
Abstract
Background
Inoperable hepatocellular carcinoma (HCC) is treated by conventional transarterial chemoembolization (cTACE) using cone-beam computed tomography (CBCT) or digital subtraction angiography (DSA). We compared patient survival outcomes between CBCT-cTACE with automated tumor-feeder detection (AFD) software and DSA-cTACE alone in inoperable HCC patients.
Methods
We reviewed the data of 337 HCC patients treated by CBCT-cTACE or DSA-cTACE between January 2015 and December 2019. Treatment response, progression-free survival (PFS), overall survival (OS), and complications between the CBCT-cTACE and DSA-cTACE groups were compared. Univariate and multivariate logistic regression analyses examined the potential prognostic factors affecting survival after chemoembolization.
Results
Tumor response rates in complete response, partial response, and stable disease at 1 month were 67%, 28%, and 4% in the CBCT-cTACE group and 22%, 48%, and 9% in the DSA-cTACE group, respectively. OS rates of patients in the CBCT-cTACE versus DSA-cTACE groups were 87% versus 54%, 44% versus 15%, and 34% versus 7% at 1, 3, and 5 years, respectively. The CBCT-cTACE group had significantly improved PFS (p < 0.001) and OS (p < 0.001). Multivariate analysis showed that CBCT with AFD software was an independent factor associated with longer OS (hazard ratio, 0.38; p < 0.001).
Conclusions
Compared with conventional DSA, combining selective cTACE with CBCT and AFD software leads to better tumor response and prolongs OS in patients with inoperable HCC.
Similar content being viewed by others


Background
Conventional transarterial chemoembolization (cTACE) is the standard treatment in patients with inoperable hepatocellular carcinoma (HCC), especially in Barcelona Clinic Liver Cancer (BCLC) stage B (intermediate stage) [1,2,3]. It is crucial to perform selective catheterization of all tumor-feeding arteries and precisely administer chemotherapeutic drugs and iodized oil to the tumor for effective cTACE. However, inoperable stage HCC varies in terms of tumor size, number of tumor nodules, and complex multiple hepatic arterial branches that require multiple angiographic runs. Two-dimensional digital subtraction angiography (DSA) is routinely used for cTACE procedures to identify the tumor-feeding branches and for tumor targeting. However, conventional DSA has some limitations in terms of identifying small tumor nodules and their feeding-arteries. Furthermore, DSA does not accurately assess accumulation of the iodized oil inside the tumors that might affect tumor recurrence and prognostic outcome [4, 5].
Nowadays, C-arm cone-beam computed tomography (CBCT) is a valuable tool for obtaining three-dimensional images providing additional information including visualization of subtle tumor nodules, tiny hepatic feeding arteries, extrahepatic collateral arteries, and to monitor the embolized area during the cTACE procedure [6,7,8,9]. Iwazawa et al. [10] reported that CBCT in addition to DSA during cTACE can prolong survival in unresectable HCC patients.
Automated tumor-feeder detection (AFD) software is a new promising technology for the identification of intrahepatic and extrahepatic tumor-feeding arteries using CBCT data. The rates of identifying tumor-feeding arteries by AFD software were reported to be from 88 to 90% higher than using DSA guidance [7, 11, 12]. Accordingly, CBCT with AFD software has become an essential tool for performing cTACE safely and effectively in the treatment of liver tumors. To our knowledge, the efficacy of intraprocedural CBCT with AFD software assisted cTACE on survival outcome in unresectable HCC patients has not been identified in the literature. Therefore, for the first time, we retrospectively compared the survival outcome in patients who underwent CBCT using AFD software assisted cTACE and patients who underwent cTACE using DSA alone. We also evaluated the prognostic factors affecting the survival in HCC patients.
Methods
Ethics statement
This study complies with the standards of the Declaration of Helsinki and current ethical guidelines, and approval was obtained from the institutional ethics committee (REC No. 64-257-7-1). The requirement for informed consent for this study was waived by the Institutional Review Board, and all the data were analyzed anonymously.
Patient population
We followed the American Association for the Study of Liver Disease criteria for the diagnosis of HCC [13]. Hepatic lesions larger than 1 cm were assessed by multiphasic contrast-enhanced computed tomography (CT) or dynamic magnetic resonance imaging (MRI). If the imaging characteristics were the typical appearance of HCC, no further diagnostic procedure was attempted.
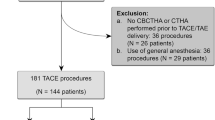
The data of 337 HCC patients treated with selective cTACE between January 2015 and December 2019 at our hospital were collected for this study. Eligible patients for inclusion included: (1) patients aged > 18 years, (2) HCC patients with tumor size ≤ 7 cm in diameter and the number of nodules ≤ 5, (3) patients ineligible for surgical resection or transplantation, (4) patients treated with selective cTACE, and (5) patients who underwent imaging examination by either dynamic MRI or 4-phase contrast-enhanced CT scan within one month after the initial procedure. The excluded patients were those with severe impaired hepatic function (Child–Pugh class C), extrahepatic metastasis, concomitant malignancy, severe arterioportal shunt, history of spontaneous tumor rupture, presence of vascular invasion, and cotreatment with any systemic or locoregional therapies during the cTACE session.
