
Abstract
Background
Empiric triple treatments for Helicobacter pylori (H. pylori) are increasingly unsuccessful. We evaluated factors associated with failure of these treatments in the central region of Portugal.
Methods
This single-center, prospective study included 154 patients with positive 13C-urea breath test (UBT). Patients with no previous H. pylori treatments (Group A, n = 103) received pantoprazole 40 mg 2×/day, amoxicillin 1000 mg 12/12 h and clarithromycin (CLARI) 500 mg 12/12 h, for 14 days. Patients with previous failed treatments (Group B, n = 51) and no history of levofloxacin (LVX) consumption were prescribed pantoprazole 40 mg 2×/day, amoxicillin 1000 mg 12/12 h and LVX 250 mg 12/12 h, for 10 days. H. pylori eradication was assessed by UBT 6–10 weeks after treatment. Compliance and adverse events were assessed by verbal and written questionnaires. Risk factors for eradication failure were determined by multivariate analysis.
Results
Intention-to-treat and per-protocol eradication rates were Group A: 68.9% (95% CI: 59.4–77.1%) and 68.8% (95% CI: 58.9–77.2%); Group B: 52.9% (95% CI: 39.5–66%) and 55.1% (95% CI: 41.3–68.2%), with 43.7% of Group A and 31.4% of Group B reporting adverse events. Main risk factors for failure were H. pylori resistance to CLARI and LVX in Groups A and B, respectively. Another independent risk factor in Group A was history of frequent infections (OR = 4.24; 95% CI 1.04–17.24). For patients with no H. pylori resistance to CLARI, a history of frequent infections (OR = 4.76; 95% CI 1.24–18.27) and active tobacco consumption (OR = 5.25; 95% CI 1.22–22.69) were also associated with eradication failure.
Conclusions
Empiric first and second-line triple treatments have unacceptable eradication rates in the central region of Portugal and cannot be used, according to Maastricht recommendations. Even for cases with no H. pylori resistance to the used antibiotics, results were unacceptable and, at least for CLARI, are influenced by history of frequent infections and tobacco consumption.
Similar content being viewed by others

Background
Approximately 50% of the world population is infected by Helicobacter pylori (H. pylori). This bacterium is responsible for multiple gastric diseases, including gastroduodenal ulcer, gastric adenocarcinoma and mucosa-associated lymphoid tissue lymphoma [1-3]. After almost thirty years of treating H. pylori, the ideal regimen has not been found. Some consensus conferences have recommended treatments with cure rates of ≥80% on an intention-to-treat (ITT) basis [4]. More recently, regimens of at least 90–95% efficacy, and preferably 95–100%, have been suggested as the standard of care [5].
Although meta-analyses have reported a decreased effectiveness for triple regimens containing clarithromycin (CLARI), the so-called “legacy triple therapy” is still widely used in several countries; the last Maastricht consensus maintained it as a first-line treatment under certain conditions [2,5,6]. The main reason for failure of this regimen is increased resistance to CLARI [2,7]. In Europe, primary H. pylori resistance to this drug increased from 9.9% to 17.5% in one decade [8,9]. In fact, H. pylori infections refractory to first treatment attempts are becoming more frequent with expanding use of antibiotics for multiple infections and the rising number of patients who undergo H. pylori treatment.
After failure of a therapy containing proton pump inhibitor (PPI) and CLARI, either bismuth-based quadruple therapy or PPI–levofloxacin (LVX) triple therapy is recommended by the most recent Maastricht consensus (2012) [2]. Multiple studies and meta-analysis have shown LVX to be a valid alternative to standard antimicrobial agents in first- and second-line regimens [10-12]. It is active even in H. pylori strains resistant to CLARI and metronidazole. Eradication rates of patients who harbor these doubly resistant strains are reportedly 92% if the isolates are sensitive to LVX [13]. Levofloxacin-based therapy can be used as second-line treatment in countries with low prevalence of LVX-resistant strains, but should probably be used only as third-line therapy if resistance to this fluoroquinolone is higher than 15% [14].
The H. pylori prevalence rate in Portuguese adults is 84.2% [15]. Although the aforementioned empirical triple-therapies are regularly used in the central region of Portugal, to our knowledge, there is no information about the efficacy of these treatments.
This study evaluated eradication rates of a 14-day triple therapy with PPI, amoxicillin and CLARI as empiric first-line therapy and a 10-day triple treatment with PPI, amoxicillin and LVX as a rescue therapy. As secondary aim, we intended to identify clinical and bacterial factors associated with treatment failure.
