
Abstract
Purpose
The link between dietary fiber intake and Non-alcoholic fatty liver disease (NAFLD) is under exploration, yielding inconsistent findings. Considering the limitations of previous research and the significance of dietary fiber in hepatic steatosis, this study investigates the association between dietary fiber intake and Controlled Attenuation Parameter (CAP) among 5935 participants from the National Health and Nutrition Examination Survey (NHANES).
Materials and methods
Multivariable regression was used to evaluate the association between dietary fiber intake and CAP. Smoothed curve fitting and threshold effect analysis techniques were applied to illustrate non-linear relationships.
Results
After adjusting for other variables, a negative correlation emerged between dietary fiber intake and CAP. Subgroup analysis by gender and race/ethnicity revealed a sustained negative association between dietary fiber intake and CAP among females and Whites. Additionally, an inverted U-shaped relationship was observed between dietary fiber intake and CAP among women and other race, with inflection points at 13.80 g/day and 33.45 g/day, respectively.
Conclusion
Our research indicates that in the majority of Americans, there is an inverse relationship between dietary fiber intake and hepatic steatosis. This relationship exhibits an inverted U-shaped curve in women and other race, with a threshold effect. The findings of this study hold potential significance for clinical nutrition interventions, personalized dietary guidance, and advancing research into the diet-disease mechanism relationship.
Similar content being viewed by others


Introduction
The most common chronic liver disease worldwide and a major contributor to severe liver disorders is non-alcoholic fatty liver disease (NAFLD) [1]. NAFLD is a multifactorial condition influenced by environmental, genetic, and dietary factors, metabolic imbalances such as insulin resistance, lipid toxicity, inflammation triggered by micro-inflammation, and immune changes, cytokine imbalances, innate immune activation, and alterations in the microbiota [2, 3]. Studies indicate that NAFLD impacts approximately 25% of people globally, significantly burdening healthcare systems [4]. Hepatic steatosis, or liver fat accumulation, is a defining characteristic and primary histological feature of NAFLD [5]. This condition is not only NAFLD’s initial abnormality but also crucial across the disease spectrum [6]. It ranges from simple fat buildup to complex changes such as inflammation, fibrosis, cirrhosis, and liver cancer [7]. Thus, early diagnosis and prevention of hepatic steatosis are essential [8].
Liver biopsy, the gold standard for assessing liver fat, is invasive [9]. To reduce the need for liver biopsy, various non-invasive biomarkers have been studied. While non-invasive biomarkers cannot currently replace liver biopsy and histological assessment, they may play a crucial role in screening patients for liver biopsy [10]. Non-invasive methods such as magnetic resonance imaging (MRI) or computed tomography (CT) scans can assess liver fat [11, 12]. However, they are time-consuming, costly, and not suited for large-scale studies. Transient elastography, favored for NAFLD screening for its precision and non-invasiveness, evaluates hepatic steatosis via the Controlled Attenuation Parameter (CAP) [13, 14]. Numerous studies demonstrate a strong correlation between CAP values and liver fat levels as determined by biopsies [11, 15, 16].
Recently, the influence of diet on health has garnered more attention. Research indicates that consuming more dietary fiber, mainly from grains, fruits, and vegetables, correlates with lower risks of hypertension, hyperuricemia, type 2 diabetes, cardiovascular diseases, and cancer [17,18,19,20,21,22]. The link between dietary fiber consumption and NAFLD is being explored, with inconsistent results. Some studies indicate lower dietary fiber consumption in NAFLD patients [23,24,25], whereas others note no significant difference compared to non-NAFLD individuals [26,27,28]. Variations in study design and populations may explain these discrepancies. Often, these studies diagnose NAFLD using abdominal ultrasonography or the Fatty Liver Index, derived from body mass index (BMI), waist circumference, triglycerides, and gamma-glutamyl transferase. However, these methods do not directly and objectively measure liver fat changes.
