal variability. Accessibility is measured from the perspective of an individual’s capacity to make use of resources within the context of their normal routine and time restrictions [26]. Such measures may well address the richness of older adults’ lives, but they rely heavily on data input [27]. Accessibility includes the evaluation of
-
1.
the availability of destinations and required activities,
-
2.
physical access and walkability, and
-
3.
functionality of transport systems, including affordability and acceptability (safety, information support, etc.) [28].
All these components are highly influenced by personal factors. The qualitative assessment of accessibility (modelled accessibility) significantly differs from perceived accessibility evaluated by personal survey tools.
Accessibility indexes and mode choice studies are receiving more attention from researchers. “Aging in place” refers to the desire of the elderly to remain in the homes and communities they have been in for the longest possible period of time after retiring [21]. It is not unusual for individuals to choose the same neighbourhood where they have spent most of their adult years as a retirement location, especially in suburban settings.
Mobility opportunities in relation to emerging technologies
Elsy [29] has observed that technologies are developing towards an environment where humans, robots, or artificial intelligence (AI) coexist and work together to improve the quality of life by offering specialised services for the needs of diverse users. This enables an increased level of autonomy by proactively collecting data from the environment, making decisions, and providing services for humans. Older adults’ healthcare solutions include (1) connecting and sharing information in the network between users of medical data, including medical check-up records and treatment and care records; (2) providing remote medical care services; (3) and using AI and robots in the care facilities to support community independence.
However, existing new mobility options have left a large population of harder-to-serve older adults out of the new mobility revolution, so that they are unable to access its benefits. Those with more limitations (physical, cognitive, multiple disabilities, financial, technology access/understanding) or certain specific needs (transportation that accommodates mobility aids, low-income, rural location) often face barriers:
-
1.
Using emerging transportation technologies requires smartphone and internet access, as well as the ability to make online payments, which can be challenging for many older adults who may lack even a basic level of tech fluency and comfort.
-
2.
The vehicles can be difficult to enter and exit and may not easily accommodate walking aids or wheelchairs, which are used by approximately a quarter of all older adults.
-
3.
Current ride-hailing and projected autonomous vehicle (AV) services primarily focus on curb-to-curb service, while many older adults need door-to-door or hand-to-hand service due to challenges such as identifying the vehicle when it arrives; stowing and retrieving bags or mobility aids; finding the correct door at complex locations such as hospitals or shopping centres; and physically navigating busy streets and sidewalks [30].
This systematic review will examine and identify mobility limitations in the context of technology development, highlighting opportunities for further development.
Method
Study design
Traditionally, the evaluation of older adults’ mobility is based on self-reporting and subjective indicators. Although such indicators are usually considered appropriate to characterize the individual mobility of seniors, they are unsuitable for effectively assessing the situation on a larger scale. To overcome this limitation, we conducted a scoping review using bibliometric mapping and clustering. This approach provides an independent view of the structure of scientific discussion on the topic and allows for the identification of common groups of problems and neutral assessment/quantification of co-occurrences and associations, free from the researchers’ biases.
We followed the five-step research process outlined by Arksey and O'Malley [31] as the methodological framework for a scoping review. Before making a final decision, the research questions were determined and the significance of the study was established. Data were then collected, summarized, reported, and eventually visualised. To ensure a comprehensive and methodical overview of the factors affecting mobility in the elderly, we employed the above-mentioned framework for the scoping review approach in accordance with PRISMA standards [11] and the bibliometric mapping study method [12].
To minimize bias and potential for errors, two groups of reviewers (first group: Krejcar, Maskuriy, Abu Bakar, Selamat and second group: Maresova, Truhlarova, Vitkova, Joukl, Horak) independently coded each study with a present form or data extraction tool. They collected study details, such as methods and design, participants, setting, interventions, and results.
Data extraction and study quality evaluation eligibility
Eligible works were sorted by the researchers who had independently reviewed the studies. Each paper was examined in terms of its title, the author(s), publication type, and language. Studies meeting the following specific set of criteria were selected for further review:
-
1.
Published until 2021
-
2.
Focusing on studies related to older adults
-
3.
Focusing on studies analysing life space environment and mobility determinants
Publications were excluded if they met any of the following criteria:
-
1.
If the mobility was understood as a senior’s willingness to move
-
2.
If mobility was perceived as a part of recreational travel (holidays, etc.)
-
3.
If seniors were a minority group in the research and their perspective was analysed only marginally
-
4.
If the focus was on aspects of population distribution in specific urban areas by age
-
5.
If mobility was examined as one of the factors at the end of the research objective (mobility, perception of loneliness, evaluation of the type of accommodation, etc.)
We collected bibliometric studies of papers published from 2007 to 2021 in Scopus and Web of Science (WoS) as of 16 November 2021. The starting year was set at a minimum number of 10 papers per year, which was reached in 2007 with 11 papers. The number of papers increased over time, with 108 papers in 2021 in WoS. The search used the following keywords: (((spatial mobility) and ((elderly) or (senior) or (geriatric) or (older) or (aging)) and (home or model))) in all fields. For WoS, only the Social Sciences Citation Index (SSCI) and Science Citation Index Expanded (SCI-E) were selected. The search criteria were also limited in terms of publication type, and this to Article, Early Access, or Review Article. The number of results obtained is listed in Table 1. The majority of papers were published in the International Journal of Environmental Research and Public Health [17], Journal of Transport Geography [16], Population Space and Place [16], Plos One [14], and ISPRS International Journal of Geo Information [9]. Eight articles were published in Scientific Reports, Transportation and Transportation Research Record. The papers covered various WoS Categories, with the highest numbers in Geography [32], Public Environmental Occupational Health [33], Transportation [34], Environmental Sciences [35], Environmental Studies [36], and others.
Data selection
The final data selection process from the search result set was conducted following the PRISMA framework [11], as shown in Fig. 1.

Systematic review and meta-analysis following the PRISMA flow of articles with the final selection
A total of 760 publications were initially identified through the search on WoS and Scopus using the search term “(((spatial mobility) and ((elderly) or (senior) or (geriatric) or (older) or (ageing)) AND (home OR model))”. This resulted in 536 papers from WoS and 252 papers from Scopus. After removing duplicates, the number was reduced to less than 132 papers. Due to the lack of granularity in the keyword search and the inability to narrow down the search topics based on keywords and focus areas, a manual scoping process was employed to identify the most relevant papers. Many of the initially identified works were found to be irrelevant, resulting in the final selection of 139 articles with correct and suitable content based on a deeper analysis of their abstracts. Additional 87 papers were excluded from the selection, finally leaving a total of 52 fully synthesized records for analysis. Details of these analysed records are summarised in Tables 6 and 7.
Bibliometric mapping
Bibliometric mapping is a technique that provides a visual representation of the performance of published studies, describing the perception and information related to a specific research area and the real possibilities of mobility.
This technique, introduced by Garfield [37], involves the application of a set of mathematical methods and statistics to analyse and measure publications. It aims to establish qualitative and quantitative changes within a given scientific research topic and detect publication profiles and trends within a discipline [38].
Bibliometric analyses use bibliographical material to organize and analyse information in a particular field, providing valuable insights for experts assessing scientific activity. These analyses help in understanding the past, identifying advances in research, and enhancing future investigations.