Methods
Patients
In this single-center study, patients with dyspepsia, iron-deficient anemia, need for chronic therapy with PPI and/or first-degree relatives with gastric carcinoma were prospectively considered for inclusion. Each had a recent positive 13C-urea breath test (UBT) and indication for upper endoscopy. Exclusion criteria were: age <18 years; pregnancy; lactating and/or fertile women who were not using safe contraceptive methods; history of allergy/hypersensitivity to any antibiotic or PPI; previous gastric malignancy and/or gastric surgery; current use of anticoagulants; marked thrombocytopenia; systemic severe disease (hepatic, cardio-respiratory or renal disease; uncontrolled diabetes; active malignant diseases, coagulopathies); use of antibiotics in the last 4 weeks; use of PPI in the last 2 weeks; intolerance/refusal to undergo upper endoscopy; previous H. pylori eradication treatments including fluoroquinolones or known use of this antibiotic for other infections.
They were divided in two groups: Group A—patients who had never received eradication treatments (n = 103; 73 female; mean age: 41.6 ± 12.9 years); Group B—patients who failed ≥1 eradication attempts that did not include LVX (n = 51; 39 female; mean age: 45.2 ± 13.9 years) and had no documented history of treatment with fluoroquinolones.
Empiric triple treatments and efficacy assessment
After undergoing upper endoscopies, patients in Group A were immediately prescribed pantoprazole 40 mg 2×/day, amoxicillin 1000 mg 12/12 h and CLARI 500 mg 12/12 h, for 14 days. Patients in Group B were prescribed pantoprazole 40 mg 2×/day, amoxicillin 1000 mg 12/12 h, and LVX 250 mg 12/12 h, for 10 days. We provided detailed explanation of the therapies and potential secondary effects to patients and their families, who were given diaries to record all administrations, side effects and symptoms during therapy. Patients were phoned immediately after treatment to register compliance and any potential symptoms or side effects. They underwent UBT 6–10 weeks after treatment to assess H. pylori status. At this time, compliance was confirmed by counting tablets returned by each patient. Treatment was considered complete if all medication was taken. Poor compliance was assumed if <80% of the prescribed drugs were taken.
Patients also returned the diaries they maintained during treatment and were asked to assess tolerability and efficacy of treatment in resolving symptoms by visual scales from 0 to 10 (0: not tolerable at all, 10: excellent tolerability; and 0: not efficacious, 10: fully efficacious, respectively). Adverse events were scored as mild, moderate or severe by their effect on daily activities (daily activities not limited, limited to some extent, or not possible at all, respectively) and need to discontinue treatment. The scoring system was based on that proposed by de Boer et al., with minor modifications [16]. During the study, patients could directly telephone an investigator to resolve any doubts or problems that occurred. Patients were allowed no antibiotics or antisecretory drugs 4 and 2 weeks, respectively, before their UBTs, which were considered positive if δ above baseline was ≥4‰.
Microbiological studies
As this was a research protocol and patients each had indication for upper endoscopy, we took biopsies for H. pylori culture, susceptibility testing and genotyping. Minimum inhibitory concentrations (MIC) for amoxicillin, CLARI and LVX, and point mutations in gene 23S rRNA and in the quinolones resistance-determining region of the gyrA gene were determined by a previously published protocol [17]. The cagA and vacA genotypes were obtained with real-time PCR by using specific primers selected from previously published works [18,19].
Stopping rules
Efficacy assessment was performed in each group for every 50 included patients. Inclusion was halted if this preliminary analysis revealed eradication rates <80%.
Statistics
Categorical variables are shown with their relative and absolute values; quantitative variables are expressed as mean ± standard deviation or median + range. The H. pylori eradication success was analyzed on both an ITT basis (including all eligible enrolled patients, regardless of compliance with study protocol; patients with unavailable data were assumed to be unsuccessfully treated) and “per protocol” (PP) (including only patients with good compliance and whose data was all evaluable at end of treatment).
Univariate analyses with Student’s t test, Mann–Whitney and Fisher’s exact test were used to evaluate associations between treatment effectiveness and age, sex, ethnicity, symptoms/indication for H. pylori treatment, body mass index (BMI), location of residence, education level, olive oil, alcohol and tobacco consumption, frequent infections, use of antibiotics in the last 12 months, family history of gastric pathology, H. pylori genotype, adverse events during treatment and compliance. Significant variables were subsequently included in a binomial logistic regression that assumed H. pylori eradication as the dependent variable. We used the statistical software package SPSS 20.0 (IBM Corp., Armonk, NY, USA).
