
Abstract
Introduction
Gastric cancer (GC), as a highly lethal malignancy, is the fourth most common malignancy and the second leading cause of cancer-related death worldwide. This study is an umbrella review of systematic reviews and meta-analyses to present an overview of the extent and reliability of the claimed association between physical activity and the likelihood of developing or dying from GC.
Method
This study was conducted following the Joanna Brigs Institute (JBI)’s methods for conducting umbrella reviews. A systematic search was performed in PubMed, Scopus, Web of Science, and ProQuest databases until July, 2024 with predefined keywords. Two independent authors assessed the Risk of Bias in included studies using the JBI critical appraisal tool for the assessment of the quality of systematic reviews and disagreements between the authors were resolved through discussion or the opinion of another author.
Result
Five systematic reviews were included in this analysis, offering a more comprehensive understanding of the inverse relationship between physical activity and gastric cancer risk. Compared to previous studies, this review provides stronger evidence that moderate-to-high levels of physical activity significantly reduce the overall risk of developing gastric cancer.
Conclusion
While a link between physical activity and reduced cancer risk is promising, further research is crucial to unravel the specific mechanisms at play and to quantify the impact of increased activity levels on cancer prevention. Based on the findings of this study, physical activity is found to be associated with a decreased risk of GC; however, the limitation of the evidence suggested a need for future studies on this topic.
Similar content being viewed by others


Introduction
Gastric cancer (GC), also known as stomach cancer, a highly life-threatening disease, is the fourth most prevalent type of cancer and the second deadliest cause of cancer globally [1]. The etiology of gastric cancer is multifactorial that results from complex interplay of genetic, environmental, and lifestyle factors [2].
Studies show that migrants from a high to low-risk area acquire the host place’s cancer pattern, proofing the potential role of environmental factors as a trigger in the carcinogenic process [3]. Several environmental risk factors such as H. pylori infection, gastric surgery, peptic ulcer disease, dietary factors, consumption of fruit and vegetables, salt, nitrite and nitrate, ionizing radiation, pernicious anemia, smoking, alcohol consumption, exposure to asbestoses and other factors are believed to play a role in incidence of GC [4].
In addition to genetic factors [5, 6], various environmental factors such as lifestyle factors are suggested to contribute to the pathogenesis of the GC [7]. A healthy lifestyle was found to be associated with extended gains in life-lived cancers [8], which suggested lifestyle medicine, a cost-effective approach to the prevention and management of multiple conditions [9].
Previously, the conducted studies have assessed the role of dietary factors on the incidence of GC which found modifiable lifestyle habits, such as a balanced diet that emphasizes fresh fruits, vegetables, and whole grains while minimizing salt-preserved foods and alcohol consumption, can significantly lower the risk of developing gastric cancer (GC) [10]; On the other hand, consuming a diet rich in antioxidants, such as vitamin C, carotenoids, and flavonoids, along with fiber and following a Mediterranean-style diet, appears to be associated with a lower risk of gastric cancer [11, 12].
Studies suggested beneficial effects of physical activity in prevention of malignancies [13].Physical activity refers to the movements generated by skeletal muscles that lead to the consumption of energy. [14]. According to the results of studies, one of the important modifiable factors in cancer prevention research is physical activity. Numerous studies have demonstrated its link to lower all-cause mortality risk and decreased incidence of major causes of death, including cardiovascular disease and cancer [15,16,17,18]. In addition, other studies have shown that maintaining a high level of physical activity can help reduce the risk of various types of cancer. However, given the limited research on the relationship between physical activity and gastric cancer risk, no definitive conclusions can be drawn about this particular tumor. A recent evaluation highlighted the pressing necessity for additional and improved research focusing on the impact of physical activity in the development of gastric cancer [19]. Currently, the relationship between physical activity and gastric cancer risk remains inconclusive, according to the World Cancer Research Fund [20].
In the context of gastric cancer, the relationship between physical activity and risk of gastric cancer is of particular interest. Several studies, including cohort studies, case-control studies, and randomized controlled trials (RCTs), have investigated this association with different results. While some studies suggest a protective effect of physical activity against gastric cancer, others report no significant association. A comprehensive study is needed to combine the results of these studies and determine the relationship between these two issues. The umbrella review synthesis the result from multiple systematic reviews and meta-analyses to provide the association between physical activity and gastric cancer risk.
This study performed an umbrella review of systematic reviews and meta-analyses to present an overview of the extent and reliability of the claimed association between physical activity and the likelihood of developing or dying from GC. Our comprehensive evaluation sought to assess the robustness of evidence between physical activity and GC, while also highlighting hints of uncertainty and bias in the literature.
