
Abstract
Background
Ulcerative colitis (UC) is a chronic inflammatory bowel disease with recurrent episodes of debilitating symptoms negatively affecting work productivity and health-related quality of life (HRQoL). The use of biologics in UC treatment improves work and HRQoL but prospective long-term data concerning the treatment with TNFα inhibitor golimumab in UC patients are still rare. Therefore, our study aimed to evaluate the change in work productivity, capacity for daily activities and HRQoL in UC patients treated with golimumab in Germany.
Methods
Using the Work Productivity and Activity Impairment questionnaire, the change in work productivity and in capacity for daily activities after 3 months and over the whole observational period of 24 months were assessed (both primary endpoints). Disease-specific and health-related quality of life (QoL) were analyzed with the Inflammatory Bowel Disease Questionnaire (IBDQ), the Short-Form 12 Health Survey Questionnaire (SF-12), and the Partial Mayo Score (secondary endpoints). Further, disease-related hospitalization rates were assessed.
Results
This prospective non-interventional study included 286 patients. Thereof, 212 patients were employed at baseline (modified intention to treat analysis set employed at baseline, mITTe). 61.3% of the mITTe patients had moderate and 17.0% had severe UC. Three months after initiation of golimumab therapy, total work productivity impairment (TWPI) score and activity impairment score improved significantly from baseline with a mean change of − 17.3% (p < 0.0001) and − 14.4% (p < 0.0001), respectively. Results persisted over 24 months (mean change TWPI score: − 24.5%, mean change activity impairment score: − 30.0%). Disease- and health-related QoL also improved significantly under golimumab treatment as indicated by increased IBDQ [mean change: 28.0 (SD: ± 36.1, month 3), 42.1 (SD: ± 39.5, month 24)] and SF-12 scores [PCS-12: 45.9 (SD: ± 8.5), MCS-12: 4.9 (SD: ± 10.6, month 3), PCS-12: 5.9 (SD: ± 9.0), MCS-12: 6.4 (SD: ± 11.1, month 24)]. Disease-related hospitalization rate decreased from 16.0% (BL) to 4.3% at month 24 and the mean number of missed working days due to UC decreased from 8.2 (SD: 17.6, BL) to 0.7 (SD: 2.1) after golimumab induction.
Conclusions
Golimumab leads to notable long-term improvements in work productivity, daily activity, HRQoL, and disease-related hospitalization rates in patients with moderate to severe UC.
Trial registration: PEI (Paul-Ehrlich-Institute, Langen, Germany) Registration Nr: NIS#255 (https://www.pei.de/SharedDocs/awb/nis-0201-0300/0255.html)
Similar content being viewed by others

Background
Ulcerative colitis (UC) is a chronic inflammatory disorder of the gastrointestinal tract that typically begins in the second and third decades of life [1,2,3]. Mucosal inflammation extending proximally from the rectum and the development of extensive superficial ulceration are the key features [4]. Symptoms include recurrent flares of bloody diarrhea with numerous liquid bloody stools, fecal urgency, abdominal pain, incontinence, weight loss, and general malaise [3]. Moderate to severe ulcerative colitis highly impairs health-related quality of life (QoL) [5,6,7,8]. Additionally, a negative association between health-related QoL and unemployment, sick leave, and disability pension in patients with inflammatory bowel disease has been reported [9,10,11,12]. Since this represents a strenuous and challenging situation for the patients, rapid achievement and stable maintenance of clinical remission are the primary goals in UC therapy [13, 14].
Due to the early onset of UC and the associated high utilization of health services, UC causes significant socioeconomic burden [15, 16]. Since budget limitations and pressure on healthcare spending have been increased during the last years, data on indirect costs like productivity losses and health care resource utilization data have recently become extremely important in the German healthcare system [17]. Additionally, patient-reported outcomes and relevant additional benefit of new treatment options have come into focus of German sick funds to provide optimal medically and economically sensible healthcare services for affected patients [18].
Better understanding of the pathogenesis in UC has led to new treatment options such as tumor necrosis factor alpha inhibitors (anti-TNFα). The human monoclonal anti-TNFα antibody golimumab (Simponi®) is indicated for the treatment of moderately to severely active UC in adult patients who have had an inadequate response to conventional therapy, including corticosteroids and 6-mercaptopurine or azathioprine, or who are intolerant of or have medical contraindications to such therapies [19,20,21]. In moderate to severe Crohn´s disease, clinically meaningful improvement of work productivity and disease-specific QoL was found for anti-TNFα adalimumab [17, 22]. In the two Active Ulcerative Colitis Trials 1 and 2 (ACT-1 and ACT-2, respectively) among others the relationships of clinical response and/or remission to another anti-TNFα, infliximab, with health-related QoL, employment, and productivity was assessed [23]. For patients in remission the improvements from baseline in productivity and both actual and fully productive hours worked per week were greater [24]. However, systematic data for golimumab in UC patients regarding work productivity and activity impairment as well as health-related QoL are still sparsely available in the literature. Therefore, the GO CUTE study was initiated to evaluate the changes in work productivity and Qol in UC patients treated with golimumab in Germany to characterize the benefit of this treatment option. Additionally, data on health economic aspects were collected to evaluate whether golimumab therapy may affect disease-related health care resource utilization.