The National Health and Nutrition Examination Survey (NHANES) is a program designed to assess the health and nutritional status of American adults and children [29]. It merges interviews and physical examinations, compiling a comprehensive dataset of dietary intake, laboratory data, and health outcomes [30]. The 2017–2020 NHANES introduced transient elastography for the first time to measure liver fat changes, offering the largest U.S. sample of CAP observations. Acknowledging previous studies’ limitations and dietary fiber’s critical role in liver health, this study leverages the broad population from the 2017–2020 NHANES. It employs CAP to explore further the relationship between dietary fiber intake and liver fat changes.
Materials and methods
Statement of ethics
All participants gave their informed agreement, and the project was authorized by the National Center for Health Statistics Research Ethics Review Board.
Study population
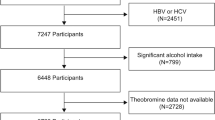
In order to achieve nationwide representation, NHANES, a thorough and ongoing cross-sectional national survey in the US, uses a stratified, multistage, clustered random sampling to collect diet and health data from the whole population [29]. Out of 15,560 participants in the 2017–2020 NHANES cycle, 9698 had available CAP data. We excluded 2,451 participants testing positive for hepatitis B antigen, hepatitis C antibody, or hepatitis C RNA, 799 with significant alcohol consumption (4, 5, or more drinks daily), and 513 lacking dietary fiber data. Ultimately, 5935 participants were included in the study. Figure 1 illustrates the sample selection flowchart.

Flowchart of participant selection. NHANES, National Health and Nutrition Examination Survey; CAP, controlled attenuation parameter
Variables
The investigation focused on dietary fiber intake as the exposure factor. Dietary fiber intake assessment involved two 24-hour food recall interviews. Three to ten days after the first interview, which took place at a mobile exam facility, there was a telephone interview. The United States Department of Agriculture’s Food and Nutrient Database for Dietary Studies was the source of information on nutrient intakes, including dietary fiber [31]. Dietary fiber intake per participant was averaged from two days of dietary recall data when available, or based on a single day’s data otherwise.
The study’s outcome variable, CAP, was measured using the FibroScan® 502 V2 Touch equipped with liver ultrasonography transient elastography. This device records CAP by measuring ultrasonic attenuation, which reflects hepatic steatosis and indicates liver fatness. According to a recent key study, there is 90% sensitivity in detecting different degrees of hepatic steatosis when CAP values ≥ 274 dB/m, which indicate NAFLD status, are present [32]. This study, which is based on three earlier investigations, classifies CAP ≥ 302 dB/m as a sign of severe steatosis in instances of NAFLD [33,34,35].
Our study incorporated categorical covariates such as gender, race/ethnicity, education level, marital status, smoking behavior, diabetes, hypertension, and cholesterol levels. Continuous covariates in our analysis included age, BMI, waist circumference, serum glucose, high density lipoprotein (HDL)-cholesterol, low density lipoprotein (LDL)-cholesterol, aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transpeptidase (GGT), serum albumin, serum creatinine, and uric acid. Detailed data on dietary fiber intake, CAP, and other variables are publicly accessible at http://www.cdc.gov/nchs/nhanes/.
Statistical analysis
We utilized a weighted variance estimate approach to account for significant volatility in our data set. For categorical data, the weighted χ2 test was used to evaluate the differences between groups, and for continuous variables, the weighted linear regression model was employed. Utilizing a weighted multivariate regression model, we investigated the relationship between CAP and dietary fiber consumption. It’s worth noting that due to collinearity between serum glucose and diabetes status, as well as between HDL-cholesterol and LDL-cholesterol with high cholesterol levels, the multivariable regression equation did not include HDL-cholesterol, LDL-cholesterol, and serum glucose. Stratified multivariate regression analysis was used to carry out subgroup analysis. In order to examine the nonlinear association between dietary fiber intake and CAP, generalized additive models and smooth curve fits were employed. Upon discovering nonlinearity, we calculated the inflection point in the dietary fiber intake and CAP relationship using a recursive technique, followed by applying a two-piecewise linear regression model to both sides of this point. R (http://www.Rproject.org) and EmpowerStats (http://www.empowerstats.com) were used for all analyses, with a P value < 0.05 being regarded as statistically significant.
