
Abstract
Background
Unhealthy alcohol use involves a spectrum from hazardous use (exceeding guidelines but no harms) through to alcohol dependence. Evidence-based management of unhealthy alcohol use in primary health care has been recommended since 1979. However, sustained and systematic implementation has proven challenging. The Continuing Quality Improvement (CQI) process is designed to enable services to detect barriers, then devise and implement changes, resulting in service improvements.
Methods
We conducted a systematic review of literature reporting on strategies to improve implementation of screening and interventions for unhealthy alcohol use in primary care (MEDLINE EMBASE, PsycINFO, CINAHL, the Australian Indigenous Health InfoNet). Additional inclusion criteria were: (1) pragmatic setting; (2) reporting original data; (3) quantitative outcomes related to provision of service or change in practice. We investigate the extent to which the three essential elements of CQI are being used (data-guided activities, considering local conditions; iterative development). We compare characteristics of programs that include these three elements with those that do not. We describe the types, organizational levels (e.g. health service, practice, clinician), duration of strategies, and their outcomes.
Results
Fifty-six papers representing 45 projects were included. Of these, 24 papers were randomized controlled trials, 12 controlled studies and 20 before/after and other designs. Most reported on strategies for improving implementation of screening and brief intervention. Only six addressed relapse prevention pharmacotherapies. Only five reported on patient outcomes and none showed significant improvement. The three essential CQI elements were clearly identifiable in 12 reports. More studies with three essential CQI elements had implementation and follow-up durations above the median; utilised multifaceted designs; targeted both practice and health system levels; improved screening and brief intervention than studies without the CQI elements.
Conclusion
Utilizing CQI methods in implementation research would appear to be well-suited to drive improvements in service delivery for unhealthy alcohol use. However, the body of literature describing such studies is still small. More well-designed research, including hybrid studies of both implementation and patient outcomes, will be needed to draw clearer conclusions on the optimal approach for implementing screening and treatment for unhealthy alcohol use. (PROSPERO registration ID: CRD42018110475).
Similar content being viewed by others

Background
Unhealthy alcohol use involves a broad spectrum of conditions from hazardous or risky drinking to the diagnosis of alcohol use disorder. ICD-11 defines hazardous drinking as use that increases the risk of harmful physical or mental health consequences to the user or to others, while disorders due to alcohol involve use patterns that have already caused harm or dependence [1]. Evidence-based management of unhealthy alcohol use in primary health care (PHC), particularly the use of screening and brief intervention (SBI), has been advocated since the World Health Organization (WHO) called for the development of strategies and guidelines for SBI applicable in PHC settings [2,3,4,5]. SBI is now widely accepted as best practice and recommended by both national and international guidelines [6].
Meta-analyses of studies of implementation of alcohol screening and treatment have shown that multi-faceted programs with longer duration and alcohol-focused programs are better at achieving improvements. Specifically, programs oriented towards multiple-organizational levels, as well as studies longer than 12 months were associated with significant effects on improvement of implementation of screening and/or brief intervention compared to single strategy programs [7, 8]. Programs combining strategies that targeted the clinician, organization and patient were more effective in decreasing alcohol consumption than clinician-only strategies [8]. However, sustained and systematic implementation of evidence-based care for alcohol use in PHC continues to be a problem [6, 9,10,11,12]. Furthermore, there is little evidence of significant effects of implementation strategies on patients’ alcohol consumption [8]. Barriers, such as time pressures, staff retention, lack of training and leadership, as well as the clinicians’ perception of alcohol discussions as sensitive, have been identified [6, 11, 13]. To improve detection and treatment of unhealthy alcohol use, more work is needed to develop and test approaches that are sensitive to facilitators and barriers in an individual PHC setting.
Continuous quality improvement (CQI) in health care has been defined as “a structured organizational process for involving people in planning and executing a continuous flow of improvement to provide quality health care that meets or exceeds expectations” [14]. Originating from industrial process improvement approaches, this approach has been used in health care since the 1990s [14, 15]. CQI is designed to improve health care by using data to identify where services are doing well and not so well, implementing and monitoring corrective action and then reviewing its effectiveness, in continuous improvement cycles. Studies, including the largest CQI program in Australia [16], have shown that with consistent policy and infrastructure it can facilitate ongoing improvement of PHC service delivery and subsequently, better health outcomes [16,17,18,19]. This largest program includes research in Aboriginal community controlled primary health care services [16]. However, to our knowledge, there is no literature review specifically on the use of CQI strategies in improving service provision for unhealthy alcohol use in the PHC setting.
This systematic review aims to: 1) describe types, levels and duration of implementation strategies to improve screening and treatment for unhealthy alcohol use in PHC, and their outcomes, as available in peer-reviewed literature; 2) investigate to what extent elements of CQI are being used in these strategies; 3) compare characteristics of programs with all CQI elements with programs that do not have these elements.
Methods
We performed a systematic review of peer-reviewed literature from January 1990 to September 2018 (referred to from here on as ‘reports’). The year 1990 was chosen because it marked the beginning of the decade following the WHO’s first release of guidelines for alcohol screening and brief intervention, as well as the beginnings of CQI in health care [3, 14, 15].
Search strategy
To construct the search strategy, we first conducted a broad text-word search in MEDLINE.