Scientific mapping, as used in analysing the evolution of specific research subjects [13], enables the identification of subject fields and demonstrates their progress using various visualization tools in research planning.
VOSviewer, a free software solution developed by van Eck and Waltman [39], is employed for building and visualizing bibliometric maps. It offers the major advantage of selecting and classifying scientific documents, particularly for constructing conceptual maps.
Results
Bibliometric mapping
Results according to countries
First, the analysis of countries where research on the mobility of seniors is focused was conducted. Figure 2 illustrates the co-authorship of countries that have published at least 5 papers related to the search defined in “Study design” section in the respective databases from 2007 to 2021.

Co-authorship of countries in Web of Science (left) and Scopus (right)
Table 2 shows the co-authorship data for both databases. Link strength is a metric that captures the number of other keywords with which the specified keyword co-occurred (i.e., was linked) in the reviewed database [39]. In Web of Science, out of 70 countries, 29 meet the thresholds. The United States published the most with 176 documents, followed by England [40] and the Netherlands [41]. In Scopus, out of 53 countries, 19 meet the thresholds. The United States still published the most in Scopus with 76 documents, followed by Canada [28] and China [27]. The United States has the strongest connection to the keywords searched, with links to a maximum of 24 countries and a links strength of 117, making it the leader in the research topic. The last row in Table 2 represents the results for EU countries, which show higher values compared to the United States.
Figure 3 shows that the correlation between the population of people aged 65 + in a country and the number of papers on spatial mobility is weak. Some countries (Japan) do not investigate the issue of spatial mobility, while the Nordic countries do. The United States is an exception, where the publishing activity is proportional to the senior population.

A Sankey diagram of the connection between the shares of seniors (Population 65 + ; left part) in a selected country [42] and the share of the searched papers from the total publishing activity of the given country in the period from 2007 to 2021 in WoS
Cluster analysis of keywords
Using the terms “spatial mobility” and (“elderly” or “senior” or “geriatric” or “older” or “ageing”) AND “(home OR model)” in Web of Science and Scopus from 2007 to 2021, we were able to locate, evaluate, and analyse the published works to determine their structure and trends. The most frequently used keywords for conducting keyword searches were identified, as shown in Fig. 4 generated by VOSviewer. In VOSviewer, the overall strength of each keyword’s linkages with other terms and its frequency of occurrence were calculated. Co-occurrence analysis was performed to establish the proximity of keywords within articles (name, abstract, or keyword set) and focus on the topic of research [43]. Each individual circle represents one keyword, with the size of the circle indicating the number of occurrences of the specific keyword. The links between these keywords (circles) represent papers where both keywords occur, and the thickness of the links represents the strength of their connections (links).

Co-occurring keywords in Web of Science and Scopus clustered into 4 clusters with different colours (red, green, blue, yellow)
The graph of the WoS collection shows an intersection of four clusters or domains. These clusters include the individual performance cluster (yellow), which consists of keywords related to balance, dementia, gait, etc.; the basic health and social cluster (blue), likely formed by sociological papers; the mobility cluster (green); and an overlap between the mobility cluster and the environment cluster (red). This indicates three main drivers for older adults: individual performance, health and social factors, and mobility connected with the environment and social aspects.
The WoS collection contains more medical and geriatric papers, often related to LSM, as reflected in the individual performance cluster.
Co-occurrence refers to the proximity of a keyword in the title of the research work, the abstract, and its list of keywords [44].
Tables 3 and 4 show the most commonly associated keywords within the identified clusters, considering keywords that co-occurred in at least 10 articles. In Web of Science, out of a total of 3716 keywords, 70 met the threshold, and 5 clusters were identified from the top 50 keywords. In Scopus, although the number of publications was much lower than in Web of Science, the total number of keywords found was similar, with a minimum of 10 occurrences of a keyword. Overall, 3221 keywords were found in Scopus, 65 keywords met the threshold, and 3 clear clusters were identified. The top co-occurring keywords in Web of Science, apart from the main keywords and demography, were ‘pattern’ (43 occurrences), ‘health’ [45], ‘physical activity’ [42], ‘migration’ [38], and ‘behavior’ [37]. In Scopus, the top co-occurring keywords were ‘population dynamics’ (41 occurrences), ‘spatial analysis’ [38], ‘activities’ [26], ‘cognition’ [25], ‘physiology‘ [25], and ‘walking’ [24]. The co-occurrences and connection strengths to the keywords are shown in Table 5.
Some keywords, such as ‘Accessibility’ and ‘mobility’, can be seen as factors or determinants related to the keyword search, as confirmed in Tables A1, A2 and A3 in the annex, which show that the top 10 keywords are most closely linked to the keywords ‘mobility’, ‘Accessibility’, and ‘spatial mobility’ in Web of Science and may serve as determinants for the keywords search. For example, ‘patterns’, ‘health’, ‘migration’, ‘built environment’, ‘transport’, ‘risk’, ‘disability’, ‘neighborhood’, ‘physical activity’, and ‘distance’ were linked to ‘mobility’ in WoS.
In Scopus, ‘mobility’ and ‘spatial analysis’ have similar weights as in Web of Science, as confirmed in Tables A4 and A5 in the annex. Both terms indicate high overlap in the list of keywords, particularly in keywords with higher total link strength (TLS). However, spatial analysis is linked with the urban environment (keywords: ‘urban area’, ‘urban population’), socioeconomic factors, and risk factors.
Preliminary clustering conducted with VOSviewer provided insights into the relationships, occurrences, and co-occurrences of keywords and helped to select those that represent the main common influencing factors. This enabled the proposal of a final clustering/categories in Fig. 5. Three comprehensive clustering distributions with nine sub-clusters were selected and named (Fig. 5). The first cluster encompasses a wide range of challenges related to accessibility and ability. The second cluster focuses on individual and environmental conditions that influence determinants of mobility. The third cluster reflects opportunities in the community, facility, technology, and individuality that influence perception, accessibility, and the improvement of spatial mobility.

Thematic mobility clusters based on the co-occurring keywords identified with VOSviewer
Determinants of elderly mobility
Table 6 provides an overview of selected publications that focused on mobility determinants in older adults, including their main purpose, methods used, results, and constraints. A qualitative approach was employed in the research in this section. The keywords clustered below are already included within the thematic clusters, which encompass studies from the areas of accessibility, personal ability and disability, individual and environmental conditions, community, facility, and technology.
The issue of mobility among older adults can be divided into three thematic units, although due to some overlaps, there are three thematic units based on four clusters. The titles of clusters represent the thematic focus, with subtitles specifying the main topic within each cluster. The first group, termed ‘challenges’, primarily based on cluster 1, encompasses accessibility, personal ability and disability, and factors related to older adults’ behaviour, QoL, and health complications that are relevant to mobility. This area focuses on personal challenges, self-activity, healthy lifestyle, rehabilitation, and exercise that can promote mobility. The second area, termed ‘conditions’, based on clusters 2 and 4, focuses on defining individual and environmental conditions that affect mobility and accessibility. The last area is related to community, facility, technologies, and individual possibilities. It explores opportunities to improve mobility, treatment models in healthcare, the use of modern technologies to promote mobility, and new technologies for its monitoring and research. This topic also considers research on facilities where older adults receive care, as these often incorporate equipment with modern technologies, as indicated by cluster 3, particularly evident form Scopus keywords in Table 6. The individual topic focuses on the interplay between neighbourhood and individual factors, such as health conditions and individual perception of mobility as an opportunity to influence overall health status, improve metabolism, overcome some disabilities, and reduce the risk of mortality. Table 6 summarises 52 studies considered crucial within the above thematic units.
