
Abstract
Introduction
The Indian population is rapidly aging with huge proportion of illiterate and socioeconomically disadvantaged people and there is a dearth of research on the relationships between factors of socioeconomic vulnerability and frailty in older people. The present study examined the cross-sectional associations between socioeconomic vulnerability and physical frailty in community-dwelling older individuals in India.
Materials and methods
The data for the study were obtained from the Longitudinal Aging Study in India (LASI), which was conducted in 2017–18. The effective sample size was 14,652 older males and 15,899 older females aged 60 and over. The outcome variable was physical frailty phenotype measured from exhaustion, unintentional weight loss, weak grip strength, low physical activity, and slow walking time. The main explanatory variable was vulnerability status based on education, wealth and caste. The study carried out bivariate analysis to observe the association between vulnerability status and physical frailty. Further, multivariable binary logistic regression analysis was conducted to fulfil the objective of the study.
Results
A proportion of 10.5 and 14.4% of older males and females respectively were in the overall vulnerable category. The prevalence of physical frailty was high among older males from vulnerable population (31.4% vs 26.9%; p < 0.001). The adjusted estimates from multivariate analysis revealed that older adults from vulnerable category had 14% significantly higher odds of being frail in comparison to non-vulnerable category [AOR: 1.14; CI: 1.06,1.24]. The adjusted model further revealed that there were no significant gender differentials in physical frailty among older adults. Model-3 (adjusted model) revealed that older males and females from vulnerable population had 18% [AOR: 1.18; CI: 1.04,1.34] and 8% [AOR: 1.08; CI: 1.01,1.21] significantly higher odds of being physically frail in comparison to older males from non-vulnerable population respectively.
Conclusions
Adverse socioeconomic circumstances such as low education, lower wealth and caste status that are associated with increased prevalence of physical frailty raise urgent questions both for public health practitioners and clinicians. The current findings may help to adapt public policies focusing on screening physical frailty in the clinical settings, especially among vulnerable populations as a marker of a possibly reversible vulnerability to adverse outcomes in old age.
Similar content being viewed by others

Background
The rapid growth in proportion of older population has affected the healthcare settings worldwide and increased the need for developing long-term care services. Aging is often associated with accumulation of chronic conditions which in turn lead to disability among older adults [1,2,3]. Similarly, poor socioeconomic status may affect the individuals’ disease diagnosis, treatment adherence, resilience and physiological reserves [4,5,6].
Physical frailty phenotype among community-dwelling older adults, developed by Fried and colleagues refers to a clinical syndrome in which three or more of the following are present; exhaustion, weak grip strength, slow walk, low physical activity and unintentional weight loss [7, 8]. On the other hand, unlike physical frailty, vulnerability refers to social and environmental components affecting individuals’ wellbeing; including economic circumstances which themselves are recognized as determinants of health. However, physically frail individuals are vulnerable and environmental factors are more likely to increase their level of frailty and to have an independent effect on their level of vulnerability [9], suggesting a bidirectional linkage. Meanwhile, the influence of factors such as socioeconomic status in older age on increasing the risk of physical frailty is much debated among geriatric researchers [10].
Some of the earlier studies on physical frailty have demonstrated the social and environmental determinants of frailty including income, social participation and occupation [10, 11]. Studies showed that a holistic social vulnerability index in older adults including social factors from various domains of social support, social engagement and socioeconomic status (SES) predicts both cognitive decline and mortality [12, 13]. The increased mortality risk due to social vulnerability has also been observed among fittest older adults in a community setting reporting 0–1 out of 31 self-reported health deficits [14]. A couple of studies found that increasing social vulnerability, as measured by an index was associated with increased mortality and decreased survival rate in older adults [13,14,15], and other populations [16]. On the other hand, a study in China found physical frailty as a stronger predictor of mortality among higher socioeconomic groups than those with low SES [17].
Researchers have suggested that considering several indicators of SES such as income and education, the importance of which may diminish at older ages, some factors such as household wealth status, personal assets and social statuses remain important in assessing the status of older people [18,19,20]. Previous findings have also contributed to discussion of how to best measure SES in older age, where income, education and occupational status, may have more limited importance due to several old age pension schemes, changes in educational norms and retirement [21]. Besides, studies in India suggest that several socio-cultural and contextual factors such as social class and caste categories may also affect the health and wellbeing of older population, especially women [22,23,24]. Thus, we have broadened our consideration of social and economic vulnerability factors in the current study to create a more holistic representation of socioeconomic circumstances in Indian context by including caste status of individuals along with education and wealth status.