Methods
This study was conducted following the Joanna Brigs Institute (JBI)’s methods for conducting umbrella reviews [21], and the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA 2020) statement [22].
Eligibility criteria
Specific criteria were applied to select eligible articles in order to guarantee the reliability and validity of the data.
The inclusion criteria were as follows:
-
1.
Systematic review studies evaluating the association between physical activity and incidence of GC.
-
2.
All systematic review studies regardless of the type of reviewed studies.
The exclusion criteria were as follows.
-
1.
Studies in languages other than English
-
2.
Systematic review of animal studies or in vitro studies.
-
3.
Conference abstracts, letters, commentaries, opinion articles, narrative reviews.
-
4.
Articles whose full text could not be accessed. Two articles excluded for this reason including Shaodi Ma (2023) [23] and Besseling (2022) [24].
Search methods
A systematic search was performed in PubMed, Scopus, Web of Science, and ProQuest databases and google scholar without time limit with predefined keywords. The details of search strategies are presented in supplementary material 1. Also, a manual search was conducted based on the references and citations of included articles.
Search strategy
An example of a search strategy is provided in this section. Pubmed: (((“physical activity“[MeSH Terms] OR (“physical“[All Fields] AND “activity“[All Fields]) OR “physical activity“[All Fields] OR “exercise“[MeSH Terms] OR “exercise“[All Fields]) AND (“stomach neoplasms“[MeSH Terms] OR (“stomach“[All Fields] AND “neoplasms“[All Fields]) OR “stomach neoplasms“[All Fields] OR “gastric cancer“[All Fields])) AND (“systematic review“[Publication Type] OR “meta-analysis“[Publication Type]))
Scopus: TITLE-ABS-KEY((“physical activity” OR exercise OR “physical fitness” OR “recreational activity”) AND (“gastric cancer” OR “stomach neoplasms” OR “gastric neoplasms”) AND (“systematic review” OR “meta-analysis”)).
WoS: TS=(“physical activity” OR exercise OR “physical fitness” OR “recreational activity”) AND TS=(“gastric cancer” OR “stomach neoplasms” OR “gastric neoplasms”) AND TS=(“systematic review” OR “meta-analysis”).
Screening methods
The results of hand search were also added and the records were exported to EndNote software. Two independent authors reviewed the articles in title/abstracts and full-text stages and selected the articles that met the eligibility criteria. Any disagreements between the authors were resolved through discussion or the opinion of another author.
Risk of bias assessment
Two independent authors assessed the Risk of Bias in included studies using the JBI critical appraisal tool for the assessment of the quality of systematic reviews and disagreements between the authors were resolved through discussion or the opinion of another author. This tool assessed the explicitly of the review question, appropriate eligibility criteria and search strategy, search for sources and resources, appropriate appraisal tool and methods, methods to minimize errors in data extraction, appropriate methods for combine studies, assessment of publication bias, appropriate recommendations s for policy and/or practice and directives for new research based on the findings.
Data extraction
The data extraction was conducted in a data extraction table which included the study name, the final search date, the number of included studies, the RoB assessment of included studies and appraisal ratings, the publication bias, GC subtypes and physical activity, and finally the reported outcome of meta-analysis. One author supplemented the data extraction table and another one checked the extracted data.
Results
Search results and screening process
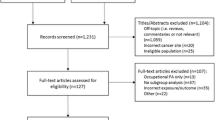
Out of 1440 results of database searches, finally, five systematic review studies were included in this umbrella review. The detailed information on searching, selecting, and reasons for excluded studies is summarized in the PRISMA diagram (Fig. 1). A summary of the included studies is presented in Table 1 and the details of RoB assessments are presented in Table 2.

PRISMA flow diagram
The studies that were excluded due to unavailability of the article full text or lack of examination the relationship between the risk of gastric cancer and physical activity listed in the Table 3.