Regarding the determinants of mobility, several main findings have been identified. The selected determinants for further consideration are those that appear in multiple studies.
The total number of trips, including trips away from home, tends to decrease among older adults in higher age groups. Reduced mobility in people over the age of 65 is associated with factors such as living alone, physical disabilities, reliance on foot or bicycle transportation, lower education levels, longer distance to public transportation, inability to drive, and residing in less affluent areas. Furthermore, the frequency of work-related and shopping trips decreases with increasing age. Older adults who live alone travel less for work and leisure activities. Individuals with severe disabilities make fewer trips for work, shopping, and recreation, but they have more frequent doctor visits. The presence of employment influences travel patterns, with employed individuals making more work-related trips and fewer trips for physical activity, recreation, and socialising. The frequency of their outings for shopping, physical activity, leisure, and socialising remains consistent on weekdays and weekends. Gender primarily affects the frequency of shopping trips. Older adults who are less likely to travel outside their immediate neighbourhood tend to be those who are more elderly, severely disabled, rely on the bicycle, walking, or local bus as their primary mode of transportation; are less educated; live further than 10 min from the nearest subway; or are unable to drive themselves. Travelling for pleasure is less common, but activities such as shopping, dining, attending church, and seeing friends are more frequent among those aged 65 to 69 years old (i.e., the youngest older persons). This age group engages in a variety of activities, often within their neighbourhoods. In terms of the frequency of leisure trips, older adults aged 80 or more years come in second, followed by those who are severely incapacitated [64].
The mobility habits of older individuals are influenced by the time of day and the location in which they reside. Mandatory journeys tend to be shorter, while non-mandatory excursions are longer, especially during off-peak hours when transportation options are more readily available. Although their impacts are less pronounced than previously suggested, they nonetheless have a major impact. Age-specific light buses, which have evolved from a legislative concept to community-based organisations, offer transportation services for older persons within their districts [71].
In 2017–2018, older individuals reported frequent visits to various activity sites, including museums, libraries, and parks. Exercise, mobility, and other activities linked to everyday life (e.g., grocery shopping and the utilisation of health and meal services) were all included in these destinations of cultural and social visits. COVID-19 restrictions enforced by the Finnish government in 2020 resulted in older individuals reporting only physical exercise-related destinations as their preferred mode of transportation. As a result of these restrictions, it was either difficult or unpleasant to participate in other activities (e.g., eateries, museums, and planned collective events). During the COVID-19 pandemic, additional activities of individuals were primarily tied to their everyday routines. According to previous research, older individuals were more physically active when they were near their homes, and the elderly spent more time at home and within their neighbourhoods when mobility restrictions were in place to minimise the spread of COVID-19 [88, 89].
Based on the current state of knowledge, especially from the areas of strategic documents and government acts, it can be assumed that availability, local mobility systems (LMS), and technologies are important for the mobility of seniors. In the following text, the findings from the scoping review are therefore interpreted in relation to these assumptions.
Zones of living space
In the review process shown in Fig. 5, the findings of the studies were classified into three groups, with one group named ‘condition’ and further divided into individual and environmental subgroups. These classifications were connected to five zones of living. As shown in Table 6, the studies focus mainly on the external environment, such as neighbourhoods and distant places.
Table 7 shows the distribution of papers, indicating better coverage for zones 4–5 [90], while papers focusing on in-house mobility are less frequent in the sample. Regarding environmental conditions, studies indicate determinants that affect senior mobility. For instance, Peel et al. [91] found that living space was related to mobility, physical performance assessments, transportation problems, mental state, and depression in a population-based sample of seniors.
Different zones of life space were associated with performance-based measures of function, namely, visual impairment, and several measures of lower extremity motor function. Moreover, even after controlling for demographic variables (age, sex, education, and time of year), visual impairment, and lower extremity motor function, life space was also associated with levels of global cognition, extraversion, and having a future goal-oriented purpose in life. Higher scores on each of these variables were associated with larger life spaces.
A decline in LSM is associated with a decline in QoL among community-dwelling older people, even after considering potential confounders. The association between the decline in LSM and QoL can be explained in several ways. First, diminished opportunities for participation in outdoor activities and the resulting insufficient social interaction may lead to social isolation and loneliness, which, in turn, may lead to poor QoL [92]. Second, reduced time spent outdoors and hence, lower levels of physical activity and increased sedentary behaviour may have adverse effects on health and thus a negative influence on QoL [93]. Spending time outdoors may also have a direct effect on QoL, as people, especially in the Finnish context, often like to enjoy the outdoors, which has been shown to enhance their well-being [32]. Third, a decline in LSM may indicate difficulties in taking care of daily errands independently, which may also contribute to a sense of losing control over one’s life [61].
Increased LSM is associated with objectively measured physical activity indicators, such as step count, moderate and low activity time, and sedentary time. Going outdoors in the neighbourhood at least once a week has been found to be beneficial for maintaining physical function in frail older people. Finding ways to encourage community-dwelling older people to go outdoors more often may increase their physical activity level and help to maintain their physical function. Poor health, low physical activity, and mobility limitations often coincide in the same individuals [34].
Some studies explore the link between mobility and other aspects of the natural environment. To give one example, Hinrichs et al. [62] have discovered that elderly people who perceive parks or green spaces in their neighbourhood as encouraging outdoor mobility are more likely to visit their regular grocery shop, regardless of whether they walk to the grocery store or not. The impression of a path as a mobility facilitator is not correlated with an increase in the likelihood of walking for transportation. Additional factors positively associated with walking as a mode of transportation include low private car use, short distance to the store, and a high level of street connectedness.
Accessibility
In terms of accessibility, barriers that affect seniors are identified in their immediate vicinity, including the condition of the terrain and the availability of services, doctors, and basic facilities. The field of research in this area is rapidly developing, with preparations being made to support governments and regions. According to the findings of Ståhl et al. [94], older individuals face mobility issues related to accessing and navigating bus stops, as well as getting on and off buses. Transitioning from a fixed-route system that is not accessible to one that is fully accessible, including the cars, stops, and stations, may take many years. The structure of public transportation networks is determined by the demographics of the population. Rural and suburban communities, particularly those with low population density, still face challenges in terms of mobility. Older individuals living in rural settings are more likely to experience social isolation and have limited socialisation options apart from their families and friends compared to their suburban counterparts [95]. According to the results of Siren et al. [96], providing older people with general mobility and accessibility is essential for their independent living, but it is equally important to support activities that enhance their sense of community belonging.
Physical determinants of mobility within the neighbourhood can include unsuitable environments and equipment at stops, difficulties in boarding and alighting, suboptimal air or temperature conditions inside, orientation in timetables, lack of shade, greenery, toilets, railings, benches, lighting, views of the surroundings, obstacles such as stairs, curbs, parked cars, bicycles, other obstructing objects (posts, stands, bushes), noise, and unpleasant environments. Older adults living in rapidly urbanising environments face challenges in either integrating into or becoming isolated from the society [97]. The concept of New Urbanism and Transit-Oriented Development emphasizes compact forms, mixed-use, high density, and convenient public transportation [98] in order to facilitate spatial mobility among the ageing community and ensure productive ageing.