From this search (14,764 results) we identified a set of representative reports that met the inclusion criteria (a sentinel set; n = 25) by systematically screening 20% of the search results for abstracts that met the inclusion criteria. Medical Subject Headings (MeSH) and keywords of the 25 sentinel articles were then used to progressively refine the search strategy: subject headings and subheadings not already in the original search strategy were identified and used to modify the search strategy. Retention of the sentinel set was checked with each modification. The strategy was then further refined through an independent review by an expert in drug and alcohol health services research. The resulting final strategy consisted of three groups of search terms reflecting the problem (e.g. alcohol, binge drinking), setting (e.g. primary care, general practice), and intervention (e.g. program. strategy) of interest to this review. A summary of the strategy is presented in Table 1. This strategy was applied to MEDLINE, EMBASE and PsycINFO with modifications made as required. An adapted set of search terms was used in CINAHL and the Australian Indigenous Health InfoNet. Search results were restricted to English language. Hand searches were performed on reference lists of 21 major reviews, sourced from Cochrane (including Cochrane EPOC and Cochrane Drugs and Alcohol Review Group) and the above literature search. The final set included for analysis was checked for any additional reports. A detailed protocol and search strategy are available in the international prospective register of systematic reviews, PROSPERO (ID CRD42018110475), https://www.crd.york.ac.uk/prospero/.
Reports were included if they described experimental or observational studies that: (1) were conducted in a pragmatic PHC setting, that is the strategies were integrated into routine practice and delivered primarily by existing PHC staff [20]; (2) described an intervention/initiative/program designed to improve service provision or improve evidence-based practice to address unhealthy alcohol use; (3) reported original data; and (4) reported quantitative outcomes related to provision of service or change in practice for unhealthy alcohol use. Reports that utilized clinician self-reported outcome measures were included only if they quantified the change in service provision. Exclusion criteria comprised non-original data reports, reviews, commentaries and editorials, method reports, a citation without abstract available, and conference abstracts.
Data extraction
Literature searches were downloaded into Endnote X8.2 and duplicates removed. Irrelevant reports and ineligible publication types were removed at the stage of the title screen. Titles and abstracts of the resulting set were independently reviewed for inclusion criteria by two reviewers (MD, CW). Where agreement could not be reached a third reviewer (KC or KL) was consulted. Full text review was performed by MD and CW with further discrepancies discussed with KC. Data from the final set was extracted by MD in consultation with KC and KL.
We extracted the following data:
-
information on study design and setting
-
description of the improvement strategy including targeted clinical actions
-
whether strategy was multifaceted (that is they employed more than one component [e.g. training plus financial incentive] to target implementation barriers and achieve improvement)
-
organizational levels targeted by the strategy, defined as:
-
National – targeting the health care system for an entire population
-
Health system – targeting organizational structures within a health system (e.g. local, state-based, or private health insurance company)
-
Practice – targeting individual primary care practices
-
Clinician – targeting clinicians working within PHC practice settings
-
Patient – targeting the patient or population being served by the practices
-
-
details of follow-up
-
type of outcome measure and outcomes.
Identifying CQI elements
Because in academic literature, CQI methodology is not always clearly identified [15, 21, 22], we screened for the presence of three essential CQI elements defined by Rubenstein et al. [22]:
-
(i)
Using ‘systematic data guided activities’ to identify problems and achieve improvement
-
(ii)
‘designing with local conditions in mind’
-
(iii)
using an ‘iterative development and testing process’
We defined element (i) as present if there was clear indication that the improvement strategy included systematic use of data to conduct assessment of the problem to be addressed and/or to diagnose improvement and a response to this data that modified the improvement strategy. We defined element (ii) as present if there was clear indication of designing and/or allowing adaptation of strategies to fit the special characteristics of the local setting. Element (iii) required evidence that the data collection and response in element 1 was conducted in at least two cycles. The elements were coded as ‘present’, ‘absent’ or ‘unclear’. For the purposes of descriptive analyses below any instances of ‘unclear’ were treated as absent.
Descriptive analysis was performed on all reports that met the selection criteria as well as on the subset of reports describing initiatives that included all three CQI elements.
Results
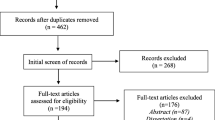
Fifty-six reports representing 45 studies were included in the review (Fig. 1). Of these, 24 reports were randomized controlled trials (RCTs) [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46], 12 were controlled designs [47,48,49,50,51,52,53,54,55,56,57,58] and 20 were before/after and other designs [59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78]. Thirty-five were alcohol-specific, while 21 focused on broader prevention (Table 2).

Search strategy flow chart. aOne additional paper was identified from final set of reports included in analysis
All studies were conducted in member countries of the Organization for Economic Co-operation and Development (OECD) and all countries but one were part of the Group of Twenty (G-20). Twenty-four reports represented projects conducted exclusively in the United States of America (USA), 12 in Australia, seven in the United Kingdom, seven in individual European countries and one in Canada. Three reports were from the Optimizing Delivery of Health Care Interventions (ODHIN) trial, which reported on aggregated outcomes in five European countries, and two reports from the international WHO Collaborative Project. The clinical setting was predominantly a generalist, general practitioner-led PHC service; however, four reports [28, 35, 52, 57] representing three projects were conducted in nurse-led community health centres. Likewise, populations served by these were general, except two in adolescent PHC and four in PHCs predominantly serving Indigenous peoples [54, 63, 65, 78].
Targeted clinical actions
The majority of reports (52/56) examined improvement in rates of screening or brief intervention (BI) and/or referral to treatment. Twenty-four reports recommended or reported on the use of a validated screening measure, with 14 using either AUDIT (Alcohol Use Disorders Identification Test), its shorter version, AUDIT-C or both. Other validated screening tools included Single Alcohol Screening Question (SASQ), Fast Alcohol Screening Test (FAST), CAGE (an acronym for its four questions) and Short Michigan Alcohol Screening Test (sMAST). There was a wide range of terms used to describe screening and BI. For example, asking about alcohol consumption, eliciting alcohol history, ‘assessment’ of alcohol consumption or similar was used for screening; ‘brief advice’, ‘brief counselling’, and discussing alcohol was used for BI. Only six reports addressed improvement in rates of pharmacotherapy uptake for relapse prevention [31, 42, 43, 49, 61, 75]. None included implementation of psychosocial therapies, though referral to such therapies was mentioned as a treatment option.