Methods
Study design and study population
The GO CUTE study was a prospective, multicentre, open-label, non-interventional study conducted in 51 gastroenterological practices in Germany between March 2014 (first patient first visit) and July 2019 (last patient last visit). Biologic-naïve and biologic-experienced, golimumab naïve patients aged ≥ 18 years (inclusion criterion, IC 1), with UC diagnosed by a gastroenterologist (IC 2) who were suitable for golimumab therapy in accordance with the approved summary of product characteristics (SmPC) [19] and clinical standards (IC 3) and had given his/her signed consent form, were included in the study (IC 4). Patients with a contraindication according to the current Simponi® (golimumab) SmPC (exclusion criterion, EC 1) [19], a previous treatment with golimumab (EC 2), with previous biologic treatment which was changed due to a serious adverse event (SAE), an opportunistic infection or hypersensitivity reaction (EC3), or/and a current participation in another clinical trial (with exception of register studies, EC 4) were not eligible for study participation.
Observational phase lasted 24 months starting with a baseline visit followed by 6 post-baseline visits in month 3, 6, 9, 12, 18, and 24 (end of observation). Treatment during observational phase was carried out in accordance with the current Simponi® (golimumab) SmPC [19]. The decision to initiate golimumab therapy was made by the treating physician based on individual medical indication. According to the SmPC, golimumab was administered intravenously at a dose of 200 mg initially administered by subcutaneous injection in week 0, followed by 100 mg at week 2 and then 100 mg (if body weight ≥ 80 kg) or 50 mg (if body weight < 80 kg) every 4 weeks as maintenance therapy [19]. All patient-related data were recorded in pseudonymized form using an electronic case report form.
Study endpoints and data collection
The primary endpoint of the study was to evaluate the changes in work productivity or activity impairment in month 3, 6, 9, 12, 18, and 24 (from baseline) compared to baseline in UC patients after induction of golimumab therapy using the work productivity and activity impairment questionnaire specified for UC (WPAI-UC V2.0) [25]. The WPAI (in general) represents the psychometrically best validated instrument for determining health-related work productivity [26, 27] and was proved in patients with UC in randomized, controlled trials as well as in non-interventional observational studies. All four WPAI scores (absenteeism, presenteeism, total work productivity impairment [TWPI], and daily activity) were assessed in the current study [28].
Secondary endpoints of the study were to assess the change in disease-related and health-related QoL determined by the Inflammatory Bowel Disease Questionnaire (IBDQ) and the 12-item Short-Form Health Survey Questionnaire (SF-12) as well as the change in disease activity measured by the Partial Mayo Score over 3, 6, 9, 12, 18, and 24 months. The IBDQ evaluates disease-related QoL and considers systemic and bowel symptoms as well as social function and emotional health by 32 items [29, 30]. The SF-12 comprises 12 questions on physical and mental status (physical component score [PCS-12] and mental component score [MCS-12]) to assess the overall state of health and evaluate the ability to engage in moderate activities [31]. The SF-12 is applicable regardless of the patients´ disease and age. The Partial Mayo Score is an instrument to measure disease activity without sigmoidoscopy by assessing stool frequency, rectal bleeding and physician’s global assessment (i.e. the three non-invasive components of the full Mayo score [32]). Each parameter ranges from 0–3, with a maximum total score of 9, where 0 to 1 = remission, 2 to 4 = mild disease, 5 to 6 = moderate disease, and 7 to 9 = severe disease (i.e. higher scores indicate worsening of the disease).
Assessment of changes in health care resource utilization, changes in the number of missed working days due to UC and changes in disease-related hospitalizations, each from baseline to month 12 as well as from month 12 to month 24, represented exploratory endpoints of the current study. Health care resource utilization assessment was deemed to provide an insight on UC impact on health care budgets [17]. Therefore, information concerning alternative treatment, rehabilitation, cure for UC or other reasons, ambulant, non-medical treatment, consultations due to UC, and UC-related sick leave (only for employed patients) were recorded. Using the Partial Mayo Score, the relationship of clinical baseline parameters and response to the therapy with health care resource utilization and work productivity can be assessed to identify patient groups with highest effects on health resources. Information about disease-related hospitalizations was derived from the physician’s own records, patient records in patient´s diary, and discharge summaries from the hospital where the patient was hospitalized. Disease-related was defined as any medical intervention with a direct, causal relation to UC, which aimed at the prevention of disease progression or prevention, reduction, or cure of symptoms/damage of UC or secondary diseases due to the underlying disease. Relationship was determined by the treating physician.
Furthermore, at each study visit, a complete physical examination was performed.