Ethics
The study was approved by the ethical committee of our hospital and the Faculty of Medicine, and performed in accordance with the Declaration of Helsinki, the International Conference on Harmonisation of Good Clinical Practice Guidelines, and applicable local laws and regulations. Signed informed consent was obtained from each patient.
Results
Demographic variables
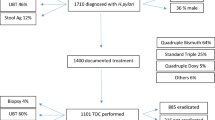
During the 4-year period, we included 154 patients (Group A: n = 103; Group B: n = 51; Table 1). Group B patients received a median of one eradication (range: 1 to 5) before inclusion with the following drugs: amoxicillin: 100%; CLARI: 92.2%; nitroimidazoles: 29.4%. The most common regimen was triple therapy with PPI, amoxicillin and CLARI, followed by PPI, CLARI and nitroimidazoles, and by PPI, amoxicillin and nitroimidazoles.
Compliance, tolerability/adverse events and follow-up losses
Of the 103 patients in Group A, 25 (24.3%) failed to take at least one pill during treatment but only 7 (6.8%) were noncompliant; and 45 Group A patients (43.7%) experienced adverse events (mild: 36; moderate: 8; severe: 1). The patient with severe side effects had an allergic reaction with diffuse rash. Patients’ median assessments of the regimens according to a visual scale, were tolerability: 8 (range: 2–10); efficacy: 8 (range: 0–10). Of the 51 patients in Group B, 3 (5.9%) failed to take at least one pill during treatment but only 2 (3.9%) were noncompliant; and 16 (31.4%) experienced adverse events (mild: 13; moderate: 2; severe: 1). The patient with severe side effects had intractable nausea, vomiting and diarrhea. Patients’ median assessments of treatment according to a visual scale, were tolerability: 8 (range: 2–10) and efficacy: 7 (range :2–9). No patient was lost to follow-up in either group.
Microbiological studies
Endoscopies with biopsies and culture were successfully and safely performed in all patients. H. pylori resistance to CLARI was detected in 22 isolates (21.4%) in Group A, and resistance to LVX in 13 (25.5%) isolates of Group B. Only one case showed resistance to amoxicillin, with a MIC level of 2 mg/L.
Twenty isolates of Group A had point mutations in the 23S rRNA gene (A2143G/A2142G), and 9 isolates of Group B in the gyrA gene. All isolates with mutations had in vitro resistance to antibiotics related with those genetic patterns. H. pylori cagA and vacA genotypes are presented in Table 2.
Efficacy of eradication therapy
For Group A, the eradication rate was 68.9% (95% CI 59.4–77.1%) on ITT and 68.8% (95% CI: 58.9–77.2%) on PP analysis. For Group B eradication rate was 52.9% (95% CI: 39.5–66%) on ITT and 55.1% (95% CI: 41.3–68.2%) on PP analysis.
Factors associated with eradication failure
We successfully treated 85.2% of patients with CLARI-susceptible H. pylori, but only 9.1% of patients with CLARI-resistant H. pylori (P <0.0001). None (0%) of the Group B patients with LVX-resistant infections had successful therapy, compared with 71.1% of patients with LVX-susceptible infections (P <0.0001). Antibiotic resistance was independently associated with treatment failure in both groups (Table 3); however multivariate analysis showed only history of frequent infections to independently predict treatment failure in Group A (odds ratio [OR]: 4.24; 95% CI: 1.04–17.24).
We then repeated the analysis excluding patients with CLARI-resistant strains in Group A and LVX-resistant strains in Group B. In susceptible-only Group A, history of frequent infections (OR: 4.76; 95% CI: 1.24–18.27) and active tobacco consumption (OR: 5.25; 95% CI: 1.22–22.69) were associated with treatment failure. In susceptible-only Group B, noncompliance was higher in patients with treatment failure but not significantly so (18.2% vs 0%; P = 0.078).
Discussion
Over the last two decades, widespread use of certain antibiotics has progressively decreased H. pylori antimicrobial susceptibility [20-22]. Resistance to CLARI and fluoroquinolones develops rapidly and cannot be overcome by increasing dose or duration of therapy [23]. The only way to identify effective drug combinations is to regularly monitor the success of H. pylori eradication and antibiotic resistance in every region.