Characteristics of improvement strategies
Types and levels of implementation
A variety of strategies were employed to improve screening and treatment for unhealthy alcohol use. These targeted one or more different organizational levels. Of the 56 reports, none targeted all five levels, and only two were targeted at four levels. The majority of reports (50/56) included clinicians as targets, followed by the practice (35/56), with 32 reports targeting both. Of those, only nine reports also targeted the health-system level, and two reports targeted four levels, including the patient. Table 3 summarizes strategies by implementation level. Most implementation strategies (42/56) were multifaceted. Of these, 33 targeted two or more organizational levels.
Duration of implementation and follow-up
For studies where it was possible to extract these data, the median duration of the implementation phase was 28.2 weeks (IQR = 40, n = 50), and median duration from commencement of implementation to last data collection was 52 weeks (IQR = 52, n = 53). Of the 49 reports, where both types of duration data were available, 20 had their last data collection event after the end of implementation phase, indicating a follow-up period.
Reports with CQI elements
Of the included reports, 22 described strategy components that were consistent with at least one of the three essential CQI elements (Table 4) [23]. An attempt to design or allow adaptation of implementation strategies to fit local conditions was the most commonly identified element (n = 20), followed by the use of iterative development and testing processes (n = 14). Using ‘systematic data guided activities’ to identify problems and achieve improvement, such as responding with corrective actions to regular practice audit reports and monitoring implemented changes,was identified in 13 reports.
All three essential CQI elements were clearly identifiable in 12 reports. Of these, three were RCTs and seven were focused on broader prevention of risky behaviours (rather than being solely focused on unhealthy alcohol use). All examined screening and/or BI. Two also examined relapse prevention medicines. In contrast to other reports, more studies with all CQI elements targeted health system practice and clinician levels for implementation strategies and all were multifaceted (Table 5). Studies with all CQI elements also had higher median implementation duration.
Outcomes in relation to type of implementation strategy
The majority of reports (n = 51, 91.1%) showed a statistically significant increase in utilization of at least one clinical action. Significant increases in implementation were shown most often for screening and least often for referrals (Table 6). Only five reports (8.9%) included patient outcomes [29, 35, 40, 44, 45]. Of those, one [44] reported on changes in blood pressure and the rest on patient-reported changes in alcohol consumption. No significant between-group differences in these outcomes were shown, although there were some significant within-group outcomes in two reports [44, 45].
The proportion of reports with any positive outcome was similar in the 12 reports that included all three essential CQI elements, compared with the 44 reports that did not (91.7% compared to 90.1%). However, a higher proportion of the reports with three CQI elements achieved a significant improvement for two of the examined clinical actions: 81.8% for screening, 66.7% for brief intervention (compared with 75.6 and 57.6% respectively). Of the two reports with all CQI elements that aimed to examine pharmacotherapies, one reported a significant improvement and the other did not report results specific to this action. Of the five reports that presented patient outcomes, one [44] had all three CQI elements and reported a significant within-group improvement of systolic blood pressure but not between-groups.
Discussion
This is the first systematic review to investigate incorporation of CQI elements into strategies to improve implementation of screening and treatment for unhealthy alcohol use in primary care. There was much variation in the studies’ design and delivery and studies concentrated mainly on screening and brief intervention for non-dependent alcohol use. There was little work on implementing onsite management of alcohol dependence, for example, pharmacotherapy for relapse prevention. Only 12 studies included all three CQI elements considered core to the CQI approach, while 22 studies incorporated at least one CQI element.
General practitioners are most often the first point of contact with healthcare for any drinkers. Therefore, it is important that PHCs are equipped to deal with the full spectrum of unhealthy alcohol use. Currently, screening and brief intervention are widely advocated as an effective secondary prevention approach for hazardous or harmful alcohol use in PHC settings [6]. If more severe alcohol problems are detected during the course of screening and brief intervention, referral to treatment away from the PHC service is often used. However, there is little evidence that this approach actually leads to effective linking with specialised services for patients who need them [79]. Furthermore, in many settings referral to specialist healthcare may not be an option due to costs, geographic isolation, long waiting periods or associated stigma. Thus, prescription of relapse prevention medicines in PHC rather than by referral to specialist centres may result in increased patient engagement at the point of detection or when the patient may be motivated and open to change.
Yet in the large volume of literature reviewed, only six studies included pharmacotherapies for relapse prevention as a target of implementation strategies. Only four of these also included BI for non-dependent (hazardous or harmful) drinkers, thus addressing the full range of unhealthy alcohol consumption.
Types, levels and duration of strategies used to improve implementation
Strategies that are alcohol-specific, multifaceted and target multiple organizational levels have previously been shown to be associated with improved implementation outcomes [7, 8]. While the reviewed reports all tended to display some combination of these characteristics, reports with all three CQI elements more commonly utilized multifaceted designs and targeted the practice and health system levels (33.3%) than reports without these elements (11.4%). Overall, fewer studies incorporated the patient-level action as a target of implementation (none of the reports with three CQI elements and four of the other reports). This warrants more attention as there is evidence that strategies that include patient-oriented components of action (e.g. mailouts) in combination with other levels may be better at decreasing alcohol consumption than clinician-oriented strategies alone [8].
We found that details of study duration were often lacking in the included reports either due to omission or the nature of the study design. It was often difficult to distinguish the duration of individual phases of the study: baseline, implementation and follow-up, making systematic data extraction challenging. We therefore used the duration from start of strategy implementation to end of data collection as a proxy for study duration. When the end of data collection was later than duration of implementation, this was considered as an indication of follow-up. The median study duration for studies with all three CQI elements was much higher than for studies without these (104 and 38.2 weeks respectively). In addition, only 20 reports had a clear indication of follow-up after the conclusion of active implementation. While there is evidence that study duration of 12 months or more is a significant predictor of improvement in BI implementation [8], it is not clear whether this is due to longer duration of implementation or longer follow-up. The lack of consistent duration data on implementation and follow-up is an important gap in the evidence-base as these are likely to influence the uptake of the implementation strategy, its sustainability and effects on both service-level and patient outcomes. For example, longer duration of implementation may be necessary to implement more complex treatment regimens and to allow for late adopters. Insufficient duration and frequency of follow-up may also lead to loss of information about potential improvements in patient outcomes as well as optimal length of strategy implementation to ensure sustainability.
