
Abstract
Background
Evidence concerning health care use related to virtual visits is conflicting. More research has been called for regarding the effectiveness of text-based virtual visits (eVisits). Therefore, we investigated patient characteristics, diagnoses, and subsequent health care contacts after eVisits to primary care.
Methods
We conducted a register-based cohort study of eVisits to an all-virtual public primary care unit in Sweden and subsequent health care contacts within 14 days. Data for 2021 were acquired from the regional health care databases. Diagnoses were sorted into relevant diagnostic groups, such as skin diagnoses and respiratory tract diagnoses. Multiple logistic regression was performed with subsequent health care contact as the outcome variable and diagnostic group for the eVisit as the predictor variable. Analyses were adjusted for age, sex, and socioeconomic index.
Results
There were 5817 eVisits to a nurse and 4267 eVisits to a general practitioner (N = 10 084). Most patients were 20 to 39 years of age (41.8%). Skin diagnoses were most frequent (47.3%), followed by respiratory tract diagnoses (19.9%). Approximately one-fourth (25.8%) of the patients who completed an eVisit with a nurse or a general practitioner had a subsequent face-to-face visit within 14 days, mostly in primary care. Subsequent contacts were more frequent after an eVisit to a nurse than to a general practitioner. After an eVisit to a general practitioner, patients with infections (especially respiratory tract but also urinary tract) and unspecified diagnoses (especially skin-related) were more likely to require further health care contact compared to a group with various other diagnoses.
Conclusions
eVisits to an all-virtual primary care unit may be appropriate for uncomplicated medical complaints. Nonetheless, the effectiveness of eVisits in terms of substitution of physical visits, and resource utilization in relation to the more complex care needs of a primary care population, should be further studied.
Similar content being viewed by others


Background
After a gradual increase during the last decade, virtual visits to primary care were catalyzed by the COVID-19 pandemic [1,2,3,4]. The visits can be conducted via video, or via synchronous or asynchronous text [3, 5]. Expectations from policymakers and health care providers have been numerous and include increased access and improved efficiency [5, 6]. However, concerns have been raised regarding the effects on health care equity and resource use [5,6,7].
According to prior research, users of virtual visits to primary care are more commonly women, younger than 65 years of age and have high socioeconomic status [3, 8,9,10]. Recent systematic reviews indicate that clinical outcomes may be comparable to face-to-face visits, but more research is needed [8, 11, 12]. Regarding health care use related to virtual visits, the evidence is mixed [8, 11, 12]. Most prior studies have been conducted in the United States [2, 8, 11, 12]. Research has primarily concerned video visits, or covered several types of remote forms of contact, with fewer studies specifically on text-based visits.
A commonly used term for text-based visits is “eVisits”. In this paper, we define an eVisit as a synchronous or asynchronous two-way communication via a digital platform (app- or web-based). As of 2023, most Swedish primary care providers had introduced virtual visits, and more than half of the providers specifically offered or planned to offer eVisits via asynchronous chat [13, 14]. However, scientific publications regarding eVisits in a Swedish context were sparse.
More research has been called for regarding the effectiveness of eVisits, and to determine which conditions are suitable for eVisits [11]. One way to assess this may be through analysis of whether patients require additional health care contact following an eVisit. Prior studies vary in context and describe subsequent face-to-face contact rates from 5 to 25% after an eVisit to primary care [8, 11, 15,16,17,18,19,20,21,22,23]. Some register-based comparisons have been made with face-to-face visits, primarily regarding urinary tract infections and respiratory tract infections, finding similar subsequent health care contact frequencies [18,19,20,21,22,23]. However, there may be a selection bias when comparing virtual and face-to-face care, as the patients differ in characteristics and may also differ in seriousness of the condition [24]. No studies have investigated the need for follow-up depending on health care professional for the eVisit nor compared follow-up between different conditions when treated via eVisit. Such information could indicate seriousness of symptoms and if eVisits substitute physical visits, which would add to the ongoing discussion regarding the effectiveness of eVisits in different contexts.
The aim of this study was therefore to describe patient characteristics, diagnoses, and subsequent health care contact in a cohort of patients who completed an eVisit to a nurse or a physician in primary care in southern Sweden during 2021, and to analyze whether the need for subsequent health care contacts varied depending on diagnosis for the eVisit.