Although PPI-CLARI-amoxicillin is probably the most common anti-H. pylori treatment, its eradication rates have decreased as resistance to antibiotics, particularly macrolides, rises. Almost all consensus statements and reviews still recommend it [2,4,20,24], although some authors suggest longer therapy duration (10–14 days instead of 7 days) or avoiding this regimen in regions where H. pylori resistance to CLARI is higher than 15–20% [2,20].
Levofloxacin-based second-line therapies are an encouraging strategy for addressing eradication failures. Multiple studies and meta-analyses show that combined PPI, amoxicillin and LVX regimens have better results, even in patients with more than one failed eradication attempt and CLARI- and metronidazole-resistant strains [10,12,25-27]. Unfortunately, fluoroquinolone resistance is rapidly increasing in many countries [9,28].
The H. pylori prevalence rate in Portugal is > 80% [15]. Multiple drugs commonly used for this infection, such as bismuth salts, tetracycline, furazolidone and rifabutin, are not easily available in Portugal, and doxycycline has disappointing results [17]. Although quadruple non-bismuth, sequential and hybrid therapies have been proposed as alternative first-line options, these treatments are complex. Empiric triple-therapy with CLARI is still the preferred first-line treatment and was recommended by the Portuguese Society of Gastroenterology in 2008 [29], with LVX-based treatment recently assuming a major second-line or rescue position. Although by 2000, Cabrita et al. reported H. pylori resistance to be 14.6% to CLARI and 11.1% to ciprofloxacin among adults from the Lisbon area [30], and a European multicenter study found resistance rates in the same population of 20.7% for CLARI and 33.3% for metronidazole, the empiric triple treatment remained the most common first-line regimen. In 2013, Megraud et al. reported primary resistance as 31.5% to CLARI and 26.3% to LVX in Portugal [9], and reportedly, obese patients proposed for bariatric surgery in northern Portugal have low eradication rates with CLARI- and LVX-based ITT triple therapies [31]. However, the efficacy of empiric H. pylori treatments in Portugal is little studied. To our knowledge, this is the first study of the efficacy of empiric triple regimens among patients in the central region of Portugal.
Our eradication rates were 68.9% for first-line ITT treatment with 14-day PPI-CLARI-amoxicillin and 52.9% for second-line/rescue treatment with 10-day PPI-LVX-amoxicillin. These first-line results are slightly better than the ones published by Cerqueira et al. for patients treated in 2009–2010, and our second-line/rescue results are similar [31].
The main risk factor for treatment failure is undoubtedly antibiotic resistance [7]. We found 21.4% of H. pylori isolates were for CLARI-resistant in Group A, and 25.5% were LVX-resistant in Group B. Only two patients with CLARI-resistant H. pylori, and none with LVX-resistant H. pylori, achieved eradication. Strains of H. pylori in Central Portugal are thus often resistant to CLARI and LVX. Notably, although Group B excluded patients with known histories of exposure to fluoroquinolones, its resistance rate to LVX was very high, probably due to common use and misuse of macrolides and fluoroquinolones for respiratory and urinary infections in Portugal and the cross-resistance of H. pylori to all macrolides and fluoroquinolones [9,32].
Macrolide-resistant H. pylori will certainly become more prevalent in the near future. A recent study of children found a primary resistance rate to CLARI of 34.7% [33]. Clearly macrolides and fluoroquinolones cannot be used to treat H. pylori in patients previously exposed to them, as resistance is practically universal in such circumstances [28].
Although we prescribed empiric treatments in patients for whom H. pylori susceptibility patterns were determined, this study was a research protocol, the main objective of which was to establish the efficacy of commonly used empiric treatments. Prescriptions were implemented immediately after the endoscopies, but we received antibiotic susceptibility results much later, 2–3 weeks after these procedures. Even among only those patients infected by H. pylori strains with no resistance to CLARI in Group A or LVX in Group B, eradication rates were 85.2% and 71.1%, respectively—well below the 90% accepted as the minimum efficacy rate for H. pylori treatment regimens [5]. As compliance and adverse event rates did not significantly differ, these factors cannot be considered as responsible for such failures. However, in Group B, treatment failure tended to be higher in noncompliant patients, although not significantly so, due to the limited number of patients.