Mobility aspects under consequences of development emerging technologies
The study of topics and keywords in the current period of spatial mobility research has revealed that technological factors are playing an increasingly significant role. Scholars have recognized that the spatial mobility of older adults cannot overlook the technological dimension, which has the potential to significantly improve their physical and mental capabilities and performance. However, there is also a concern about an increase in social inequity due to the affordability and accessibility of such technological tools. Technologies are being developed to focus on mobility within the home, as well as on mobility and safety outside the house and in the neighbourhood. New technology is being designed to address geriatric mobility problems such as falls, bed rail entrapment, patient management, and wandering. These technologies aim to prevent or reduce adverse events that hinder therapy, delay rehabilitation, exacerbate impairment, and jeopardize patient safety. Examples of such technologies include hip guards, wheelchair and scooter safety systems, smart walkers, falling alerts, and environment assistance, which can help to reduce falls and fall-related injuries [99].
Technological solutions for the healthcare needs of the elderly include (1) linking and sharing medical data in networks among users, including medical check-ups, treatment, and care records; (2) providing remote medical care assistance; and (3) utilising AI and robots in treatment facilities to support autonomy [29]. Wearable transfer aid robots are a priority in order to alleviate the physical burden on caregivers. While the usefulness of these robots in nursing homes is still uncertain, they have shown to be beneficial in experimental settings for a variety of activities. Evaluation of care tasks and time ratios while using these robots indicates that they were prominently used for direct patient care in more than 70% of transits, particularly in transfer assistance and toileting [100]. The use of new outdoor and indoor mobility technologies for individual or medical purposes has both advantages and disadvantages, as shown in Table 8.
To address the challenges mentioned earlier, it is important to ensure that new technology is affordable, easy to use, and secure, and that it seamlessly integrates with existing systems and devices. Furthermore, efforts should be made to provide doctors with training and support to help them to effectively use and implement new technology in outdoor settings. The use of smart technology by seniors presents numerous opportunities for medical specialists, including improved patient outcomes, remote monitoring, increased access to information, improved communication, and better tracking of patient data. To fully realize these benefits, it is important to ensure the seamless integration of new technology with existing systems and devices and to provide seniors with education and support to help them to effectively use and implement new technology in their daily lives.
Discussion
The objective of the study is to identify the factors that have had a significant impact on mobility in recent years and currently, as well as to identify gaps in our understanding of these factors. The study aims to emphasize areas where further research is needed and where new and effective solutions are required.
Within the scoping review, we employed clustering for database results, which provides an independent view of the structure of the scientific discourse on the given problem. Furthermore, it allowed for the identification of common groups of problems and a neutral evaluation of co-occurrences and associations, not influenced by the researchers’ biases. Several studies from our review report that lower mobility among older people is related to family status, health status, and housing location. Family status plays a crucial role, with factors such as living alone or with someone influencing the motivation and need to run a larger household and to engage in mobility-related activities, such as making trips and visiting family members. If this condition of motivation is met and options are available, for example in the form of a driving licence, health status becomes an important factor. Health status is also significant, as deteriorating mental or physical health tends to decrease the distances travelled by older adults. Within urban areas, concerns about personal safety when using certain means of transportation, such as bicycles or cars, are raised. Several innovative solutions are available to address these issues, as these new solutions have been rapidly developing in the past decade and are being discussed within the context of the Society 5.0 phenomenon.
Webber et al. [16] have established fundamental categories of determinants for older adults’ mobility: cognitive, psychosocial, physical, environmental, and financial categories. The clusters generated from the co-occurrence of keywords in this study cover only a part of these fundamental categories, as specific keywords related to individual financial context or cognitive factors were not significantly investigated in the mobility-related papers. Among the fundamental categories, environmental determinants have been frequently studied, and the ‘condition’ cluster in this study combines environmental and individual conditions. The individual condition cluster is closely related to psychosocial factors, among which Webber et al. [16] include self-efficacy, depression, coping mechanisms, anxiety, fearfulness, and relationships with others, which affect interest and motivation for mobility. The combination of environmental and individual conditions confirms the close interdependence of these factors, as a person’s skill level combined with their surroundings contribute to successful mobility outcomes [101]. Physical determinants are mainly reflected in the ‘person disability’ group of ‘challenges’, indicating that the interpretation of these factors is mainly negative and focuses on the gradual erosion of older adults’ physical abilities related to spatial mobility [16]. Table 9 provides a summary of the main mobility factors discussed.
The selected studies highlight accessibility discrepancies between seniors and non-seniors, urban seniors and suburban seniors, and seniors who own vehicles and those who do not (e.g. [50]). In older individuals, possessing a valid driver’s licence is associated with a reduced risk of reporting life space constriction and an increased likelihood of life space recovery if constriction occurs. A total of 71 studies demonstrate that older adults have a higher demand for public transit and experience greater mobility disadvantages than younger adults because they are more reliant on public transit. To facilitate access to healthcare for older individuals, additional healthcare resources should be committed and public transit to healthcare facilities should be improved, particularly in outlying areas. In a total of 72 studies, the results indicate a strong attachment to the place of residence and the surrounding community among older individuals. The particularly high rates of homeownership suggest that future older adults will continue to live at home. The remaining individuals who are potentially mobile aim to relocate within the region or utilize their second homes more frequently, indicating a likelihood of living in multiple locations in the future.
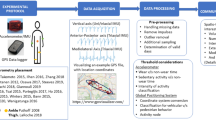
Healthcare solutions for older adults include connecting and sharing information in a network between users of medical data, including medical check-up records and treatment and care records, providing remote medical care services, and integrating AI and robots in care facilities to promote community independence. GPS technology has proven to be a robust and valuable method for acquiring new information, particularly when paired with qualitative data, as is demonstrated in [72]. GPS data loggers can be incorporated into evaluations and interventions. Rantakokko et al. [61] suggest in their findings that longer GPS use is significantly associated with higher cognitive ability. These results indicate that GPS watches may be able to continuously monitor changes in functional health, allowing for informed preventative efforts.
The determinants of mobility examined in the studies include environmental, physical, psychosocial, and cognitive factors, which are investigated in almost all studies. Financial determinants, along with gender, culture, and biography, are less frequently studied. Additionally, the role of technology and the solutions mentioned in Chapter 4.2.3 on Society 5.0 should also be considered as new determinants of mobility. Figure 6 provides a visual representation of the confirmed determinants of mobility (green), those currently deemed non-essential (yellow), and those that require reclassification (blue).

Mobility determinants overview
Johnson et al. [7] have found the following main factors influencing mobility (LSM as an outcome variable): age, gender, education, health issues, and physical capabilities and activities. Our findings confirm the main role of age, education, family status, health issues, and physical capabilities. However, the role of gender as well as biography, culture, and financial aspects has not been extensively studied in the studies included in our review. Johnson et al. [7] provide detailed insight into health issues that contribute to decreased LSM, such as stroke, depressive symptoms, undernutrition, and obesity. Among other factors described by the same authors in their review, the role of car utilization, both as drivers and passengers, is also confirmed, usually combined with walking difficulties.