Method
Setting
Sweden has a regionalized health care system with universal health coverage. Swedish primary care is delivered at primary health care centers (PHCCs), which can be run through a regional public provider or through private providers who are publicly reimbursed. Skåne is the third largest region in Sweden by population, with 1.4 million inhabitants distributed between urban and rural areas in the southernmost part of the country [25].
In 2020, the public primary care provider in Region Skåne initiated an all-virtual unit for eVisits called Primary Health Care Skåne Online (PHC Online). The primary aim of the service was to provide eVisits to patients listed at a public PHCC in Region Skåne, as virtual visits were not otherwise provided by the PHCCs. However, the service was available to all inhabitants. The opening hours were weekdays 8am through 5pm and weekends 10am through 3pm. The service was operated separately from the physical PHCCs but was primarily staffed by general practitioners (GPs) and nurses who also worked at a public PHCC. Patients could be recommended to seek care at PHC Online when they got in contact with their public PHCC with a suitable complaint. They could also contact PHC Online directly without any prior health care contact. The service was only recommended for patients with certain types of complaints (allergies, skin conditions, urogenital problems, airways and infections, stomach and intestines, common childhood problems, and renewal of prescription). The visit was initiated with an automated digital anamnesis. Patients selected their type of complaint, and subsequent questions were prompted by the patients’ selection. Patients were also asked to fill out a general health profile. A nurse then initiated an eVisit through text communication that could be synchronous or asynchronous, primarily depending on whether the patient was available. If needed, the nurse offered the patient to continue the eVisit with a GP. In this paper, we refer to the eVisits as “with a nurse” or “with a GP” even though most eVisits with a GP were preceded by a contact with a nurse. Patients and staff could attach photos as part of the text-based communication. The nurse and the GP had the option to convert the visit into a video call, but the option was rarely used.
Study design and participants
We conducted a register-based cohort study of the patients who completed an eVisit with PHC Online from February 19 to December 31, 2021. In addition to demographics and the Swedish version of the International Classification of Diseases (ICD-10-SE) diagnoses for the eVisit, we studied subsequent contacts with any health care facility in Region Skåne within 14 days after the eVisit. Furthermore, we analyzed whether subsequent health care contact rates differed depending on the diagnosis for the eVisit. We only included index eVisits, i.e., the patient’s first visit to PHC Online during the study period. Patients who had completed a face-to-face or virtual visit to a physician for the same diagnostic group within 14 days before the eVisit were excluded. All other index eVisits were analyzed, including eVisits where the patient may have been advised by the nurse or GP to seek physical care. The study was carried out in adherence with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [26].
Data sources and variables
Pseudonymized datasets of eVisits to PHC Online, and health care contacts within 14 days before and after the eVisit, were acquired from Region Skåne’s Health Care Databases. Data did not include health care units outside of Region Skåne. Neither did data include diagnoses set by health care units that were not regionally funded (a minority of units, totaling 1% of Sweden’s health care costs [3]). Variables included age, sex, which PHCC the patient was registered at, type of health care contact, health care unit, health care professional and visit ICD-10 diagnoses.
Visit diagnoses were sorted into relevant diagnostic groups based on common complaints for patients using PHC Online: skin, urinary tract, respiratory tract, gastrointestinal, genital, eye, psychiatric, other, and unspecified diagnoses (ICD-10 codes that did not indicate symptom or diagnosis). As a measure of socioeconomic index, we acquired the Care Need Index (CNI) for the PHCC that the patient was registered at, i.e., as a clinic-level index [27]. The CNI includes seven different factors: single households > 65 years, children < 5 years, single parents, birthplace abroad, high mobility, low educational level, and unemployment. It is used in Sweden as a measure for the allocation of public primary care resources [27].
Outcome variables
A subsequent health care contact was defined as any type of contact with a nurse or a physician at any health care level within 14 days after the index eVisit. Modes of subsequent health care contact included face-to-face visit, virtual visit, telephone contact, and other remote contact (virtual or letter). Health care levels included primary care, emergency unit, inpatient care, and specialist outpatient care. The subsequent contacts were grouped into outcome variables regarding different types of contact (mode of contact, health care level, health care professional, and whether the subsequent contact concerned the same diagnostic group as the eVisit) and dichotomized as “yes” or “no”, where “yes” indicated one or more subsequent contacts and “no” indicated no subsequent contact of the specified type.