History of frequent infections was a risk factor for eradication failure in all circumstances, even in patients with no H. pylori resistance to CLARI. One possible explanation is that our methodology underestimated H. pylori resistance to macrolides. Infection by multiple strains, with different resistance patterns, is common, but subculture testing might mask identification of resistant strains [34,35]. This is a potential cause of treatment failure and negative cultures; thus direct molecular studies of biopsy specimens might be more illuminating [36]. For CLARI, De Francesco et al. recently reported that the prevalence of usually identified point mutations A2143G, A2142G and A2142C might be decreasing [37]. However, we identified mutations in positions A2143G/A2142G of 23S rRNA gene in 20 of the 22 resistant strains. Notably, the methodology we used does not distinguish A2143G from A2142G, but the clinical significance of this limitation is controversial, although some authors state that the A2143G mutation is the one that significantly lowers H. pylori eradication rate [7]. Point mutation A2142C was not detected and we did not search for other mutations; this can be a limitation of our work [37].
Active tobacco consumption was also a risk factor for failure in patients with CLARI-susceptible H. pylori. This negative effect is already known and may result from a reduction of antibiotic delivery due to a decreased gastric blood flow, lower intragastric pH or increased activity of the vacuolating toxin activity in gastric cells [2,38].
We had only one case of H. pylori resistance to amoxicillin, but that did not determine eradication failure. Resistance to this antibiotic has also been held responsible for treatment failure, but there is no accurate estimate of its effect [39,40].
H. pylori genotype can be important as it is reported to be strongly associated with eradication success, antibiotic susceptibility and H. pylori virulence factors [14,41,42]. Genotypes cagA negative and vacA s2m2 induce less inflammation and may contribute to reduced antibiotic delivery and decreased H. pylori eradication. Our univariate analysis also suggested this association but logistic regression did not confirm it, although the limited number of patients might have affected these results.
Another possible explanation for our results is that PPI and amoxicillin might have been prescribed in inadequate doses and/or intervals between administrations. Generally, Caucasians metabolize PPI quickly and might need higher doses and frequency of PPI administration [43]. The same might be needed for amoxicillin, as its bactericidal effect depends on % time above MIC and its plasma half-life is very short; thus frequent dosing for amoxicillin is necessary [44]. However, we prescribed the combinations traditionally supported in the literature. Different combinations, with four daily administrations of PPI and amoxicillin, could eventually be tested in future studies.
Various diseases can influence H. pylori eradication rates. Patients with peptic ulcers tend to respond better to treatment than patients with non-ulcer dyspepsia [2,45,46]. Although our study found no association between disease manifestations and therapeutic failure, relatively few patients with peptic ulcers were included. The predominance of non-ulcer dyspepsia in our series explains the high number of female patients, as non-ulcer dyspepsia is more common in women [47].
Another limitation of our study was the relatively small study cohort. First, we included only patients with previous positive UBT and indications for upper endoscopy, with very restrictive exclusion criteria, which limited the number of includible patients. Second, when our protocol was designed, no clear rules were in place on interrupting treatment of patients in prospective studies for H. pylori treatments. However, Maastricht III consensus established that proposed therapies must achieve eradication rates ≥80%. In following these recommendations, we decided to perform preliminary analyses of each 50 patients and to stop the study if eradication rate was less than 80%. That threshold occurred in the first analysis for Group B and in the second one for Group A. Even stricter stopping rules were more recently proposed by Graham (50 patients; eradication rate <90%) [48].
Finally, some recent studies suggest that 14-day LVX-based triple therapy can provide a >90% H. pylori eradication rate, but a 10-day duration may be suboptimal [49]. Although our LVX-treated patients in Group B received a 10-day regimen, 7- and 10-day regimens with LVX were acceptable when our protocol was designed; we chose the longer one specifically to optimize results. Another problem with LVX is lack of consensus about dosage: 250 mg 2×/day, 500 mg 1×/day, or 500 mg 2×/day. The 10-day 500 mg 2×/day dose reportedly has higher eradication rates, but still <80% [50]. Other authors still use a 10-day rescue regimen with PPI, amoxicillin 1 g and LVX 250 mg, all 2×/day [51].
Conclusions
Empiric triple-therapies with PPI-CLARI-amoxicillin and PPI-LVX-amoxicillin are ineffective as first- and second-line H. pylori regimens, respectively, in the central region of Portugal and they are now unacceptable as treatments. The main reason for treatment failure is high H. pylori resistance to CLARI and LVX.
History of frequent infections and active tobacco consumption contribute to unsuccessful treatments with CLARI for H. pylori strains with no resistance to this drug. In patients with these characteristics, another tailored first-line treatment is preferable.