The need for an early care of physical frailty has been recently emphasised since it has an impact on patients, caregivers, healthcare professionals, and on society as a whole [25]. Although research on genetic and biological aspects of frailty is burgeoning, studies on the possible associations between factors of socioeconomic vulnerability and frailty are scarce. This is particularly important in India, as the population is rapidly aging with greater illiteracy and socioeconomic disadvantages. Thus, the objective of this study was to examine the relationship between socioeconomic vulnerability and frailty in community-dwelling older individuals in India. The study hypothesised that older adults who are socioeconomically vulnerable are more likely to be physically frail in India.
Materials and methods
Data
The data for this study came from the Longitudinal Aging Study in India (LASI), which was conducted in 2017–18. The Harvard T.H. Chan School of Public Health, the International Institute for Population Sciences (IIPS), and the University of Southern California (USC) collaborated on the study. The nationally representative longitudinal survey will collect crucial information on the physical, social, and cognitive well-being of India’s older citizens over a 25-year period. The LASI collected data of over 72,000 people aged 45 and over, as well as their spouses (of any age), across India’s states and union territories. The data collected were related to demographics, household economic status, chronic health conditions, symptom-based health conditions, functional health, mental health (cognition and depression), biomarkers, health insurance and healthcare utilization, family and social networks, welfare programmes, work and employment, retirement, satisfaction, and life expectations. The sample is based on a multistage stratified cluster sample design that includes three and four separate phases of rural and urban region selection. The survey gives scientific insights and allows for a standardised methodology that can be compared to other similar worldwide research. The LASI report contains information on sample design, survey instruments, fieldwork, data collecting and processing, and response rates [26]. For this investigation, the effective sample size after dropping the missing cases for physical frailty, was 14,652 older males and 15,899 older females aged 60 and over. The present study only analysed the data for older people defined as those who aged 60 years and above and hence the total sample size for the study was 30,551. The study was approved by an ethical committee of the Indian Council of Medical Research (ICMR) and was conducted in accordance with the relevant guidelines and regulations.
Variable description
Outcome variable
Frailty
The physical frail older adults was assessed using an adapted version of the frailty phenotype described by Fried and colleagues. The physical frailty phenotype consists of five components: (1) self-reported exhaustion, (2) unintentional weight loss, (3) weak grip strength, (4) self-reported low physical activity, and (5) slow walking time. (1) Exhaustion was assessed using two questions from the Center for Epidemiologic Studies Depression (CES-D) scale: in the past week, how often do you feel “everything you did was an effort,” and “feel tired or low in energy” answered with “three or more days = 1” and “less than three days = 0”. (2) Unintentional weight loss was assessed using the question: “Do you think that you have lost weight in the last 12 months because there was not enough food at your household?” with responses “Yes = 1” and “No = 0.” (3) LASI measured handgrip strength in kilograms using a handheld Smedley’s Hand Dynamometer. The final handgrip strength score (in kg) was calculated as the average score (in kg) of two successive trials in the dominant hand, and was adjusted for the gender and body mass index, as shown in Table 1. (4) In LASI, respondents were asked about their physical activity: “How often do you take part in sports or vigorous activities, such as running or jogging, swimming, going to a health center or gym, cycling, or digging with a spade or shovel, heavy lifting, chopping, farm work, fast bicycling, cycling with loads: everyday, more than once a week, once a week, one to three times a month, or hardly ever or never?” The low physical activity was defined as: “One to three times a month or hardly ever or never = 1” and “once a week or more than once a week= 0”. LASI asked respondents to walk 4-m twice, and slowness was assessed by averaging the time (in seconds) taken in completing the 4 m (stratified by gender and height), as shown in Table 1. The overall physical frailty phenotype score lies between 0 and 5. Respondents with a score of 0 were classified as “not frail,” 1–2 as “pre-frail,” and three or higher as “frail.” The outcome variable was coded as binary i.e., physically frail which include (frail and pre-frail) and not frail. Assessment of the individual domains is described in Table 1.