Sample size
The sample size was calculated to discern a 5 percentage point difference in subsequent health care contact rates between common diagnostic groups for the eVisit with an α level of 0.05 and 80% power. From preliminary data from PHC Online, we estimated the occurrence of common diagnostic groups (skin, urinary tract, and respiratory tract diagnoses) to be at least 10% of the study population for each diagnostic group. The follow-up rates in previous studies of 5–25% were used as an estimate [8, 11, 15,16,17,18,19,20,21,22,23]. Power calculations rendered a study size of approximately 4500 patients who had completed an eVisit with a nurse or a GP, respectively.
Statistical methods
IBM SPSS Statistics (version 29) was used for statistical processing. Patient characteristics per diagnostic group, and characteristics of those who had subsequent health care contacts, were visualized through crosstabulations. Differences between groups were analyzed using Pearson’s chi-square test for categorical variables and one-way ANOVA test or Kruskal-Wallis test for continuous variables as appropriate. Post-hoc tests were conducted using the Bonferroni correction. Data were analyzed to ensure that assumptions for the use of logistic regression analysis were met.
Multiple logistic regression was performed with subsequent contact (yes/no) as the outcome variable and diagnostic group for the eVisit as the predictor variable. The diagnostic groups gastrointestinal, genital, eye, psychiatric, and other were merged into the group “all other diagnoses”. The group “all other diagnoses” was used as the reference as it constituted a varied selection of primary care diagnoses. As a subsequent analysis, the largest diagnostic groups (skin and respiratory tract diagnoses) were separated into subgroups. The regression models were adjusted for age, sex, and CNI of the patient’s registered PHCC. Type of health care professional for the eVisit was considered a mediator rather than a confounder of effects and was therefore not used for adjustment as the regression model was intended to study total effects (Additional file 1) [28]. Instead, analyses were conducted for all eVisits, and separately for eVisits to a nurse and to a GP. For goodness of fit, Nagelkerke R2 was reported and the Hosmer-Lemeshow test was applied.
Regarding the handling of missing data, this almost exclusively concerned diagnoses for index eVisits and subsequent health care contacts. Index eVisits that did not have a diagnosis were included in descriptive statistics but excluded from the analyses regarding follow-up as they lacked the predictor variable (diagnostic group). Considering the subsequent health care contacts, analysis regarding follow-up for the same diagnostic group as the index eVisit was only performed for the types of contacts where at least 95% had a diagnosis.
Results
Sample characteristics
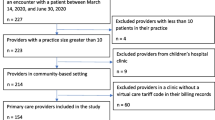
Figure 1 illustrates the inclusion and exclusion of eVisits. A total of 10 084 eVisits were analyzed, of which 5817 were visits to a nurse and 4267 were visits to a GP (Fig. 1).

Flow chart of eVisits included and excluded at each stage of the study
eVisits
Patient characteristics are presented in Table 1. Women completed more eVisits than men. Considering age groups, young children aged 1 to 5 years (1051/10 084, 10.4%) and adults aged 20–39 years were the most frequent eVisitors, while few patients were 60 years of age or older. The median CNI for the patients’ registered PHCC was close to the median value for all PHCCs in the studied region. The most common diagnostic group was skin diagnoses, followed by respiratory tract diagnoses and urinary tract diagnoses. Less common diagnostic groups, such as gastrointestinal and eye diagnoses, were summarized into the group “all other diagnoses” (Table 1).
Table 2 details patient characteristics per diagnostic group, including statistical and post hoc testing of differences between groups. Patients with urinary tract diagnoses were almost exclusively women and of older age compared to the other diagnostic groups. Patients with urinary tract diagnoses and “all other diagnoses” were more often handled by a GP (Table 2).
Subsequent health care contact
All registered subsequent health care contacts are summarized in Additional file 2. Due to missing data on diagnosis for several types of contacts, only subsequent face-to-face visits to a physician could be analyzed regarding follow-up for the same diagnostic group as the eVisit.
Frequencies of different types of subsequent health care contacts are specified in Additional file 3. A total of 43.6% (4395/10 084) of the eVisits were followed by one or more remote or face-to-face health care contacts within 14 days. The frequency of subsequent face-to-face visits to a nurse or a physician was 25.8% (2606/10 084). Most of the subsequent contacts took place in primary care, with the most common in-person contact being a face-to-face visit to a primary care physician (1671/10 084, 16.6%). The frequency of emergency unit visits (160/10 084, 1.6%) and admissions to hospital (36/10 084, 0.4%) was low, especially if limited to the same diagnostic group as the eVisit (50/9872, 0.5% and 8/9872, 0.1%, respectively).