Of the 337 HCC patients included in this study, 141 underwent cTACE using DSA alone and 196 underwent cTACE with CBCT (with or without AFD software) between January 2015 and December 2019. We assigned our patients to each technique on the basis of a discussion with interventional radiology staff. To minimize selection bias, patients treated by both techniques (i.e., first treated by cTACE with DSA alone and subsequently underwent cTACE by CBCT) were excluded from this study.
Selective cTACE protocols
All HCC patients underwent selective cTACE using an angiographic system (Allura Clarity FD20, Philips Healthcare, Eindhoven, the Netherlands) under the supervision of two interventional radiologists with more than 8 years of experience in body interventional radiology through the transfemoral route. Celiac and superior mesenteric arteries were selected at the beginning of the procedure using a 5-Fr diagnostic catheter and a 0.035-inch J-tip guidewire. We performed selective catheterization to the tumor feeding hepatic arteries or in extrahepatic collaterals as distal as possible in each tumor lesion using a 1.98-Fr to 2.4-Fr microcatheter. After the microcatheter was inserted into the target arterial feeder, we slowly administered a mixture of iodized oil (range, 2‒16 ml) (Lipiodol, Guerbet) and doxorubicin hydrochloride (range, 5 to 50 mg) (Adriamycin, Pfizer) or mitomycin (range, 10‒20 mg) (Vesimycin, Naprod Life Sciences) under real time monitoring with DSA. We prepared the cTACE mixture using the water-in-oil technique in which the emulsion contains a chemotherapeutic agent (powder form) diluted with contrast media (Iohexol 350 mgI/ml contrast agent) and subsequently mixed with iodized oil [14]. The amount of water-in-oil-emulsion (1:2 or 1:4 ratio) was adjusted according to the total tumor size and number of nodules. Subsequently, the feeding artery was embolized using gelatin sponge particles. We completed the procedure when the tumor feeding branch was completely obstructed and tumor staining from DSA completely disappeared.
Intraprocedural CBCT technique with AFD software
The CBCT data were acquired using an Allura Clarity FD20 which enabled CBCT acquisition and volumetric image reconstruction. A total of 242 projection images (60 frames/second) with X-ray parameters of 121 kV and 200‒300 mAs were obtained with the motorized C-arm covering a 220° clockwise rotation of the flat panel detectors. The patients were instructed to be at end-expiratory apnea during the CBCT scanning. All CBCT images of 5 mm thickness were interpreted using a workstation (Philips Healthcare, Eindhoven, the Netherlands). We performed CBCT with AFD software assisted cTACE in three steps (Fig. 1).

Cone-beam computed tomography (CBCT) with automated tumor-feeder detection software assisted conventional transarterial chemoembolization (cTACE). A Gadoxetic acid-enhanced MRI in the arterial phase in a 58-year-old male with chronic viral hepatitis-B cirrhosis showing two hyperenhancing nodules (arrows) in liver segment 5. Hepatobiliary phase imaging at 20 min after injection shows two hypointense nodules (arrows) against the background of enhancing liver parenchyma, which may indicate HCC. B‒C Dual-phase CBCT during hepatic arteriography could depict all tumors (arrows) with corona enhancement (arrowheads). D Common hepatic arteriogram showed two faint tumor stains (arrows). However, the tumor-feeders were unclear. E Automated tumor-feeder detection software identified the feeders (arrowhead) of each tumor (arrows). F Tumor-feeder (arrowhead) was selectively embolized during cTACE. Complete tumor staining (arrows) was demonstrated from spot image on digital subtraction angiography. G‒H CBCT immediately after cTACE showed dense iodized oil accumulation in all tumors (arrows) with a sufficient safety margin (arrowheads). I Enhanced CT performed 1 year after selective cTACE showed dense iodized oil accumulation in all tumors without tumor recurrence
Step 1: Identification of tumor nodules
We placed the catheter at the proper or common hepatic artery and performed CBCT during hepatic arteriography (CBCTHA). A total of 24 ml of non-diluted contrast media (Omnipaque 350 mgI/ml, Bayer, Bangkok, Thailand) was injected via a 5-Fr diagnostic catheter at the rate of 2 ml/second. The first phase of CBCTHA started after contrast material injection for 7 s and the second scan was achieved 30 s after finishing the first scan. The patients held their breath twice during the gantry rotation. All hepatic lesions with corona enhancement, which represented venous drainage through hypervascular HCC nodules [15] on the second scan of CBCTHA were targeted for treatment with cTACE.