Explanatory variables
Main explanatory variable
Vulnerability measures
To understand multiple vulnerabilities, a variable integrating the three dimensions of vulnerability based on education, wealth, and caste was constructed as they were used in the two Human Poverty Indexes and the Multidimensional Poverty Index (instead of the caste they used health). For constructing the individual index, low education is classified as those older adults who did not complete 5 years of schooling. For education, an older adult is considered to be deprived or vulnerable if he/she reported in his/her individual survey that he/she had not completed 5 years of schooling. This cut off is chosen because people with only a few years of education have been found to have health-seeking behaviour similar to those with no education [27]. Using household consumption data, the monthly per-capita consumption expenditure (MPCE) quintile was determined. The sample households were canvassed using sets of 11 and 29 questions on food and non-food expenses, respectively. Food spending was gathered over a seven-day reference period, whereas non-food expenditure was collected over 30-day and 365-day reference periods. The 30-day reference period has been used to standardise food and non-food expenses. The MPCE is calculated and used to summarise consumption. The variable was divided into five quintiles i.e., from poorest to richest. Those who belonged to the poorest or poorer wealth quintile have been considered as economically “poor” and middle, richer, and richest are “non-poor”. For caste, an older adult is considered vulnerable if he or she belonged to the Scheduled Caste or Scheduled Tribe.
In this way, using the three dimensions of vulnerability based on education, wealth, and caste, eight categories of vulnerability were possible: education, wealth and caste; education and wealth; education and caste; wealth and caste; education only; wealth only; caste only and anyone. The first four categories classified vulnerability in multiple dimensions, the next three in one dimension and the last category in any-one [27].
Other explanatory variables
Age was recoded as young-old (60–69 years), old-old (70–79 years) and oldest-old (80+ years); living arrangement was recoded as living alone, living with spouse, living with children and living with others; marital status was recoded as currently married, widowed and others (others included divorced/ separated/ never married) [28]; work status was recoded as never worked, currently working, currently not working and retired [29]. Further, social participation was recoded as no and yes. Respondents were said to be participating in social activities if they participate in any of the following; eat out of house (Restaurant/Hotel); go to park/ beach for relaxing/ entertainment; play cards or indoor games; play out door games/ sports/ exercise/ jog/ yoga; visit relatives /friends; attend cultural performances /shows/ Cinema; attend religious functions /events such as bhajan/ satsang/ prayer; attend political/ community/ organization group meetings; read books/ newspapers/ magazines; watch television/ listen to radio and use a computer for e-mail/net surfing etc. [26].
Self-rated health was recoded as (good which includes excellent, very good, and good whereas poor includes fair and poor) [30]. The probable major depression with symptoms of dysphoria was calculated using the CIDI-SF (Short Form Composite International Diagnostic Interview). This scale estimates a probable psychiatric diagnosis of major depression and has been validated in field settings and widely used in population-based health surveys [26]. The scale was validated for older adults [31]. The respondent was considered to be depressed if the score was 3 and above in the scale of 0–10 [26, 32]. Difficulty in activities of daily living (ADL) was recoded as (no and yes). The ability or inability to perform ADLs is used to assess a person’s functional state, particularly for persons with impairments and those who are older [33]. If the respondent reported any difficulty in ADLs then difficulty in ADL was coded as yes otherwise no. Difficulty in instrumental ADL (IADL) was recoded as (no and yes). These tasks are necessary for independent functioning in the community. If the respondent reported any difficulty in IADLs then difficulty in IADL was coded as yes and otherwise no [34]. Morbidity status was categorized as 0 “no morbidity”, 1 “any one morbid condition” and 2+ “co-morbidity” [35]. Religion was recoded as Hindu, Muslim, Christian, and Others. Place of residence was recoded as (rural and urban). The regions were recoded as North, Central, East, Northeast, West, and South.
Statistical analysis
The study carried out bivariate analysis to observe the association between dependent and independent variables. Further, multivariable binary logistic regression analysis [36] was used to fulfil the objective of the study. The results were presented in the form of odds ratio (OR) with a 95% confidence interval (CI).
Model-1 provides the unadjusted estimates whereas model-2 and 3 provide the adjusted estimates (adjusted for age, living arrangement, marital status, working status, social participation, self-rated health, depression, difficulty in ADL, difficulty in IADL, morbidity status, religion and place of residence and regions of India). The unadjusted and adjusted estimates of interaction of sex and vulnerability on physical frailty are provided in model-1 and model-3, respectively [34, 37]. While analysing the interaction effects, a new categorical variable is created based on vulnerability and sex.