Ethical considerations
This study was conducted in compliance with the principles of the Declaration of Helsinki. Prior to initiation of this non-interventional study at any site, the observational plan and the informed consent form were approved (reference number 13104) by the competent independent ethics committee of the Bavarian State Medical Association (Ethik-Kommission der Bayerischen Landesärztekammer, Munich/Germany). All study participants provided informed written consent prior to study enrolment. This non-interventional study was further registered at the Paul-Ehrlich-Institute, Langen, Germany (Registration Nr: NIS#255, https://www.pei.de/SharedDocs/awb/nis-0201-0300/0255.html).
Statistical analysis
Statistical analyses were performed using SAS version 9.4. Categorical variables are presented as number and percentages. Quantitative variables are shown as mean with standard deviation (SD) or median with range. Differences or changes from baseline are indicated as mean change with SD or percentage change (%). Dependent sample t test was used for continuous variables if they were normally distributed. If the assumption of normal distribution was questionable, the Wilcoxon ranked sum test were performed to determine statistical significance. Differences were considered significant at p < 0.05. All enrolled patients who received at least one dose of golimumab, fulfilled all inclusion and exclusion criteria, had a baseline assessment and at least one documented additional visit, regardless of any protocol violation during the study and irrespective if he/she was still on golimumab treatment were included in the modified intention to treat (mITT) analysis set. Additionally, a mITTe subset was analyzed comprising of all patients of the mITT being full-time or employed at baseline.
Results
Patient disposition
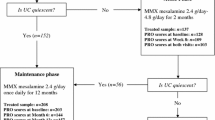
A total of 286 UC patients were enrolled in the study. One patient did not start treatment with golimumab; therefore, 285 patients remained in the study (Fig. 1). The mITT set consisted of 282 patients since three patients did not perform a second visit. As shown in Table 1, a total of 212 patients were employed at baseline and were evaluated for the primary endpoints of the study (mITTe). A total of 107 patients prematurely discontinued study participation, mostly due to withdrawal of informed consent (n = 61/107, Fig. 1). The gender balanced mITT population were aged from 18 to 95 years with a median age of 39.5 years (data not shown).

Patient flow diagram. n: number of patients, mITT: modified intention-to-treat analysis set
UC was the most frequently stated reason for full reduction of work (n = 8/12) or incapacity to work (n = 11/11) but not for working in part-time (20.0%, n = 8/40, Table 2).
Nearby half of the patients (45.0%, n = 127/282) reported at least one concomitant disease at BL (Table 3).
For 11.0% of the patients (n = 31/282 patients) extraintestinal manifestations of UC were documented. The majority of patients (69.9%, n = 197/282 patients) received concomitant medication at baseline, including aminosalicylates (41.5%, n = 117/282) and corticosteroids (24.1%, n = 68/282, Table 3). Additional details concerning patient demographics and disease characteristics, occupational status as well as concomitant diseases and concomitant medications are shown in Tables 1, 2, and 3, respectively.
Work productivity and activity impairment in UC patients (mITTe set)
After 3 months of onset of golimumab treatment a statistically significant reduction in all WPAI-UC scores compared to baseline was observed (p value < 0.0001, t test or Wilcoxon ranked sum test, Fig. 2a–d). For total work productivity impairment, a mean change of − 17.3% (SD: ± 32.3) was detected (Fig. 2a). At the end of the study, the mean value in the total work productivity impairment subscore decreased from 49.4% (SD: ± 27.8, baseline) to 23.4% (SD: ± 23.8, month 24). This corresponded to a mean change of − 24.5% (SD ± 29.4, Fig. 2a). Similar results were observed for the activity impairment score with a reduction of − 14.4% (mean change, SD: ± 28.5, month 3) and − 30.0% (mean change, SD: ± 31.5, month 24) from baseline to the respective timepoints (Fig. 2b). For the subscore absenteeism, a mean change from baseline of − 13.8% (SD: ± 38.8) at month 3 and a mean change of − 23.2% (SD: ± 41.5) at month 24, respectively, was observed (Fig. 2d). The mean change from baseline of the presenteeism subscore was − 14.8% (SD: ± 29.0) after 3 months and − 22.5% (SD: ± 27.2) at month 24, respectively.