Step 2: Detection of tumor feeding arteries
The automated tumor-feeder software (EmboGuide, Philips Healthcare, Best, the Netherlands) used the data from the first scan of CBCTHA to identify the tumor feeders in about 2 min at the workstation. We used AFD software to detect segmental tumor feeders in case they were not clearly seen on conventional DSA images. After the feeder branches were identified, embolization was performed without obtaining further DSA images.
Step 3: Evaluation of iodized oil accumulation
We performed plain CBCT without contrast media injection just after the selective cTACE procedure to monitor the distribution of iodized oil. The goal of chemoembolization is to completely embolize the entire target tumor with or without an adequate safety margin. If incomplete tumor stains occurred, further chemoembolization was performed.
Analysis of the prognostic factors for overall survival
Univariate and multivariate analyses were used to define the significant independent factors affecting overall survival (OS). Fourteen clinical factors were analyzed: age, gender, alcohol drinking, hepatitis B or C virus carrier, Child–Pugh class, albumin-bilirubin (ALBI) score, total bilirubin, albumin, international normalized ratio (INR), platelet count, serum alpha-fetoprotein (AFP) level, ascites, and BCLC staging. Also analyzed were four tumor factors: size of largest tumor, number of tumor nodules, lobar involvement, and the up-to-7 criteria plus two procedure-related factors: complete remission at 1 month and use of CBCT-assisted cTACE.
Outcome and treatment evaluation
All eligible patients were followed up after selective cTACE with a detailed clinical examination, blood chemistries, and an imaging study using 4-phase contrast-enhanced CT scan or dynamic MRI within one month after the initial procedure. If no definite evidence of residual or recurrent tumor presented, imaging investigation was performed subsequently at 3-month intervals. We used the modified Response Evaluation Criteria in Solid Tumors (mRECIST) to assess HCC after treatment [16]. Assessment of tumor response was reviewed independently by two radiologists with expertise in liver imaging (TT: > 10 years; KB: 8 years) to minimize variability in this critical instance [17]. In cases of discordance, the final decisions were achieved by consensus. The decision to repeat the cTACE procedure was based on tumor response by mRECIST, BCLC-staging of the disease, and the patient’s tolerance.
Complications
cTACE-related complications were classified as major or minor following the standard Society of Interventional Radiology (SIR) guidelines [18]. Major complications of cTACE were defined as admission to a hospital for therapy, an unplanned increase in the level of care, prolonged hospitalization, permanent adverse sequelae, or death after the procedures by SIR guidelines [18].
Data and statistical analysis
All data analyses were performed using R software (version 4.1.0). Numerical data are given descriptively using the central tendency (mean, median, and mode) and a measure of dispersion (standard deviation and range). We used chi-square or t-test to compare baseline characteristics between the HCC patients who underwent cTACE with CBCT assistance and patients who received cTACE with DSA. Local progression-free survival (PFS) was calculated from the date of selective cTACE to the last date of local tumor progression or the date of patient death. Local tumor progression was diagnosed when an arterial enhancing lesion was depicted in or adjacent to the treated tumor on follow-up imaging. OS was calculated from the date of selective cTACE to the date of patient death. Patient status at the end of the study (December 31, 2020) was defined as alive or dead using data from the Thailand civil registration database. The local PFS and OS rates for the two groups of HCC patients were compared using the Kaplan–Meier estimator. The probability of OS for the two groups was estimated using the Cox’s proportional hazards regression model. The OS rates at 1, 3, and 5 years were calculated and compared for each group.
Baseline clinical characteristics, tumor appearances, and procedure-related factors affecting survival were initially assessed by univariate analysis. Subsequently, all prognostic factors having p values ≤ 0.2 from the univariate analysis were entered into the initial multivariate Cox's proportional hazards regression. The model was refined by sequentially removing non-significant variables. p Values < 0.05 were considered statistically significant.
Results
Patient characteristics
A total of 337 HCC patients were treated with selective cTACE as the first treatment for HCC. One hundred and ninety-six patients were treated by cTACE with CBCT assistance (CBCT-cTACE group) and 141 patients were treated by cTACE with DSA alone (DSA-cTACE group). One hundred and fifty-one patients were categorized into BCLC-B stage and the rest were classified into BCLC stage 0 and stage A within the Milan criteria. Surgery or ablation was avoided in 186 patients in our study for these reasons: not eligible for surgery due to unfavorable remnant liver function, location of the tumor near a blood vessel or another organ, patient intention, inadequate visualization during ultrasonography, presence of ascites, advanced obesity, and severe abnormal coagulopathy.
