
Abstract
Objective
To evaluate the efficacy and safety of the combination of camrelizumab and apatinib in the treatment of liver cancer and to furnish clinical recommendations for pharmacological interventions.
Methods
PubMed, Embase, Web of Science and the Cochrane Library were scrutinized for research publications from their inception to 22 December 2023. Bibliographic perusal and data procurement were executed. The quality of the included studies was evaluated employing the MINORS tool. Meta-analysis was conducted utilizing Stata 15.0 software.
Results
A total of 10 studies involving 849 patients were included in the meta-analysis. The study revealed that the objective response rate (ORR) of the combined therapy was 28% (95% CI: 23%-34%), the disease control rate (DCR) was 69% (95% CI: 64%-73%), the median progression-free survival (mPFS) was 5.87 months (95% CI: 4.96–6.78), the median overall survival (mOS) was 19.35 months (95% CI: 17.53–21.17), the incidence of any grade adverse events was 90% (95% CI: 85%-95%), and the occurrence of grade 3 or higher adverse events was 49% (95% CI: 27%-71%).
Conclusion
The combination of camrelizumab and apatinib exhibits commendable effectiveness in the management of liver cancer; nevertheless, vigilance should be exercised concerning potential adverse reactions in clinical applications to enhance the safety of pharmacological interventions.
Similar content being viewed by others

Introduction
Liver cancer constitutes one of the most prevalent malignant neoplasms globally, ranking 6th in incidence amidst all cancers and 3rd in fatalities, exhibiting the most accelerated escalation in mortality throughout the past several decades [1,2,3]. Hepatocellular carcinoma accounts for the highest proportion of liver cancer cases, ranging from 75 to 85% [4, 5]. The onset of liver cancer is often latent, and the preponderance of patients have already advanced to intermediate or progressive stages at the time of initial detection, thereby losing the prospects for surgical intervention and localized therapy. Systemic pharmacological intervention typically constitutes the sole recourse, and the swift advancement of immune checkpoint inhibitors (ICIs) has introduced novel therapeutic alternatives and engendered optimism for patients afflicted with intermediate and advanced liver cancer [6,7,8]. Nonetheless, studies [9, 10] have ascertained that the impact of ICI monotherapy on hepatic neoplasms is less than optimal, thereby inciting inquiries into concomitant therapy with molecularly targeted pharmaceuticals. Targeted agents reconfigure the neoplastic immune microenvironment, efficaciously amplifying the potency of immunotherapy and yielding a synergistic outcome [11, 12]. The initial clinical ramifications of the conjunction of the immune checkpoint inhibitor camrelizumab and the antiangiogenic inhibitor apatinib have manifested as auspicious, and this strategy has surfaced as a novel trajectory in the therapeutic landscape of hepatic malignancies. Camrelizumab, a programmed cell death receptor-1 (PD-1) inhibitor, operates by impeding the interplay between PD-1 and its cognate ligand, programmed cell death ligand-1 (PD-L1), subsequently interrupting the immunosuppressive pathway exploited by malignant entities. This revitalizes the immunological response, reestablishes immune surveillance capabilities, and generates sustained anti-neoplastic effects. At present, camrelizumab has exhibited propitious results in the clinical handling of classical Hodgkin's lymphoma, hepatocellular carcinoma, pulmonary neoplasms, and esophageal squamous cell carcinoma [13, 14]. Apatinib, a vascular endothelial growth factor receptor-2 (VEGFR-2) antagonist, functions by impeding the phosphorylation of VEGFR-2, thereby attenuating downstream signalling cascades and curbing tumour angiogenesis to exert its anti-neoplastic properties. This agent has demonstrated promising therapeutic outcomes in advanced gastric adenocarcinoma, gastroesophageal junction adenocarcinoma, and hepatocellular carcinoma [15, 16]. Presently, emerging clinical investigations suggest that the combination therapy of camrelizumab and apatinib may offer certain advantages in the clinical management of liver cancer [15, 16]. However, the precise therapeutic efficacy and safety profile of this regimen remain to be conclusively established [17]. Consequently, this study conducted a comprehensive systematic review and meta-analysis to evaluate the efficacy and safety of camrelizumab in conjunction with apatinib for the treatment of liver cancer, with the aim of providing evidence-based guidance for clinical practice.