Results
Our study included 5395 participants. The clinical features of CAP participants are shown in Table 1, which is arranged in columns for stratification. The group with severe steatosis is older, primarily male, married, and has a higher percentage of non-Hispanic White people. It also has a higher prevalence of cardiometabolic risk factors, including high blood pressure, smoking, diabetes, raised BMI, and hypercholesterolemia, than the non-NAFLD group. Increases in serum glucose, HDL-cholesterol and LDL-cholesterol, liver enzymes (AST, ALT, GGT), uric acid, and dietary fiber intake correlate with higher CAP values, while albumin levels decrease. There were no significant differences in the income to poverty ratio among the groups.
Table 2 shows the results of the multivariate regression analysis. In the unadjusted Model 1, daily fiber intake showed no significant association with CAP (β = 0.00, 95% CI: -0.19, 0.19, P = 0.9900). But when age, sex, and race/ethnicity were taken into account, Model 2 showed a significant correlation between increased fiber consumption and decreased CAP (β=-0.43, 95% CI: -0.61, -0.25, P < 0.0001). Even after accounting for extra factors, Model 3’s negative connection persisted (β=-0.19, 95% CI: -0.38, -0.01, P = 0.0398). Analysis by quartiles of dietary fiber intake in Model 3 showed that the highest quartile (Q4) had significantly lower CAP than the lowest quartile (Q1) (β = -5.78, 95% CI: -10.40, -1.15, P = 0.0144), demonstrating a significant linear trend (P for trend = 0.026). The inverse link between dietary fiber consumption and CAP remained significant for women (β=-0.29, 95% CI: -0.56, -0.02, P = 0.0329) and Whites (β=-0.39, 95% CI: -0.69, -0.09, P = 0.0113) in Model 3, according to subgroup analyses by age, sex, and race/ethnicity in Table 2.
Figures 2, 3, 4 and 5 illustrate smooth curve fits and generalized additive models, demonstrating an inverted U-shaped relationship between dietary fiber intake and CAP in women and other race. In women, the two-piecewise linear model indicated a dietary fiber intake inflection point at 13.80 g/day (Table 3). Below this threshold, there was no significant association between dietary fiber intake and CAP levels (β = 0.44, 95% CI: -0.26, 1.13, P = 0.2172). Above 13.80 g/day, a higher dietary fiber intake significantly correlated with lower CAP levels (β=-0.62, 95% CI: -1.01, -0.23, P = 0.0021). The statistically significant likelihood ratio test between the standard linear and two-piecewise linear models supports a threshold effect (P = 0.025). Similarly, in other race, inflection points occur at a dietary fiber intake of 33.45 g/day, as evidenced by a significant likelihood ratio (P = 0.004) (Table 4). For dietary fiber intakes below 33.45 g/day, each 1 g/day increase was related to a 0.65 dB/m raise in CAP (95% CI: -0.08, 1.39, P = 0.0801); by comparison, for individuals with a dietary fiber intake > 33.45 g/day, a 1 g/day upregulation was connected with a 3.46 dB/m drop in CAP (95%CI: -5.95, -0.97, P = 0.0069).

The association between Dietary fiber intake and controlled attenuation parameter. (a) Each black point represents a sample. (b) Solid rad line represents the smooth curve fit between variables. Blue bands represent the 95% of confidence interval from the fit. Age, sex, race/ethnicity, education level, marital status, body mass index, Waist circumference, smoking behavior, and the existence of diabetes, hypertension, and high cholesterol level, aspartate aminotransferase, alanine aminotransferase, γ- glutamyl transpeptidase, serum albumin, serum creatinine and uric acid were adjusted

The association between Dietary fiber intake and controlled attenuation parameter stratified by age. Sex, race/ethnicity, education level, marital status, body mass index, Waist circumference, smoking behavior, and the existence of diabetes, hypertension, and high cholesterol level, aspartate aminotransferase, alanine aminotransferase, γ- glutamyl transpeptidase, serum albumin, serum creatinine and uric acid were adjusted

The association between Dietary fiber intake and controlled attenuation parameter stratified by sex. Age, race/ethnicity, education level, marital status, body mass index, Waist circumference, smoking behavior, and the existence of diabetes, hypertension, and high cholesterol level, aspartate aminotransferase, alanine aminotransferase, γ- glutamyl transpeptidase, serum albumin, serum creatinine and uric acid were adjusted

The association between Dietary fiber intake and controlled attenuation parameter stratified by race/ethnicity. Age, sex, education level, marital status, body mass index, Waist circumference, smoking behavior, and the existence of diabetes, hypertension, and high cholesterol level, aspartate aminotransferase, alanine aminotransferase, γ- glutamyl transpeptidase, serum albumin, serum creatinine and uric acid were adjusted
Discussion
This study analyzed data from the NHANES in the United States from 2017 to 2020. Using the CAP for direct assessment, the study explored the relationship between dietary fiber intake and hepatic steatosis. Multivariate logistic regression analysis, adjusting for potential confounding factors, revealed that higher dietary fiber intake is associated with lower CAP values. This suggests that dietary fiber consumption and hepatic steatosis are negatively correlated, especially in women and White individuals.