While studies with all three CQI elements appear to have more favourable design characteristics than studies without these, it is less clear if this leads to better outcomes in improving delivery of screening and treatment for unhealthy alcohol use. A higher proportion of reports with three CQI elements improved screening outcomes and, to a lesser extent BI outcomes. However, they did not improve uptake of pharmacotherapies. These results need to be interpreted with caution, given the small number of reports with all three CQI elements, and even smaller number (n = 2) of these that investigated use of pharmacotherapies.
It is notable that three of the four reports on studies in indigenous settings included all essential CQI elements. These represented two CQI studies (in Australia and US), both set in community controlled health services. This perhaps reflects CQI’s suitability to facilitate efficient service improvements in settings where lack of adequate resources and multiple health priorities can be a challenge and where stakeholder-driven, culturally relevant programs are crucial [80]. Finally, very few implementation studies (n = 5) reported patient outcomes and those that did were unable to demonstrate significant reductions in patient alcohol consumption [8]. Just one report considered patient outcomes other than alcohol consumption. The demonstrated lack of evidence of significant effect on patient outcomes may be due to not enough consideration being given to the complexity of studies that test implementation strategies as well as effectiveness of clinical interventions [81, 82].
Recommendations for practice and research
Improving screening and treatment uptake in PHC
Given the dearth in evidence, there is a need for more implementation studies on treatment for the full spectrum of unhealthy alcohol use, particularly the use of pharmacotherapies to treat dependent drinkers. This is particularly important in low-income countries where alcohol-attributable mortality is highest [83], where specialist services may be limited, but where few such studies are conducted.
The effectiveness of implementation strategies may depend on how well they fit the services’ own circumstances, address the barriers to implementation and how they can co-exist with existing local enablers in a specific service. Furthermore, studies rarely analyse the contribution of individual components of the studied strategies to the overall effect on service-level outcomes. This detail could help services tailor their approaches to improving screening and treatment for unhealthy alcohol use. The fact that uptake of screening and treatment for unhealthy alcohol use in PHC remains low [84] suggests that future research effort should concentrate on “service-friendly” strategies as they may increase uptake and sustainability of effect.
The CQI approach provides a framework for how to carry out an improvement process systematically and on an ongoing basis. What activity is carried out to achieve the improvement and how it is measured is left up to the services to decide. Services can work towards a national benchmark or choose their own implementation goal. If implemented well, the CQI approach can offer the advantage of being sensitive and responsive to local conditions, and to newly arising challenges. The Plan-Do-Study-Act of the CQI cycle can facilitate the identification of the optimal combination of strategy components for a particular clinical setting. It is compatible with reflective learning and change to enable interventions to adapt to complex environments [85]. However, there may be barriers to implementation of CQI itself, including staff time and resources [86].
CQI in implementation research
The ultimate goal of implementing and improving service delivery is to improve patients’ health, but evidence for this in relation to screening and treatment of unhealthy alcohol use is lacking. One approach to closing this evidence gap could be to simultaneously test implementation strategies and the effectiveness of clinical interventions through hybrid designs. This approach is thought to enable a more rapid generation of evidence base for the clinical interventions in “real life” settings than the traditional stepped processes: efficacy-effectiveness-implementation [81, 82].
Implementation research utilizing hybrid designs and quality improvement research can complement each other, with the former contributing more rigorous, scientifically robust summative evaluation and the latter providing information to enable a systematic refinement of the studied implementation strategy [87]. Inclusion of CQI in implementation research, particularly in hybrid designs thus has the potential to provide the optimal study design: flexible and responsive implementation strategies, scientific rigor to detect improvements in both service and patient-level outcomes, and ability to simultaneously provide information of value to healthcare managers and policy makers.
Limitations
Due to the volume of work and logistic constraints the search was limited to English language and only peer-reviewed literature was included in this study. Some health organization-based programs are published only in annual and commissioned reports and so would not have been included. However, a review of grey literature was out of scope of this review.
It has been previously noted that CQI studies are not easily identifiable in the academic literature as these are often not reported clearly or consistently [15, 22, 88]. Furthermore, the word and formatting limits of peer reviewed journals may contribute to underreporting and imprecise reporting of CQI methods [15]. Data extraction in this review was done by single person (MD) because of resource constraints. This may have introduced bias to the coding of key characteristics of strategies, particularly the three CQI elements. However, a priori definitions and clear criteria were used to reduce subjectivity.
Future meta-analysis of these studies may offer deeper insights into the benefits of incorporating elements of CQI into implementation research in alcohol service delivery. However, the heterogeneity of the studies, gaps in reporting and generally low numbers of reports that meet the inclusion criteria will pose challenges.
Conclusions
The uptake of screening and treatment of unhealthy alcohol use in PHC continues to be low despite national and international guideline recommendations. Many studies of implementation strategies have yet to show significant improvement in patient outcomes. There remains a lack of implementation studies for treatment for the full spectrum of unhealthy alcohol use. There is also a lack of information in the effectiveness of particular components of multifaceted strategies, or inclusion of patient-level implementation strategies and outcomes. Incorporating CQI elements into implementation strategies may offer promise as an approach to deliver flexible and responsive solutions for sustained implementation of alcohol care. However, further well-designed research, including hybrid studies of both implementation and patient outcomes are needed to draw clearer conclusions on the most effective way to implement screening and treatment for unhealthy alcohol use in PHC.