Results
Table 2 presents the socio-economic profile of the study participants. About 2.5% of older men and 8.6% older women were living alone. A proportion of 16.5% of older men and 53.5% of older women were widowed. About 43.1% of older men and 19.2% older women were currently working. Also, 7.4 and 9.7% of older men and women respectively had no social participation. A proportion of 46.7 and 50.2% of older men and women had poor self-rated health respectively. Nearly 7.5% of older men and 9.7% of older women were suffering from depression. Similarly, 20.1 and 38.0% of older men and 25.4 and 56.2% of older women had difficulty in ADL and IADL respectively. And, 22.1 and 25.3% of older men and women had two or more morbidities.
Table 3 presents the percentage of older men and women by various vulnerabilities and their combinations. It was found that 10.5 and 14.5% of older men and women were in the overall vulnerable category respectively. Additionally, 73.1 and 87.3% of older men and women were from any one vulnerable category respectively.
Table 4 presents the percentage distribution of physical frailty among older men and women by their background characteristics. It was revealed that the prevalence of physical frailty was high among older men with vulnerability status (31.4% vs 26.9%); however, in case of older women, the prevalence was slightly high in those with vulnerability status (32.7% vs 32.1%). Additionally, it was found that there were significant gender differentials (differences: 4.8%; p < 0.001) in physical frailty among older adults. The prevalence of physical frailty was higher among older men and women in the higher age group, those with no social participation, with poor health outcomes such as depression, poor self-rated health and difficulty in functional health and those residing in rural areas of the country. Higher percentage of older male and female from Muslim religion were physically frail. The prevalence of frailty was high among older male and females from rural areas. Also, the older adults from eastern part of India had higher prevalence of frailty.
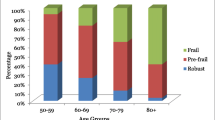
Figure 1 presents the percentage of physical frailty among older males and females with respective vulnerability status. It was found that vulnerable older females had high prevalence of frailty in all categories in reference to older males. Table S1 presents the percentage prevalence of each components of physical frailty by various vulnerabilities stratified by sex (supplementary file).

Percentage prevalence of physical frailty among older males and females by various vulnerabilities
Table 5 presents the logistic regression estimates of physical frailty among older adults by their background characteristics. Model-1 revealed that the vulnerable older adults had 8% significantly higher odds of being frail in comparison to non-vulnerable older adults [UOR: 1.08; CI: 1.01, 1.16]. Moreover, the same model revealed that older females had 32% significantly higher odds of being frail in reference to older males [UOR: 1.32; CI: 1.26,1.39]. It was further found that the odds of frailty were significantly high among older females from vulnerable category in comparison to older males from non-vulnerable category [UOR: 1.34; CI: 1.27,1.46].
Model-2 which represents the adjusted estimates revealed that older adults from vulnerable category had 14% significantly higher odds of being physically frail in reference to non-vulnerable category [AOR: 1.14; CI: 1.06,1.24]. The adjusted model further revealed that there were no significant gender differentials in physical frailty among older adults. Model-3 (adjusted model) revealed that older males and females from vulnerable category had 18% [AOR: 1.18; CI: 1.04,1.34] and 8% [AOR: 1.08; CI: 1.01,1.21] significantly higher odds of being physically frail in comparison to older males from non-vulnerable category respectively.
Discussion
This population-based cross-sectional study depicted the vulnerability factors that are associated with frailty in older adults. The higher prevalence of physical frailty, with 27.4% older men and 32.2% older women being physically frail suggests that frailty in community-dwelling older Indian adults is common and needs to be prioritized in policy formation for geriatric population. This is consistent with previous studies that concluded that irrespective of definitions of frailty, the prevalence is higher in India compared to other low and middle income countries [38, 39]. In this regard, future studies on urban-rural and regional variations of old age frailty in India are warranted. Although increasing age is a risk factor for physical frailty, not all the older people are frail which suggests for further investigation on reasons other than normal aging process to augment this condition in aged population. We found that among older Indian adults, those with greater vulnerability were more likely to be frail in comparison to those with no social vulnerability. The risk for being frail was especially higher among older women who are more vulnerable than older men with same vulnerability status.