Our findings are consistent with research from different populations across various countries and animal models. For instance, a study conducted in the Netherlands showed that higher liver fat indices were associated with lower dietary fiber intake [24]. Likewise, an Iranian case-control study found that NAFLD patients consumed less dietary fiber than healthy individuals [23]. NAFLD and total dietary fiber consumption were also found to be negatively correlated in another Chinese investigation [25]. Animal experiments further support these observations. One study observed that high-viscosity dietary fiber intake could reduce obesity and liver fat changes caused by a high-fat diet [36]. Another experiment, simulating a Western diet in mice, showing that a long-term high-fat, low-fiber diet (HFFD) resulted in liver fat changes [37]. Collectively, these studies suggest a protective effect of dietary fiber against liver fat changes, underscoring its potential significance in dietary guidelines for liver health.
Nevertheless, an Israeli cross-sectional study revealed no notable disparities in dietary fiber consumption between NAFLD patients and healthy individuals [26]. This outcome might be attributed to the study’s lack of adjustment for confounding factors. Similarly, a case-control study involving 36 Chinese individuals indicated no variance in dietary fiber intake between those with NAFLD and healthy subjects [27]. The limited sample size and incomplete adjustment for confounding factors could explain this observation. Additionally, a recent cross-sectional study of 3,882 elderly participants did not find a consistent link between dietary fiber consumption and NAFLD [28]. The limitations present in these studies contribute to the inconclusive evidence about the link between dietary fiber intake and alterations in hepatic steatosis.
Insufficient dietary fiber is linked to an increased risk of hepatic steatosis, as it plays a crucial role in regulating lipid synthesis pathways and preventing liver fat alterations [38]. Dietary fiber could also mitigate hepatic steatosis via the liver’s G-protein-coupled receptor (GPR) 41/43-calmodulin-dependent protein kinase II (CaMKII), histone deacetylase 1 (HDAC1)-cyclic adenosine monophosphate response element-binding protein (CREB) pathway [37]. Furthermore, studies suggest that dietary fiber intake is associated with regulating glucose homeostasis and gut microbiota, which may help prevent liver fat changes [39,40,41].
Furthermore, in smooth curve fitting and threshold effect analysis across different ages, genders, and races, we observed a nonlinear relationship between dietary fiber intake and CAP in women and other race, with inflection points at 13.8 g/day and 33.45 g/day respectively. To our knowledge, this might be the first study to uncover an inverse U-shaped relationship between dietary fiber intake and hepatic steatosis in American women and other race American. This indicates that these groups need to exceed certain fiber intake thresholds for dietary fiber to benefit liver health. Clinically, this suggests the advantage of personalized dietary recommendations, particularly for women and other racial groups, emphasizing increased intake of high-fiber foods like fruits and vegetables to reduce the risk of liver fat accumulation.
The relationship between dietary fiber and hepatic steatosis is intricate, potentially involving various mechanisms such as insulin resistance, hepatic lipid metabolism, and changes in gut microbiota [42]. According to the research [43], the consumption of total fiber, insoluble fiber, and soluble fiber differs among different ethnicities and genders, leading to varying risks of insulin resistance and hypertension. Additionally, dietary fiber intake may play a role in modulating gut microbiota activity, which could have different effects on hepatic steatosis depending on gender [44]. Variations in risk factors between ethnicities can also be explained by differences in genetic predisposition, obesity rates, and other factors. However, further prospective studies with substantial sample sizes are needed to elucidate the complex relationship between dietary fiber and hepatic steatosis among different genders and ethnicities. In our research, the scale of the cohort strengthens the findings, as NHANES aims to generate nationally representative estimates.