Work productivity and activity impairment in UC patients (mITTe set). The mean change in total work productivity impairment (TWPI, a) and activity impairment (b) is shown for month 3 and for month 24 (both primary endpoints). For both impairments a statistically significant improvement was observed at month 3 and month 24, respectively. For absenteeism (c) as well as presenteeism (d), similar outcomes were reported. a–d Analyses were performed for the mITT analysis set employed at BL (mITTe set). Data were shown as mean change (SD) from baseline in %. n: number of patients. BL: baseline. SD: standard deviation
Disease- and health-related QoL in UC patients (mITT set)
After onset of golimumab treatment, a significant improvement of disease-related QoL measured by the Inflammatory Bowel Disease Questionnaire was observed (p value < 0.0001, t test, Fig. 3a). After 3 months, mean change from baseline in total IBDQ score was 26.5 points (SD: ± 36.5, Fig. 3a). At the end of the 24 months study, mean change in Inflammatory Bowel Disease Questionnaire score amounted to 41.4 (SD: ± 39.5) points. Health-related QoL, evaluated by the 12-item Short-Form Health Survey Questionnaire, was also markedly improved in UC patients since the majority of patients (n = 194) had a significant increase in both subscores of the 12-item Short-Form Health Survey Questionnaire after 3 months [PCS-12: mean change from baseline of 3.3 (SD: ± 8.2) points, MCS-12: mean increase of 4.3 (SD: ± 10.1) points] as well as after 24 months [PCS-12: + 6.4 (SD: ± 9.1) points, MCS-12: + 6.2 (SD: ± 10.7) points, for both subscores: p value < 0.0001, t test, Fig. 3c, d].

Disease- and health-related quality of life and disease severity in UC patients (mITT). The mean change of the total Inflammatory Bowel Disease Questionnaire score is presented in a revealing a statistically significant change in month 3 and month 24 in comparison to BL. A statistically significant decrease in disease severity was observed in month 3 as well as in month 24 after onset of golimumab treatment as shown in b. Health-related quality of life measured by SF-12 (c [PCS-12], d [MCS-12]) was also improved in UC patients at both time points when compared to BL data. Analyses were done for the mITT analysis set and p values were generated using the paired t test (*) or Wilcoxon ranked sum test (*1). n: number of patients. BL: baseline. SD: standard deviation. IBDQ: inflammatory bowel disease questionnaire. PMS: partial Mayo score. SF-12: 12-item short form health survey. PCS-12: physical condition score of the SF-12. MCS-12: mental condition score of the SF-12
Disease severity and disease-related hospitalizations (mITT set)
Physicians assessed disease severity by the Partial Mayo Score. Three months after baseline, the Partial Mayo Score decreased notably with a mean change of − 1.9 (SD: ± 2.7) points (mITT set, p value < 0.0001, Wilcoxon ranked sum test, Fig. 3b). A significant reduction in Partial Mayo Score was also observed after 24 months, with a mean change from baseline of − 3.3 (SD: ± 2.5) points in two third of the patients (n = 152, mITT set, p value < 0.0001, Wilcoxon ranked sum test, Fig. 3b).
During the observational period, the disease-related hospitalization rate (per 100-person-years) decreased from 16.0% to 11.0% (after 1st year of observation, mean change of − 5.0 [95%CI: − 8.73, − 1.26]) and to 4.3% (after 2nd year of observation, mean change of − 11.6 [95%CI: − 13.55, − 9.71], Fig. 4a). At baseline (based on the year before), the mean number of disease-related hospitalization days was 0.5 (SD: ± 1.71) per 100 patient years (Fig. 4b). After 1st year of observation, just a minor decline in the mean number of disease-related hospitalization days was observed [0.4 days (SD: ± 1.52) per 100 patient years] whereas after the 2nd year of observation, the mean number of disease-related hospitalization days was notably declined to 0.1 days (SD: ± 0.71) per 100 patient years (Fig. 4b). Additively, a reduction in the mean duration of hospitalization was observed during observational period [from 1.4 days (SD: ± 5.17) (year before baseline) to 1.0 days (SD: ± 4.12) after 1st year of observation and to 0.2 days (SD: ± 1.62) after 2nd year of observation, Fig. 4c].

Disease-related hospitalizaton rate. The hospitalization rate of the mITT set is shown in a for the year before baseline (BL) visit and for the 1st (month 12) and 2nd year (month 24) of observation. b displayed the mean number of hospitalization days per 100 patient years with SD before BL and during the observational period. The mean duration of hospitalization in days is shown in c. Linear regression line was calculated using Graph Pad Prism 7.05. n: number of patients. Yrs: years
Health care resource utilization and missed working time
Health care resource utilization assessment revealed that the number of patients seeking general practitioners [baseline: 23.8% of the patients (n = 67/282); month 24: 17.1% of the patients (n = 26/152)] or gastroenterologists [baseline: 52.5% of the patients (n = 148/282); month 24: 33.6% of the patients (51/152)] for medical advice declined after onset of golimumab treatment (Fig. 5a). Additionally, a slight reduction in the mean number of visits were observed [general practitioners: from 3.6 (SD: ± 3.38, baseline) to 1.9 (SD: ± 1.17, month 24), gastroenterologists: from 4.3 (SD: ± 2.74, baseline) to 2.7 (SD: ± 2.02, month 24), Fig. 5a]. The number of patients utilizing alternative treatment [baseline: 3.6% (n = 10/282) of the patients, month 24: 1.3% (n = 2/152) of the patients] or ambulatory treatment [baseline: 3.9% (n = 11/282) of the patients, month 24: 2.0% (n = 3/152) patients], was also reduced after golimumab treatment (data not shown). Three months before baseline, the mean number of working days missed was 8.2 days/3 months. After 1st year of observation, this number declined to 3.0 days/3 months. At the end of the observational phase, solely 0.7 working days/3 months were missed by the patients (Fig. 5b).