Availability of data and materials
The search strategy used to generate the initial systematic review search result is available in PROSPERO (protocol ID CRD42018110475). https://www.crd.york.ac.uk/prospero/. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AUDIT:
-
Alcohol Use Disorders Identification Test
- BI:
-
Brief intervention
- CAGE:
-
Alcohol screening tool; abbreviation in an acronym for its four questions
- CQI:
-
Continuous Quality Improvement
- EPOC:
-
Effective Practice and Organisation of Care
- FAST:
-
Fast Alcohol Screening Test
- G-20:
-
Group of Twenty
- ICD11:
-
International Classification of Diseases, 11th Revision
- MeSH:
-
Medical Subject Headings
- ODHIN:
-
Optimizing Delivery of Health Care Interventions
- OECD:
-
Organization for Economic Co-operation and Development
- PHC:
-
Primary health care
- RCT:
-
Randomized controlled trial
- SASQ:
-
Single Alcohol Screening Question
- SBI:
-
Screening and brief intervention
- sMAST:
-
Short Michigan Alcohol Screening Test
- WHO:
-
World Health Organization
References
World Health Organization. ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS): World Health Organization; 2019. Available from: https://icd.who.int/.
WHO Expert Committee on Problems Related to Alcohol Consumption. Meeting Meeting 1979: Geneva S. Problems related to alcohol consumption: report of a WHO expert committee [meeting held in Geneva from 20 to 26 November 1979]. Geneva: World Health Organization; 1980.
World Health Organization. AUDIT - the Alcohol Use Disorders Identification Test: guidelines for use in primary health care/Thomas F. Babor...[et al.]. 1st ed. Geneva: World Health Organization; 1989. p. 24.
World Health Organization. AUDIT : the Alcohol Use Disorders Identification Test : guidelines for use in primary health care / Thomas F. Babor ... [et al.]. 2nd ed. Geneva: World Health Organization; 2001. p. 38.
World Health Organization. Brief intervention for hazardous and harmful drinking : a manual for use in primary care / Thomas F. Babor, John C. Higgins-Biddle. Geneva: World Health Organization; 2001.
Zhang DX, Li ST, Lee QK, Chan KH, Kim JH, Yip BH, et al. Systematic review of guidelines on managing patients with harmful use of alcohol in primary healthcare settings. Alcohol Alcohol. 2017;52(5):595–609.
Anderson P, Laurant M, Kaner E, Wensing M, Grol R. Engaging general practitioners in the management of hazardous and harmful alcohol consumption: results of a meta-analysis. J Stud Alcohol. 2004;65(2):191–9.
Keurhorst M, van de Glind I, Bitarello do Amaral-Sabadini M, Anderson P, Kaner E, Newbury-Birch D, et al. Implementation strategies to enhance management of heavy alcohol consumption in primary health care: a meta-analysis. Addiction. 2015;110(12):1877–900.
Anderson P, Wojnar M, Jakubczyk A, Gual A, Reynolds J, Segura L, et al. Managing alcohol problems in general practice in Europe: results from the European ODHIN survey of general practitioners. Alcohol Alcohol. 2014;49(5):531–9 erratum appears in alcohol alcohol 2016 Sep;51(5):630; PMID: 27522030.
Johnson M, Jackson R, Guillaume L, Meier P, Goyder E. Barriers and facilitators to implementing screening and brief intervention for alcohol misuse: a systematic review of qualitative evidence. J Public Health. 2011;33(3):412–21.
McNeely J, Kumar P, Rieckmann T, Sedlander E, Farkas S, Kannry J, et al. Barriers and facilitators affecting the implementation of substance use screening in primary care clinics: A qualitative study of patients, providers, and staff. J Gen Intern Med. 2017;32(2 Supplement 1):S128.
Williams EC, Matson TE, Harris AHS. Strategies to increase implementation of pharmacotherapy for alcohol use disorders: a structured review of care delivery and implementation interventions. Addict Sci Clin Pract. 2019;14(1):6.
Bailie J, Laycock A, Matthews V, Bailie R. System-Level Action Required for Wide-Scale Improvement in Quality of Primary Health Care: Synthesis of Feedback from an Interactive Process to Promote Dissemination and Use of Aggregated Quality of Care Data. Front Public Health. 2016;4:86.
Sollecito WA, Johnson JK. Mclaughlin and Kaluzny's continuous quality improvement in health care. 4th ed. Sudbury: Jones & Bartlett Learning; 2013.
Taylor MJ, McNicholas C, Nicolay C, Darzi A, Bell D, Reed JE. Systematic review of the application of the plan–do–study–act method to improve quality in healthcare. BMJ Qual Saf. 2013;23:290–8.
Bailie R, Matthews V, Larkins S, Thompson S, Burgess P, Weeramanthri T, et al. Impact of policy support on uptake of evidence-based continuous quality improvement activities and the quality of care for indigenous Australians: a comparative case study. BMJ Open. 2017;7(10):e016626.
Matthews V, Schierhout G, McBroom J, Connors C, Kennedy C, Kwedza R, et al. Duration of participation in continuous quality improvement: a key factor explaining improved delivery of type 2 diabetes services. BMC Health Serv Res. 2014;14:578.
Bodicoat DH, Mundet X, Gray LJ, Cos X, Davies MJ, Khunti K, et al. Identifying effective pathways in a successful continuous quality improvement programme: the GEDAPS study. J Eval Clin Pract. 2014;20(6):1137–43.
Woods C, Carlisle K, Larkins S, Thompson SC, Tsey K, Matthews V, et al. Exploring systems that support good clinical Care in Indigenous Primary Health-care Services: a retrospective analysis of longitudinal systems assessment tool data from high-improving services. Front Public Health. 2017;5:45.
Nilsen P, Aalto M, Bendtsen P, Seppa K. Effectiveness of strategies to implement brief alcohol intervention in primary healthcare. A systematic review. Scand J Prim Health Care. 2006;24(1):5–15.