Our study boasts numerous strengths. Firstly, we used a large and nationally representative sample from the United States, minimizing selection bias. Secondly, we directly measured liver fat content using the reliable CAP method, rather than indirect assessment through imaging or biochemical markers, enhancing the accuracy of our findings. Furthermore, our comprehensive analysis methods, including subgroup analysis for women and Whites, confirm the overall results, increasing the reliability of our conclusions. Most notably, employing curve fitting and nonlinear models to explore the non-linear relationship between dietary fiber and liver fat changes highlighted threshold effects.
Nonetheless, there are limitations to our study. First off, as a cross-sectional study, it cannot establish causality. Additionally, the dietary fiber intake data, derived from two 24-hour dietary recalls, may be potentially susceptible to reporting bias. Finally, the fact that participants were exclusively from the United States limits the generalizability of the results to other populations.
Conclusions
Our research indicates that in the majority of Americans, there is an inverse relationship between dietary fiber intake and changes in hepatic steatosis. In females and individuals of other races, this relationship demonstrates an inverted U-shaped curve, indicative of a threshold effect. This implies that a specific amount of dietary fiber is required for beneficial effects on liver health in these groups. The findings of this study hold potential significance for clinical nutrition interventions, personalized dietary guidance, and advancing research into the diet-disease mechanism relationship.
Data availability
All NHANES data for this study are publicly available and can be found here: https://wwwn.cdc.gov/nchs/nhanes.
References
Lazo M, Hernaez R, Eberhardt MS, et al. Prevalence of nonalcoholic fatty liver disease in the United States: the Third National Health and Nutrition Examination Survey, 1988–1994[J]. Am J Epidemiol. 2013;178(1):38–45.
Abenavoli L, Giubilei L, Procopio AC, et al. Gut microbiota in non-alcoholic fatty liver Disease patients with Inflammatory Bowel diseases: a Complex Interplay[J]. Nutrients. 2022;14(24):5323.
Abenavoli L, Maurizi V, Boccuto L, et al. Nutritional Support Acute Liver Failure[J] Dis. 2022;10(4):108.
Moon AM, Singal AG, Tapper EB. Contemporary epidemiology of Chronic Liver Disease and Cirrhosis[J]. Clin Gastroenterol Hepatol. 2020;18(12):2650–66.
Wong C, Lee MH, Yaow CYL et al. Glucagon-like Peptide-1 receptor agonists for non-alcoholic fatty liver disease in type 2 diabetes: a Meta-Analysis[J]. Front Endocrinol, 2021,12.
Cast A, Kumbaji M, D’Souza A, et al. Liver proliferation is an essential driver of fibrosis in mouse models of nonalcoholic fatty liver Disease[J]. Hepatol Commun. 2019;3(8):1036–49.
Goldberg D, Ditah IC, Saeian K, et al. Changes in the prevalence of Hepatitis C virus infection, nonalcoholic steatohepatitis, and alcoholic liver disease among patients with cirrhosis or liver failure on the Waitlist for Liver Transplantation[J]. Gastroenterology. 2017;152(5):1090–9.
Masuoka HC, Chalasani N. Nonalcoholic fatty liver disease: an emerging threat to obese and diabetic individuals[J]. Ann N Y Acad Sci. 2013;1281(1):106–22.
Burhans MS, Balu N, Schmidt KA, et al. Impact of the Analytical Approach on the reliability of MRI-Based Assessment of hepatic Fat Content[J]. Curr Developments Nutr. 2020;4(12):nzaa171.
Elsayed A, Ismaiel A, Procopio AC, et al. Noninvasive biochemical markers and surrogate scores in evaluating nonalcoholic steatohepatitis[J]. Minerva Med. 2022;113(5):864–74.