Disease-related health care resource utilization und working time missed. Disease-related health care resource utilization (HCRU) were assessed among other items by the number of medical specialty consultations in regard to UC in the mITT analysis set. An overview is given in a. Additionally, the missed working time in the 3 months before BL and after 3 and 24 months after start of golimumab treatment in the mITTe analysis set is shown in b indicated as mean number of days/3 months. A marked decrease in the number of missed working days was observed after onset of golimumab treatment. BL: baseline. n: number of patients
Discussion
The GO CUTE study was a prospective, multicenter study in Germany, demonstrating that golimumab treatment markedly improved work productivity and ability to perform daily activities in UC patients 3 months after induction of golimumab. These benefits were already shown in a 12-months interim analysis [33] but persisted over the whole observational period of 24 months. Furthermore, golimumab treatment led to a reduction of missed working days and to a marked improvement of health- and disease-related QoL shown by increase scores of Inflammatory Bowel Disease Questionnaire and 12-item Short-Form Health Survey Questionnaire. Additionally, a decline of the disease-related hospitalization rates after 1st and 2nd year of observation with shorter residence times in hospital were observed after start of golimumab treatment. Evaluation of UC-related health care resource utilization showed that the number of patients with medical specialty consultations markedly decreased and less ambulatory treatments have been utilized by the study population during observational period.
UC patients with active disease have severely impaired work life since they are faced with lower ability to concentrate, reduced working speed and minor work productivity additionally to gastrointestinal symptoms leading to a notable reduction in health-related QoL [9, 11]. Beside the affected patients, UC-dependent work impairment and incapacity cause an increase of direct and indirect healthcare costs [15, 16]. Therefore, an adequate maintenance of disease is important for the patients and the healthcare system. Our results showed that golimumab positively affects the work productivity in UC patients and reduces missed working days. These findings support the results of studies such as the Active Ulcerative Colitis Trials 1 and 2 which investigated the effect of biologic treatment on UC [24]. Those trials demonstrated that UC patients who achieved clinical remission or response were able to increase their hours per week (i.e., hours actually worked) as well as their work productivity. Further, they improved their disease- and health-related QoL as observed by increased Inflammatory Bowel Disease Questionnaire and 36-item Short Form Health survey scores. In the GO CUTE study, most of the patients also achieved clinical remission and an improved QoL, both representing well-accepted therapeutic goals in UC treatment [14, 34]. Consequently, golimumab represents, such as other anti-TNFs [17, 35], an effective therapeutic option to improve work life conditions and patients´ well-being in those people suffering from moderate to severe UC.
UC represents a cost-intensive disease [36], therefore health insurance providers are interested in medical and economical effects of new treatment options. Our results revealed that beside an improved work life and an enhanced QoL, golimumab decreased the number of disease-related hospitalizations in treated patients over 24 months. A reduced hospitalization rate together with reduced medical specialist consultations after golimumab induction as observed in the current study, appear to lower costs of health care resource utilization. Several studies reported that there is a shift from UC-related hospitalization costs due to costs caused by biologics-based treatment in patients with UC [37]. However, patients with reduced number of hospitalizations also reported an improved disease- and health-related QoL [38] and consequently might use healthcare services less often than patients with active disease. Our study supports such observations since on the one hand, most patients achieved an enhanced QoL and on the other hand, health care resource utilization decreased during observational phase. Those findings underline the necessity to consider all aspects of a treatment option to ensure a reasonable pharmacoeconomic evaluation by health policy makers to support the medically most appropriate and resource-conserving treatment that effectively normalizes QoL in UC patients.
Remarkable, large number of patients had withdrawn informed consent during observational phase. Several studies reported a higher rate of treatment failure in patients treated with golimumab than in patients receiving adalimumab, infliximab or a biosimilar to infliximab often associated with a treatment switch [39]. Such a switch could be a reason for patients to withdraw their informed consent, but patients are not obliged to explain their motives, thus only speculations will be possible. Due to a high rate of withdrawn informed consents, the number of patients with adequate treatment response could be overrepresented in the current study. However, since patients were selected by the treating physician in accordance to the current SmPC for golimumab treatment independently of study inclusion, we think, the study represent the real-world situation in Germany and therefore, results are reliable and meaningful.
In summary, the GO CUTE study illustrated that golimumab is an effective treatment in patients suffering from moderate to severe UC in this real-world outpatient setting. Golimumab treatment allowed sustained improvement in WPAI and disease- and health-related QoL. Further, after golimumab induction a notable reduction of disease-related hospitalizations and health care resource utilization is observable which also improved disease-related QoL.