For first-line empiric treatment, we suggest empiric concomitant or hybrid therapies for 14 days. However, study of the efficacy of these treatments in our region is urgently needed. In light of the scarcity of effective H. pylori antimicrobials in our country, if these regimens fail, it is our opinion that second-line treatments must be prescribed according to susceptibility testing.
Abbreviations
- H. pylori :
-
Helicobacter pylori
- ITT:
-
Intention-to-treat
- PPI:
-
Proton pump inhibitor(s)
- UBT:
-
13C-urea breath test
- MIC:
-
Minimum inhibitory concentrations
- PP:
-
Per protocol
- OR:
-
Odds ratio
References
Correa P, Piazuelo MB. Natural history of Helicobacter pylori infection. Dig Liver Dis. 2008;40(7):490–6.
Malfertheiner P, Megraud F, O’Morain CA, Atherton J, Axon AT, Bazzoli F, et al. Management of Helicobacter pylori infection–the Maastricht IV/Florence Consensus Report. Gut. 2012;61(5):646–64.
Chuah SK, Tsay FW, Hsu PI, Wu DC. A new look at anti-Helicobacter pylori therapy. World J Gastroenterol. 2011;17(35):3971–5.
Malfertheiner P, Megraud F, O’Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 2007;56(6):772–81.
Graham DY, Fischbach L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut. 2010;59(8):1143–53.
Fischbach LA, Goodman KJ, Feldman M, Aragaki C. Sources of variation of Helicobacter pylori treatment success in adults worldwide: a meta-analysis. Int J Epidemiol. 2002;31(1):128–39.
Giorgio F, Principi M, De Francesco V, Zullo A, Losurdo G, Di Leo A, et al. Primary clarithromycin resistance to Helicobacter pylori: is this the main reason for triple therapy failure? World J Gastrointest Pathophysiol. 2013;4(3):43–6.
Glupczynski Y, Megraud F, Lopez-Brea M, Andersen LP. European multicentre survey of in vitro antimicrobial resistance in Helicobacter pylori. Eur J Clin Microbiol Infect Dis. 2001;20(11):820–3.
Megraud F, Coenen S, Versporten A, Kist M, Lopez-Brea M, Hirschl AM, et al. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut. 2013;62(1):34–42.
Gisbert JP, Morena F. Systematic review and meta-analysis: levofloxacin-based rescue regimens after Helicobacter pylori treatment failure. Aliment Pharmacol Ther. 2006;23(1):35–44.
Gisbert JP, Pajares JM. Helicobacter pylori “rescue” therapy after failure of two eradication treatments. Helicobacter. 2005;10(5):363–72.
Saad RJ, Schoenfeld P, Kim HM, Chey WD. Levofloxacin-based triple therapy versus bismuth-based quadruple therapy for persistent Helicobacter pylori infection: a meta-analysis. Am J Gastroenterol. 2006;101(3):488–96.
Gatta L, Zullo A, Perna F, Ricci C, De Francesco V, Tampieri A, et al. A 10-day levofloxacin-based triple therapy in patients who have failed two eradication courses. Aliment Pharmacol Ther. 2005;22(1):45–9.
Sugimoto M, Yamaoka Y. Virulence factor genotypes of Helicobacter pylori affect cure rates of eradication therapy. Arch Immunol Ther Exp (Warsz). 2009;57(1):45–56.
Bastos J, Peleteiro B, Barros R, Alves L, Severo M, de Fatima PM, et al. Sociodemographic determinants of prevalence and incidence of Helicobacter pylori infection in Portuguese adults. Helicobacter. 2013;18(6):413–22.
de Boer WA, Thys JC, Borody TJ, Graham DY, O’Morain C, Tytgat GN. Proposal for use of a standard side effect scoring system in studies exploring Helicobacter pylori treatment regimens. Eur J Gastroenterol Hepatol. 1996;8(7):641–3.
Almeida N, Romaozinho JM, Donato MM, Luxo C, Cardoso O, Cipriano MA, et al. Triple therapy with high-dose proton-pump inhibitor, amoxicillin, and doxycycline is useless for Helicobacter pylori eradication: a proof-of-concept study. Helicobacter. 2014;19(2):90–7.
Atherton JC, Cao P, Peek Jr RM, Tummuru MK, Blaser MJ, Cover TL. Mosaicism in vacuolating cytotoxin alleles of Helicobacter pylori, association of specific vacA types with cytotoxin production and peptic ulceration. J Biol Chem. 1995;270(30):17771–7.