Del Chicca F, Schwarz A, Meier D, et al. Non-invasive quantification of hepatic fat content in healthy dogs by using proton magnetic resonance spectroscopy and dual gradient echo magnetic resonance imaging[J]. J Vet Sci. 2018;19(4):570.
Zhao R, Hernando D, Harris DT, et al. Multisite multivendor validation of a quantitative MRI and CT compatible fat phantom[J]. Med Phys. 2021;48(8):4375–86.
Zhang X, Wong GL, Wong VW. Application of transient elastography in nonalcoholic fatty liver disease[J]. Clin Mol Hepatol. 2020;26(2):128–41.
Noureddin M, Ntanios F, Malhotra D, et al. Predicting NAFLD prevalence in the United States using National Health and Nutrition Examination Survey 2017–2018 transient elastography data and application of machine learning[J]. Hepatol Commun. 2022;6(7):1537–48.
Leonard BJ. Nonalcoholic fatty liver Disease[J]. J Diagn Med Sonography. 2012;28(1):43–6.
Kang B, Kim M, Song S et al. Feasibility of modified Dixon MRI techniques for hepatic fat quantification in hepatic disorders: validation with MRS and histology[J]. Br J Radiol, 2017:20170378.
Atteritano M, Mazzaferro S, Bitto A, et al. Genistein effects on quality of life and depression symptoms in osteopenic postmenopausal women: a 2-year randomized, double-blind, controlled study[J]. Osteoporos Int. 2014;25(3):1123–9.
de la Parra C, Castillo-Pichardo L, Cruz-Collazo A, et al. Soy isoflavone genistein-mediated downregulation of miR-155 contributes to the Anticancer effects of Genistein[J]. Nutr Cancer. 2015;68(1):154–64.
Sureda A, Sanches Silva A, Sánchez-Machado DI, et al. Hypotensive effects of genistein: from chemistry to medicine[J]. Chemico-Biol Interact. 2017;268:37–46.
Wang S, Wang Y, Pan M, et al. Anti-obesity molecular mechanism of soy isoflavones: weaving the way to new therapeutic routes[J]. Food Funct. 2017;8(11):3831–46.
Zhang Z, Chen B, Zeng J, et al. Associations between Consumption of Dietary fibers and the risk of type 2 diabetes, hypertension, obesity, Cardiovascular diseases, and mortality in Chinese adults: longitudinal analyses from the China Health and Nutrition Survey[J]. Nutrients. 2022;14(13):2650.
Xu X, Zhang J, Zhang Y et al. Associations between dietary fiber intake and mortality from all causes, cardiovascular disease and cancer: a prospective study[J]. J Translational Med, 2022,20(1).
Zolfaghari H, Askari G, Siassi F, et al. Intake of nutrients, Fiber, and Sugar in patients with nonalcoholic fatty liver disease in comparison to healthy Individuals[J]. Int J Prev Med. 2016;7:98.
Rietman A, Sluik D, Feskens EJM, et al. Associations between dietary factors and markers of NAFLD in a general Dutch adult population[J]. Eur J Clin Nutr. 2018;72(1):117–23.
Xia Y, Zhang S, Zhang Q, et al. Insoluble dietary fibre intake is associated with lower prevalence of newly-diagnosed non-alcoholic fatty liver disease in Chinese men: a large population-based cross-sectional study[J]. Nutr Metab (Lond). 2020;17:4.
Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, et al. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): a population based study[J]. J Hepatol. 2007;47(5):711–7.
Cheng Y, Zhang K, Chen Y et al. Associations between Dietary Nutrient intakes and hepatic lipid contents in NAFLD patients quantified by (1)H-MRS and dual-Echo MRI[J]. Nutrients, 2016,8(9).
Alferink LJ, Kiefte-de Jong JC, Erler NS, et al. Association of dietary macronutrient composition and non-alcoholic fatty liver disease in an ageing population: the Rotterdam Study[J]. Gut. 2019;68(6):1088–98.
Akinbami LJ, Chen TC, Davy O, et al. National Health and Nutrition Examination Survey, 2017-March 2020 Prepandemic file: Sample Design, Estimation, and Analytic Guidelines[J]. Vital Health Stat. 2022;1(190):1–36.
