
Abstract
Aims
To investigate the association between the triglyceride glucose (TyG) index and all-cause and cause-specific mortality in middle age and elderly population.
Methods and results
A total of 9,254 participants with age ≥ 45 years were enrolled from the National Health and Nutrition Examination Survey cycle of 1999–2014. The TyG index was determined as ln [fasting triglycerides (mg/dL) x fasting glucose (mg/dL)/2]. Primary outcomes were all-cause mortality and cause-specific mortality (cardiovascular diseases and malignant neoplasms). The association between the levels of TyG and the risk of mortality was explored with Cox regression models. After a median follow-up of 7.6 years, 1,774 all-cause death occurred. Univariate analysis showed that the TyG was associated with all-cause mortality (hazard ratio [HR] 1.18, 95% confidence interval [CI] [1.11,1.26]; p < 0.001). Furthermore, multivariate-adjusted analysis found that the third TyG quartile (8.72 ~ 9.16) was associated with the lowest risk of all-cause mortality (HR 0.84, 95%CI [0.73, 0.98]; p < 0.05). Restricted cubic splines showed that the association between levels of TyG index and the risk of all-cause mortality was non-linear (p for nonlinearity < 0.001) and the inflection point was 9.18 using threshold effect analysis. The HR was 0.82 (95%CI [0.71,0.96]) below 9.18 while the HR was 1.32 (95%CI [1.12,1.55]) above 9.18.
Conclusion
TyG index was U-shaped associated with all-cause mortality and the TyG index associated with the lowest risk of all-cause mortality was 9.18.
Similar content being viewed by others

Introduction
The triglyceride glucose (TyG) index has been suggested as a surrogate marker of insulin resistance [1, 2]. It was a promising biomarker for glycemic control in diabetic patients and paralleled the prevalence of metabolic syndrome and its components [3, 4].
Several studies have examined the associations between TyG index and all-cause and cause-specific mortality [5, 6]. It has been demonstrated that TyG index was an independent predictor of mortality in patients with type 2 diabetes [7], hypertension [8] and stroke [9]. Besides, the positive relationship was also seen in subclinical myocardial injury [10], ST-elevation myocardial infarction [11] and non-ST elevation acute coronary syndrome [12]. In the healthy population, elevated TyG index was associated with an increased risk of all-cause mortality and cardiovascular mortality [13]. However, it was not clear about the predictive role of TyG index on all-cause and cardiovascular mortality in middle age and elderly population.
Therefore, our study evaluated the association between the TyG index and all-cause and cause-specific mortality in middle age and elderly population based on a large representative database.
Methods
Study population
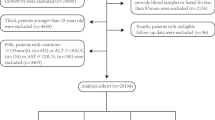
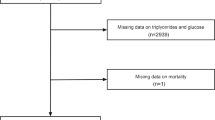
The study included individuals from the National Health and Nutrition Examination Survey (NHANES) between the periods of 1999–2014, a nationwide survey conducted by the Centers for Disease Control and Prevention in United States. Sample weight were used to estimate the representative distribution using the supplied masked variance pseudo-stratum and masked variance pseudo-primary sampling units. Details of study implementation are available for online access (https://www.cdc.gov/nchs/nhanes/index.htm). Firstly, we excluded participants with missing data on triglyceride and glycose (n = 56,983) and participants with age < 45 years old (n = 14,930). In addition, we excluded those having cancer and pregnancy (n = 2), as well as unavailable mortality status (n = 1531). In total, 9,254 participants were enrolled in our study. Figure 1 depicted the selection process. Written informed consent was acquired from each participant and the protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention.

The flow chart of participant selection
Exposure variable and outcomes
TyG index was calculated as ln [fasting triglycerides (mg/dL) x fasting glucose (mg/dL)/2] [14]. There was a median follow-up of 7.6 years. The primary outcome was all-cause mortality while the secondary outcomes included death from cardiovascular disease and malignant neoplasms. Mortality status was obtained by linkage to the National Death Index by 31 December 2015. Cardiovascular disease was defined as ICD-10 codes I00-I09, I11, I13, or I20-I51. Malignant neoplasm was defined as ICD-10 codes C00-C97 [15].