In our study, environmental conditions and locality play an essential role in mobility. Johnson et al. [7] identified a single paper oriented at environmental factors related to restricted LSM (Rantakokko et al. [61]). This particular paper reported environmental barriers, such as high curbs, lack of sidewalks, and missing environmental facilitators, including safe crossings or good lighting. Our findings substantially extend the list of environmental factors and underline the roles of other factors, such as unsuitable environment and equipment of stops, difficulties in boarding and alighting, poor air conditions, orientation in timetables, shade, greenery, toilets, railings, benches, views of the surroundings, stairs, parked cars, bicycles, obstructing objects, noise, or unpleasant environment, and non-aesthetic factors. Understanding which environmental factors are perceived as significant and how they can be improved is crucial for enhancing elderly mobility.
The present research has generated valuable discoveries, but it is important to acknowledge its limitations. To begin with, the precision of search keywords may have led to the exclusion of relevant papers from our study, and the selection of keywords influenced the investigated zones of living, so that, for instance, the coverage of in-house mobility is limited.
Second, differing aims, demographics, and findings were used to classify the publications under analysis. We have excluded travelling for recreational purposes to distinguish gerontological and travel studies related to different determinants. Finally, clustering results in some overlap of topics, which are therefore not as clearly delineated as if they were formulated by researchers. However, such overlap allows an insight into how these factors are interlinked and mutually conditioned.
Conclusion
Reduced mobility among older adults is a complex problem stemming from many areas of human activity and perhaps has more options for improvement. The results of this study reveal that the key determinants of mobility are environmental, physical, cognitive, psychosocial, and technological. In relation to the previous results, we underline the role of modern emerging technologies in overcoming disabilities (or more common geriatric mobility problems). We also emphasise the role of the environment and the interactions between individuals and the environment. Additionally, we have identified more environmental factors than previous studies, including the role of suitable equipment of dwellings and public spaces, as well as street furniture. Based on these key determinants, future research can focus on several areas, including:
-
understanding the interactions between different determinants of mobility: Further research could examine how the different determinants of mobility interact with one another and jointly influence mobility outcomes.
-
Addressing environmental factors that impact mobility: Research could examine the impact of environmental factors such as air pollution, climate change, and access to green spaces on mobility outcomes and identify interventions to address these factors.
-
Identifying interventions to improve cognitive and psychosocial determinants of mobility and examining the impact of mobility on health and well-being.
Given the importance of technological determinants of mobility, future research could focus on developing new technologies or improving existing ones to enhance mobility outcomes. In the context of emerging technologies, important opportunities for future research include:
-
integration of smart home technologies to enhance accessibility and safety for seniors in their homes,
-
development of assistive technologies for mobility, such as exoskeletons and robotic devices, to help seniors with physical limitations move around more easily,
-
design of accessible and age-friendly public spaces, such as sidewalks, public transportation systems, and buildings, to improve mobility for seniors in their communities.
-
utilization of AI and machine learning algorithms to optimize transportation systems and make them more accessible to seniors.
-
study of the impact of autonomous vehicles on senior mobility and the development of policies and regulations that support their safe and equitable use by seniors.
-
investigation of the relationship between physical activity, mobility, and quality of life for seniors and the development of interventions to support healthy ageing.
-
exploration of innovative financing models to support the integration of assistive technologies into the lives of seniors, including the use of public-private partnerships.
Further research on these determinants can help arrive at solutions that, in turn, will improve mobility. Financial determinants have not been widely investigated, so future research should focus of financial determinants, especially since many technological solutions are expensive and not commonly available, which limits their use.
The number of older adults is increasing in developed countries, and there is increased consumer potential. This may be a strong motivation for public and private entities to develop innovative and supportive activities for this target group. Addressing mobility challenges for older adults involves a multidisciplinary approach that includes healthcare providers, policymakers, urban planners, and families.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Burlando C, Cusano I. Growing old and keep mobile in Italy. Active ageing and the importance of urban mobility planning strategies. Tema J Land Use. 2018:43–52. Mobility and Environment.
National Institute on Aging. Maintaining mobility and preventing disability are key to living independently as we age. 2020; Available from: https://www.nia.nih.gov/news/maintaining-mobility-and-preventing-disability-are-key-living-independently-we-age#.
World Health Organization. WHO Global Report on Falls Prevention in Older Age. 2007; Available from: https://extranet.who.int/agefriendlyworld/wp-content/uploads/2014/06/WHo-Global-report-on-falls-prevention-in-older-age.pdf.
World Health Organization. Global age-friendly cities: a guide. Feuille de route pour des ‘villes-amies’ des ainés. 2007; Available from: https://apps.who.int/iris/handle/10665/43755 [cited 3 Feb 2023].
How to deal with competing access needs. Independence Australia. 2020; Available from: https://www.independenceaustralia.com.au/tips-and-advice/competing-access-needs-tips/.
European Comission. Employment, Social Affairs & Inclusion. Available from: https://ec.europa.eu/social/main.jsp?catId=1202.
Johnson J, Rodriguez MA, Al SS. Life-space mobility in the elderly: current perspectives. CIA. 2020;15:1665–74.
Porter AL, Roessner JD, Jin XY, Newman NC. Measuring national ‘emerging technology’ capabilities. Sci and Pub Pol. 2002;29(3):189–200.
Cozzens S, Gatchair S, Kang J, Kim KS, Lee HJ, Ordóñez G, et al. Emerging technologies: quantitative identification and measurement. Technol Anal Strateg Manag. 2010;22(3):361–76.
Smalheiser NR. Predicting emerging technologies with the aid of text-based data mining: the micro approach. Technovation. 2001;21(10):689–93.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):97.
Leung XY, Sun J, Bai B. Bibliometrics of social media research: a co-citation and co-word analysis. Int J Hosp Manag. 2017;66:35–45.
Rodríguez-Bolívar MP, Alcaide-Muñoz L, Cobo MJ. Analyzing the scientific evolution and impact of e-Participation research in JCR journals using science mapping. Int J Inf Manage. 2018;40:111–9.
Bowling A, Banister D, Sutton S, Evans O, Windsor J. A multidimensional model of the quality of life in older age. Aging Ment Health. 2002;6(4):355–71.
European Council, Council of the European Union. Accessibility to products and services for disabled and elderly people. Available from: https://www.consilium.europa.eu/en/policies/accessibility-goods-services/.
Webber SC, Porter MM, Menec VH. Mobility in older adults: a comprehensive framework. Gerontologist. 2010;50(4):443–50.
Cao X (Jason), Mokhtarian PL, Handy SL. Neighborhood design and the accessibility of the elderly: an empirical analysis in Northern California. Int J Sustain Transp. 2010;4(6):347–71.
Lyubomirsky S. The how of happiness: a practical approach to getting the life you want. Paperback edition. 2010. p. 373.
Kafková MP, Vidovićová L, Wija P. Older Adults and civic engagement in rural areas of the Czech Republic. Eur Countryside. 2018;10(2):247–62.
Tiran J, Lakner M, Drobne S. Modelling walking accessibility: a case study of Ljubljana. Slovenia Moravian Geograph Rep. 2019;27(4):194–206.
Hemingway A, Jack E. Reducing social isolation and promoting well being in older people. Qual Ageing Older Adults. 2013;14(1):25–35.
Umberson D, Karas Montez J. Social relationships and health: a flashpoint for health policy. J Health Soc Behav. 2010;51(1):S54–66.