Materials and methodology
Literature search
The search encompassed databases such as PubMed, Embase, Web of Science, the Cochrane Library, and ClinicalTrials.gov, spanning from their inception to 22 December 2023. Search terms incorporated "Hepatocellular Carcinomas", "Liver Cancer", "Liver Cell Carcinoma", "camrelizumab", "SHR-1210", "apatinib", "rivoceranib" and "YN-968D1", utilizing both MeSH terms and free-text queries.
We have applied for the PROSPERO registration (CRD42023442948).
Inclusion and exclusion criteria
Inclusion criteria
(1) Eligible patients were aged 18 years or older with histopathologically or cytologically confirmed hepatocellular carcinoma or radiologically assessed by enhanced computed tomography or magnetic resonance imaging combined with detection of serum tumour markers; (2) The intervention under investigation is the combined treatment of camrelizumab and apatinib; (3) Studies must report efficacy endpoints and adverse events, encompassing an objective response rate (ORR), disease control rate (DCR), median overall survival (mOS), median progression-free survival (mPFS),adverse events (AEs) and grade 3 or higher adverse events (AEs); (4) Study designs comprise randomised control trials, non-randomised control trials and single-arm studies, etc.
Exclusion criteria
(1) Animal and in vitro experiments, basic research; (2) Conference abstracts, reviews, commentaries, case reports; (3) Aggregate reporting of results from multiple populations or disease cohorts; (4) Duplicate publications; (5) Literature from which valid outcome data cannot be extracted.
Data extraction
Two investigators independently assessed the titles and abstracts of identified publications, performing full-text analysis on eligible articles to determine their final inclusion. Disagreements were resolved through discussions involving a third reviewer. Key information extracted from the original studies encompassed: (1) basic information about the included studies, such as author details, publication dates, and study design; (2) fundamental characteristics of study participants, including total sample size and age and gender distribution of enrolled cases; (3) specific intervention approaches and follow-up durations; (4) pertinent outcome measures; (5) information required for literature quality appraisal.
Literature quality assessment
Given that the most included studies were single-arm trials, the Methodological Index for Non-Randomized Studies (MINORS) assessment criteria were employed for literature quality evaluation [18]. The assessment entailed 12 indicators, with the first eight (I-VIII) pertaining to single-arm studies without a control group. The numbers I-VIII in the assessment criteria mean: I, a clearly stated objective; II, inclusion of consecutive patients; III, prospective data collection; IV, endpoints appropriate to the objective of the study; V, unbiased assessment of the study endpoint; VI, follow-up period appropriate to the study objective; VII, loss to follow-up less than 5%;VIII, prospective calculation of study size. Each indicator was scored on a scale of 0–2 points: 0 points denoted non-reporting, 1 point signified reported but with insufficient information and 2 points indicated reported with adequate information, and a very objective assessment of each indicator was made. A final score of 13–16 points indicated high-quality studies, and 9–12 points denoted medium-quality studies. According to the MINORS appraisal instrument, this meta-analysis incorporated solely literature of intermediate to high quality.
Statistical analysis methods
Stata 15.0 software was utilized to perform the statistical analysis of the extracted data. The odds ratio (OR) was used for dichotomous variables and the mean difference (MD) was used as the combined effect statistic for continuous variables. The effect size of all pooled results was reported as a 95% confidence interval (CI) with upper and lower limits. The heterogeneity of the included studies was assessed using I2 and Cochran's Q test. A fixed-effects model was implemented for analysis when I2 ≤ 50% and P ≥ 0.1. In contrast, when I2 > 50% and P < 0.1, indicating significant study heterogeneity, a random-effects model was adopted for analysis. The sensitivity analysis was performed for the pooled results with high heterogeneity. In addition, meta-regression is used to further explore the sources of heterogeneity. The collective findings were visually depicted using forest plots. The potential publication bias was scrutinized utilizing Egger's test, with a P > 0.05, suggesting an absence of significant publication bias.
Results
Retrieval results and fundamental characteristics of the literature
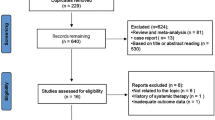
The search in collective databases yielded a total of 293 pertinent articles. After rigorous screening based on the inclusion and exclusion criteria, 92 duplicates were removed. Furthermore, based on a thorough assessment of their titles and abstracts, an additional 177 irrelevant articles were discarded. Ultimately, ten articles [19,20,21,22,23,24,25,26,27,28]were deemed eligible for analysis following a meticulous examination of their full text. The detailed flowchart outlining the literature screening process is demonstrated in Fig. 1, while the essential characteristics of the selected articles are comprehensively depicted in Table 1.