Ahluwalia N, Dwyer J, Terry A, et al. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical considerations, and uses to inform Public Policy[J]. Adv Nutr. 2016;7(1):121–34.
Ahuja JKC, Moshfegh AJ, Holden JM, et al. USDA Food and Nutrient Databases Provide the Infrastructure for Food and Nutrition Research, Policy, and Practice[J]. J Nutr. 2013;143(2):S241–9.
Eddowes PJ, Sasso M, Allison M, et al. Accuracy of FibroScan Controlled Attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver Disease[J]. Gastroenterology. 2019;156(6):1717–30.
Xie R, Liu M. Relationship between non-alcoholic fatty liver disease and degree of hepatic steatosis and bone Mineral Density[J]. Front Endocrinol (Lausanne). 2022;13:857110.
Yang N, Lu Y, Cao L, et al. The association between non-alcoholic fatty liver disease and serum ferritin levels in American adults[J]. J Clin Lab Anal. 2022;36(2):e24225.
Xie R, Xiao M, Li L, et al. Association between SII and hepatic steatosis and liver fibrosis: a population-based study[J]. Front Immunol. 2022;13:925690.
Brockman DA, Chen X, Gallaher DD. High-viscosity dietary fibers reduce adiposity and decrease hepatic steatosis in rats fed a high-fat diet[J]. J Nutr. 2014;144(9):1415–22.
Zheng M, Yang X, Wu Q, et al. Butyrate attenuates hepatic Steatosis Induced by a High-Fat and Fiber-Deficient Diet via the hepatic GPR41/43-CaMKII/HDAC1-CREB Pathway[J]. Mol Nutr Food Res. 2023;67(1):e2200597.
Noguchi Y, Nishikata N, Shikata N, et al. Ketogenic essential amino acids modulate lipid synthetic pathways and prevent hepatic steatosis in mice[J]. PLoS ONE. 2010;5(8):e12057.
Grover GJ, Koetzner L, Wicks J, et al. Effects of the Soluble Fiber Complex PolyGlycopleX on glucose homeostasis and body weight in Young Zucker Diabetic Rats[J]. Front Pharmacol. 2011;2:47.
Schoeler M, Ellero-Simatos S, Birkner T, et al. The interplay between dietary fatty acids and gut microbiota influences host metabolism and hepatic steatosis[J]. Nat Commun. 2023;14(1):5329.
Zhu W, Zhou Y, Tsao R, et al. Amelioratory Effect of resistant starch on non-alcoholic fatty liver Disease via the Gut-Liver Axis[J]. Front Nutr. 2022;9:861854.
Zhao H, Yang A, Mao L et al. Association between Dietary Fiber Intake and non-alcoholic fatty liver disease in Adults[J]. Frontiers in Nutrition, 2020,7.
Dong Y, Chen L, Gutin B, et al. Total, insoluble, and soluble dietary fiber intake and insulin resistance and blood pressure in adolescents[J]. Eur J Clin Nutr. 2019;73(8):1172–8.
Song M, Yuan F, Li X et al. Analysis of sex differences in dietary copper-fructose interaction-induced alterations of gut microbial activity in relation to hepatic steatosis[J]. Biology Sex Differences, 2021,12(1).
Acknowledgements
We thank the staff at the National Center for Health Statistics of the Centers for Disease Control for designing, collecting, and collating the NHANES data and creating the public database.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to this article. XC: Data curation, Investigation, Methodology, Software, Writing – original draft. YW: Methodology, Project administration, Writing – original draft. LF: Investigation, Writing – review & editing. ZZ: Project administration, Writing – review & editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by CDC’s National Center for Health Statistics Institutional Research Ethics Review Board. The patients/participants provided their written informed consent to participate in this study. All our methods followed the guidelines of the Helsinki Declaration. And secondary analysis does not require additional institutional review committee approval.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, X., Fu, L., Zhu, Z. et al. Exploring the association between dietary fiber intake and hepatic steatosis: insights from NHANES. BMC Gastroenterol 24, 160 (2024). https://doi.org/10.1186/s12876-024-03256-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-024-03256-1