Schrempft S, Jackowska M, Hamer M, Steptoe A. Associations between social isolation, loneliness, and objective physical activity in older men and women. BMC Public Health. 2019;19(1):74.
Hwang TJ, Rabheru K, Peisah C, Reichman W, Ikeda M. Loneliness and social isolation during the COVID-19 pandemic. Int Psychogeriatr. 2020;32(10):1217–20.
Geurs KT. Accessibility, land use and transport: accessibility evaluation of land-use and transport developments and policy strategies. 2006. Available from: http://igitur-archive.library.uu.nl/dissertations/2006-0613-200112/full.pdf [cited 16 Jan 2022].
Sloan CD, Nordsborg RB, Jacquez GM, Raaschou-Nielsen O, Meliker JR. Space-time analysis of testicular cancer clusters using residential histories: a case-control study in Denmark. PLoS One. 2015;10:285 1160 Battery street, STE 100, San Francisco, CA 94111 USA: Public library science.
Benenson I, Martens K, Rofé Y, Kwartler A. Public transport versus private car GIS-based estimation of accessibility applied to the Tel Aviv metropolitan area. Ann Reg Sci. 2011;47(3):499–515.
Shrestha BP, Millonig A, Hounsell NB, McDonald M. Review of public transport needs of older people in european context. Popul Ageing. 2017;10(4):343–61.
Elsy P. Elderly care in the society 5.0 and kaigo rishoku in Japanese hyper-ageing society. Indones J Commun Stud. 2020;4(2):435.
Fraade-Blanar L, Larco N, Best R, Swift T, Blumenthal MS, AARP Public Policy Institute. Older Adults, New Mobility, and Automated Vehicles. Washington, DC: AARP Public Policy Institute; 2021. Available from: https://www.aarp.org/ppi/info-2021/older-adults-new-mobility-and-automated-vehicles.html. [cited 13 Jan 2022].
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32.
Fagerholm N, Eilola S, Arki V. Outdoor recreation and nature’s contribution to well-being in a pandemic situation - Case Turku, Finland. Urban For Urban Green. 2021;64:127257.
Isaacson M, Tripathi A, Samanta T, D’Ambrosio L, Coughlin J. Giving voice to the environment as the silent partner in aging: examining the moderating roles of gender and family structure in older adult wellbeing. Int J Environ Res Public Health. 2020;17:4373 ST Alban-Anlage 66, CH-4052 Basel, Switzerland: MDPI.
Tsai LT, Portegijs E, Rantakokko M, Viljanen A, Saajanaho M, Eronen J, et al. The association between objectively measured physical activity and life-space mobility among older people. Scand J Med Sci Sports. 2015;25:e368–73 111 River St, Hoboken 07030-5774, NJ USA: Wiley.
Saajanaho M, Rantakokko M, Portegijs E, Tormakangas T, Eronen J, Tsai LT, et al. Personal goals and changes in life-space mobility among older people. Prevent Med. 2015;81:163–7 525 B ST, STE 1900, San Diego, CA 92101-4495 USA: Academic Press Inc Elsevier Science.
Shoval N, Wahl HW, Auslander G, Isaacson M, Oswald F, Edry T, et al. Use of the global positioning system to measure the out-of-home mobility of older adults with differing cognitive functioning. Ageing Soc. 2011;31:849–69 32 Avenue of the Americas, New York, NY 10013-2473 USA: Cambridge Univ Press.
Garfield E. Citation indexes for science: a new dimension in documentation through association of ideas. Science. 1955;122(3159):108–11.
Daim TU, Rueda G, Martin H, Gerdsri P. Forecasting emerging technologies: use of bibliometrics and patent analysis. Technol Forecast Soc Chang. 2006;73(8):981–1012.
van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–38.
Wu D, Gao X, Xie Z, Xu Z. Understanding the unmet needs among community-dwelling disabled older people from a linkage perspective. Int J Environ Res Public Health. 2021;18:389 ST Alban-Anlage 66, CH-4052 Basel, Switzerland: MDPI.
Portegijs E, Rantakokko M, Viljanen A, Sipila S, Rantanen T. Identification of older people at risk of ADL disability using the life-space assessment: a longitudinal cohort study. J Am Med Dir Assoc. 2016;17:410–4 360 Park Ave South, New York, NY 10010-1710 USA: Elsevier Science Inc.
Health Nutrition And Population Statistics. The World Bank; 2022. Available from: https://datacatalog.worldbank.org/search/dataset/0037652/Health-Nutrition-and-Population-Statistics?showIndicators=true [cited 4 Jul 2022].
Bornmann L, Haunschild R, Hug SE. Visualizing the context of citations referencing papers published by Eugene Garfield: a new type of keyword co-occurrence analysis. Scientometrics. 2018;114(2):427–37.
van Eck NJ, Waltman L. Visualizing bibliometric networks. measuring scholarly impact. 2014:285–320.
Sartori AC, Wadley VG, Clay OJ, Parisi JM, Rebok GW, Crowe M. The relationship between cognitive function and life space: the potential role of personal control beliefs. Psychol Aging. 2012;27:364–74 750 First St NE, Washington, DC 20002-4242 USA: Amer Psychological Assoc.
Bayat S, Naglie G, Rapoport MJ, Stasiulis E, Widener MJ, Mihailidis A. A GPS-based framework for understanding outdoor mobility patterns of older adults with dementia: an exploratory study. Gerontology. 2022;68(1):106–20. https://doi.org/10.1159/000515391. Epub 2021 Apr 23.
Giannouli E, Bock O, Zijlstra W. Cognitive functioning is more closely related to real-life mobility than to laboratory-based mobility parameters. Eur J Ageing. 2018;15:57–65 233 Spring ST, New York, NY 10013 USA: Springer.
DiSalvio NL, Rosano C, Aizenstein HJ, Redfern MS, Furman JM, Jennings JR, et al. Gray matter regions associated with functional mobility in community-dwelling older adults. J Am Geriatr Soc. 2020;68:1023–8 111 River ST, Hoboken 07030-5774, NJ USA: Wiley.
Byles JE, Leigh L, Vo K, Forder P, Curryer C. Life space and mental health: a study of older community-dwelling persons in Australia. Aging Mental Health. 2015;19:98–106 2-4 Park Square, Milton PARK, Abingdon OX14 4RN, Oxon, England: Routledge Journals, Taylor & Francis LTD.
Roberts H, Helbich M. Multiple environmental exposures along daily mobility paths and depressive symptoms: a smartphone-based tracking study. Environ Int. 2021;156:106635 The boulevard, Langford lane, Kidlington, Oxford OX5 1GB, England: Pergamon-Elsevier Science Ltd.
Schwenk M, Mohler J, Wendel C, D’Huyvetter K, Fain M, Taylor-Piliae R, et al. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: baseline results of the arizona frailty cohort study. Gerontology. 2015;61:258–67 Allschwilerstrasse 10, CH-4009 Basel, Switzerland: Karger.
Ullrich P, Werner C, Eckert T, Bongartz M, Kiss R, Feisst M, et al. Cut-off for the life-space assessment in persons with cognitive impairment. Aging Clin Exp Res. 2019;31:1331–5 233 Spring St, New York, NY 10013 USA: Springer.