PRISMA flow diagram of the study process. PRISMA, Preferred Reporting Items for Systematic review and Meta-analysis
Literature quality assessment
The most included articles were single-arm studies; thus, the MINORS criteria were employed for quality assessment. The results of the quality evaluation are presented in Table 2.
Therapeutic efficacy indicators
Objective Response Rate (ORR)
In total, 10 publications were incorporated, encompassing 849 patients, with 239 individuals attaining objective disease remission. The aggregated analysis indicated that the ORR of camrelizumab combined with apatinib for liver cancer was 28% (95% CI: 23%-34%, I2 = 56.9%, p = 0.013), as depicted in Fig. 2A. As I2 = 56.9% > 50%, the random effects model was selected for the analysis, and the sensitivity analysis was continued to test the source of heterogeneity, the results of the sensitivity analysis showed good stability of the study, as shown in Fig. 2B. Moreover, a supplementary subgroup analysis of the objective remission by first-line and second-line therapies was performed. The findings revealed that the ORR for camrelizumab combined with apatinib as a first-line intervention was 30% (95% CI: 25%-36%, I2 = 37.7%, p = 0.170), while for second-line therapy, it was 22% (95% CI: 13%-30%, I2 = 43.3%, p = 0.133), as illustrated in Fig. 2C, suggesting that this combined strategy exhibits a higher objective remission rate when employed as first-line treatment for liver cancer.

A Forest plot delineating ORR of camrelizumab in combination with apatinib for liver cancer treatment; B Sensitivity analysis on ORR of camrelizumab in combination with apatinib for liver cancer treatment; C Forest plot of subgroup analysis on ORR of camrelizumab in combination with apatinib as first-line or second-line therapy for liver cancer
Disease Control Rate (DCR)
Altogether, 6 articles comprising 7 research groups were included (Zhiming Zeng (2021) was subdivided into first-line and second-line treatment cohorts), totalling 345 patients, with 234 individuals exhibiting controlled disease progression. The aggregated analysis revealed that the DCR of camrelizumab combined with apatinib for liver cancer treatment was 69% (95% CI: 64%-73%, I2 = 30.5%, p = 0.195), as depicted in Fig. 3A.

A Forest plot illustrating DCR of camrelizumab combined with apatinib for liver cancer treatment; B Forest plot delineating mPFS of camrelizumab in combination with apatinib for liver cancer treatment; C Sensitivity analysis on mPFS of camrelizumab in combination with apatinib for liver cancer treatment; D Forest plot illustrating mOS of camrelizumab combined with apatinib for liver cancer treatment
Median Progression-Free Survival (mPFS)
In total, 6 articles encompassing 7 research groups were incorporated (Jianming Xu (2021) was categorized into first-line and second-line treatment cohorts), and the aggregated analysis indicated that the mPFS of camrelizumab combined with apatinib for liver cancer treatment was 5.87 months (95% CI: 4.96–6.78, I2 = 73.1%, p = 0.001), as illustrated in Fig. 3B. As I2 = 73.1%, we selected the random effects model for the analysis and continued the sensitivity analysis to test the source of heterogeneity. The results of the sensitivity analysis showed good stability of the analysis, as shown in Fig. 3C.
Median Overall Survival (mOS)
Three studies were incorporated into the statistical analysis, and the results demonstrated that the mOS of camrelizumab combined with apatinib for liver cancer treatment was 19.35 months (95% CI: 17.53–21.17, I2 = 49.7%, p = 0.137), as depicted in Fig. 3D.