Summary of findings
In the most updated one, Xie et al. [25], in a systematic review of the association between physical activity and digestive system cancers, showed that high physical activity can reduce the incidence of GC. In this study quality of physical activity was assessed based on weekly metabolic equivalent tasks; which resulted in low, moderate, and high physical activity categories. What is important in this systematic review is the evaluation of the combined relationship between high vs. low physical activity levels and the risk of digestive-system cancer (DSC) (gastric cancer (RR = 0.83, 95%CI: 0.76–0.91)). The results of the meta-analysis were consistent across different study designs, with case-control studies (RR = 0.73, 95%CI: 0.68–0.78) and prospective cohort studies (RR = 0.88, 95%CI: 0.80–0.91) showing a similar pattern. The meta-analysis of 9 studies suggests a possible association between moderate physical activity (PA) and a reduced risk of developing gastric cancer (DSC). Compared to low PA, moderate PA was associated with a lower risk (RR = 0.89, 95%CI: 0.80–1.00). While the findings for high PA were not statistically significant, there was a slight indication of an increased risk compared to moderate PA (RR = 1.11, 95%CI: 0.94–1.32). Limited evidence from 5 studies suggests that meeting the recommended PA guidelines may not have a significant impact on DSC risk (RR = 0.96, 95%CI: 0.91–1.02).
Chen et al. [26] indicated that the risk of GC was 13% lower among the most physically active people than among the least active people. This study did not report a significant difference in subgroup analysis with respect to study designs, sex, and risk of bias, study population, and domain and subtype of physical activity. In addition, this study suggested a dose-response relationship between physical activity and risk of GC. A comprehensive meta-analysis of 15 studies revealed that individuals engaged in the highest levels of physical activity exhibited a 13% reduced risk of developing gastric cancer compared to those with the least physical activity (RR = 0.87, 95% CI: 0.78, 0.97). The meta-analysis findings indicated a moderate degree of heterogeneity among the studies (I2 = 49.8%, P = .012). Some evidence of publication bias was observed in the primary meta-analysis. Meta-regression analyses revealed that no variables significantly influenced the association between physical activity and gastric cancer (P > .05 in all regression analyses). Begg’s and Egger’s tests did not provide evidence of significant publication bias in the studies examined. The P value of Egger’s test for the highest versus lowest physical activity analysis was 0.134.
Psaltopoulou et al. [27], in a systematic review in 2016, reported an association between a lower risk of gastric cancer with any type of physical activity. In sub-group analyses, this relationship was more evident in men, the Asian population, and non-cardia type of GC. A total of 10 cohort studies (7,551 incident cases in 1,541,208 participants) and 12 case-control studies (5,803 cases and 73,629 controls) were included in the meta-analysis. he pooled relative risk (RR) for gastric cancer associated with any physical activity was 0.81 (95% CI: 0.73, 0.89), indicating that individuals who engaged in any amount of physical activity had a 19% lower risk of developing gastric cancer compared to those who did not. The protective effect of physical activity was evident in both men and women, with pooled RRs of 0.87 (95% CI: 0.77, 0.99) and 0.73 (95% CI: 0.65, 0.82), respectively. The protective effect of physical activity was particularly pronounced for noncardia gastric cancer (pooled RR = 0.62; 95% CI: 0.52, 0.75) and studies conducted in Asia (pooled RR = 0.82; 95% CI: 0.74, 0.90).
Ajibola Ibraheem Abioye et al. [28] also reported the protective effects of physical activity against GC. In sub-group analyses of this study, the associations appear weaker in smokers, and distal none-cardia type of the disease in meta-regressions. In this study, sufficient physical activity was defined as 150 min of moderate-intensity aerobics 75 min of vigorous-intensity activity, or an equivalent combination of both in a week and based on the findings, high-level physical activity did not significantly differ from the sufficient physical activity group. The meta-analysis included a comprehensive dataset drawn from seven prospective cohort studies and four case-control studies, encompassing 1,535,006 individuals and 7,944 cases of gastric cancer.
The meta-analysis found a modest but consistent protective association between sufficient physical activity and gastric cancer risk. This association was observed in both prospective cohort studies and case-control studies, with a pooled relative risk of 0.81 (95% CI: 0.69, 0.96). However, the association was found to be weaker in smokers compared to non-smokers and may also be weaker for gastric cardia cancer compared to the distal non-cardia subtypes.
Siddharth Singh et al.’s study [29] also approved the findings of previously mentioned studies regarding the protective effects of physical activity against GChe meta-analysis revealed a consistent association between physical activity and reduced gastric cancer risk. Individuals who were the most physically active had a 21% lower risk of developing the disease compared to those who were the least active (OR, 0.79; 95% CI, 0.71, 0.87). This protective effect was seen for both gastric cardia and distal stomach cancer subtypes.
Discussion
This study aims to evaluate the possible relationship between physical activity and the risk of gastric cancer. Based on the previously published systematic review and meta-analysis studies, physical activity is found to be associated with decreased risk of GC.