Santos A, Queiroz DM, Menard A, Marais A, Rocha GA, Oliveira CA, et al. New pathogenicity marker found in the plasticity region of the Helicobacter pylori genome. J Clin Microbiol. 2003;41(4):1651–5.
Vakil N, Megraud F. Eradication therapy for Helicobacter pylori. Gastroenterology. 2007;133(3):985–1001.
Boyanova L, Mitov I. Geographic map and evolution of primary Helicobacter pylori resistance to antibacterial agents. Expert Rev Anti Infect Ther. 2010;8(1):59–70.
De Francesco V, Giorgio F, Hassan C, Manes G, Vannella L, Panella C, et al. Worldwide H. pylori antibiotic resistance: a systematic review. J Gastrointestin Liver Dis. 2010;19(4):409–14.
Graham DY, Fischbach LA. Empiric therapies for Helicobacter pylori infections. CMAJ. 2011;183(9):E506–8.
Fock KM, Katelaris P, Sugano K, Ang TL, Hunt R, Talley NJ, et al. Second Asia-Pacific Consensus Guidelines for Helicobacter pylori infection. J Gastroenterol Hepatol. 2009;24(10):1587–600.
Gisbert JP. Rescue therapy for Helicobacter pylori infection 2012. Gastroenterol Res Pract. 2012;2012:974594.
Gisbert JP. “Rescue” regimens after Helicobacter pylori treatment failure. World J Gastroenterol. 2008;14(35):5385–402.
Gisbert JP, Gisbert JL, Marcos S, Jimenez-Alonso I, Moreno-Otero R, Pajares JM. Empirical rescue therapy after Helicobacter pylori treatment failure: a 10-year single-centre study of 500 patients. Aliment Pharmacol Ther. 2008;27(4):346–54.
Graham DY, Shiotani A. New concepts of resistance in the treatment of Helicobacter pylori infections. Nat Clin Pract Gastroenterol Hepatol. 2008;5(6):321–31.
Gastrenterologia SPd. Normas de orientação clínica - helicobacter pylori. GE - Jornal Português de Gastrenterologia. 2008;15:192–4.
Cabrita J, Oleastro M, Matos R, Manhente A, Cabral J, Barros R, et al. Features and trends in Helicobacter pylori antibiotic resistance in Lisbon area, Portugal (1990–1999). J Antimicrob Chemother. 2000;46(6):1029–31.
Cerqueira RM, Correia MR, Fernandes CD, Vilar H, Manso MC. Cumulative Helicobacter pylori eradication therapy in obese patients undergoing gastric bypass surgery. Obes Surg. 2013;23(2):145–9.
Adriaenssens N, Coenen S, Versporten A, Muller A, Minalu G, Faes C, et al. European surveillance of antimicrobial consumption (ESAC): outpatient antibiotic use in Europe (1997–2009). J Antimicrob Chemother. 2011;66 Suppl 6:vi3–vi12.
Oleastro M, Pelerito A, Nogueira P, Benoliel J, Santos A, Cabral J, et al. Prevalence and incidence of Helicobacter pylori Infection in a healthy pediatric population in the Lisbon area. Helicobacter. 2011;16(5):363–72.
Kim JJ, Kim JG, Kwon DH. Mixed-infection of antibiotic susceptible and resistant Helicobacter pylori isolates in a single patient and underestimation of antimicrobial susceptibility testing. Helicobacter. 2003;8(3):202–6.
Van Doorn LJ, Figueiredo C, Megraud F, Pena S, Midolo P, Queiroz DM, et al. Geographic distribution of vacA allelic types of Helicobacter pylori. Gastroenterology. 1999;116(4):823–30.
Kanizaj TF, Kunac N. Helicobacter pylori: future perspectives in therapy reflecting three decades of experience. World J Gastroenterol. 2014;20(3):699–705.
De Francesco V, Zullo A, Giorgio F, Saracino I, Zaccaro C, Hassan C, et al. Change of point mutations in Helicobacter pylori rRNA associated with clarithromycin resistance in Italy. J Med Microbiol. 2014;63(Pt 3):453–7.
Suzuki T, Matsuo K, Ito H, Sawaki A, Hirose K, Wakai K, et al. Smoking increases the treatment failure for Helicobacter pylori eradication. Am J Med. 2006;119(3):217–24.
Gerrits MM, van Vliet AH, Kuipers EJ, Kusters JG. Helicobacter pylori and antimicrobial resistance: molecular mechanisms and clinical implications. Lancet Infect Dis. 2006;6(11):699–709.