O'Neill SM, Hempel S, Lim YW, Danz MS, Foy R, Suttorp MJ, et al. Identifying continuous quality improvement publications: what makes an improvement intervention 'CQI'? BMJ Qual Saf. 2011;20(12):1011–9.
Rubenstein L, Khodyakov D, Hempel S, Danz M, Salem-Schatz S, Foy R, et al. How can we recognize continuous quality improvement? Int J Qual Health Care. 2014;26(1):6–15.
Anderson P, Bendtsen P, Spak F, Reynolds J, Drummond C, Segura L, et al. Improving the delivery of brief interventions for heavy drinking in primary health care: outcome results of the optimizing delivery of health care intervention (ODHIN) five-country cluster randomized factorial trial. Addiction. 2016;111(11):1935–45.
Anderson P, Coulton S, Kaner E, Bendtsen P, Kloda K, Reynolds J, et al. Delivery of brief interventions for heavy drinking in primary care: outcomes of the ODHIN 5-country cluster randomized trial. Ann Fam Med. 2017;15(4):335–40.
Anderson P, Kaner E, Wutzke S, Funk M, Heather N, Wensing M, et al. Attitudes and managing alcohol problems in general practice: an interaction analysis based on findings from a WHO collaborative study. Alcohol Alcohol. 2004;39(4):351–6.
Bendtsen P, Mssener U, Karlsson A, Pelayo HL, Vieira JP, Colom J, et al. Implementing referral to an electronic alcohol brief advice website in primary healthcare: Results from the ODHIN implementation trial. BMJ Open. 2016;6(6). https://doi.org/10.1136/bmjopen-2015-01027.
Bonevski B, Sanson-Fisher RW, Campbell E, Carruthers A, Reid AL, Ireland M. Randomized controlled trial of a computer strategy to increase general practitioner preventive care. Prev Med. 1999;29(6 Pt 1):478–86.
Chan BC, Jayasinghe UW, Christl B, Laws RA, Orr N, Williams A, et al. The impact of a team-based intervention on the lifestyle risk factor management practices of community nurses: outcomes of the community nursing SNAP trial. BMC Health Serv Res. 2013;13:54.
Chossis I, Lane C, Gache P, Michaud PA, Pecoud A, Rollnick S, et al. Effect of training on primary care residents' performance in brief alcohol intervention: a randomized controlled trial. J Gen Intern Med. 2007;22(8):1144–9.
Dubey V, Mathew R, Iglar K, Moineddin R, Glazier R. Improving preventive service delivery at adult complete health check-ups: the preventive health evidence-based recommendation form (PERFORM) cluster randomized controlled trial. BMC Fam Pract. 2006;7:44.
Friedmann PD, Rose J, Hayaki J, Ramsey S, Charuvastra A, Dube C, et al. Training primary care clinicians in maintenance care for moderated alcohol use. J Gen Intern Med. 2006;21(12):1269–75.
Funk M, Wutzke S, Kaner E, Anderson P, Pas L, McCormick R, et al. A multicountry controlled trial of strategies to promote dissemination and implementation of brief alcohol intervention in primary health care: findings of a World Health Organization collaborative study. J Stud Alcohol. 2005;66(3):379–88.
Gomel MK, Wutzke SE, Hardcastle DM, Lapsley H, Reznik RB. Cost-effectiveness of strategies to market and train primary health care physicians in brief intervention techniques for hazardous alcohol use. Soc Sci Med. 1998;47(2):203–11.
Hansen LJ, De Fine ON, Beich A, Barfod S. Encouraging GPs to undertake screening and a brief intervention in order to reduce problem drinking: a randomized controlled trial. Fam Pract. 1999;16(6):551–7.
Harris MF, Chan BC, Laws RA, Williams AM, Davies GP, Jayasinghe UW, et al. The impact of a brief lifestyle intervention delivered by generalist community nurses (CN SNAP trial). BMC Public Health. 2013;13:375.
Harris MF, Parker SM, Litt J, Van Driel M, Russell G, Mazza D, et al. Implementing guidelines to routinely prevent chronic vascular disease in primary care: The Preventive Evidence into Practice cluster randomised controlled trial. BMJ Open. 2015;5(12):e009397 (no pagination).
Haskard KB, Williams SL, DiMatteo MR, Rosenthal R, White MK, Goldstein MG. Physician and patient communication training in primary care: effects on participation and satisfaction. [erratum appears in health Psychol. 2009 mar;28(2):263]. Health Psychol. 2008;27(5):513–22.
Kaner E, Lock C, Heather N, McNamee P, Bond S. Promoting brief alcohol intervention by nurses in primary care: a cluster randomised controlled trial. Patient Education & Counseling. 2003;51(3):277–84.
Kaner EF, Lock CA, McAvoy BR, Heather N, Gilvarry E. A RCT of three training and support strategies to encourage implementation of screening and brief alcohol intervention by general practitioners. Br J Gen Pract. 1999;49(446):699–703.
Krist AH, Glasgow RE, Heurtin-Roberts S, Sabo RT, Roby DH, Gorin SN, et al. The impact of behavioral and mental health risk assessments on goal setting in primary care. Transl Behav Med. 2016;6(2):212–9.
Mertens JR, Chi FW, Weisner CM, Satre DD, Ross TB, Allen S, et al. Physician versus non-physician delivery of alcohol screening, brief intervention and referral to treatment in adult primary care: the ADVISe cluster randomized controlled implementation trial. Addict Sci ClinPract. 2015;10:26.
Navarro HJ, Shakeshaft A, Doran CM, Petrie DJ. The cost-effectiveness of tailored, postal feedback on general practitioners' prescribing of pharmacotherapies for alcohol dependence. Drug Alcohol Depend. 2012;124(3):207–15.
Ornstein SM, Miller PM, Wessell AM, Jenkins RG, Nemeth LS, Nietert PJ. Integration and sustainability of alcohol screening, brief intervention, and pharmacotherapy in primary care settings. J Stud Alcohol Drugs. 2013;74(4):598–604.