Ngui AN, Apparicio P, Fleury MJ, Gregoire JP, Moisan J, Lesage A, et al. Disentangling the influence of neighborhood and individual characteristics on early residential mobility among newly diagnosed patients with schizophrenia: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2014;49:1569–78 Tiergartenstrasse 17, D-69121 Heidelberg, Germany: Springer Heidelberg.
Paez A, Mercado RG, Farber S, Morency C, Roorda M. Accessibility to health care facilities in Montreal Island: an application of relative accessibility indicators from the perspective of senior and non-senior residents. Int J Health Geogr. 2010;9:1–5 Campus, 4 Crinan St, London N1 9XW, England: BMC.
Chung J, Ozkaynak M, Demiris G. Examining daily activity routines of older adults using workflow. J Biomed Inform. 2017;71:82–90.
Shah RC, Maitra K, Barnes LL, James BD, Leurgans S, Bennett DA. Relation of driving status to incident life space constriction in community-dwelling older persons: a prospective cohort study. J Gerontol A Biol Sci Med Sci. 2012;67:984–9.
Mercado R, Paez A. Determinants of distance traveled with a focus on the elderly: a multilevel analysis in the Hamilton CMA, Canada. J Transport Geogr. 2009;17:65–76 The boulevard, Langford lane, Kidlington, Oxford OX5 1GB, Oxon, England: Elsevier Sci Ltd.
Portegijs E, Rantakokko M, Mikkola TM, Viljanen A, Rantanen T. Association between physical performance and sense of autonomy in outdoor activities and life-space mobility in community-dwelling older people. J Am Geriatr Soc. 2014;62:615–21 111 River ST, Hoboken 07030-5774, NJ USA: Wiley.
Barnes LL, Wilson RS, Bienias JL, de Leon CFM, Kim HJN, Buchman AS, et al. Correlates of life space in a volunteer cohort of older adults. Exp Aging Res. 2007;33:77–93 325 Chestnut St, SuitE 800, Philadelphia, PA 19106 USA: Taylor & Francis Inc.
Choi M, O’Connor ML, Mingo CA, Mezuk B. Gender and racial disparities in life-space constriction among older adults. Gerontologist. 2016;56:1153–60 Journals Dept, 2001 Evans Rd, Cary, NC 27513 USA: Oxford Univ Press Inc.
Rantakokko M, Portegijs E, Viljanen A, Iwarsson S, Kauppinen M, Rantanen T. Changes in life-space mobility and quality of life among community-dwelling older people: a 2-year follow-up study. Qual Life Res. 2016;25:1189–97 van Godewijckstraat 30, 3311 GZ Dordrecht, Netherlands: Springer.
Hinrichs T, Keskinen KE, Pavelka B, Eronen J, Schmidt-Trucksass A, Rantanen T, et al. Perception of parks and trails as mobility facilitators and transportation walking in older adults: a study using digital geographical maps. Aging Clin Exp Res. 2019;31:673–83 One New York Plaza, Suite 4600, New York, NY, United States: Springer.
Chung J, Boyle J, Wheeler DC. Relationship between life-space mobility and health characteristics in older adults using global positioning system watches. J Appl Gerontol. 2022;41(4):1186–95. https://doi.org/10.1177/07334648211054834. Epub 2021 Oct 31.
Noh SH, Joh CH. Analysis of elderly travel patterns in Seoul metropolitan area, South Korea, through sequence alignment and motif search. Transp Res Rec. 2012;2323:25–34 2455 ℡LER Rd, Thousand Oaks, CA 91320 USA: Sage Publications Inc.
Bruechert T, Hasselder P, Quentin P, Bolte G. Walking for transport among older adults: a cross-sectional study on the role of the built environment in less densely populated areas in Northern Germany. Int J Environ Res Public Health. 2020;17:9479 ST Alban-Anlage 66, CH-4052 Basel, Switzerland: MDPI.
Perchoux C, Kestens Y, Thomas F, Hulst AV, Thierry B, Chaix B. Assessing patterns of spatial behavior in health studies: their socio-demographic determinants and associations with transportation modes (the RECORD Cohort Study). Soc Sci Med. 2014;119:64–73.
Hasanzadeh K, Kytta M, Lilius J, Ramezani S, Rinne T. Centricity and multi-locality of activity spaces: the varying ways young and old adults use neighborhoods and extra-neighborhood spaces in Helsinki Metropolitan area. Cities. 2021;110:103062 The boulevard, Langford Lane, Kidlington, Oxford OX5 1GB, Oxon, England: Elsevier Sci Ltd.
Lord S, Joerin F, Theriault M. Daily mobility of aging and elderly suburbanites: trips, aspirations and meanings of mobility. Can Geographer-Geographe Canadien. 2009;53:357–75 111 River St, Hoboken 07030-5774, NJ USA: Wiley.
Li KK, Yang DF. Identification of Key Building Environment Factors Affecting Walking Efficiency of the Elderly [影响老年人步行效能的关键性建成环境要素识别]. Jiaotong Yunshu Xitong Gongcheng Yu Xinxi/J Transp SysT Eng Inform Technol. 2021;21(2):245–50.
Snih SA, Peek KM, Sawyer P, Markides KS, Allman RM, Ottenbacher KJ. Life-space mobility in mexican americans aged 75 and older. J Am Geriatr Soc. 2012;60(3):532–7.
He SY, Cheung YHY, Tao S. Travel mobility and social participation among older people in a transit metropolis: a socio-spatial-temporal perspective. Transp Res Part A Policy Pract. 2018;118:608–26 The boulevard, Langford lane, Kidlington, Oxford OX5 1GB, England: Pergamon-Elsevier Science Ltd.
Fillekes MP, Giannouli E, Kim EK, Zijlstra W, Weibel R. Towards a comprehensive set of GPS-based indicators reflecting the multidimensional nature of daily mobility for applications in health and aging research. Int J Health Geogr. 2019;18:17 Campus, 4 Crinan St, London N1 9XW, England: BMC.
Su R, Xiao J, McBride EC, Goulias KG. Understanding senior’s daily mobility patterns in California using human mobility motifs. J Transport Geogr. 2021;94:103117 the boulevard, Langford lane, Kidlington, Oxford OX5 1GB, Oxon, England: Elsevier Sci Ltd.
Frantal B, Klapka P, Novakova E. When home becomes a cage: Daily activities, space-time constraints, isolation and the loneliness of older adults in urban environments. Moravian Geogr Rep. 2020;27:322–37 Bogumila Zuga 32A, Warsaw, Mazovia, Poland: Sciendo.
Heatwole Shank KS. Fidelity and utility of GPS loggers as a tool for understanding community participation of older adults. Scand J Occup Ther. 2022;29(4):282–92. https://doi.org/10.1080/11038128.2021.1921841. Epub 2021 May 25.
Tao Z, Cheng Y. Modelling the spatial accessibility of the elderly to healthcare services in Beijing, China. Environ Planning B-Urban Anal City Sci. 2019;46:1132–47 1 Olivers yard, 55 City road, London EC1Y 1SP, England: Sage Publications Ltd.
Kramer C, Pfaffenbach C. Should I stay or should I go? Housing preferences upon retirement in Germany. J Housing Built Environ. 2016;31:239–56 van Godewijckstraat 30, 3311 GZ Dordrecht, Netherlands: Springer.