Han SR, Bhakdi S, Maeurer MJ, Schneider T, Gehring S. Stable and unstable amoxicillin resistance in Helicobacter pylori: should antibiotic resistance testing be performed prior to eradication therapy? J Clin Microbiol. 1999;37(8):2740–1.
Agudo S, Perez-Perez G, Alarcon T, Lopez-Brea M. High prevalence of clarithromycin-resistant Helicobacter pylori strains and risk factors associated with resistance in Madrid. Spain J Clin Microbiol. 2010;48(10):3703–7.
van Doorn LJ, Schneeberger PM, Nouhan N, Plaisier AP, Quint WG, de Boer WA. Importance of Helicobacter pylori cagA and vacA status for the efficacy of antibiotic treatment. Gut. 2000;46(3):321–6.
Miehlke S, Hansky K, Schneider-Brachert W, Kirsch C, Morgner A, Madisch A, et al. Randomized trial of rifabutin-based triple therapy and high-dose dual therapy for rescue treatment of Helicobacter pylori resistant to both metronidazole and clarithromycin. Aliment Pharmacol Ther. 2006;24(2):395–403.
Shirai N, Sugimoto M, Kodaira C, Nishino M, Ikuma M, Kajimura M, et al. Dual therapy with high doses of rabeprazole and amoxicillin versus triple therapy with rabeprazole, amoxicillin, and metronidazole as a rescue regimen for Helicobacter pylori infection after the standard triple therapy. Eur J Clin Pharmacol. 2007;63(8):743–9.
Broutet N, Tchamgoue S, Pereira E, Lamouliatte H, Salamon R, Megraud F. Risk factors for failure of Helicobacter pylori therapy–results of an individual data analysis of 2751 patients. Aliment Pharmacol Ther. 2003;17(1):99–109.
Wolle K, Malfertheiner P. Treatment of Helicobacter pylori. Best Pract Res Clin Gastroenterol. 2007;21(2):315–24.
Schmulson M, Adeyemo M, Gutierrez-Reyes G, Charua-Guindic L, Farfan-Labonne B, Ostrosky-Solis F, et al. Differences in gastrointestinal symptoms according to gender in Rome II positive IBS and dyspepsia in a Latin American population. Am J Gastroenterol. 2010;105(4):925–32.
Graham DY. Efficient identification and evaluation of effective Helicobacter pylori therapies. Clin Gastroenterol Hepatol. 2009;7(2):145–8.
Tai WC, Chiu CH, Liang CM, Chang KC, Kuo CM, Chiu YC, et al. Ten-Day versus 14-Day levofloxacin-containing triple therapy for second-line anti-Helicobacter pylori Eradication in Taiwan. Gastroenterol Res Pract. 2013;2013:932478.
Gisbert JP, Perez-Aisa A, Bermejo F, Castro-Fernandez M, Almela P, Barrio J, et al. Second-line therapy with levofloxacin after failure of treatment to eradicate helicobacter pylori infection: time trends in a Spanish Multicenter Study of 1000 patients. J Clin Gastroenterol. 2013;47(2):130–5.
De Francesco V, Hassan C, Ridola L, Giorgio F, Ierardi E, Zullo A. Sequential, concomitant and hybrid first-line therapies for Helicobacter pylori eradication: a prospective randomized study. J Med Microbiol. 2014;63(Pt 5):748–52.
Acknowledgments
The authors are indebted to Dr. João Casalta for his help in the statistical analysis. This work was supported by a grant from the Portuguese Institute Fundação para a Ciência e Tecnologia (PIC/IC/83122/2007).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
The involvement of each author was as follows: NA (1-8); MMD (1,2,5,7); JMR (1-8); CL (1,2,5); OC (1,2,5); MAC (1,2,5); CM (1,2,5); AF (2-6); CC (2,7); CS (5,8), [Key: (1) Study concept and design; (2) Acquisition of data; (3) Analysis and interpretation of data; (4) Drafting of the manuscript; (5) Critical revision of the manuscript for important intellectual content; (6) Statistical analysis; (7) Administrative, technical, or material support; (8) Study supervision.], All authors read the final version of this manuscript, approve its’ content and submission for publication.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Almeida, N., Donato, M.M., Romãozinho, J.M. et al. Beyond Maastricht IV: are standard empiric triple therapies for Helicobacter pylori still useful in a South-European country?. BMC Gastroenterol 15, 23 (2015). https://doi.org/10.1186/s12876-015-0245-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-015-0245-y