Conclusions
Golimumab treatment improves notably patients´ work productivity and daily activity as well as disease- and health-related quality of life over 24 months after golimumab induction.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- Anti-TNFα:
-
Anti tumor necrosis factor alpha
- BL:
-
Baseline
- EC:
-
Exclusion criterion
- HCRU:
-
Health care resource utilization
- HRQoL:
-
Health-related quality of life
- IBDQ:
-
Inflammatory bowel disease questionnaire
- IC:
-
Inclusion criterion
- MCS-12:
-
Mental component score of the SF-12
- mITT:
-
Modified intention to treat analysis set
- mITTe:
-
Modified intention to treat analysis set (employed at baseline)
- PCS-12:
-
Physical component score of the SF-12
- PMS:
-
Partial Mayo score
- QoL:
-
Quality of life
- SD:
-
Standard deviation
- SF-12:
-
12-Item short-form health survey questionnaire
- SmPC:
-
Summary of product characteristics
- TNFα:
-
Tumor necrosis factor alpha
- TWPI:
-
Total work productivity impairment
- UC:
-
Ulcerative colitis
- WPAI:
-
Work productivity and activity impairment questionnaire
- WPAI-UC:
-
Work productivity and activity impairment questionnaire – ulcerative colitis
References
Loftus EV Jr, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin North Am. 2002;31(1):1–20.
Feuerstein JD, Cheifetz AS. Ulcerative colitis: epidemiology, diagnosis, and management. Mayo Clin Proc. 2014;89(11):1553–63.
Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756–70.
Xavier RJ, Podolsky DK. Unravelling the pathogenesis of inflammatory bowel disease. Nature. 2007;448(7152):427–34.
Bernklev T, Jahnsen J, Lygren I, Henriksen M, Vatn M, Moum B. Health-related quality of life in patients with inflammatory bowel disease measured with the short form-36: psychometric assessments and a comparison with general population norms. Inflamm Bowel Dis. 2005;11(10):909–18.
Casellas F, Arenas JI, Baudet JS, Fábregas S, García N, Gelabert J, Medina C, Ochotorena I, Papo M, Rodrigo L, Malagelada JR. Impairment of health-related quality of life in patients with inflammatory bowel disease: a Spanish multicenter study. Inflamm Bowel Dis. 2005;11(5):488–96.
Rubin GP, Hungin AP, Chinn DJ, Dwarakanath D. Quality of life in patients with established inflammatory bowel disease: a UK general practice survey. Aliment Pharmacol Ther. 2004;19(5):529–35.
Panés J, Domènech E, Aguas Peris M, Nos P, Riestra S, Juliá de páramo B, Cea-Calvo L, Romero C, Marín-Jiménez I. Association between disease activity and quality of life in ulcerative colitis: results from the CRONICA-UC study. J Gastroenterol Hepatol. 2017;32(11):1818–24.
Bernklev T, Jahnsen J, Henriksen M, Lygren I, Aadland E, Sauar J, Schulz T, Stray N, Vatn M, Moum B. Relationship between sick leave, unemployment, disability, and health-related quality of life in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2006;12(5):402–12.
Høivik ML, Moum B, Solberg IC, Henriksen M, Cvancarova M, Bernklev T. IBSEN Group. Work disability in inflammatory bowel disease patients 10 years after disease onset: results from the IBSEN Study. Gut. 2013;62(3):368–75.
De Boer AG, Bennebroek Evertsz’ F, Stokkers PC, Bockting CL, Sanderman R, Hommes DW, Sprangers MA, Frings-Dresen MH. Employment status, difficulties at work and quality of life in inflammatory bowel disease patients. Eur J Gastroenterol Hepatol. 2016;28(10):1130–6.
Feagan BG, Bala M, Yan S, Olson A, Hanauer S. Unemployment and disability in patients with moderately to severely active Crohn’s disease. J Clin Gastroenterol. 2005;39(5):390–5.
Theede K, Kiszka-Kanowitz M, Nordgaard-Lassen I, Mertz NA. The impact of endoscopic inflammation and mucosal healing on health-related quality of life in ulcerative colitis patients. J Crohns Colitis. 2015;9(8):625–32.
Peyrin-Biroulet L, Sandborn W, Sands BE, Reinisch W, Bemelman W, Bryant RV, D’Haens G, Dotan I, Dubinsky M, Feagan B, Fiorino G, Gearry R, Krishnareddy S, Lakatos PL, Loftus EV Jr, Marteau P, Munkholm P, Murdoch TB, Ordás I, Panaccione R, Riddell RH, Ruel J, Rubin DT, Samaan M, Siegel CA, Silverberg MS, Stoker J, Schreiber S, Travis S, Van Assche G, Danese S, Panes J, Bouguen G, O’Donnell S, Pariente B, Winer S, Hanauer S, Colombel JF. Selecting therapeutic targets in inflammatory bowel disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol. 2015;110(9):1324–38.
Cohen RD, Yu AP, Wu EQ, Xie J, Mulani PM, Chao J. Systematic review: the costs of ulcerative colitis in Western countries. Aliment Pharmacol Ther. 2010;31(7):693–707.