The most evident reason for older adults who are socioeconomically advantaged turning to be less frail than those who are disadvantaged is their potential for prevention suggested by a spontaneous reversibility of frailty in individuals in their early stages of frailty. Factors such as availability of resources, increased access to healthcare and health literacy among high economic groups in India which help older adults detect their disability and diseases earlier and prevent from further accumulation of such conditions are supportive of this argument [40, 41]. However, this potential in wealthy and higher social groups is challenged by the lack of specific public interventions of proven effectiveness and efficacy in socioeconomically poor frail individuals [42]. This may be substantiated by studies on the association of lack of social resources among the poor people with their functional decline in old age [43]. The previous findings in India suggesting that rural populations are disproportionately affected by poor health outcomes due to barriers to diagnosis also suggest their increased vulnerability to physical frailty in old age [44].
The female disadvantage in physical frailty prevalence observed in our study is consistent with other research in developing countries. Several cross-sectional and longitudinal studies in China found that the prevalence and incidence of physical frailty was significantly higher in women [45, 46]. In comparison to China, treatment levels of various chronic diseases were lower in India and women in particular [47], which might also have worsened the physical frailty status of vulnerable older Indian female population. Similarly, studies in low- and middle income countries observed that differential exposure and differential vulnerability to social conditions and biological factors in men and women are associated with gender differences in physical functioning and mental health status in older ages [48,49,50,51]. However, the interaction of sex and vulnerability on physical frailty revealed that older men who are socioeconomically vulnerable are more likely to be physically frail than women who are vulnerable after adjusting for several confounders. This suggests that several health-related variables might have led to increased physical frailty in women, whereas; a poor SES results in higher risk of physical frailty in men.
Studies in various settings have revealed a marked educational gradient in frailty, where older individuals with no formal education or little education showed greater odds of physical frailty than their counterparts with higher education [49, 52, 53]. Several studies in India also found lower levels of disability and physical frailty among older adults with higher levels of education and wealth [38, 54,55,56,57,58]. This low education- frailty association consistently found in the current study, can be attributed to the increased material, health and behavioural resources available to those who are highly educated [49, 59, 60].
With regard to the prevalence of physical frailty among different ethnic groups, the findings are inconclusive. Some studies among Mexican Americans and European Americans showed higher prevalence in ethnic minorities [61, 62], whereas several studies have shown that African-American race in comparison to white races was independently associated with frailty [63, 64]. This suggests that higher prevalence of frailty among vulnerable ethnic groups in India (Scheduled Castes and Scheduled Tribes) requires future investigation. Furthermore, frailty prevalence differs between the regions, mainly because of great regional disparities in health care, which are related to socioeconomic characteristics [65]. This is substantiated by findings of other studies showing that rural residents in India who have low income and educational levels and less access to health services and insurance, which lead to poorer health are at increased risk of becoming physically frail [38].
This study has several limitations that should be addressed in the studies in future. First, our study was cross-sectional in design, and thus the direction of causality could not be ascertained. It is possible that frailty in old age may accelerate the vulnerability, for example, frail older adults being economically poor. It is also possible that frail older adults are less likely to participate in social activity, which is associated which in turn increase their vulnerability to frailty, suggesting the other pathways which are not considered in the current study. These mechanisms therefore warrant further investigation to determine what other factors may account for the unexplained variance between vulnerability factors and physical frailty in older individuals. Future studies with follow-up rounds of LASI survey also should be conducted to better understand the aspect by exploring other vulnerability factors.
Conclusion
The findings highlight the higher prevalence of physical frailty among community-dwelling older adults and among those who had lower educational, wealth or caste status or a combination of these factors. Adverse socioeconomic circumstances that are associated with increased prevalence of physical frailty raise urgent questions both for public health practitioners and clinicians. The current findings may help to adapt public policies focusing on screening physical frailty in the clinical settings, especially among vulnerable populations as a marker of a possibly reversible vulnerability to adverse outcomes in old age. Also, the observed relationships between several socioeconomic factors as determinants of adverse late-life physical frailty need further research.
References
Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385:549–62.
Quiñones AR, Markwardt S, Botoseneanu A. Multimorbidity combinations and disability in older adults. J Gerontol Ser A Biol Sci Med Sci. 2016;71:823–30.
Calderón-Larrañaga A, Santoni G, Wang HX, et al. Rapidly developing multimorbidity and disability in older adults: does social background matter? J Intern Med. 2018;283:489–99.
Cesari M, De Carvalho IA, Thiyagarajan JA, et al. Evidence for the domains supporting the construct of intrinsic capacity. J Gerontol Ser A Biol Sci Med Sci. 2018;73:1653–60.