There are other individual studies (not included in a systematic review) in this area, including these studies, Body mass and physical activity and gastric cancer risk in a population-based cohort study [31] and Physical activity and gastric cancer risk in patients with and without Helicobacter pylori infection: a hospital-based case-control study [32] and because it has not been systematically reviewed and the evidence and reasons for the effect of physical activity on the risk of gastric cancer have not been comprehensively reviewed in them, it was reasoned that Do not use in this study.
GC is a significant burden on global health. In 2020, there were an estimated 1.1 million new cases of gastric cancer and 800,000 deaths globally [33]. The burden of gastric cancer is particularly high in low- and middle-income countries, where over two-thirds of cases occur. The five year overall age-standardized relative survival rate of GC is about 40%, which decreased to about 10% in patients with distant-stage GC [34]. The economic burden of gastric cancer is also significant so the disease can lead to lost productivity and income for patients and their families. In this condition, seeking prevention methods is key to reducing the burden of gastric cancer. This covers tactics including expanding access to healthcare and screening programs, encouraging healthy lifestyles, and minimizing exposure to established risk factors like smoking and H. pylori infection [35]. One of the easy-accessible methods in this regard is physical activity.
The exact mechanism by which physical activity decreases the risk of gastric cancer is not fully understood [36]; However, several hypotheses such as reduced inflammation, improved immune function, reduced risk of obesity, as well as alternation of gut microbiome are suggested. Physical activity has been shown to reduce chronic inflammation in the body, which is a risk factor for cancer development [37]. In addition, physical activity can improve insulin sensitivity and reduce insulin resistance [38]. Insulin resistance has been linked to an increased risk of several types of cancer, including gastric cancer [39].
In contrast to previous studies, this study provides a more comprehensive analysis of the inverse relationship between physical activity and the risk of gastric cancer, as indicated by five systematic reviews. The updated meta-analysis data support the notion that moderate to high levels of PA act as a protective factor, significantly lowering overall GC risk. However, the reduction rate for specific GC subtypes may vary. Furthermore, limited evidence suggests that meeting the international PA guidelines might not significantly impact GC risk. Therefore, more research is warranted to establish the optimal PA regimen for effectively reducing GC risk.
In the second study a comprehensive review of existing studies indicates that physical activity may offer some protection against esophageal and gastric cancer. This finding suggests that future research should delve deeper into the remaining ambiguities of this association, such as whether sedentary behavior or non-aerobic physical activity increases cancer risk and whether the intensity of physical activity influences the protective effect of physical activity against gastric and esophageal cancer. Additionally, further studies are needed to elucidate the mechanisms through which physical activity may safeguard against these cancers and determine whether increasing physical activity can effectively reduce cancer risk.
In the third study A comprehensive meta-analysis of 10 cohort and 12 case-control studies examining the link between physical activity and gastric cancer risk suggests a substantial protective association. Individuals engaging in the highest levels of physical activity exhibited a 19% lower risk of developing gastric cancer compared to those with the lowest physical activity levels. This finding corroborates the protective effects of physical activity observed for other cancer sites.8,14,20 Importantly, the protective association held true across both case-control and cohort studies. In summary, the fourth meta-analysis highlights a potential protective role of regular physical activity (PA) in reducing the risk of gastric cancer. This finding has crucial implications for comprehending the underlying causes of gastric cancer and developing effective prevention strategies. Additionally, it provides further evidence supporting the benefits of an overall healthy lifestyle with regular PA in minimizing the risk of noncommunicable diseases. In the last study stated due to the high incidence and dismal prognosis of gastric cancer, the development of cost-effective preventive strategies is urgently needed. Although chemoprevention holds promise, its cost-effectiveness and risk-benefit profile remain uncertain. This systematic review and meta-analysis of 16 observational studies encompassing 1.6 million patients and 11,111 gastric cancer cases revealed a 21% lower risk of gastric cancer among the most physically active individuals compared to the least physically active individuals, after controlling for relevant confounders like age, obesity, and other gastric cancer risk factors (smoking, alcohol consumption, dietary patterns, and socioeconomic status).
Based on the findings of this study, physical activity is found to be associated with a decreased risk of GC; however, the limitation of the evidence suggested a need for future studies on this topic. Several methodological flaws in the research on the connection between physical activity and GC prevent us from drawing a definite conclusion [40]. A limited number of well-designed prospective studies, lack of appropriate adjustment for all of the known cofounders such as genetic factors, the companionship of high physical activity with other lifestyle factors such as healthy diet as well as better socioeconomic condition, self-administered nature of the studies, lack of attention to histology of GC, and finally the observed great level of heterogeneity between the studies, were the main limitation of the studies.