Subsequently, baseline characteristics were compared between HCC patients in the CBCT-cTACE group and patients in the DSA-cTACE group (Table 1). There were no significant differences between the two groups in terms of age, gender, alcohol drinking, hepatitis B virus (HBV) positivity, hepatitis C virus (HCV) positivity, Child–Pugh class, ALBI score, total bilirubin level, albumin level, INR level, platelet count, serum AFP level, presence of ascites, size of the largest tumor, tumor number, lobar involvement, up-to-7 criteria, and BCLC-staging. However, compared with HCC patients in the DSA-cTACE group, the CBCT-cTACE group had a considerably lower proportion of BCLC-B HCC patients (p = 0.130), and trends to have higher serum albumin (p = 0.064) and INR (p = 0.052) levels.
cTACE procedures
A total of 628 HCC nodules in 337 patients underwent selective cTACE. The mean size of the largest tumor was 34.2 ± 15.1 mm (range, 11‒70 mm) and the mean number of treated tumor nodules per cTACE session was 1.9 ± 1.2 nodules (range, 1‒5). Most of the HCC patients had tumor nodules within the up-to-7 criteria (79.2%) and were characterized as unilobar involvement (84.0%).
Procedural details and tumor response between HCC patients in the CBCT-cTACE group and patients in the DSA-cTACE group are summarized in Table 2. In the CBCT-cTACE group, we performed selective cTACE in 196 patients in 311 hepatic segmental areas. In the DSA-cTACE group, we performed selective cTACE in 141 patients in 213 hepatic segmental areas. The mean dose of iodized oil in one session of cTACE was not significantly different between the two groups (p = 0.068). The mean dose of doxorubicin in one session of cTACE was 21.6 mg (range, 5‒50 mg) in the CBCT-cTACE group and 33.6 mg (range, 5‒50 mg) in the DSA-cTACE group. The mean dose of doxorubicin in the DSA-cTACE group was significantly higher than the CBCT-group (p < 0.001). The mean fluoroscopic time in one session of cTACE in the CBCT-group was significantly longer than in the DSA-cTACE group (16.3 vs. 12.4 min, p < 0.001). However, the mean number of cine acquisitions for HCC patients in the CBCT group were significantly lower than the DSA group (4.6 vs. 5.1, p = 0.017).
The mean number of CBCT acquisitions for the HCC patients in the CBCT-cTACE group was 3.4 times (range, 1‒11). In our study, CBCT was used to identify tumor nodules, detect tumor feeding arteries with AFD software, and evaluate iodized oil accumulation. First, of the 196 HCC patients in the CBCT-cTACE group, the CBCT showed additional HCC nodules that were not evident on CT, MRI, or angiography in 34 patients (17.4%). A total of 48 new HCC nodules were detected on CBCT images (1 new nodule in 23 patients, 2 new nodules in 8 patients, and 3 new nodules in 3 patients). The mean size of the newly detected HCC nodules was 10 ± 3.1 mm (range, 5‒21 mm). All newly found HCC nodules were subsequently treated with selective cTACE. Second, we used the AFD software to detect all segmental tumor-feeding arteries in 139 of the 196 patients (70.9%) when the feeding arteries were not clearly seen on conventional DSA images. The tumor feeding arteries were correctly detected by the AFD software in 133 of 139 patients (95.7%). The reasons for failure to detect the feeding arteries in six patients were: motion artifacts (4 patients), hypovascular tumor nodule (1 patient), and very small caliber feeder vessel to the tumor (1 patient). Third, we monitored the distribution of the iodized oil immediately after the selective cTACE procedure. If iodized oil deposition in the tumors was incomplete, further selective chemoembolization was performed.
Post-treatment assessments were evaluated by 4-phase contrast-enhanced CT scan or dynamic MRI 4 weeks after initial selective cTACE. Tumor response rates by mRECIST in the CBCT-cTACE group with complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) were 67% (131 patients), 28% (55 patients), 4% (7 patients), and 1% (3 patients), respectively. In the DSA-cTACE group, the CR, PR, SD, and PD response rates were 22% (31 patients), 48% (67 patients), 9% (13 patients), and 21% (30 patients), respectively. The response rates after selective cTACE were significantly better in the CBCT-cTACE group than in the DSA-cTACE group (p < 0.001). The number of additional cTACE procedures was not significantly different between the two groups (p = 0.400).
Complications
All cTACE-related complications were classified as minor. The most common procedure-related complication was post-embolization syndrome in 34 patients without requiring extended stay or re-admission. Post-embolization syndrome was not significantly different between the CBCT-cTACE and DSA-cTACE groups (p = 0.920). Groin hematoma was found in eight patients without any treatment. Minimal iodized oil stains in the gallbladder wall due to non-target embolization without symptomatic cholecystitis was found in two patients in the DSA-cTACE group without further treatment. Biloma occurred in one patient and was followed up without any treatment due to no symptoms. The remaining 221 patients were alive at the time of analysis.