Rogers SE, Thrasher AD, Miao Y, et al. Discrimination in healthcare settings is associated with disability in older adults: health and retirement study, 2008–2012. J Gen Intern Med. 2015;30:1413–20.
Arokiasamy P, Uttamacharya KP, et al. Chronic noncommunicable diseases in 6 low- and middle-income countries: findings from wave 1 of the world health organization’s study on global Ageing and adult health (SAGE). Am J Epidemiol. 2017;185:414–28.
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol Ser A Biol Sci Med Sci. 2001;56:146–57.
Clegg A, Young J, Iliffe S, et al. Frailty in elderly people. Lancet. 2013;381:752–62.
Santos-Eggimann B, Sirven N. Screening for frailty: older populations and older individuals. Public Health Rev. 2016;37:1–16.
Woo J, Goggins W, Sham A, et al. Social determinants of frailty. Gerontology. 2005;51:402–8.
Woods NF, LaCroix AZ, Gray SL, et al. Frailty: emergence and consequences in women aged 65 and older in the Women’s health initiative observational study. J Am Geriatr Soc. 2005;53:1321–30.
Andrew MK, Rockwood K. Social vulnerability predicts cognitive decline in a prospective cohort of older Canadians. Alzheimer’s Dement. 2010;6:319–325.e1.
Andrew MK, Mitnitski AB, Rockwood K. Social vulnerability, frailty and mortality in elderly people. PLoS One. 2008;3:1–8.
Andrew MK, Mitnitski A, Kirkland SA, et al. The impact of social vulnerability on the survival of the fittest older adults. Age Ageing. 2012;41:161–5.
Schofield MJ, Powers JR, Loxton D. Mortality and disability outcomes of self-reported elder abuse: a 12-year prospective investigation. J Am Geriatr Soc. 2013;61:679–85.
Mishra PS, Sinha D, Kumar P, et al. Linkages of multi-dimensional vulnerabilities with infant and child mortality rates in India and its specific regions: are social determinants of health still relevant? Omega (United States). Epub ahead of print; 2021. https://doi.org/10.1177/0030222821997704.
Gu D, Yang F, Sautter J. Socioeconomic status as a moderator between frailty and mortality at old ages. BMC Geriatr. 2016;16:17–9.
Assari S. Socioeconomic status and self-rated oral health; diminished return among hispanic whites. Dent J. 2018;6:1–12.
Smith K, Goldman N. Socioeconomic differences in health among older adults in Mexico. Soc Sci Med. 2007;65:1372–85.
Roy K, Chaudhuri A. Influence of socioeconomic status, wealth and financial empowerment on gender differences in health and healthcare utilization in later life: evidence from India. Soc Sci Med. 2008;66:1951–62.
Von Dem Knesebeck O, Lüschen G, Cockerham WC, et al. Socioeconomic status and health among the aged in the United States and Germany: a comparative cross-sectional study. Soc Sci Med. 2003;57:1643–52.
Jensen R. Caste, culture, and the status and well-being of widows in India: Analyses in the Economics of Aging; 2013. p. 357–76.
Perkins JM, Lee H, James KS, et al. Marital status, widowhood duration, gender and health outcomes: a cross-sectional study among older adults in India. BMC Public Health. 2016;16:1032.
Subramanian SV, Nandy S, Irving M, Gordon D, Davey Smith G. Role of socioeconomic markers and state prohibition policy in predicting alcohol consumption among men and women in India: a multilevel statistical analysis. Bull World Health Organ. 2005;83(11):829-36. Epub 2005 Nov 10.
Subramaniam A, Tiruvoipati R, Green C, et al. Frailty status, timely goals of care documentation and clinical outcomes in older hospitalised medical patients. Intern Med J. 2020. https://doi.org/10.1111/imj.15032 Epub ahead of print.
International Institute for Population Sciences (IIPS), National Programme for Health Care of Elderly (NPHCE), MoHFW, Harvard T. H. Chan School of Public Health (HSPH) and the University of Southern California (USC) 2020. Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18, India Report, International Institute for Population Sciences, Mumbai.
Mohanty SK. Multiple deprivations and maternal care in India. Int Perspect Sex Reprod Health. 2012;38:6–14.
Srivastava S, Sulaiman K, Drishti D, et al. Factors associated with psychiatric disorders and treatment seeking behaviour among older adults in India. Sci Rep. 2021;11:1–14.