Covariates collection
Information on age, sex, race, education level, poverty income ratio (PIR), smoking status, alcohol habit, activity habits, comorbid illness (hypertension [HBP], diabetes mellites [DM] and cardiovascular diseases [CVD], chronic obstructive pulmonary disease [COPD] and liver diseases) and medication use (hypoglycemic drug and lipid-lowering drug) were collected by using standardized questionnaires. Low density lipoprotein (LDL) and creatinine were measured by standard biochemistry assays. The height and weight of each participant were obtained from the physical examinations. Body mass index (BMI, kg/m2) was calculated as weight divided by height squared. Race/ethnicity was classified as non-Hispanic white, non-Hispanic black, Mexican American or other race. Education level was categorized as less than high school, high school or equivalent and college or above. PIR was categorized as < 1, 1–3, and > 3. Smoking status were defined as current, past and never. Activity habits was categorized as vigorous, moderate and inactive. The estimated glomerular filtration rate (eGFR) was calculated according to the Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) equation. HBP was defined as the self-report hypertension, or systolic blood pressure ≥ 140 mmHg, or diastolic blood pressure ≥ 90 mmHg, or taking antihypertensive drugs. Diabetes was defined as a history of diabetes or fasting glucose > 7 mmol/L or glycated hemoglobin A1c > 6.5% or use of hypoglycemic medication. Multiple imputation was performed for covariates with missing values.
Statistical analysis
Data are presented as mean ± SD or number (proportions). Differences among different TyG groups were explored by one-way analysis of variance and Chi-square test. Associations between TyG index and the risk of all-cause and specific-cause mortality were estimated by multivariate Cox regression models. The reference category f was the lowest TyG quartile. Model 1 was unadjusted. Model 2 was adjusted for age, gender, and race. Model 3 was adjusted for age, gender, race, education, PIR, BMI, smoker, drinking, physical activity, HBP, DM, CVD, hypoglycemic drug, lipid-lowering drug, LDL, and eGFR. The dose–response association was evaluated on a continuous scale with restricted cubic spline curves. If nonlinearity was detected, a two-piecewise Cox regression model was utilized to calculated the inflection point. All analysis were performed using R version 3.6. All P values were two-sided with a significance level of < 0.05.
Results
The present study included 9,254 participants with a median 7.6-year-of follow-up. The baseline characteristics of the study population according to TyG quartile were shown in the Table 1. There were significant differences between TyG quartiles, except for drinking status and eGFR. Participants with a higher TyG index tended to have a higher BMI and more percentage of smokers, as well as more percentage of comorbidities. In addition, there were more presence of all-cause mortality and cardiovascular mortality in a higher TyG group.
The Kaplan–Meier analysis was performed to explore the prognostic effect of TyG index on all-cause mortality (Fig. 2A), cardiovascular mortality (Fig. 2B) and cancer mortality (Fig. 2C). As shown, a higher TyG index was only associated with a higher risk of all-cause mortality (p for log-rank < 0.001).

The Kaplan–Meier analysis of the prognostic effect of TyG index on all-cause mortality (A), cardiovascular mortality (B) and cancer mortality (C). TyGcat represented the quartiles of TyG index. The unit of time was Month
As shown in Table 2, we constructed three models for analyzing the independent role of TyG index in mortality. When compared with the lowest quartile, the highest quartile of TyG increased the risk of all-cause mortality (HR 1.30, 95% CI [1.13, 1.48]; p < 0.001). Per 1-unit increasement of TyG was associated with 1.18-fold higher risk of mortality (HR 1.18, 95% CI [1.11, 1.26]; p < 0.001). However, after adjusted for all covariates, TyG index was not related to all-cause mortality. However, we observed a significant association between the third quartile of TyG index with all-cause mortality (HR 0.84, 95%CI [0.73, 0.98]; p < 0.05). In addition, a second quartile of TyG was associated with the lowest risk of cardiovascular mortality (HR 0.62, 95%CI [0.43, 0.88]; p < 0.01). However, no association between TyG quartile and cancer mortality was observed.
Restricted cubic spline regressions (Fig. 3A, B&C) suggested that TyG index was only nonlinearly associated with the risk of all-cause mortality (p for nonlinearity < 0.001). What’s more, we used two-piecewise Cox regression to determine the inflection point. As shown (Fig. 4& Table 3), the TyG index associated with the lowest risk of all-cause mortality was 9.18 and below 9.18, TyG index was negative associated with all-cause mortality (HR 0.82, 95%CI [0.71,0.96]) while above 9.18, TyG index was positively associated with all-cause mortality (HR 1.32, 95%CI [1.12,1.55]).