Progression-free survival
The mean follow-up time for the HCC patients who underwent selective cTACE was 20.0 ± 15.3 months (range, 0.4‒71.1). The overall recurrence rate was about 96% (136/141 patients) in the DSA-cTACE group and about 79% (155/196 patients) in the CBCT-cTACE group. The median tumor PFS periods for HCC patients in the DSA-cTACE and CBCT-cTACE groups were 33 days (95% CI 32‒35 days) and 467 days (95% CI 262‒848 days), respectively. The median PFS rates for HCC patients in the CBCT-cTACE group were significantly higher than in the DSA-cTACE groups at 1 year (52% vs. 10%), 3 years (38% vs. 6%), and 5 years (38% vs. 4%) by log-rank test (p < 0.001).
Overall survival of patients in the CBCT-cTACE and DSA-cTACE groups
The median OS time of the entire cohort was 23.9 months (95% CI 21.5‒27.9 months). The median OS times in the DSA-cTACE and CBCT-cTACE groups were 13.1 months (95% CI 11.4‒16.8 months) and 32.1 months (95% CI 29.5‒46.4 months), respectively. The cumulative survival rates in the CBCT-cTACE group were significantly higher than in the DSA-cTACE group at 1 year (87% vs. 54%), 3 years (44% vs. 15%), and 5 years (34% vs. 7%) by log-rank test (p < 0.001) (Fig. 2). The mortality rate was 91.5% (129/141 patients) in the DSA-cTACE group and 46.9% (92/196 patients) in the CBCT-cTACE group.

Cumulative overall survival of HCC treated with selective conventional transarterial chemoembolization (cTACE) with cone-beam computed tomography (CBCT) and automated tumor-feeder detection software assistance (CBCT-cTACE group) or with digital subtraction angiography (DSA-cTACE group)
Prognostic factors of overall survival
Among the 20 prognostic factors affecting OS, univariate analysis revealed that Child–Pugh class A (p < 0.001), ALBI score 1 or 2 (p < 0.001), total bilirubin level ≤ 1.0 mg/dl (p < 0.001), albumin > 3.5 g/dl (p < 0.001), INR ≤ 1.2 (p < 0.001), serum AFP level ≤ 200 ng/ml (p = 0.041), no presence of ascites (p = 0.005), and BCLC staging 0 or A (p < 0.001) were the significant clinical factors. Considering the tumor factors, size of largest tumor ≤ 3 cm in diameter and single HCC nodule were significant tumor factors on univariate analysis (p = 0.012 and p = 0.011). In addition, use of CBCT assisted cTACE and presence of CR at 1 month after cTACE were significant procedure-related factors (p < 0.001 and p < 0.001) (Table 3). Multivariate analysis for the potential prognostic factors affecting OS showed that ALBI score 1 or 2 (hazard ratio [HR]: 0.48; p < 0.001), serum AFP level ≤ 200 ng/ml (HR: 0.63; p = 0.003), presence of CR at 1 month after cTACE (HR: 0.55; p < 0.001), and use of CBCT assisted cTACE (HR: 0.38; p < 0.001) were the only four independently significant prognostic factors associated with longer OS (Table 3).
Discussion
In our study, the additional information provided by CBCT resulted in a change in treatments, including visualization of angiographically occult HCC nodules in 34 patients (17.4%) in the CBCT-cTACE group, that were not demonstrated on CT, MRI, or angiography. All 48 small HCC nodules (mean diameter, 10.0 ± 3.1 mm) that could not be detected on other images could be depicted by dual-phase CBCTHA. These findings suggested that the sensitivity of HCC detection increases using CBCT assistance, as reported in previous studies [8, 19, 20]. Additionally, we used the corona enhancement on second phase CBCTHA images to distinguish between HCC nodules and hypervascular pseudolesions [15]. Corona enhancement represents venous drainage through hypervascular HCC and is detected in 89% of HCC nodules [21]. On the contrary, pseudolesions, such as arterioportal shunts, do not demonstrate corona enhancement [20]. Subsequently, all HCC lesions with corona enhancement on the second scan of CBCTHA were targeted for selective cTACE.
The volumetric information from CBCT provides a rotational three-dimensional map of the hepatic arterial anatomy and detection of tumor-feeding branches for selective cTACE. Based on our study, tumor feeders were correctly detected by the AFD software in 95.7% (133/139 patients), which was similar to previous studies [6, 22, 23] that reported the detectability rate of the vessel tracking software was about 81% to 93%. When a tumor-feeding branch was identified by AFD software, we performed selective cTACE of that branch without performing additional DSA runs. These results reduced the number of cine acquisitions in the CBCT group compared to the DSA group (4.6 vs. 5.1; p = 0.017). A previous study [24] demonstrated that the feeder-vessel detection software also reduced the overall procedural time in cTACE. However, mean fluoroscopic time in the CBCT-cTACE group was significantly longer than in the DSA-cTACE group (16.3 vs. 12.4 min, p < 0.001). This occurred probably because the patients in the CBCT-cTACE group had small and subtle tumor-feeding branches that required more fluoroscopic time for selective catheterization. Some limitations of CBCT images are due to motion artifacts caused by inadequate breath-holding. We found that motion artifacts causing failure to detect feeding arteries using AFD software was 2.9% in the CBCT-cTACE group, which was similar to the 3% of patients in a previous report [25]. We can reduce these motion errors by training the patients to hold their breath before the procedures and performing the dual-phase CBCTHA in a propeller-fashion (from the head-end of the table) that requires a scan time of 5 s.