Rose HL, Miller PM, Nemeth LS, Jenkins RG, Nietert PJ, Wessell AM, et al. Alcohol screening and brief counseling in a primary care hypertensive population: a quality improvement intervention. Addiction. 2008;103(8):1271–80.
Saitz R, Horton NJ, Sullivan LM, Moskowitz MA, Samet JH. Addressing alcohol problems in primary care: a cluster randomized, controlled trial of a systems intervention. The screening and intervention in primary care (SIP) study. Ann Intern Med. 2003;138(5):372–82.
van Beurden I, Anderson P, Akkermans RP, Grol RP, Wensing M, Laurant MG. Involvement of general practitioners in managing alcohol problems: a randomized controlled trial of a tailored improvement programme. Addiction. 2012;107(9):1601–11.
Bradley KA, Epler AJ, Bush KR, Sporleder JL, Dunn CW, Cochran NE, et al. Alcohol-related discussions during general medicine appointments of male VA patients who screen positive for at-risk drinking. J Gen Intern Med. 2002;17(5):315–26.
Hamilton FL, Laverty AA, Gluvajic D, Huckvale K, Car J, Majeed A, et al. Effect of financial incentives on delivery of alcohol screening and brief intervention (ASBI) in primary care: longitudinal study. J Public Health. 2014;36(3):450–9.
Harris AHS, Brown R, Dawes M, Dieperink E, Myrick DH, Gerould H, et al. Effects of a multifaceted implementation intervention to increase utilization of pharmacological treatments for alcohol use disorders in the US veterans health administration. J Subst Abus Treat. 2017;82:107–12.
Khadjesari Z, Hardoon SL, Petersen I, Hamilton FL, Nazareth I. Impact of financial incentives on alcohol consumption recording in primary health care among adults with schizophrenia and other psychoses: a cross-sectional and retrospective. Alcohol Alcohol. 2017;52(2):197–205.
Mason P. Alcohol counsellors in general practice. J Subst Misuse. 1997;2(2):85–93.
McElwaine KM, Freund M, Campbell EM, Knight J, Bowman JA, Wolfenden L, et al. Increasing preventive care by primary care nursing and allied health clinicians: a non-randomized controlled trial. Am J Prev Med. 2014;47(4):424–34.
O'Donnell A, Haighton C, Chappel D, Shevills C, Kaner E. Impact of financial incentives on alcohol intervention delivery in primary care: a mixed-methods study. BMC Fam Pract. 2016;17(1):165.
Onders R, Spillane J, Reilley B, Leston J. Use of electronic clinical reminders to increase preventive screenings in a primary care setting: blueprint from a successful process in Kodiak, Alaska. J Prim Care Community Health. 2014;5(1):50–4.
Ozer EM, Adams SH, Lustig JL, Gee S, Garber AK, Gardner LR, et al. Increasing the screening and counseling of adolescents for risky health behaviors: a primary care intervention. Pediatrics. 2005;115(4):960–8.
Thomas K, Krevers B, Bendtsen P. Long-term impact of a real-world coordinated lifestyle promotion initiative in primary care: a quasi-experimental cross-sectional study. BMC Fam Pract. 2014;15:201.
Wiggers J, McElwaine K, Freund M, Campbell L, Bowman J, Wye P, et al. Increasing the provision of preventive care by community healthcare services: a stepped wedge implementation trial. Implement Sci. 2017;12(1):105.
Wilson A, McDonald P, Hayes L, Cooney J. Health promotion in the general practice consultation: a minute makes a difference. BMJ. 1992;304(6821):227–30.
Aalto M, Pekuri P, Seppa K. Primary health care professionals' activity in intervening in patients' alcohol drinking during a 3-year brief intervention implementation project. Drug Alcohol Depend. 2003;69(1):9–14.
Aspy CB, Mold JW, Thompson DM, Blondell RD, Landers PS, Reilly KE, et al. Integrating screening and interventions for unhealthy behaviors into primary care practices. Am J Prev Med. 2008;35(5 Suppl):S373–80.
Bobb JF, Lee AK, Lapham GT, Oliver M, Ludman E, Achtmeyer C, et al. Evaluation of a Pilot Implementation to Integrate Alcohol-Related Care within Primary Care. Int J Environ Res Public Health. 2017;14(9):08.
Chavez LJ, Williams EC, Lapham GT, Rubinsky AD, Kivlahan DR, Bradley KA. Changes in patient-reported alcohol-related advice following veterans health administration implementation of brief alcohol interventions. J Stud Alcohol Drugs. 2016;77(3):500–8.
Clifford A, Shakeshaft A, Deans C. Training and tailored outreach support to improve alcohol screening and brief intervention in aboriginal community controlled health services. Drug Alcohol Rev. 2013;32(1):72–9.
Cowan PF. An intervention to improve the assessment of alcoholism by practicing physicians. Fam Pract Res J. 1994;14(1):41–9.
Gibson-Helm ME, Rumbold AR, Teede HJ, Ranasinha S, Bailie RS, Boyle JA. Improving the provision of pregnancy care for aboriginal and Torres Strait islander women: a continuous quality improvement initiative. BMC Pregnancy Childbirth. 2016;16:118.
Gilkes LA, Liira H, Emery J. Audit and feedback by medical students to improve the preventive care practices of general practice supervisors. Aust Fam Physician. 2017;46(1):65–9.
Gowin E, Avonts D, Horst-Sikorska W, Dytfeld J, Michalak M. Stimulating preventive procedures in primary care. Effect of PIUPOZ program on the delivery of preventive procedures. Arch Med Sci. 2012;8(4):704–10.
Holtrop JS, Dosh SA, Torres T, Arnold AK, Baumann J, White LL, et al. Nurse consultation support to primary care practices to increase delivery of health behavior services. Appl Nurs Res. 2009;22(4):243–9.