Muhammad T, Sulaiman K, Srivastava S. Migration of adult male children and associated depression among community-dwelling older parents: A cross-sectional gender analysis from LASI, 2017–18. Int J Geriatr Psychiatry. 2021. https://doi.org/10.1002/gps.5675 Epub ahead of print.
Muhammad T, Srivastava S. Tooth loss and associated self-rated health and psychological and subjective wellbeing among community-dwelling older adults: A cross-sectional study in India. BMC Public Health. 2022;22:7. https://doi.org/10.1186/s12889-021-12457-2.
Kessler RC, Üstün BB. The World Mental Health (WMH) Survey Initiative version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). Int J MethodsPsychiatr Res. 2004. https://doi.org/10.1002/mpr.168 Epub ahead of print.
Muhammad T, Meher T. Association of late-life depression with cognitive impairment: evidence from a cross-sectional study among older adults in India. BMC Geriatr. 2021;21:1–13.
Muhammad T, Srivastava S. Why Rotational Living Is Bad for Older Adults ? Evidence from a Cross- Sectional Study in India. J Popul Ageing. 2020;1. https://doi.org/10.1007/s12062-020-09312-4 Epub ahead of print.
Srivastava S, Muhammad T. Violence and associated health outcomes among older adults in India: a gendered perspective. SSM Popul Heal. 2020;12. https://doi.org/10.1016/j.ssmph.2020.100702 Epub ahead of print 1.
Keetile M, Navaneetham K, Letamo G. Prevalence and correlates of multimorbidity among adults in Botswana: a cross-sectional study. Plos One. 2020. https://doi.org/10.1371/journal.pone.0239334 Epub ahead of print.
Osborne J, King JE. Binary logistic regression. In: Best Practices in Quantitative Methods: SAGE Publications, Inc.; 2011. p. 358–84.
Chauhan S, Srivastava S, Kumar P, Patel R, Preeti Dhillon MT. Interaction of substance use with physical activity and its effect on depressive symptoms among adolescents. J Substance Use. 2021;26(5):524-30. https://doi.org/10.1080/14659891.2020.1851411
Kendhapedi KK, Devasenapathy N. Prevalence and factors associated with frailty among community-dwelling older people in rural Thanjavur district of South India: a cross-sectional study. BMJ Open. 2019;9. https://doi.org/10.1136/bmjopen-2019-032904 Epub ahead of print.
Siriwardhana DD, Hardoon S, Rait G, et al. Prevalence of frailty and prefrailty among community-dwelling older adults in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Open. 2018;8:1–18.
BRK S. Multidimensional Approach to Quality of Life Issues: A Spatial Analysis; 2019. https://doi.org/10.1007/978-981-13-6958-2. Epub ahead of print 2019
Bose M, Dutta A. Health financing strategies to reduce out-of-pocket burden in India: a comparative study of three states. BMC Health Serv Res. 2018;18:1–10.
Gordon AL, Masud T, Gladman JRF. Now that we have a definition for physical frailty, what shape should frailty medicine take? Age Ageing. 2014;43:8–9.
Cappelli M, Bordonali A, Giannotti C, et al. Social vulnerability underlying disability amongst older adults: a systematic review. Eur J Clin Investig. 2020;50:1–12.
Basu S, King AC. Disability and chronic disease among older adults in India: detecting vulnerable populations through the WHO SAGE study. Am J Epidemiol. 2013;178:1620–8.
Zheng Z, Guan S, Ding H, et al. Prevalence and incidence of frailty in community-dwelling older people: Beijing longitudinal study of aging II. J Am Geriatr Soc. 2016;64:1281–6.
Ma L, Tang Z, Zhang L, et al. Prevalence of frailty and associated factors in the community-dwelling population of China. J Am Geriatr Soc. 2018;66:559–64.
Kowal P, Williams S, Jiang Y, et al. Aging, Health, and Chronic Conditions in China and India: Results from the Multinational Study on Global AGEing and Adult Health (SAGE). In: Smith J, Majmundar M, editors. National Research Council (US) Panel on Policy Research and Data Needs to Meet the Challenge of Aging in Asia; 2012. p. 415–37.
Alvarado BE, Zunzunegui MV, Béland F, et al. Social and gender inequalities in depressive symptoms among urban older adults of Latin America and the Caribbean. J Gerontol Ser B Psychol Sci Soc Sci. 2007;62:226–37.