Safety
A comprehensive analysis of the adverse reaction incidence rates for liver cancer treatment utilizing camrelizumab combined with apatinib was conducted, encompassing 6 articles and a total of 674 patients. Among them, 622 patients encountered general adverse reactions, with an occurrence rate of 90% (95% CI: 85%-95%, I2 = 92.8%, p = 0.000); 455 patients experienced grade 3 or higher adverse reactions, with an incidence rate of 49% (95% CI: 27%-71%, I2 = 97.7%, p = 0.000), as delineated in Table 3. Due to the high level of heterogeneity, we performed meta-regression analyses by study design, which showed any grade AEs (p = 0.939) and grade 3 or higher AEs (p = 0.229), as delineated in Table 4, indicating that study design covariate was not significantly associated with PFS and OS and other factors may be at play. Predominantly, the general adverse reactions with a higher incidence encompass Thrombocytopenia (51%, 95% CI: 41%-62%, I2 = 71.3%, p = 0.031), Hypertension (45%, 95% CI: 27%-62%,I2 = 95.6%, p = 0.000), and Hand-foot skin reaction (45%, 95% CI: 33%-57%, I2 = 84.1%, p = 0.000), in addition to Leukopenia (40%), Proteinuria (37%), Abdominal pain (34%), Diarrhea (31%), Hepatotoxicity (24%), Fever (20%), Hypothyroidism (20%), RCCEP (19%), Rash (18%), Fatigue (17%), and Nausea and vomiting (11%), as delineated in Table 3. Primarily, severe adverse reactions with a higher incidence include Hypertension (19%, 95% CI: 4%-34%, I2 = 98.5%, p = 0.000), Thrombocytopenia (9%, 95% CI: 1%-17%, I2 = 88.7%, p = 0.000), and Hand-foot skin reaction (6%, 95% CI: 3%-9%, I2 = 32.4%, p = 0.218), along with Proteinuria (5%), Hepatotoxicity (3%), Abdominal pain (2%), Diarrhea (2%), and Rash (1%), as portrayed in Table 3.
Publication bias analysis
An analysis of publication bias was executed on the incorporated studies utilizing the Egger test. The results revealed that ORR (p = 0.268), DCR (p = 0.068), mPFS (p = 0.469), mOS (p = 0.828), incidence of general adverse reactions (p = 0.420), and incidence of ≥ 3-grade adverse reactions (p = 0.250) conformed to the criterion of p > 0.05. This implies that no significant publication bias exists within the study.
All of the above results are summarised in Table 5.
Discussion
In recent years, the burgeoning development of immunosuppressive agents has ushered liver cancer treatment into a new epoch of immunotherapy [29]. Particularly, the collaborative strategy with antivascular targeted therapy has demonstrated promising application potential in liver cancer clinical treatment, offering new therapeutic hopes for patients afflicted with liver cancer [30,31,32,33]. Research indicates that the synergy between immunotherapy and anti-vascular targeted therapy yields an augmented antitumor effect [34, 35]. Anti-angiogenic drugs can facilitate the infiltration and activation of immune cells within tumours, mediate the upregulation of IFNγ, enhance the expression of PD-1 and PD-L1, boost the sensitivity of immunotherapy within tumours, alter the M1/M2 ratio of tumour-associated macrophages, diminish the infiltration of regulatory T cells and monocytes in tissues, restructure the tumour immune microenvironment, and effectively elevate the efficacy of immunotherapy [11, 12]. Furthermore, immunosuppressive agents may trigger the recruitment of immune subpopulations possessing vascular regulatory activity, potentially serving as a target for anti-angiogenic treatment [36]. Consequently, the combined utilization of both can ameliorate the local vascular microenvironment, effectively eradicate tumour cells, and jointly enhance clinical treatment outcomes. Among these, the PD-1 inhibitor camrelizumab combined with the VEGFR-2 inhibitor apatinib has exhibited favourable treatment prospects in the clinical management of liver cancer.
Through a comprehensive analysis of the ten incorporated articles in this study, it was discovered that the clinical efficacy of camrelizumab combined with apatinib in treating liver cancer is commendable. This combination not only yields satisfactory objective remission rates and disease control rates but also provides patients with significant benefits in terms of median progression-free survival and median overall survival. Moreover, through an in-depth subgroup analysis, it was discerned that the objective remission rate of the combined regimen as first-line therapy was considerably higher compared to second-line therapy. On the one hand, this could be attributed to the diminished functional status of patients when their second-line treatment was adopted, which results in a lower tolerable drug dosage, thereby directly reducing the therapeutic effect of the combined regimen. On the other hand, prior treatment may render the immune microenvironment within the patient’s body increasingly complex. For instance, if first-line treatment has already involved immunosuppressive agents, it might lead to the development of drug-resistant antibodies, engendering resistance to immunotherapy [37] and subsequently weakening the therapeutic effect of second-line medications. Nonetheless, due to the limited number of studies presently incorporated in the analysis, the research findings necessitate more clinical trial data and a larger sample size for validation and substantiation.