Data availability
Not applicable (this manuscript does not report data generation or analysis).
References
Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends—an update. Cancer Epidemiol Biomarkers Prev. 2016;25(1):16–27.
Fuchs CS, Mayer RJ. Gastric carcinoma. N Engl J Med. 1995;333(1):32–41.
Kamineni A, Williams MA, Schwartz SM, Cook LS, Weiss NS. The incidence of gastric carcinoma in Asian migrants to the United States and their descendants. Cancer Causes Control. 1999;10:77–83.
Kelley JR, Duggan JM. Gastric cancer epidemiology and risk factors. J Clin Epidemiol. 2003;56(1):1–9.
Lee S, Yang HK, Lee HJ, Park DJ, Kong SH, Park SK. Systematic review of gastric cancer-associated genetic variants, gene-based meta-analysis, and gene-level functional analysis to identify candidate genes for drug development. Front Genet. 2022;13:928783.
Ghojazadeh M, Somi MH, Naseri A, Salehi-Pourmehr H, Hassannezhad S, Hajikamanaj Olia A, et al. Systematic review and Meta-analysis of TP53, HER2/ERBB2, KRAS, APC, and PIK3CA genes expression pattern in gastric Cancer. Middle East J Dig Dis. 2022;14(3):335–45.
Hui Y, Tu C, Liu D, Zhang H, Gong X. Risk factors for gastric cancer: a comprehensive analysis of observational studies. Front Public Health. 2022;10:892468.
Nyberg ST, Singh-Manoux A, Pentti J, Madsen IEH, Sabia S, Alfredsson L, et al. Association of Healthy Lifestyle with years lived without Major Chronic diseases. JAMA Intern Med. 2020;180(5):760–8.
Bodai BI, Nakata TE, Wong WT, Clark DR, Lawenda S, Tsou C, et al. Lifestyle Medicine: a brief review of its dramatic impact on Health and Survival. Perm J. 2018;22:17–025.
Bouras E, Tsilidis KK, Triggi M, Siargkas A, Chourdakis M, Haidich AB. Diet and Risk of Gastric Cancer: an Umbrella Review. Nutrients. 2022;14(9).
Lee YY, Derakhshan MH. Environmental and lifestyle risk factors of gastric cancer. Arch Iran Med. 2013;16(6):0.
Psaltopoulou T, Kosti RI, Haidopoulos D, Dimopoulos M, Panagiotakos DB. Olive oil intake is inversely related to cancer prevalence: a systematic review and a meta-analysis of 13800 patients and 23340 controls in 19 observational studies. Lipids Health Dis. 2011;10:1–16.
Wang Q, Zhou W. Roles and molecular mechanisms of physical exercise in cancer prevention and treatment. J Sport Health Sci. 2021;10(2):201–10.
Laporte RE, Montoye HJ, Caspersen CJ. Assessment of physical activity in epidemiologic research: problems and prospects. Public Health Rep. 1985;100(2):131.
Lee CD, Folsom AR, Blair SN. Physical activity and stroke risk: a meta-analysis. Stroke. 2003;34(10):2475–81.
Sofi F, Capalbo A, Cesari F, Abbate R, Gensini GF. Physical activity during leisure time and primary prevention of coronary heart disease: an updated meta-analysis of cohort studies. Eur J Cardiovasc Prev Rehabilitation. 2008;15(3):247–57.
Boyle T, Keegel T, Bull F, Heyworth J, Fritschi L. Physical activity and risks of proximal and distal colon cancers: a systematic review and meta-analysis. J Natl Cancer Inst. 2012;104(20):1548–61.
Wolin KY, Yan Y, Colditz GA. Physical activity and risk of colon adenoma: a meta-analysis. Br J Cancer. 2011;104(5):882–5.
Forman D, Burley V. Gastric cancer: global pattern of the disease and an overview of environmental risk factors. Best Pract Res Clin Gastroenterol. 2006;20(4):633–49.
Fund WCR. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Research AIfC. American Institute for Cancer Research; 2007.
Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. Int J Evid Based Healthc. 2015;13(3):132–40.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Ma S, Liu H, Sun C, Meng M, Qu G, Jiang Y, et al. Effect of physical activity on incidence and mortality in patients with gastric cancer: evidence from real-world studies. Cancer Causes Control. 2023;34(12):1095–111.