Johnson JA, Seale JP, Shellenberger S, Hamrick M, Lott R. Impact of system-level changes and training on alcohol screening and brief intervention in a family medicine residency clinic: a pilot study. Subst Abuse Treat Prev Policy. 2013;8:9.
Lapham GT, Achtmeyer CE, Williams EC, Hawkins EJ, Kivlahan DR, Bradley KA. Increased documented brief alcohol interventions with a performance measure and electronic decision support. Med Care. 2012;50(2):179–87.
Lawner K, Doot M, Gausas J, Doot J, See C. Implementation of CAGE alcohol screening in a primary care practice. Fam Med. 1997;29(5):332–5.
Lustig JL, Ozer EM, Adams SH, Wibbelsman CJ, Fuster CD, Bonar RW, et al. Improving the delivery of adolescent clinical preventive services through skills-based training. Pediatrics. 2001;107(5):1100–7.
Marco Garcia MT, Cabrera De Leon A, Torres Lana A, Perez Mendez LI, Marquez Montero MA, Sierra Lopez A. Continuous quality improvement in primary health care: a five year project. Eur J Pub Health. 1999;9(2):131–6.
Olfson M, Braham RL. The detection of alcohol problems in a primary care clinic. J Community Health. 1992;17(6):323–31.
Seale JP, Johnson JA, Clark DC, Shellenberger S, Pusser AT, Dhabliwala J, et al. A multisite initiative to increase the use of alcohol screening and brief intervention through resident training and clinic systems changes. Acad Med. 2015;90(12):1707–12.
Seale JP, Shellenberger S, Boltri JM, Okosun IS, Barton B. Effects of screening and brief intervention training on resident and faculty alcohol intervention behaviours: a pre- post-intervention assessment. BMC Fam Pract. 2005;6:46.
Seale JP, Shellenberger S, Tillery WK, Boltri J, Vogel R, Barton B, et al. Implementing alcohol screening and intervention in a family medicine residency clinic. Subst Abus. 2005;26(1):23–31.
Si D, Bailie RS, Dowden M, O'Donoghue L, Connors C, Robinson GW, et al. Delivery of preventive health services to indigenous adults: response to a systems-oriented primary care quality improvement intervention. Med J Aust. 2007;187(8):453–7.
Glass JE, Hamilton AM, Powell BJ, Perron BE, Brown RT, Ilgen MA. Specialty substance use disorder services following brief alcohol intervention: a meta-analysis of randomized controlled trials. Addiction. 2015;110(9):1404–15.
Gardner K, Bailie R, Si D, O'Donoghue L, Kennedy C, Liddle H, et al. Reorienting primary health care for addressing chronic conditions in remote Australia and the South Pacific: review of evidence and lessons from an innovative quality improvement process. Aust J Rural Health. 2011;19(3):111–7.
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–26.
Wolfenden L, Williams CM, Wiggers J, Nathan N, Yoong SL. Improving the translation of health promotion interventions using effectiveness-implementation hybrid designs in program evaluations. Health Promot J Austr. 2016;27(3):204–7.
World Health Organization. Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.
Segura L, Anderson P, Gual A. Optimizing the delivery of interventions for harmful alcohol use in primary healthcare: an update. Curr Opin Psychiatry. 2018;31(4):324–32.
Patton MQ, McKegg K, Wihipeihana N. Developmental evaluation exemplars: principles in practice. New York: The Guildford Press; 2016.
Gardner K, Sibthorpe B, Chan M, Sargent G, Dowden M, McAullay D. Implementation of continuous quality improvement in aboriginal and Torres Strait islander primary health care in Australia: a scoping systematic review. BMC Health Serv Res. 2018;18(1):541.
Bernet AC, Willens DE, Bauer MS. Effectiveness-implementation hybrid designs: implications for quality improvement science. Implement Sci. 2013;8(1):S2.
Sibthorpe B, Gardner K, Chan M, Dowden M, Sargent G, McAullay D. Impacts of continuous quality improvement in aboriginal and Torres Strait islander primary health care in Australia: a scoping systematic review. J Health Organ Manag. 2018;32(4):545–71.
Acknowledgements
This work was supported by the Australian National Health and Medical Research Council (NHMRC) through a Project Grant (Project Grant ID#105339) and Practitioner Fellowship (K. Conigrave, Grant ID#117582). We would like to acknowledge the input and advice of Professor Simon Coulton of the Centre for Health Services Studies, University of Kent; and Professor Ross Bailie of the Centre of Research Excellence in Integrated Quality Improvement in Indigenous Primary Health Care, the University of Sydney.
Funding
This work was supported by the Australian National Health and Medical Research Council (NHMRC; Project Grant ID#105339) and by an Australian National Health and Medical Research Council Practitioner Fellowship for K Conigrave (Grant ID# 1117582). The funder had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
MD: designed search strategy and protocol, undertook abstract and full text screening, extracted data, drafted paper, synthesised co-authors’ comments. KL: chief investigator on the grant supporting this work; contributed to protocol development, screening process, reviewed drafts of paper. CW: contributed to planning of the review; independently undertook abstract and full text screening, reviewed draft of paper. JB: reviewed drafts of paper and interpretation of findings with regards to CQI. NP: reviewed drafts of paper and interpretation of findings with regards to CQI. JC: contributed to planning of the review; reviewed draft of paper. NH: chief investigator on the grant supporting this work; informing team on practical aspects of primary care delivery; reviewed draft of paper. KC: chief investigator on the grant supporting this work; contributed to protocol development, screening process, oversaw the scientific integrity of the study, reviewed drafts of paper. All listed authors have reviewed the manuscript and approved the submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Dzidowska, M., Lee, K.S.K., Wylie, C. et al. A systematic review of approaches to improve practice, detection and treatment of unhealthy alcohol use in primary health care: a role for continuous quality improvement. BMC Fam Pract 21, 33 (2020). https://doi.org/10.1186/s12875-020-1101-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-020-1101-x