The results of CARES-310, a global phase 3 randomized open-label trial on camrelizumab plus apatinib indicate that this combination therapy presents a promising first-line treatment option for unresectable HCC with a positive benefit-to-risk profile. This study is the first to report significant benefits in progression-free survival and overall survival with the combination of an anti-PD-1 antibody and an oral small molecule anti-angiogenic agent as first-line treatment for unresectable HCC, compared to sorafenib. However, it is important to acknowledge the limitations of this study, including its open-label design and the fact that the majority of participants were from Asia and had hepatocellular carcinoma of viral aetiology. Further research is required to confirm the effectiveness of the treatment in other patient subgroups [27]. Although camrelizumab in combination with apatinib in the treatment of HCC has achieved a high probability of being the most effective treatment in terms of both OS and PFS, more direct comparative research analysis with existing standard first-line treatments is needed in the future [38, 39]. Furthermore, in the analysis of adverse reactions, it was ascertained that the overall safety profile of the combined regimen is generally acceptable. However, it may also provoke the risk of adverse reactions in patients, such as thrombocytopenia, hypertension, and hand-foot skin reaction. Meanwhile, immune-related adverse events such as liver damage also deserve clinical attention. Immune-related liver injury during treatment with ICI is relatively common in patients with HCC and is often detected by elevated ALT/AST levels [40]. Therefore, it is crucial to closely monitor relevant clinical symptoms and indicators through a more comprehensive clinical examination, such as cardiovascular function tests, routine blood tests and liver function tests, etc., so that the physician can adjust the dosage of the drug and undertake appropriate interventions to ensure clinical efficacy and safety. In addition, multidisciplinary management, which requires integrated collaboration between the specialties involved in the management of patients with HCC, is valuable. For example, treatment for HCC patients is administered after multidisciplinary assessment and according to the practice of participating institution, and continued until disease progression or unacceptable toxicity. Toxicity management, including dose modification, is performed in accordance with the summary of product characteristics for the agents [40]. The development of multidisciplinary care for HCC patients is essential to optimise the management of treatment side effects and improve patient outcomes.While this study endeavoured to incorporate as many pertinent studies as possible that fulfil the criteria, it still exhibits the following limitations: 1. Variations in disease subtypes, medication dosage, sample size, follow-up duration, and statistical methods contribute to increased research heterogeneity; 2. It is unable to acquire comprehensive data for additional subgroup analyses; 3. Some included studies have a brief follow-up period, not attaining overall survival (OS) and progression-free survival (PFS); 4. The most included studies are single-arm trials with smaller sample sizes, necessitating larger-scale, multicentre, randomized controlled clinical trials for combined analysis and evaluation, with the aim of providing more objective and efficacious evidence-based medicine for clinical treatment.
Conclusion
In conclusion, camrelizumab in combination with apatinib shows a favourable therapeutic effect and a manageable safety profile in HCC. Further investigation can delve into the effective biomarkers of this combined regimen, identify the optimal treatment population, and thus achieve precision and individualization in liver cancer therapy. Simultaneously, it may be worthwhile to explore combining this treatment with surgical procedures, radiofrequency ablation, and interventional therapies to afford liver cancer patients a broader array of treatment options and opportunities, thereby harnessing its clinical potential and value.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30.
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49.
Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, Lencioni R, Koike K, Zucman-Rossi J, Finn RS. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6.
Singal AG, Lampertico P, Nahon P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. J Hepatol. 2020;72(2):250–61.
Llovet JM, Castet F, Heikenwalder M, Maini MK, Mazzaferro V, Pinato DJ, Pikarsky E, Zhu AX, Finn RS. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19(3):151–72.
Pinter M, Jain RK, Duda DG. The current landscape of immune checkpoint blockade in hepatocellular carcinoma: a review. JAMA Oncol. 2021;7(1):113–23.
Sangro B, Sarobe P, Hervás-Stubbs S, Melero I. Advances in immunotherapy for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(8):525–43.
Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, Breder V, Edeline J, Chao Y, Ogasawara S, et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J Clin Oncol. 2020;38(3):193–202.
Yau T, Park JW, Finn RS, Cheng AL, Mathurin P, Edeline J, Kudo M, Han KH, Harding JJ, Merle P, et al. CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2019;30:874-+.