Besseling J, van Velzen M, Wierdsma N, Alonso-Duin KS, Weijs P, May AM, et al. Exercise and Nutritional interventions in patients with Advanced Gastroesophageal Cancer: a systematic review. J Gastrointest cancer. 2023;54(3):1006–9.
Xie F, You Y, Huang J, Guan C, Chen Z, Fang M, et al. Association between physical activity and digestive-system cancer: an updated systematic review and meta-analysis. J Sport Health Sci. 2021;10(1):4–13.
Chen Y, Yu C, Li Y. Physical activity and risks of esophageal and gastric cancers: a meta-analysis. PLoS ONE. 2014;9(2):e88082.
Psaltopoulou T, Ntanasis-Stathopoulos I, Tzanninis IG, Kantzanou M, Georgiadou D, Sergentanis TN. Physical activity and gastric Cancer risk: a systematic review and Meta-analysis. Clin J Sport Med. 2016;26(6):445–64.
Abioye AI, Odesanya MO, Abioye AI, Ibrahim NA. Physical activity and risk of gastric cancer: a meta-analysis of observational studies. Br J Sports Med. 2015;49(4):224–9.
Singh S, Edakkanambeth Varayil J, Devanna S, Murad MH, Iyer PG. Physical activity is associated with reduced risk of gastric cancer: a systematic review and meta-analysis. Cancer Prev Res (Phila). 2014;7(1):12–22.
Chen Y, Liu L, Wang X, Wang J, Yan Z, Cheng J, et al. Body Mass Index and Risk of Gastric Cancer: a Meta-analysis of a Population with more than ten million from 24 prospective studies. Cancer Epidemiol Biomarkers Prev. 2013;22(8):1395–408.
Sjodahl K, Jia C, Vatten L, Nilsen T, Hveem K, Lagergren J. Body mass and physical activity and risk of gastric cancer in a population-based cohort study in Norway. Cancer Epidemiol Biomarkers Prev. 2008;17(1):135–40.
Gunathilake MN, Lee J, Jang A, Choi IJ, Kim Y-I, Kim J. Physical activity and gastric cancer risk in patients with and without Helicobacter pylori infection in a Korean population: a hospital-based case-control study. Cancers. 2018;10(10):369.
Ilic M, Ilic I. Epidemiology of stomach cancer. World J Gastroenterol. 2022;28(12):1187–203.
Li Y, Feng A, Zheng S, Chen C, Lyu J. Recent estimates and predictions of 5-Year survival in patients with gastric Cancer: a model-based period analysis. Cancer Control. 2022;29:10732748221099227.
Salvatori S, Marafini I, Laudisi F, Monteleone G, Stolfi C. Helicobacter pylori and gastric Cancer: pathogenetic mechanisms. Int J Mol Sci. 2023;24(3).
Kunzmann AT, Mallon KP, Hunter RF, Cardwell CR, McMenamin ÚC, Spence AD, et al. Physical activity, sedentary behaviour and risk of oesophago-gastric cancer: a prospective cohort study within UK Biobank. United Eur Gastroenterol J. 2018;6(8):1144–54.
Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. J Sport Health Sci. 2019;8(3):201–17.
Lin Y, Fan R, Hao Z, Li J, Yang X, Zhang Y et al. The Association between physical activity and insulin level under different levels of lipid indices and serum uric acid. Front Physiol. 2022;13.
Kwon HJ, Park MI, Park SJ, Moon W, Kim SE, Kim JH, et al. Insulin resistance is Associated with early gastric Cancer: a prospective Multicenter Case Control Study. Gut Liver. 2019;13(2):154–60.
Ayán C, Cancela J, Molina A, Fernández T, Martín V. Methodological issues when analysing the role of physical activity in gastric cancer prevention: a critical review. Eur Rev Aging Phys Activity. 2013;10(1):7–13.
Acknowledgements
Not applicable.
Funding
This study was funded with the authors’ own contributions.
Author information
Authors and Affiliations
Contributions
M.M: Design, Gathering data, Analysis and Interpretation of data, Article writing. V.F: Design, Analysis and interpretation of data, Article writing. Z.M: Design, Gathering data, Analysis and interpretation of data, Article writing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by Tabriz University of Medical Sciences (TUOMS) ethical committee (IR.TBZMED.REC.1401.484). All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Maleki, M., Fatehi, V. & Mohammadzadeh, Z. The association between physical activity and risk of gastric cancer; an umbrella review. BMC Gastroenterol 24, 261 (2024). https://doi.org/10.1186/s12876-024-03360-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-024-03360-2