Alvarado BE, Zunzunegui MV, Béland F, et al. Life course social and health conditions linked to frailty in latin american older men and women. J Gerontol Ser A Biol Sci Med Sci. 2008;63:1399–406.
Kaneda T, Zimmer Z, Fang X, et al. Gender differences in functional health and mortality among the Chinese elderly: testing an exposure versus vulnerability hypothesis. Res Aging. 2009;31:361–88.
Muhammad T, Maurya P. Gender differences in the association between perceived income sufficiency and self-rated health among older adults: a population-based study in India. J Women Aging. 2021;00:1–14.
Etman A, Burdorf A, Van der Cammen TJM, et al. Socio-demographic determinants of worsening in frailty among community-dwelling older people in 11 European countries. J Epidemiol Commun Health. 2012;66:1116–21.
Szanton SL, Seplaki CL, Thorpe RJ, et al. Socioeconomic status is associated with frailty: the Women’s health and aging studies. J Epidemiol Commun Health. 2010;64:63–7.
Biritwum RB, Minicuci N, Yawson AE, et al. Prevalence of and factors associated with frailty and disability in older adults from China, Ghana, India, Mexico, Russia and South Africa. Maturitas. 2016;91:8–18.
Nagarkar A, Kashikar Y. Predictors of functional disability with focus on activities of daily living: a community based follow-up study in older adults in India. Arch Gerontol Geriatr. 2017;69:151–5.
Kashikar Y, Nagarkar A. Prevalence and determinants of frailty in older adults in India. Indian J Gerontol. 2012;9:365–82.
Chaudhary M, Chowdhary R. Age and socioeconomic gradients in frailty among older adults in India. J Public Heal. 2019;27:675–85.
Shalini T, Chitra PS, Kumar BN, et al. Frailty and Nutritional Status among Urban Older Adults in South India. J Aging Res. 2020. https://doi.org/10.1155/2020/8763413 Epub ahead of print 2020.
Hoogendijk E, Groenou MB, Tilburg T, et al. Educational differences in functional limitations: comparisons of 55-65-year-olds in the Netherlands in 1992 and 2002. Int J Public Health. 2008;53:281–9.
Hoogendijk EO, van Hout HPJ, Heymans MW, et al. Explaining the association between educational level and frailty in older adults: results from a 13-year longitudinal study in the Netherlands. Ann Epidemiol. 2014;24:538–44.
Espinoza SE, Hazuda HP. Frailty in older Mexican-American and European-American adults: is there an ethnic disparity? J Am Geriatr Soc. 2008;56:1744–9.
Espinoza SE, Jung I, Hazuda H. Lower frailty incidence among Mexican American than among European American older adults: the San Antonio longitudinal study of aging. J Am Geriatr Soc. 2010;58:2142–8.
Hirsch C, Anderson ML, Newman A, et al. The Association of Race with Frailty: the cardiovascular health study. Ann Epidemiol. 2006;16:545–53.
Ottenbacher KJ, Ostir GV, Peek MK, et al. Frailty in older Mexican Americans. J Am Geriatr Soc. 2005;53:1524–31.
Woo J, Zheng Z, Leung J, et al. Prevalence of frailty and contributory factors in three Chinese populations with different socioeconomic and healthcare characteristics. BMC Geriatr. 2015;15:1–11.
Acknowledgements
Not applicable.
Data sharing statement
The study uses secondary data which is available on reasonable request through https://www.iipsindia.ac.in/content/lasi-wave-i.
Consent to participate
The survey agencies that conducted the field survey for the data collection have collected prior informed consent (verbal and written) from the respondents.
Funding
No funding was received for the present study.
Author information
Authors and Affiliations
Contributions
Both authors conceived and designed the research paper; SS analyzed the data: TM contributed to analysis: TM and SS wrote the manuscript: SS and TM refined the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The necessary guidelines and ethics for undertaking the LASI survey were approved by the Indian Council of Medical Research (ICMR).
All methods were carried out in accordance with relevant guidelines and regulations by the Indian Council of Medical Research (ICMR).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Srivastava, S., Muhammad, T. Socioeconomic vulnerability and frailty among community-dwelling older adults: cross-sectional findings from longitudinal aging study in India, 2017–18. BMC Geriatr 22, 201 (2022). https://doi.org/10.1186/s12877-022-02891-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-02891-1