Lee WS, Yang H, Chon HJ, Kim C. Combination of anti-angiogenic therapy and immune checkpoint blockade normalizes vascular-immune crosstalk to potentiate cancer immunity. Exp Mol Med. 2020;52(9):1475–85.
Shigeta K, Datta M, Hato T, Kitahara S, Chen IX, Matsui A, Kikuchi H, Mamessier E, Aoki S, Ramjiawan RR, et al. Dual programmed death receptor-1 and vascular endothelial growth factor receptor-2 blockade promotes vascular normalization and enhances antitumor immune responses in hepatocellular carcinoma. Hepatology (Baltimore, MD). 2020;71(4):1247–61.
Markham A, Keam SJ. Camrelizumab: first global approval. Drugs. 2019;79(12):1355–61.
Mo H, Huang J, Xu J, Chen X, Wu D, Qu D, Wang X, Lan B, Wang X, Xu J, et al. Safety, anti-tumour activity, and pharmacokinetics of fixed-dose SHR-1210, an anti-PD-1 antibody in advanced solid tumours: a dose-escalation, phase 1 study. Br J Cancer. 2018;119(5):538–45.
Scott LJ. Apatinib: A Review in Advanced Gastric Cancer and Other Advanced Cancers. Drugs. 2018;78(7):747–58.
Zhao D, Hou H, Zhang X. Progress in the treatment of solid tumors with apatinib: a systematic review. Onco Targets Ther. 2018;11:4137–47.
Bai X, Chen Y, Zhang X, Zhang F, Liang X, Zhang C, Wang X, Lu B, Yu S, Liang T. CAPT: A multicenter randomized controlled trial of perioperative versus postoperative camrelizumab plus apatinib for resectable hepatocellular carcinoma. Ann Oncol. 2022;33(7):S868–S868.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6.
Xu JM, Zhang Y, Jia R, Yue CY, Chang LP, Liu RR, Zhang GR, Zhao CH, Zhang YY, Chen CX, et al. Anti-PD-1 Antibody SHR-1210 Combined with Apatinib for Advanced Hepatocellular Carcinoma, Gastric, or Esophagogastric Junction Cancer: An Open-label, Dose Escalation and Expansion Study. Clin Cancer Res. 2019;25(2):515–23.
Ju S, Zhou C, Yang C, Wang C, Liu J, Wang Y, Huang S, Li T, Chen Y, Bai Y, et al. Apatinib Plus Camrelizumab With/Without Chemoembolization for Hepatocellular Carcinoma: a real-world experience of a single center. Front Oncol. 2021;11:835889.
Xu J, Shen J, Gu S, Zhang Y, Wu L, Wu J, Shao G, Zhang Y, Xu L, Yin T, et al. Camrelizumab in Combination with Apatinib in Patients with Advanced Hepatocellular Carcinoma (RESCUE): A Nonrandomized, Open-label, Phase II Trial. Clin Cancer Res. 2021;27(4):1003–11.
Mei KM, Qin SK, Chen ZD, Liu Y, Wang LN, Zou JJ. Camrelizumab in combination with apatinib in second-line or above therapy for advanced primary liver cancer: cohort A report in a multicenter phase Ib/II trial. J Immunother Cancer. 2021;9(3):e002191.
Zeng Z, Jiang Y, Liu C, Zhu G, Ma F, Yang L, Qiu J, Tang J, Ye X, Peng T, et al. Efficacy and biomarker exploration of camrelizumab combined with apatinib in the treatment of advanced primary liver cancer: a retrospective study. Anticancer Drugs. 2021;32(10):1093–8.
Xia Y, Tang W, Qian X, Li X, Cheng F, Wang K, Zhang F, Zhang C, Li D, Song J, et al. Efficacy and safety of camrelizumab plus apatinib during the perioperative period in resectable hepatocellular carcinoma: a single-arm, open label, phase II clinical trial. J Immunother Cancer. 2022;10(4):e004656.
Yuan G, Li R, Li Q, Hu X, Ruan J, Fan W, Wang J, Huang W, Zang M, Chen J. Interaction between hepatitis B virus infection and the efficacy of camrelizumab in combination with apatinib therapy in patients with hepatocellular carcinoma: a multicenter retrospective cohort study. Ann Transl Med. 2021;9(18):1412.
Yuan GS, Cheng X, Li Q, Zang MY, Huang W, Fan WZ, Wu T, Ruan J, Dai WC, Yu WX, et al. Safety and Efficacy of Camrelizumab Combined with Apatinib for Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: a multicenter retrospective study. Onco Targets Ther. 2020;13:12683–93.