The restricted cubic regression between TyG index with all-cause mortality (A), cardiovascular mortality (B) and cancer mortality (C) in the fully adjusted model

Threshold effect analysis of TyG on all-cause mortality using two piecewise Cox regression models
Discussion
In this study, we found TyG index was U-shaped associated with the risk of all-cause mortality after adjusting for traditional risk factors of mortality. And the TyG index with the lowest risk of all-cause mortality was 9.18 among middle age and elderly population. These results confirmed that TyG index could be an independent prognostic factor and have implications for the interpretation of levels of TyG in clinical practice.
TyG is usually associated with lipid and glucose metabolism disorders [16, 17], as a risk factor of cardiovascular diseases [18]. Many studies found that TyG index was an independent predictor for adverse cardiovascular events in both nondiabetic and diabetic subjects [19, 20]. Besides, based on a large cohort of older participants, Li et al. found that increased TyG index were significantly associated with an increased risk of cardiovascular diseases [21]. Our study found that TyG index ranging between 8.32 and 8.72 was associated with the lowest risk of cardiovascular mortality. These results suggested that keeping TyG under a propriate range was favorable for cardiovascular death.
A magnitude of publications reported that TyG increased the risk of all-cause mortality in patients with cardiovascular diseases and diabetes [7]. In general population [13] or hypertensive population [8], TyG index was non-linear associated with all-cause and cardiovascular mortality, and the threshold value was 9.36 for all-cause mortality. Even our univariate analysis found TyG was positively related to all-cause mortality, multivariable regression demonstrated that TyG was nonlinearly associated with the risk of mortality in general middle-age and elderly population, which was not affected by taking lipid-lowering drugs or hypoglycemic drugs. Specifically, when TyG was below 9.18, per 1-unit increasement decreased 0.82-fold risk of all-cause mortality, while TyG above 9.18, it was positively associated with the risk of all-cause mortality. This could be explained as follows. Firstly, low TG level was associated with the recurrent ischemia and the higher mortality of acute coronary syndrome[22]. Secondly, it was reported that higher TG had a potential protective role in vascular lesions. Thirdly, participants with high TyG index had more percentage of chronic illness, contributing to increased mortality. These results suggested that normalization of glucose or triglycerides under a target range was beneficial for a good prognosis.
Our study also has some limitations. Firstly, data on triglycerides and glucose were only collected once at baseline, and it was unclear whether TyG changes over time could affect the association with mortality. Secondly, the presence of chronic illness was self-reported based on questionnaires.
Conclusions
In our study, we found TyG index was U-shaped associated with lower mortality in middle age and elderly population. And TyG index associated with the lowest risk of all-cause mortality was 9.18, which could be a prognostic factor in the clinical practice.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Guerrero-Romero F, Villalobos-Molina R, Jimenez-Flores JR, Simental-Mendia LE, Mendez-Cruz R, Murguia-Romero M, Rodriguez-Moran M. Fasting Triglycerides and Glucose Index as a Diagnostic Test for Insulin Resistance in Young Adults. Arch Med Res. 2016;47(5):382–7.
Simental-Mendia LE, Rodriguez-Moran M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304.
Hameed EK. TyG index a promising biomarker for glycemic control in type 2 Diabetes Mellitus. Diabetes Metab Syndr. 2019;13(1):560–3.
Lee SH, Han K, Yang HK, Kim HS, Cho JH, Kwon HS, Park YM, Cha BY, Yoon KH. A novel criterion for identifying metabolically obese but normal weight individuals using the product of triglycerides and glucose. Nutr Diabetes. 2015;5:e149.
Kim J, Shin SJ, Kang HT. The association between triglyceride-glucose index, cardio-cerebrovascular diseases, and death in Korean adults: A retrospective study based on the NHIS-HEALS cohort. PLoS ONE. 2021;16(11):e0259212.
Zhou Y, Pan Y, Yan H, Wang Y, Li Z, Zhao X, Li H, Meng X, Wang C, Liu L, et al. Triglyceride Glucose Index and Prognosis of Patients With Ischemic Stroke. Front Neurol. 2020;11:456.
Jin JL, Sun D, Cao YX, Guo YL, Wu NQ, Zhu CG, Gao Y, Dong QT, Zhang HW, Liu G, et al. Triglyceride glucose and haemoglobin glycation index for predicting outcomes in diabetes patients with new-onset, stable coronary artery disease: a nested case-control study. Ann Med. 2018;50(7):576–86.
Zhou D, Liu XC, Kenneth L, Huang YQ, Feng YQ. A Non-Linear Association of Triglyceride Glycemic Index With Cardiovascular and All-Cause Mortality Among Patients With Hypertension. Front Cardiovasc Med. 2021;8:778038.