Characteristics of the eVisits that were followed by a subsequent health care contact are shown in Table 3. Women had a slightly higher frequency of subsequent contacts than men. Subsequent contacts were markedly more frequent after an eVisit to a nurse than to a GP, including subsequent face-to-face visits with 31.1% vs. 18.7%. Considering only eVisits to a GP, 11.4% of the patients had a subsequent face-to-face visit to a physician in primary care. If only subsequent visits for the same diagnostic group were considered, the follow-up frequency was 6.5% (Table 3).
Subsequent health care contact by diagnostic group
The number of subsequent health care contacts per diagnostic group are reported in Table 3, while the results of regression analyses are reported in Tables 4 and 5, and Additional file 4. The patients who had completed an eVisit for a respiratory tract diagnosis, a urinary tract diagnosis, or an unspecified diagnosis had an increased odds ratio for subsequent health care contacts compared to the group with “all other diagnoses” (Table 4). This was primarily evident after eVisits to a GP (Additional file 4 and Table 5). As shown in Table 5, the difference became more marked when the subsequent contact was specified to a visit to a physician in primary care for the same diagnostic group as the eVisit. Dividing the diagnostic groups into subgroups revealed markedly increased odds for subsequent health care contact after an eVisit to a GP for respiratory tract infections and unspecified skin diagnoses compared to the group “all other diagnoses” (Table 5). We did not divide urinary tract diagnoses into subgroups as the group almost exclusively consisted of urinary tract infections (539/568, 94.9%).
Discussion
Main findings
This study of patient characteristics, diagnoses, and subsequent health care contacts after eVisits to an all-virtual public primary care unit found that women and young to middle-aged individuals were the most frequent visitors, and that skin conditions were the most common diagnostic group. Approximately one-fourth (25.8%) of the patients who completed an eVisit with a nurse or a GP had a subsequent face-to-face visit within 14 days, mostly in primary care. Subsequent contacts were more frequent after an eVisit to a nurse than to a GP. After an eVisit to a GP, patients with infections (especially respiratory tract but also urinary tract) and unspecified diagnoses (especially skin-related) were more likely to require further health care contact compared to a group with various other diagnoses.
Strengths and limitations
PHC Online was one of the first services for eVisits to public primary care, and it was introduced in Sweden’s third most populous region, which increases the novelty as well as the generalizability of the results. Another strength of this study was that we used a large dataset obtained from a regional claims database that is also maintained for research purposes. We studied all patients who completed a visit with PHC Online during almost one year, thus accounting for seasonal variations. Furthermore, we described several types of subsequent health care contacts, providing a comprehensive picture of health care use after eVisits. Finally, we analyzed subsequent contacts for the same diagnostic group as the eVisit, which increases precision.
Considering the demographics of the study population, comparably few participants were older than 60 years of age. Thus, our results are primarily valid for patients under 60 years of age, i.e., the age group that currently uses virtual care. Furthermore, patients were instructed to only use the service for certain complaints, which excluded patients with other types of complaints. It should also be noted that the study took place in 2021, during the latter stages of the COVID-19 pandemic. Thus, the selection of patients may have differed from non-pandemic conditions. These factors decrease generalizability.
Regarding missing data, a diagnosis was lacking in a significant proportion of all subsequent contacts with a nurse as well as in subsequent remote contacts with a physician. Consequently, for these types of subsequent contacts, we could not make any conclusions regarding follow-up for the same diagnostic group as the eVisit. The other main type of missing data was diagnosis for the eVisit. However, this concerned a limited number of patients (2.1%; 212/10084) with similar characteristics as the total study population and should not have affected the outcome.
The measure of socioeconomic standard, CNI, was acquired for the patient’s registered PHCC. Thus, it was a crude measure on a group level. It may suffice to partially control for socioeconomics in statistical analysis but should not be further interpreted as a descriptive statistic.
Findings in relation to prior research
The patients seeking PHC Online had similar demographic characteristics as patients in other studies of virtual visits including eVisits, with a higher proportion of younger patient groups [3, 8,9,10]. This thus remains an issue of concern in terms of equal access to health care [9].
Skin diagnoses were even more common in our study population than in prior research, while respiratory tract and urinary tract diagnoses (primarily infections) were common in accordance with other studies [11, 15, 29]. These are often simple and potentially self-healing conditions, in line with qualitative research reporting that patients choose to use virtual visits for less severe conditions [30]. This may indicate a suboptimal use of health care resources [7].