Qin S, Chan SL, Gu S, Bai Y, Ren Z, Lin X, Chen Z, Jia W, Jin Y, Guo Y, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;402(10408):1133–46.
Chen D, Chen X, Xu L, Wang Y, Zhu L, Kang M. Camrelizumab combined with apatinib in the treatment of patients with hepatocellular carcinoma: a real-world assessment. Neoplasma. 2023;70(4):580–7.
Dual Immunotherapy Makes Strides against HCC. Cancer Discov. 2022;12(4):OF1. https://doi.org/10.1158/2159-8290.CD-NB2022-0008.
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382(20):1894–905.
Galle PR, Finn RS, Qin S, Ikeda M, Zhu AX, Kim TY, Kudo M, Breder V, Merle P, Kaseb A, et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma (IMbrave150): an open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(7):991–1001.
Pinato DJ, Fessas P, Cortellini A, Rimassa L. Combined PD-1/VEGFR Blockade: a New Era of treatment for hepatocellular cancer. Clin Cancer Res. 2021;27(4):908–10.
Yi M, Jiao DC, Qin S, Chu Q, Wu KM, Li AP. Synergistic effect of immune checkpoint blockade and anti-angiogenesis in cancer treatment. Mol Cancer. 2019;18:60.
Ciccarese C, Iacovelli R, Porta C, Procopio G, Bria E, Astore S, Cannella MA, Tortora G. Efficacy of VEGFR-TKIs plus immune checkpoint inhibitors in metastatic renal cell carcinoma patients with favorable IMDC prognosis. Cancer Treat Rev. 2021;100:102295.
Saeed A, Park R, Sun W. The integration of immune checkpoint inhibitors with VEGF targeted agents in advanced gastric and gastroesophageal adenocarcinoma: a review on the rationale and results of early phase trials. J Hematol Oncol. 2021;14(1):13.
Goedegebuure RSA, de Klerk LK, Bass AJ, Derks S, Thijssen V. Combining Radiotherapy with anti-angiogenic therapy and immunotherapy; a therapeutic triad for cancer? Front Immunol. 2018;9:3107.
Enrico D, Paci A, Chaput N, Karamouza E, Besse B. Antidrug Antibodies Against Immune Checkpoint Blockers: Impairment of Drug Efficacy or Indication of Immune activation? Clin Cancer Res. 2020;26(4):787–92.
Yang Q, Li G, Wu X, Lin H, Wu W, Xie X, Zhu Y, Cai W, Shi C, Zhuo S. A novel therapeutic strategy of combined camrelizumab and apatinib for the treatment of advanced hepatocellular carcinoma. Front Oncol. 2023;13:1136366.
Celsa C, Cabibbo G, Pinato D, Maria G, Enea M, Vaccaro M: Balancing efficacy and tolerability of first-line systemic therapies for advanced hepatocellular carcinoma: a network metanalysis. Liver Cancer. 2023. https://doi.org/10.1159/000531744.
Celsa C, Cabibbo G, Fulgenzi CAM, Scheiner B, D’Alessio A, Manfredi GF, Nishida N, Ang C, Marron TU, Saeed A, et al. Characteristics and outcomes of immunotherapy-related liver injury in patients with hepatocellular carcinoma versus other advanced solid tumours. J Hepatol. 2023;S0168–8278(23):05272–8.
Acknowledgements
Not applicable.
Funding
The authors declare that they did not receive any funding from any source.
Author information
Authors and Affiliations
Contributions
Conceptualization: [Min Chen, Minyu Cheng]; Methodology: [Min Chen, Yanglei Li]; Formal analysis and investigation: [Min Chen, Yanglei Li]; Writing—original draft preparation: [Min Chen]; Writing—review and editing: [Min Chen, Yanglei Li]; Resources: [Min Chen, Minyu Cheng]; Supervision: [Minyu Cheng]And all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All analyses were based on previously published studies. Thus no ethical approval and patient consent are required.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, M., Li, Y. & Cheng, M. Efficacy and safety of the combination of camrelizumab and apatinib in the treatment of liver cancer: a systematic review and single-arm meta-analysis. BMC Gastroenterol 24, 55 (2024). https://doi.org/10.1186/s12876-024-03144-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-024-03144-8