Wolters FL, Russel MG, Sijbrandij J, Schouten LJ, Odes S, Riis L, Munkholm P, Langholz E, Bodini P, O’Morain C, Katsanos K, Tsianos E, Vermeire S, Van Zeijl G, Limonard C, Hoie O, Vatn M, Moum B, Stockbrügger RW. European Collaborative Study Group On Inflammatory Bowel Disease. Disease outcome of inflammatory bowel disease patients: general outline of a Europe-wide population-based 10-year clinical follow-up study. Scand J Gastroenterol Suppl. 2006;243:46–54.
Louis E, Löfberg R, Reinisch W, Camez A, Yang M, Pollack PF, Chen N, Chao J, Mulani PM. Adalimumab improves patient-reported outcomes and reduces indirect costs in patients with moderate to severe Crohn’s disease: results from the CARE trial. J Crohns Colitis. 2013;7(1):34–43.
Prasad M, Wahlqvist P, Shikiar R, Shih YC. A review of self-report instruments measuring health-related work productivity: a patient-reported outcomes perspective. Pharmacoeconomics. 2004;22(4):225–44.
European Medicines Agency: Simponi® Summary of product characteristics, https://www.ema.europa.eu/en/documents/product-information/simponi-epar-product-information_de.pdf. Accessed 09 Nov 2020.
Kucharzik T, Dignass AU, Atreya R, Bokemeyer B, Esters P, Herrlinger K, Kannengießer K, Kienle P, Langhorst J, Lügering A, Schreiber S, Stallmach A, Stein J, Sturm A, Teich N, Siegmund B. Collaborators: Aktualisierte S3-Leitlinie Colitis ulcerosa [August 2019 - AWMF-Registriernummer: 021–009]. Z Gastroenterol. 2019;57(11):1321–405.
Sulz MC, Burri E, Michetti P, Rogler G, Peyrin-Biroulet L, Seibold F. on behalf of the Swiss IBDnet, an official working group of the Swiss Society of Gastroenterology. Treat Algorithms Crohn’s Dis Dig. 2020;101(Suppl 1):43–57.
Binion DG, Louis E, Oldenburg B, Mulani P, Bensimon AG, Yang M, Chao J. Effect of adalimumab on work productivity and indirect costs in moderate to severe Crohn’s disease: a meta-analysis. Can J Gastroenterol. 2011;25(9):492–6.
Rutgeerts P, Sandborn WJ, Feagan BG, Reinisch W, Olson A, Johanns J, Travers S, Rachmilewitz D, Hanauer SB, Lichtenstein GR, de Villiers WJ, Present D, Sands BE, Colombel JF. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462–76.
Reinisch W, Sandborn WJ, Bala M, Yan S, Feagan BG, Rutgeerts P, Radford-Smith G, Xu S, Eisenberg D, Olson A, Colombel JF. Response and remission are associated with improved quality of life, employment and disability status, hours worked, and productivity of patients with ulcerative colitis. Inflamm Bowel Dis. 2007;13(9):1135–40.
Yarlas A, Maher SM, Bayliss MS, Lovley A, Cappelleri JC, DiBonaventura MD. Psychometric validation of the work productivity and activity impairment questionnaire in ulcerative colitis: results from a systematic literature review. J Patient Rep Outcomes. 2018;2(1):62.
Reilly MC, Gerlier L, Brabant Y, Brown M. Validity, reliability, and responsiveness of the work productivity and activity impairment questionnaire in Crohn’s disease. Clin Ther. 2008;30(2):393–404.
Reilly MC, Gooch KL, Wong RL, Kupper H, van der Heijde D. Validity, reliability and responsiveness of the work productivity and Activity Impairment Questionnaire in ankylosing spondylitis. Rheumatology (Oxford). 2010;49(4):812–9.
Reilly MA. Reilly Associates: WPAI General Information. 2002. http://www.reillyassociates.net/WPAI_General.html. Accessed 09 Nov 2020.
Irvine EJ, Feagan B, Rochon J, Archambault A, Fedorak RN, Groll A, Kinnear D, Saibil F, McDonald JW. Quality of life: a valid and reliable measure of therapeutic efficacy in the treatment of inflammatory bowel disease. Canadian Crohn’s Relapse Prevention Trial Study Group. Gastroenterology. 1994;106(2):287–96.
Janke KH, Steder-Neukamm U, Bauer M, Raible A, Meisner C, Hoffmann JC, Gregor M, Klump B, Häuser W. Lebensqualität bei chronisch entzündlichen Darmerkrankungen (CED): die deutsche Version des Inflammatory Bowel Disease Questionnaire (IBDQ-D) zur krankheitsspezifischen Lebensqualitätsmessung—erste Anwendung und Vergleich mit anderen internationalen Fassungen [Quality of life assessment in Inflammatory Bowel Disease (IBD): German version of the Inflammatory Bowel Disease Questionnaire (IBDQ-D; disease-specific instrument for quality of life assessment)—first application and comparison with international investigations]. Gesundheitswesen. 2005;67(8–9):656–64.
Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33.
Lewis JD, Chuai S, Nessel L, Lichtenstein GR, Aberra FN, Ellenberg JH. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm Bowel Dis. 2008;14(12):1660–6.
Teich N, Grümmer H, Jörgensen E, Liceni T, Holtkamp-Endemann F, Fischer T, Hohenberger S. Golimumab in real-world practice in patients with ulcerative colitis: twelve-month results. World J Gastroenterol. 2020;26(21):2852–63.
Ho EY, Cominelli F, Katz J. Ulcerative colitis: What is the optimal treatment goal and how do we achieve it? Curr Treat Options Gastroenterol. 2015;13(1):130–42.
Vogelaar L, Spijker AV, van der Woude CJ. The impact of biologics on health-related quality of life in patients with inflammatory bowel disease. Clin Exp Gastroenterol. 2009;2:101–9.
Odes S, Vardi H, Friger M, Wolters F, Russel MG, Riis L, Munkholm P, Politi P, Tsianos E, Clofent J, Vermeire S, Monteiro E, Mouzas I, Fornaciari G, Sijbrandij J, Limonard C, Van Zeijl G, O'morain C, Moum B, Vatn M, Stockbrugger R; European Collaborative Study on Inflammatory Bowel Disease Cost analysis and cost determinants in a European inflammatory bowel disease inception cohort with 10 years of follow-up evaluation. Gastroenterology. 2006;131(3):719–28.
van der Valk ME, Mangen MJ, Leenders M, Dijkstra G, van Bodegraven AA, Fidder HH, de Jong DJ, Pierik M, van der Woude CJ, Romberg-Camps MJ, Clemens CH, Jansen JM, Mahmmod N, van de Meeberg PC, van der Meulen-de Jong AE, Ponsioen CY, Bolwerk CJ, Vermeijden JR, Siersema PD, van Oijen MG, Oldenburg B; COIN study group and the Dutch Initiative on Crohn and Colitis. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFα therapy: results from the COIN study. Gut. 2014;63(1):72–9.
Regueiro M, Click B, Anderson A, Shrank W, Kogan J, McAnallen S, Szigethy E. Reduced unplanned care and disease activity and increased quality of life after patient enrollment in an inflammatory bowel disease medical home. Clin Gastroenterol Hepatol. 2018;16(11):1777–85.
Barberio B, Zingone F, Frazzoni L, D’Incà R, Maccarone MC, Ghisa M, Massimi D, Lorenzon G, Savarino EV. Real-life comparison of different anti-TNF biologic therapies for ulcerative colitis treatment: a retrospective cohort study. Dig Dis. 2021;39(1):16–24.
Acknowledgements
The authors thank Dr. Katharina Bakhaus, Alcedis GmbH, Gießen, Germany for medical writing assistance.
Funding
The study was funded by MSD Sharp & Dohme GmbH, Haar, Germany. Medical writing assistance was provided by Dr. Katharina Bakhaus, Alcedis GmbH, Gießen, Germany, funded by MSD Sharp & Dohme GmbH, Haar, Germany.
Author information
Authors and Affiliations
Contributions
Susanne Hohenberger contributed to study conception and study design; Niels Teich, Harald Grümmer, Eric Jörgensen, Thomas Liceni and Frank Holtkamp-Endemann participated in the acquisition, analysis, and interpretation of the data, and drafted the initial manuscript; Susanne Hohenberger and Tim Fischer reviewed the manuscript; all authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in compliance with the principles of the Declaration of Helsinki. The study protocol and the informed consent was reviewed and approved by the Institutional Review Board Ethics Committee of the Bavarian State Medical Association (Bayrische Landesärztekammer), Munich, Germany (no. 13104 from November 21, 2013). All study participants provided informed written consent prior to study enrolment. This non-interventional study was further registered at the Paul-Ehrlich-Institute, Langen, Germany (Registration Nr: NIS#255, https://www.pei.de/SharedDocs/awb/nis-0201-0300/0255.html).
Consent for publication
Not applicable.
Competing interests
Niels Teich has served as a speaker, a consultant and/or an advisory board member for AbbVie, Biogen, Falk Foundation, Janssen, MSD, Norgine, Takeda, Tillotts, Vifor and has received research funding from Ferring Arzneimittel GmbH; Harald Grümmer has received personal fees from MSD and AbbVie; Eric Jörgensen has received personal fees from MSD, Thomas Liceni has received personal fees from MSD, Frank Holtkamp-Endemann has received personal fees from MSD, Tim Fischer and Susanne Hohenberger are employees of MSD Sharp & Dohme GmbH. All authors certify that they have no financial interests that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Teich, N., Grümmer, H., Jörgensen, E. et al. Golimumab improves work productivity in patients suffering from moderate to severe ulcerative colitis: results of a prospective study over 24 months. BMC Gastroenterol 21, 161 (2021). https://doi.org/10.1186/s12876-021-01747-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-021-01747-z