Prior research on subsequent health care contacts after eVisits is limited. Most studies focus on urinary or respiratory tract infections. Studies differ regarding health care professional for the eVisit, time period, and type of subsequent contact. In these studies, subsequent face-to-face visit rates ranged from 5 to 25% [15,16,17,18,19,20,21,22,23]. In our study, subsequent face-to-face contacts were within the same range, from the most specific type of follow-up (with a physician in primary care after an eVisit to a GP for the same diagnostic group) at 6% to the follow-up frequency with nurse or physician for all patients for any reason at 26%. Our results thus show similar follow-up rates as prior research when considering a more varied array of diagnoses – and indicate the importance of the choice and detailing of outcome measure.
What our study primarily adds is the finding that the PHC Online patients had a higher frequency of subsequent health care contacts after an eVisit to a nurse than to a GP. Our analysis included all eVisits to PHC Online, regardless of whether the patient was advised by the nurse or the GP to seek physical care. Therefore, a reasonable explanation for our results could be that a larger proportion of the eVisits to a nurse resulted in the patient being recommended to seek a physical unit. Such visits should rather be considered triage. If so, more specific instructions to patients regarding which types of complaints are suitable for an eVisit may decrease avoidable triage contacts.
Prior studies indicate that face-to-face follow-up rates after virtual and face-to-face visits to primary care do not differ [11, 16, 19,20,21,22,23]. However, these were also registry-based studies, which means that the results must be interpreted with caution. Virtual care-seekers are generally healthier and thus should require less follow-up [3, 8,9,10, 30]. As an alternative analysis, we instead compared follow-up between eVisits for different diagnostic groups. We found that patients with infections (especially respiratory tract but also urinary tract) and unspecific complaints (especially skin-related) were more likely to require further health care contact after an eVisit with a GP than patients with various other diagnoses. This finding calls for cautious interpretation. It could indicate conditions that should be referred directly to physical care, due to seriousness of the condition or inappropriateness of the eVisit setting. However, it could also indicate actual needs that eVisits can help attend to where some follow-up is always expected, as opposed to supply-induced demand [7].
Finally, it should be noted that we did not study virtual visits with the patient’s own GP. Thus, results could be generalized to eVisits conducted within the same health care system for minor illnesses, but not to virtual visits as an integral part of a primary care with continuity. Relating to prior research, telephone or video visits with the patient’s own GP have been shown to decrease emergency department use compared to telephone or video visits with any GP [31].
Further research
Areas for future register-based studies include continuity of care, where the outcomes of eVisits provided by the patient’s own GP, integrated with the patient’s PHCC, and separate from it could be compared. A pertinent next step in the research on eVisits would be studies using a randomized controlled trial design for comparison with physical visits and telephone consultations. Such a design would counter selection bias and increase the ability to draw conclusions about causation. Possible outcome measures would be follow-up contacts, quality measures such as prescription of antibiotics, patient experience, and health care expenditure. In a randomized controlled trial design, it would also be possible to compare outcomes between different symptoms or diagnoses. Such studies could inform policy decisions on how to use digital care to meet needs but not to induce demand.
Conclusions
eVisits to an all-virtual public primary care unit primarily attracted younger patient groups, appeared to partially serve a triage function when handled by a nurse and often concern simple conditions also when managed by a GP. Most patients did not require follow-up, and those who did mainly remained in primary care. Our results thus indicate that this type of eVisits may be appropriate for uncomplicated medical complaints. Nonetheless, the effectiveness of eVisits in terms of substitution of physical visits, and resource utilization in relation to the more complex care needs of a primary care population, should be further studied.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- CNI:
-
Care Need Index
- eVisits:
-
Text-based virtual visits
- GP:
-
General Practitioner
- ICD:
-
International Classification of Diseases
- PHCC:
-
Primary Health Care Center
- PHC Online:
-
Primary Health Care Skåne Online
References
Neves AL, Burgers J. Digital technologies in primary care: implications for patient care and future research. Eur J Gen Pract. 2022;28(1):203–8.
Ward K, Vagholkar S, Sakur F, Khatri NN, Lau AYS. Visit types in Primary Care with Telehealth Use during the COVID-19 pandemic: systematic review. JMIR Med Inf. 2022;10(11):e40469.