Zhang B, Liu L, Ruan H, Zhu Q, Yu D, Yang Y, Men X, Lu Z. Triglyceride-Glucose Index Linked to Hospital Mortality in Critically Ill Stroke: An Observational Multicentre Study on eICU Database. Front Med (Lausanne). 2020;7:591036.
Liu Y, Wu M, Xu J, Sha D, Xu B, Kang L. Association between Triglyceride and glycose (TyG) index and subclinical myocardial injury. Nutr Metab Cardiovasc Dis. 2020;30(11):2072–6.
Luo E, Wang D, Yan G, Qiao Y, Liu B, Hou J, Tang C. High triglyceride-glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc Diabetol. 2019;18(1):150.
Zhao Q, Zhang TY, Cheng YJ, Ma Y, Xu YK, Yang JQ, Zhou YJ. Impacts of triglyceride-glucose index on prognosis of patients with type 2 diabetes mellitus and non-ST-segment elevation acute coronary syndrome: results from an observational cohort study in China. Cardiovasc Diabetol. 2020;19(1):108.
Liu XC, He GD, Lo K, Huang YQ, Feng YQ. The Triglyceride-Glucose Index, an Insulin Resistance Marker, Was Non-linear Associated With All-Cause and Cardiovascular Mortality in the General Population. Front Cardiovasc Med. 2020;7:628109.
Liu Y, Chang L, Wu M, Xu B, Kang L: Triglyceride Glucose Index Was Associated With the Risk of Peripheral Artery Disease. Angiology. 2022:33197211070644.
Chen Z, He J, Chen C, Lu Q. Association of Total Bilirubin With All-Cause and Cardiovascular Mortality in the General Population. Front Cardiovasc Med. 2021;8:670768.
Su WY, Chen SC, Huang YT, Huang JC, Wu PY, Hsu WH, Lee MY. Comparison of the Effects of Fasting Glucose, Hemoglobin A1c, and Triglyceride-Glucose Index on Cardiovascular Events in Type 2 Diabetes Mellitus. Nutrients. 2019;11(11):2838.
Sanchez-Inigo L, Navarro-Gonzalez D, Pastrana-Delgado J, Fernandez-Montero A, Martinez JA. Association of triglycerides and new lipid markers with the incidence of hypertension in a Spanish cohort. J Hypertens. 2016;34(7):1257–65.
Nam KW, Kwon HM, Jeong HY, Park JH, Kwon H, Jeong SM. High triglyceride-glucose index is associated with subclinical cerebral small vessel disease in a healthy population: a cross-sectional study. Cardiovasc Diabetol. 2020;19(1):53.
Zhao Q, Zhang TY, Cheng YJ, Ma Y, Xu YK, Yang JQ, Zhou YJ: Triglyceride-Glucose Index as a Surrogate Marker of Insulin Resistance for Predicting Cardiovascular Outcomes in Nondiabetic Patients with Non-ST-Segment Elevation Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. J Atheroscler Thromb. 2020; 28(11):1175–94.
Ma X, Dong L, Shao Q, Cheng Y, Lv S, Sun Y, Shen H, Wang Z, Zhou Y, Liu X. Triglyceride glucose index for predicting cardiovascular outcomes after percutaneous coronary intervention in patients with type 2 diabetes mellitus and acute coronary syndrome. Cardiovasc Diabetol. 2020;19(1):31.
Li S, Guo B, Chen H, Shi Z, Li Y, Tian Q, Shi S. The role of the triglyceride (triacylglycerol) glucose index in the development of cardiovascular events: a retrospective cohort analysis. Sci Rep. 2019;9(1):7320.
Cheng KH, Chu CS, Lin TH, Lee KT, Sheu SH, Lai WT. Lipid paradox in acute myocardial infarction-the association with 30-day in-hospital mortality. Crit Care Med. 2015;43(6):1255–64.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
S M made the statistical analysis; G HX wrote the original manuscript; M DC and W Y designed the study. All authors approved it.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants provided written informed consent and the protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention. All methods were carried out in accordance with Helsinki regulations.
Consent for publication
Not applicable.
Competing interests
The authors have nothing to disclose regarding conflict of interest with respect to this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sun, M., Guo, H., Wang, Y. et al. Association of triglyceride glucose index with all-cause and cause-specific mortality among middle age and elderly US population. BMC Geriatr 22, 461 (2022). https://doi.org/10.1186/s12877-022-03155-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03155-8