The goal of selective cTACE is complete embolization of the target HCC nodule with an adequate safety margin that leads to a good therapeutic outcome and lower rate of tumor recurrence [9]. CBCT during selective cTACE can verify the accumulation of iodized oil and guide the operator on the endpoint of chemoembolization. If, immediately after selective cTACE, the CBCT shows a non-enhancing portion within the hypervascular HCC nodule, it indicates one of three possibilities: (1) incomplete embolization of the feeding artery, (2) some small feeding arteries were missed, or (3) the presence of an extrahepatic collateral artery supplying the tumor.
In our study, the tumor response rate after selective cTACE was significantly better in the CBCT-cTACE group than in the DSA-cTACE group (p < 0.001), even though the mean dose of chemotherapeutic drugs was significantly lower in the CBCT-cTACE group. These findings suggested that modification of the procedure with cTACE guidance software can decrease local tumor recurrence and improve the tumor response, which were similar to a previous report [26] while reducing the amount of chemoembolic agents. Although post-embolization syndrome was not significantly different between the CBCT-cTACE and DSA-cTACE groups in our study, iodized oil stains in the gallbladder were found only in two patients in the DSA-cTACE group. It was reported that non-target embolization after cTACE through the cystic artery can cause serious complications, such as gallbladder infarct, that require surgery [27].
Our study determined that use of CBCT assisted cTACE is an independently significant prognostic factor associated with longer OS (HR: 0.38; p < 0.001), which was similar to a previous study by Iwazawa et al. [10]. However, there are some differences in terms of methodology. In a previous study [10], the tumor-feeding branch that supplied the target tumor was clarified manually from CBCT images and confirmed by testing with contrast injection to determine whether the entire tumor was totally enhanced. In contrast, we routinely used AFD software to detect segmental tumor-feeding arteries when they were not clearly seen on conventional DSA images. When the feeder branches were labeled from the cTACE guidance software, the branches were embolized without performing additional DSA images. In the Iwazawa study [10], the median OS time in the CBCT-cTACE group without AFD software was 27.2 months (95% CI 0.7‒49.3 months), which was shorter compared to the CBCT-cTACE group with AFD software guidance in our study (32.1 months, 95% CI 29.5‒46.4 months). Therefore, CBCT with cTACE guidance software contributed to longer patient survival compared to HCC patients who underwent cTACE with DSA guidance and was possibly higher than the patients treated with CBCT aided cTACE but without AFD software assistance.
Overall survival in HCC patients can be influenced by other clinical factors, such as hepatitis viral infection or diabetes [28]. Treating the underlying etiology and concomitant liver disease should lead to better survival outcome. Furthermore, recent advances in systemic treatment for HCC, which include second line agents such as tyrosine kinase inhibitors or immunotherapy, appear to accelerate earlier decisions on whether to repeat cTACE or switch to systemic therapy [29, 30]. The concept of switching to systemic agents might be of little benefit once liver function deterioration develops after repeated cTACE. Therefore, performing curative cTACE using CBCT technology is crucial when the tumor is localized and controllable.
In comparison with cTACE, TACE with drug-eluting beads (DEB-TACE) enables higher concentrations of drugs in the distal tumor vessels resulting in more localized chemotherapeutic delivery, but lower systemic concentrations [31]. However, the microspheres in DEB-TACE cannot embolize tumor drainage, which is contrary to cTACE [32]. Therefore, reversed flow from the surrounding portal venules into the peripheral tumor portion may cause tumor tissue to survive. Randomized controlled trials conducted in Europe showed no significant differences in tumor response and survival between the DEB-TACE and cTACE groups [33,34,35]. On the other hand, the latest randomized controlled trial conducted in Japan demonstrated significant differences in CR rates between the cTACE and DEB-TACE groups [36]. Therefore, a discrepancy of outcomes of cTACE exists between Europe and Japan, which was possibly due to different devices and techniques. Selective cTACE uses smaller microcatheters (1.7-F to 2.0-F tip) under intraprocedural monitoring by CBCT, which is the standard technique in Japan and in our institution in Thailand. Moreover, there is a debate about the long-term cost-effectiveness of DEB-TACE compared to cTACE [37], which can be assessed in future studies.
Our study has some limitations. First, this study was retrospective in nature conducted at a single center. Second, we did not evaluate the types of microcatheters, skill of the cTACE operators or level of selective catheterization that may influence the interpretation of the survival outcome. Third, histological confirmation of HCC was not obtained. All study lesions were diagnosed as HCC based on imaging findings and elevated serum levels of tumor markers. Finally, our sample size was relatively small, which limited the number of patients available for a subgroup analysis.