Ekman B, Thulesius H, Wilkens J, Lindgren A, Cronberg O, Arvidsson E. Utilization of digital primary care in Sweden: descriptive analysis of claims data on demographics, socioeconomics, and diagnoses. Int J Med Inf. 2019;127:134–40.
Milos Nymberg V, Ellegard LM, Kjellsson G, Wolff M, Borgstrom Bolmsjo B, Wallman T, et al. Trends in Remote Health Care Consumption in Sweden: comparison before and during the First Wave of the COVID-19 pandemic. JMIR Hum Factors. 2022;9(1):e33034.
Mold F, Cooke D, Ip A, Roy P, Denton S, Armes J. COVID-19 and beyond: virtual consultations in primary care-reflecting on the evidence base for implementation and ensuring reach: commentary article. BMJ Health Care Inf. 2021;28(1):e100256.
Burki T. GP at hand: a digital revolution for health care provision? Lancet. 2019;394(10197):457–60.
Rosen R. Meeting need or fuelling demand? Improved access to primary care and supply-induced demand. 2014. https://www.nuffieldtrust.org.uk/sites/default/files/2017-01/meeting-need-or-fuelling-demand-web-final.pdf. Accessed 11 Jan 2024.
Mold F, Hendy J, Lai YL, de Lusignan S. Electronic Consultation in Primary Care between providers and patients: systematic review. JMIR Med Inf. 2019;7(4):e13042.
Parker RF, Figures EL, Paddison CA, Matheson JI, Blane DN, Ford JA. Inequalities in general practice remote consultations: a systematic review. BJGP Open. 2021;5(3):BJGPO. 2021.0040.
Dahlgren C, Dackehag M, Wandell P, Rehnberg C. Determinants for use of direct-to-consumer telemedicine consultations in primary healthcare-a registry based total population study from Stockholm, Sweden. BMC Fam Pract. 2021;22(1):133.
Nguyen OT, Alishahi Tabriz A, Huo J, Hanna K, Shea CM, Turner K. Impact of Asynchronous Electronic Communication-based visits on clinical outcomes and Health Care Delivery: systematic review. J Med Internet Res. 2021;23(5):e27531.
Campbell K, Greenfield G, Li E, O’Brien N, Hayhoe B, Beaney T, et al. The impact of virtual consultations on the quality of primary care: systematic review. J Med Internet Res. 2023;25:e48920.
The Swedish Agency for Health and Care Services Analysis. [Online Visits: Resource Use and Equity Linked to Digital Health Care Visits]. 2022. https://www.vardanalys.se/rapporter/besok-via-natet/. Accessed 11 Jan 2024.
The Network for IT Directors in the Swedish Regions (SLIT). [IT and Digitalization in Health Care 2023]. 2023. https://www.inera.se/globalassets/inera/media/dokument/projekt/it-och-digitalisering-i-halso-och-sjukvarden_2023.pdf. Accessed 11 Jan 2024.
Albert SM, Shevchik GJ, Paone S, Martich GD. Internet-based medical visit and diagnosis for common medical problems: experience of first user cohort. Telemed J E Health. 2011;17(4):304–8.
Mehrotra A, Paone S, Martich GD, Albert SM, Shevchik GJ. Characteristics of patients who seek care via eVisits instead of office visits. Telemed J E Health. 2013;19(7):515–9.
Courneya PT, Palattao KJ, Gallagher JM. HealthPartners’ online clinic for simple conditions delivers savings of $88 per episode and high patient approval. Health Aff (Millwood). 2013;32(2):385–92.
Penza KS, Murray MA, Pecina JL, Myers JF, Furst JW. Electronic visits for minor Acute illnesses: analysis of patient demographics, prescription rates, and Follow-Up care within an Asynchronous text-based online visit. Telemed J E Health. 2018;24(3):210–5.
Murray MA, Penza KS, Myers JF, Furst JW, Pecina JL. Comparison of eVisit Management of urinary symptoms and urinary tract infections with Standard Care. Telemed J E Health. 2020;26(5):639–44.
Penza KS, Murray MA, Myers JF, Furst JW, Pecina JL. Management of Acute Sinusitis via e-Visit. Telemed J E Health. 2021;27(5):532–6.
Johnson KM, Dumkow LE, Burns KW, Yee MA, Egwuatu NE. Comparison of diagnosis and prescribing practices between virtual visits and Office visits for adults diagnosed with Sinusitis within a primary Care Network. Open Forum Infect Dis. 2019;6(9):ofz393.