Laatikainen TE, Haybatollahi M, Kytta M. Environmental, individual and personal goal influences on older adults’ walking in the Helsinki metropolitan area. Int J Environ Res Public Health. 2019;16:58.
Loo BPY, Lam WWY, Mahendran R, Katagiri K. How is the neighborhood environment related to the health of seniors living in Hong Kong, Singapore, and Tokyo? Some insights for promoting aging in place. Ann Am Assoc Geographers. 2017;107:812–28.
Arentze T, Timmermans H, Jorritsma P, Kalter MJO, Schoemakers A. More gray hair - but for whom? Scenario-based simulations of elderly activity travel patterns in 2020. Transportation. 2008;35:613–27 One New York Plaza, Suite 4600, New York, NY, United States: Springer.
Rosso AL, Tabb LP, Grubesic TH, Taylor JA, Michael YL. Neighborhood social capital and achieved mobility of older adults. J Aging Health. 2014;26:1301–19 2455 ℡LER RD, Thousand OakS, CA 91320 USA: Sage Publications Inc.
Phillips J, Walford N, Hockey A, Foreman N, Lewis M. Older people and outdoor environments: pedestrian anxieties and barriers in the use of familiar and unfamiliar spaces. Geoforum. 2013;47:113–24 the boulevard, Langford lane, Kidlington, Oxford OX5 1GB, England: Pergamon-Elsevier Science Ltd.
Sanchez M, Ambros A, Salmon M, Bhogadi S, Wilson RT, Kinra S, et al. Predictors of daily mobility of adults in Peri-Urban South India. Int J Environ Res Public Health. 2017;14:783 St Alban-Anlage 66, CH-4052 Basel, Switzerland: MDPI.
Grove H. Ageing as well as you can in place: applying a geographical lens to the capability approach. Soc Sci Med. 2021;288:113525 the boulevard, Langford lane, Kidlington, Oxford OX5 1GB, England: Pergamon-Elsevier Science Ltd.
Negron-Poblete P, et Lord S. Outil MAPPA (Marchabilité pour les personnes âgées). Dans Cahiers de géographie du Québec, Marchabilité des environnements urbains autour des résidences pour personnes âgées de la région de Montréal : application de l’audit MAPPA. 2014;58(164):242–3. Repéré à https://www.erudit.org/fr/revues/cgq/2014-v58-n164-cgq01924/1031168ar.pdf.
Shoval N, Auslander G, Cohen-Shalom K, Isaacson M, Landau R, Heinik J. What can we learn about the mobility of the elderly in the GPS era? J Transp Geogr. 2010;18(5):603–12.
Tokey AI. Spatial association of mobility and COVID-19 infection rate in the USA: a county-level study using mobile phone location data. J Transport Health. 2021;22:101135 the boulevard, Langford lane, Kidlington, Oxford OX5 1GB, Oxon, England: Elsevier Sci Ltd.
Portegijs E, Keskinen KE, Tuomola EM, Hinrichs T, Saajanaho M, Rantanen T. Older adults’ activity destinations before and during COVID-19 restrictions: from a variety of activities to mostly physical exercise close to home. Health Place. 2021;68:102533.
Rantanen T, Eronen J, Kauppinen M, Kokko K, Sanaslahti S, Kajan N, et al. Life-space mobility and active aging as factors underlying quality of life among older people before and during COVID-19 lockdown in Finland—a longitudinal study. J Gerontol A Biol Sci Med Sci. 2021;76(3):e60–7.
Taylor JK, Buchan IE, van der Veer SN. Assessing life-space mobility for a more holistic view on wellbeing in geriatric research and clinical practice. Aging Clin Exp Res. 2019;31(4):439–45.
Peel C, et al. Assessing mobility in older adults: the UAB Study of Aging Life-Space Assessment. Physical Therapy. 2005;85(10):1008–19.
Sayin Kasar K, Karaman E. Life in lockdown: Social isolation, loneliness and quality of life in the elderly during the COVID-19 pandemic: a scoping review. Geriatr Nurs. 2021;42(5):1222–9.
Saunders TJ, McIsaac T, Douillette K, Gaulton N, Hunter S, Rhodes RE, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S197–217.
Risser R, Haindl G, Ståhl A. Barriers to senior citizens’ outdoor mobility in Europe. Eur J Ageing. 2010;7(2):69–80.
Henning-Smith C, Moscovice I, Kozhimannil K. Differences in social isolation and its relationship to health by rurality. J Rural Health. 2019;35(4):540–9.
Haustein S, Siren A. Older people’s mobility: segments, factors. Trends Transport Rev. 2015;35(4):466–87.
Adlakha D, Krishna M, Woolrych R, Ellis G. Neighbourhood supports for active ageing in Urban India. Psychol Dev Soc. 2020;32(2):254–77.
Elsawahli H, Ahmad F, Shah AA. New urbanism design principles and young elderly active lifestyle: an analysis of TTDI neighbourhood in Kuala Lumpur, Malaysia. Urban Design Int. 2014;19(4):249–58.
Nelson A, Powell-Cope G, Gavin-Dreschnack D, Quigley P, Bulat T, Baptiste AS, et al. Technology to promote safe mobility in the elderly. Nurs Clin North Am. 2004;39(3):649–71.
Kato K, Yoshimi T, Tsuchimoto S, Mizuguchi N, Aimoto K, Itoh N, et al. Identification of care tasks for the use of wearable transfer support robots – an observational study at nursing facilities using robots on a daily basis. BMC Health Serv Res. 2021;21(1):652.
Reyer M, Fina S, Siedentop S, Schlicht W. Walkability is only part of the story: walking for transportation in Stuttgart, Germany. IJERPH. 2014;11(6):5849–65.
Acknowledgements
This work and the contributions were supported by the Czech Science Foundation, grant number 21-22276S “Accessibility modelling for seniors, perception of accessibility and determinants of their spatial mobility”.
Disclosure of potential conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Code availability (software application or custom code)
There is no code available for free.
Research involving human participants and/or animals
Not applicable.
Funding
This research was funded by the Czech Science Foundation, grant number 21-22276S “Accessibility modelling for seniors, perception of accessibility and determinants of their spatial mobility”.
Author information
Authors and Affiliations
Contributions
Conceptualization, PM, JH, OK and AS; data curation, OK, RM, NAAB, and OK; formal analysis, RM, NAAB, JH, MJ, LV, ZT; methodology, AS, PM, JH and MJ; software, OK, RM; validation, JH, PM, OK, ZT, MJ, LV; visualization, RM, OK and NAAB; writing—original draft, PM, OK, RM, NAAB and JH; writing—review & editing, AS, JH, PM, OK. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure A1.
Sunburst chart on most recent keywords and most cited keyword. Table A1. Keywords with the highest Total Link Strength (TLS) to the keyword ‘mobility’ in Web of Science. Table A2. Keywords with the highest TLS to the keyword ‘accessibility’ in Web of Science. Table A3. Keywords with the highest TLS to the keyword ‘spatial mobility’ in Web of Science. Table A4. Keywords with the highest TLS to ‘mobility’ in Scopus. Table A5. Keywords with the highest TLS to ‘spatial analysis’ in Scopus.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Maresova, P., Krejcar, O., Maskuriy, R. et al. Challenges and opportunity in mobility among older adults – key determinant identification. BMC Geriatr 23, 447 (2023). https://doi.org/10.1186/s12877-023-04106-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04106-7