In conclusion, the CBCT technology with AFD software can provide additional information during selective cTACE including identification of HCC nodules, detection of tumor feeding arteries as a 3D navigation tool, and evaluation of iodized oil accumulation, which affects the treatment response and prolongs survival in patients with inoperable HCC. The combination of selective cTACE with the capabilities of CBCT and cTACE guidance software in daily clinical practice may improve the efficacy and prognostic outcome of HCC patients.
Availability of data and materials
All analyzed data are included in this published article. The original data are available upon reasonable request to the corresponding author.
References
Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35:1164–71.
Llovet JM, Real MI, Montaña X, et al. Barcelona Liver Cancer Group. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359:1734–9.
Lencioni R, de Baere T, Soulen MC, Rilling WS, Geschwind JF. Lipiodol transarterial chemoembolization for hepatocellular carcinoma: a systematic review of efficacy and safety data. Hepatology. 2016;64:106–16.
Iwazawa J, Ohue S, Mitani T, et al. Identifying feeding arteries during TACE of hepatic tumors: comparison of C-arm CT and digital subtraction angiography. AJR Am J Roentgenol. 2009;192:1057–63.
Iwazawa J, Ohue S, Kitayama T, Sassa S, Mitani T. C-arm CT for assessing initial failure of iodized oil accumulation in chemoembolization of hepatocellular carcinoma. AJR Am J Roentgenol. 2011;197:W337–42.
Deschamps F, Solomon SB, Thornton RH, et al. Computed analysis of three-dimensional cone-beam computed tomography angiography for determination of tumor-feeding vessels during chemoembolization of liver tumor: a pilot study. Cardiovasc Interv Radiol. 2010;33:1235–42.
Miyayama S, Yamashiro M, Hashimoto M, et al. Identification of small hepatocellular carcinoma and tumor-feeding branches with cone-beam CT guidance technology during transcatheter arterial chemoembolization. J Vasc Interv Radiol. 2013;24:501–8.
Pung L, Ahmad M, Mueller K, et al. The role of cone-beam CT in transcatheter arterial chemoembolization for hepatocellular carcinoma: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017;28:334–41.
Bannangkoon K, Hongsakul K, Tubtawee T, Piratvisuth T. Safety margin of embolized area can reduce local recurrence of hepatocellular carcinoma after superselective transarterial chemoembolization. Clin Mol Hepatol. 2019;25:74–85.
Iwazawa J, Ohue S, Hashimoto N, Muramoto O, Mitani T. Survival after C-arm CT-assisted chemoembolization of unresectable hepatocellular carcinoma. Eur J Radiol. 2012;81:3985–92.
Miyayama S. Ultraselective conventional transarterial chemoembolization: when and how? Clin Mol Hepatol. 2019;25:344–53.
Cui Z, Shukla PA, Habibollahi P, Park HS, Fischman A, Kolber MK. A systematic review of automated feeder detection software for locoregional treatment of hepatic tumors. Diagn Interv Imaging. 2020;101:439–49.
Bruix J, Sherman M, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–2.
Renzulli M, Peta G, Vasuri F, et al. Standardization of conventional chemoembolization for hepatocellular carcinoma. Ann Hepatol. 2021;22:100278.
Kim HC. Role of C-arm cone-beam CT in chemoembolization for hepatocellular carcinoma. Korean J Radiol. 2015;16:114–24.
Llovet JM, Lencioni R. mRECIST for HCC: performance and novel refinements. J Hepatol. 2020;72:288–306.
Tovoli F, Renzulli M, Negrini G, et al. Inter-operator variability and source of errors in tumour response assessment for hepatocellular carcinoma treated with sorafenib. Eur Radiol. 2018;28:3611–20.
Brown DB, Cardella JF, Sacks D, et al. Quality improvement guidelines for transhepatic arterial chemoembolization, embolization, and chemotherapeutic infusion for hepatic malignancy. J Vasc Interv Radiol. 2009;20:S219–26 (S226.e1-10).
Iwazawa J, Ohue S, Hashimoto N, Abe H, Hamuro M, Mitani T. Detection of hepatocellular carcinoma: comparison of angiographic C-arm CT and MDCT. AJR Am J Roentgenol. 2010;195:882–7.
Miyayama S, Yamashiro M, Hattori Y, et al. Efficacy of cone-beam computed tomography during transcatheter arterial chemoembolization for hepatocellular carcinoma. Jpn J Radiol. 2011;29:371–7.
Ueda K, Matsui O, Kawamori Y, et al. Differentiation of hypervascular hepatic pseudolesions from hepatocellular carcinoma: value of single-level dynamic CT during hepatic arteriography. J Comput Assist Tomogr. 1998;22:703–8.