Johnson KL, Dumkow LE, Salvati LA, Johnson KM, Yee MA, Egwuatu NE. Comparison of diagnosis and prescribing practices between virtual visits and office visits for adults diagnosed with uncomplicated urinary tract infections within a primary care network. Infect Control Hosp Epidemiol. 2021;42(5):586–91.
Entezarjou A, Sjobeck M, Midlov P, Nymberg VM, Vigren L, Labaf A, et al. Health care utilization following digi-physical assessment compared to physical assessment for infectious symptoms in primary care. BMC Prim Care. 2022;23:4.
Bavafa H, Hitt LM, Terwiesch C. The impact of E-Visits on visit frequencies and Patient Health: evidence from primary care. Manage Sci. 2018;64(12):5461–80.
Region Skåne’s Unit for Social Analysis. [How has Skåne done? Follow-up of regional development work]. 2023. https://utveckling.skane.se/digitala-rapporter/huga/. Accessed 15 Jan 2024.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of Observational studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296.
Sundquist K, Malmstrom M, Johansson SE, Sundquist J. Care need Index, a useful tool for the distribution of primary health care resources. J Epidemiol Community Health. 2003;57(5):347–52.
Textor J, van der Zander B, Gilthorpe MS, Liskiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package ‘dagitty’. Int J Epidemiol. 2016;45(6):1887–94.
Nijhof D, Ingram A, Ochieng R, Roberts EJ, Poulton B, Ochieng B. Examining GP online consultation in a primary care setting in east midlands, UK. BMC Health Serv Res. 2021;21(1):1030.
Gabrielsson-Jarhult F, Kjellstrom S, Josefsson KA. Telemedicine consultations with physicians in Swedish primary care: a mixed methods study of users’ experiences and care patterns. Scand J Prim Health Care. 2021;39(2):204–213.
Lapointe-Shaw L, Salahub C, Bird C, Bhatia RS, Desveaux L, Glazier RH, et al. Characteristics and health care use of patients attending virtual walk-in clinics in Ontario, Canada: cross-sectional analysis. J Med Internet Res. 2023:25:e40267.
Acknowledgements
The authors wish to thank Patrick O’Reilly for the English language review.
Funding
Open access funding provided by Lund University. This study was financed by Swedish governmental funding of clinical research (ALF Younger Researchers) to SC and by Region Skåne to Center for Primary Health Care Research.
Author information
Authors and Affiliations
Contributions
All authors (HG, UJ, BBB, VMN, MW, SC) made a substantial contribution to the conception and design of the work. HG acquired and analyzed the data, with support primarily from SC and UJ. HG drafted the manuscript. All authors (HG, UJ, BBB, VMN, MW, SC) contributed substantially in revising the manuscript, and approved the submitted version. All authors agree to be personally accountable for all parts of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Swedish Ethical Review Authority (dnr 2019–06388, dnr 2023-06551-02). The patients received information about the study when they logged in at the PHC Online platform, including information about how to opt out. Informed consent to participate was waived by the Swedish Ethical Review Authority (dnr 2019–06388). Personal data were handled safely and in accordance with the European Union’s General Data Protection Regulation. A Data Management Plan was created and stored digitally at Lund University.
Consent for publication
Not applicable.
Competing interests
SC has a position as Head of Research in the management of Region Skåne’s public primary care (Primary Care Skåne) but has not been involved in the decision of procurement of the service for eVisits. All researchers are employees of Region Skåne’s public primary care but are not involved in the development or implementation of PHC Online. The researchers have no connection to the commercial vendor that supplies the digital system used by PHC Online. The authors declare that they have no other competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Additional file 1:
Causal diagram of the total effects of diagnostic group on follow-up adapted from DAGitty.net [28]
Additional file 2:
Flow chart of registered subsequent health care contacts within 14 days after the index eVisit
Additional file 3:
Types of subsequent health care contacts within 14 days after the index eVisit (N=10 084)
Additional file 4:
Adjusted odds ratio1 for subsequent contact per diagnostic group after eVisit to a nurse (n = 5696)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Glock, H., Jakobsson, U., Borgström Bolmsjö, B. et al. eVisits to primary care and subsequent health care contacts: a register-based study. BMC Prim. Care 25, 297 (2024). https://doi.org/10.1186/s12875-024-02541-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-024-02541-y