Iwazawa J, Ohue S, Hashimoto N, Muramoto O, Mitani T. Clinical utility and limitations of tumor-feeder detection software for liver cancer embolization. Eur J Radiol. 2013;82:1665–71.
Miyayama S, Yamashiro M, Ikuno M, Okumura K, Yoshida M. Ultraselective transcatheter arterial chemoembolization for small hepatocellular carcinoma guided by automated tumor-feeders detection software: technical success and short-term tumor response. Abdom Imaging. 2014;39:645–56.
Iwazawa J, Ohue S, Hashimoto N, Mitani T. Comparison of the number of image acquisitions and procedural time required for transarterial chemoembolization of hepatocellular carcinoma with and without tumor-feeder detection software. Radiol Res Pract. 2013;29:580839.
Lee IJ, Chung JW, Yin YH, et al. Cone-beam CT hepatic arteriography in chemoembolization for hepatocellular carcinoma: angiographic image quality and its determining factors. J Vasc Interv Radiol. 2014;25:1369–79 (quiz 1379-.e1).
Miyayama S, Yamashiro M, Hashimoto M, et al. Comparison of local control in transcatheter arterial chemoembolization of hepatocellular carcinoma ≤6 cm with or without intraprocedural monitoring of the embolized area using cone-beam computed tomography. Cardiovasc Interv Radiol. 2014;37:388–95.
Collins J, Salem R. Hepatic radioembolization complicated by gastrointestinal ulceration. Semin Interv Radiol. 2011;28:240–5.
Facciorusso A. The influence of diabetes in the pathogenesis and the clinical course of hepatocellular carcinoma: recent findings and new perspectives. Curr Diabetes Rev. 2013;9:382–6.
Facciorusso A, Abd El Aziz MA, Sacco R. Efficacy of regorafenib in hepatocellular carcinoma patients: a systematic review and meta-analysis. Cancers (Basel). 2019;12:36.
Abd El Aziz MA, Facciorusso A, Nayfeh T, et al. Immune checkpoint inhibitors for unresectable hepatocellular carcinoma. Vaccines (Basel). 2020;8:616.
Padia SA, Shivaram G, Bastawrous S, et al. Safety and efficacy of drug-eluting bead chemoembolization for hepatocellular carcinoma: comparison of small-versus medium-size particles. J Vasc Interv Radiol. 2013;24:301–6.
Minamiguchi K, Tanaka T, Nishiofuku H, et al. Comparison of embolic effect between water-in-oil emulsion and microspheres in transarterial embolization for rat hepatocellular carcinoma model. Hepatol Res. 2020;50:1297–305.
Lammer J, Malagari K, Vogl T, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Interv Radiol. 2010;33:41–52.
Sacco R, Bargellini I, Bertini M, et al. Conventional versus doxorubicin-eluting bead transarterial chemoembolization for hepatocellular carcinoma. J Vasc Interv Radiol. 2011;22:1545–52.
Golifieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111:255–64.
Ikeda M, Inaba Y, Tanaka T, et al. A prospective, randomized, controlled trial of selective DEB-TACE vs. selective cTACE with epirubicin for hepatocellular carcinoma: JIVROSG-1302 PRESIDENT study. J Clin Oncol. 2020;38:4518.
Cucchetti A, Trevisani F, Cappelli A, et al. Cost-effectiveness of doxorubicin-eluting beads versus conventional trans-arterial chemoembolization for hepatocellular carcinoma. Dig Liver Dis. 2016;48:798–805.
Acknowledgements
The authors would like to express our deep and sincere gratitude to Assoc. Prof. Teerha Piratvisuth, from the NKC Institute of Gastroenterology and Hepatology, Faculty of Medicine, Prince of Songkla University for giving me invaluable suggestions from the beginning to the end of this study. We would also like to thank Mrs. Jirawan Jayuphan, from the Epidemiology Unit, Faculty of Medicine, Prince of Songkla University for the statistical work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Study concept and design: KB, KH, TT. Data acquisition: KB, TT. Data analysis and interpretation: KB, KH. Drafting of the manuscript: KB, KH. Critical revision of the manuscript for important intellectual content: KB, KH. Statistical analysis: KB, KH, TT. All authors approved the final draft of the manuscript submitted to the journal. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study complies with the standards of the Declaration of Helsinki and current ethical guidelines, and approval was obtained from the institutional ethics committee (REC No. 64-257-7-1). The requirement for informed consent for this study was waived by the Institutional Review Board, and all the data were analyzed anonymously.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bannangkoon, K., Hongsakul, K. & Tubtawee, T. Impact of cone-beam computed tomography with automated feeder detection software on the survival outcome of patients with hepatocellular carcinoma during treatment with conventional transarterial chemoembolization. BMC Gastroenterol 21, 419 (2021). https://doi.org/10.1186/s12876-021-02004-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-021-02004-z